
Abstract
In this report, we review the use of the New Zealand White rabbit as the experimental animal for several models of abdominal wall repair. For the repair of an abdominal wall defect, such as a hernia in clinical practice, multiple types of prosthetic material exist. Before their marketing, each of these biomaterials needs to be tested in a preclinical setting to confirm its biocompatibility and appropriate behavior at the different tissue interfaces. For preclinical trials, we have always used the New Zealand White rabbit as the model owing to its ease of handling and suitable size. This size allows for laparoscopic studies designed to follow the behavior in real time of a biomaterial implanted at the peritoneal interface, a delicate interface that often gives rise to complications in human practice. The size of the rabbit also offers a sufficiently large number of implant samples to be harvested for a complete battery of tests at several time points postimplant. In this review, we first describe the models established and then provide the results obtained so far using these models to test the different types of biomaterial. We end our review with a discussion of the clinical implications of these results.
Introduction
A
The tension-free hernia repair procedure of Lichtenstein et al. 3 using a biomaterial was a cornerstone in the field of surgical techniques designed to repair abdominal wall defects. The same has occurred with the repair of incisional hernias, in which the use of a mesh to avoid recurrence is today the mainstay of treatment. 4
The development of different types of biomaterial for the repair of tissue defects in the abdominal wall is today a growing topic of research. Developments over the past 20 years have entailed modifications to the different biomaterials in pursuit of a prosthetic material showing optimal behavior at every interface. However, the ideal prosthesis does not exist and the different biomaterial designs seek to approach a normal tissue repair or regeneration process.
The new generation materials have taken into account the characteristics of the host tissue and its biology to improve integration within it, making them serve as supports or scaffolds made of materials of characteristics as similar as possible to the tissue in which they will be implanted. Hence, biologists, pathologists, chemists, and engineers all play a role as the different prototype materials must be subjected to in vitro and in vivo biocompatibility studies, and their mechanical strength and elasticity also need to be tested.
Computer simulation models and biomechanical models are also important for the development of these new materials. Using these tools, we can recreate important parameters such as pressure forces (intracavity abdominal), tension of tissues under stress, etc., which act directly on the prosthetic material to be implanted.5–7 In this way, materials that adapt in a more physiological way to the dynamic requirements of the abdominal wall can be generated. In some cases, risk factors can even be predicted for the patient who is going to undergo a major hernia procedure through an analysis of the preoperative situation of the abdominal cavity using the scanner. 8
There is therefore an obvious need for preclinical studies to address the behavior of the large number of new biomaterials emerging from industry when implanted at the different host tissue interfaces and also a need for a model capable of translating the results of such studies to human clinical practice.
Animal Models for Abdominal Hernia Research
Most models have been designed to assess the behavior of the different biomaterials available at different tissue interfaces. The two interfaces with most clinical applications are tissue/tissue and tissue/visceral peritoneum.
Several animal species have been used for such models. A recently published article that analyzes European literature on this subject between 2000 and 2014, reports around 53% of studies in the rat, 21% in rabbit, 17% in pig, and a minority in other animal models. This critical overview concluded that there is a lack of comparability among experimental hernia studies, limiting the impact of this experimental research and proposing the creation of guidelines. 9 The models most widely used have been the rat10,11 and rabbit.7,12 In our research group, the selected preclinical model was the rabbit. The selection criteria used are provided in Table 1 (in-house creation). We find the rabbit ideal for this purpose because despite its small size, in comparison with the rat, it allows us to create fairly large abdominal wall defects so that we can easily obtain samples for morphological, biocompatibility, and mechanical studies to assess the biomaterial's behavior. Another important factor that supports our choice of this animal model is that it is easier to manipulate than other larger animals such as the pig. The latter require more complex anesthesia procedures with the corresponding intubation and monitoring, 13 whereas in the case of the rabbit, an intramuscular injection is sufficient for surgery. In addition, we must also consider that larger animals need specific housing facilities in terms of size and environmental conditions not available for all animals.
+++, ideal; +, not suitable.
Finally, to examine the prosthetic material behavior at the peritoneal interface, our group and other groups 14 have implemented sequential laparoscopy studies. This endoscopic procedure allows for the sequential follow-up in a single animal of the behavior of a biomaterial at the peritoneal interface. Thus, data can be obtained at different times of study in the same animal, thus reducing the number of experimental animals. For this procedure, the New Zealand White rabbit offers several benefits such as providing a wide view of the peritoneal cavity after creating a pneumoperitoneum. This protocol has many implications for clinical practice. Through preclinical studies designed to examine this interface, many complications that may arise in patients following prosthetic mesh implant, such as intestinal obstruction, 15 fistula,16,17 or even mesh migration to hollow organs, 18 may be better understood.
Types of biomaterials for assisted healing in hernia repair
Experimental models of abdominal wall implant allow for a good assessment of how prosthetic materials behave. According to their structure and composition, we have classified prosthetic materials into four groups.
Reticular polymer
These biomaterials are generally composed of nonabsorbable polypropylene or polyester. Some of these meshes may also incorporate an absorbable component. Depending on their weight (g/m2) and pore size they are described as high and low density, otherwise known as heavyweight and lightweight.
Laminar polymer
These are sheet-like or films made of nonabsorbable materials such as expanded polytetrafluoroethylene (ePTFE) or absorbable copolymers such as polyglycolic acid:trimethylcarbonate.
Biological meshes
Also known as biomeshes or bioprostheses, these materials of laminar structure are made of decellularized dermis collagen, intestinal submucosa, or pericardium. They may feature covalent bonds between collagen fibers, known as crosslinking, which confers the material stability and lengthens its absorption time. Biomeshes that are not crosslinked show a faster absorption time than crosslinked materials.
Composites
These have two components, a reticular component (usually polypropylene or polyester) and a laminar component, which may be absorbable (films of polyethylene glycol/glycerol, hyaluronic acid, polydioxanone/cellulose, etc.) or nonabsorbable (ePTFE, polyurethane).
Preclinical models in the rabbit
In our research group, all preclinical trials are based on the use of the New Zealand White rabbit weighing 2200–3200 g depending on the model. All surgical procedures are conducted at the Experimental Animal House of the Universidad de Alcala, Madrid and approved by the Ethics Committee for Animal Experiments following the Guidelines for the Care of Laboratory Animals (Law 32/2007, Royal decree 53/2013) and European Legislation (EU Directive 2010/63/EU, European Convention ETS123).
The different abdominal wall injury/repair models have been designed and adapted according to the needs of the problem to be solved.
Complete/partial defect model (intracavity/extracavity)
Within this category, we have standardized the creation of two different types of defects in the ventral wall of the abdomen. Defects may be full thickness, involving the excision of all planes of the abdominal wall (fascial, muscular, and peritoneal)19,20 or may be partial, in which the muscular plane and the parietal peritoneum are spared. 21
For the full-thickness model, our research team has mainly used defects covering a 7 × 5 cm surface area of the ventral wall of the abdomen along its longitudinal axis, which are repaired with a prosthetic mesh of similar size to the defect and secured to the edges of the defect. Thus, the implanted mesh will be in direct contact with the visceral peritoneum (Fig. 1A). This model allows for the study of biomaterial behavior at both interfaces biomaterial/tissue and biomaterial/peritoneum.

Another possibility is to create a partial defect (including internal and external muscle, sparing the transverse muscle and parietal peritoneum) in the abdominal wall of 3 × 3 cm on both sides of the linea alba 22 (Fig. 1B). This model is especially useful when several types of biomaterial need to be tested and the experimental design is to compare the materials in terms of their morphological or biocompatibility behavior.
In both the full-thickness and partial defect models, the biomaterials are fixed to the defect with a running suture interrupted at the defect's four corners. In both cases, the skin and subcutaneous tissue are left overlying the biomaterial.
Intracavity model (within the peritoneal cavity)
Another useful model is the implant of a biomaterial inside the peritoneal cavity, fixing it to the internal sides of the cavity over the parietal peritoneum.23–26 This model is designed to examine the biomaterial/visceral peritoneum interface and thus assess the implant incorporation process involving the creation of a new or neoperitoneum, mesothelialization, and allowing also the sequential evaluation of adhesion formation. The model is scarcely aggressive as no defect is created. The prosthetic material is rather placed on the parietal peritoneum (Fig. 2). In addition, intracavity manipulation is minimal and there is no bleeding. This means the biomaterial/visceral peritoneum interface can be examined with no interference during the implant process.

Different biomaterials implanted inside the abdominal cavity on the intact parietal peritoneum. Color images available online at
In some cases, adhesion formation can be induced by making small abrasions on the visceral peritoneum10,27 or on the parietal peritoneum. 28 These models are used to evaluate the physiological mechanisms that determine adhesion formation or how the incorporation of a prosthetic material takes place in adverse conditions.
Open implant model
In the open experimental model, the biomaterial is left in contact with the outside. Temporary closure is sometimes necessary in clinical practice especially for the prevention or treatment of compartment syndrome. One of the options available for tension-free closure of the abdomen subjected to high intracavity pressure is the use of a biomaterial. 29
In a model designed by our group to assess situations of temporary closure of the abdomen, 30 full wall defects measuring 7 × 4 cm are created following the long abdominal axis, and the biomaterials are fixed to the cut muscle cutaneous edges by placing a running suture (Fig. 3). The difference with the full-thickness defect model is that in the open model the implant is not left covered by subcutaneous tissue and skin.
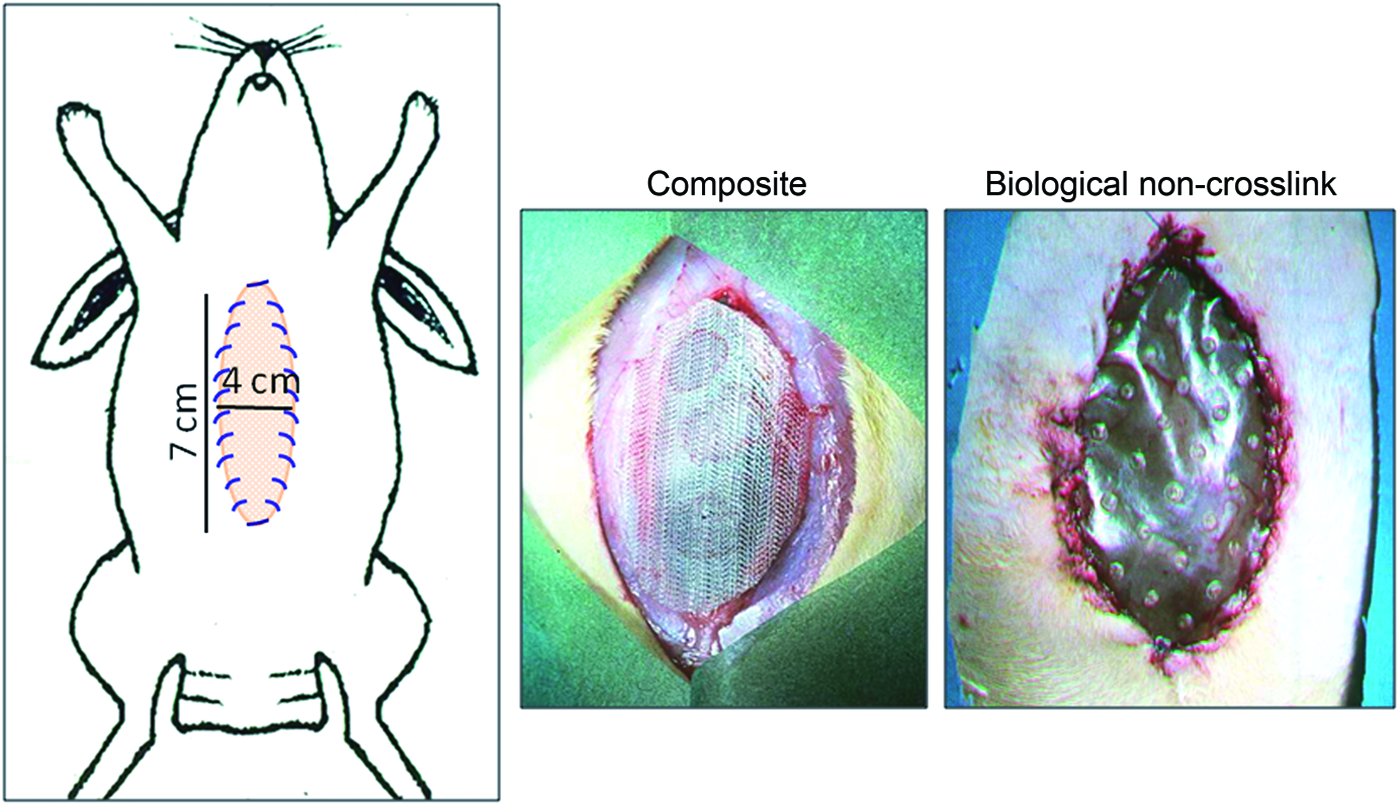
Diagram of the defect created in an experimental temporary closure model repaired using composite or biological laminar mesh. Color images available online at
Methods of Analysis in Hernia Repair
The different preclinical animal models presented above will give us very extensive and varied information that can be analyzed in different ways. The methods of analysis most commonly used in hernia repair and routinely performed in our research group are described below.
Laparoscopic examination
Usually investigations require multiple animals to verify the behavior of a biomaterial at different predetermined study times. Sequential laparoscopy allows us to examine over time the behavior of the implanted material in contact with the peritoneal cavity in a single animal. Thus, implant progress and the formation and progression of adhesions to the different biomaterials can be monitored during the initial postimplant stages (3, 7, 14 days). One of the pioneering works in this field was an experimental study by Baptista et al., in which they followed adhesion formation to an intraperitoneal polypropylene implant in the rat. 14
For the laparoscopy study in the rabbit, an optics of 3 mm and 0° (Karl Storz, Tuttlingen, Germany) is introduced into the peritoneal cavity through a metal trocar (Karl Storz) making a 0.5 cm skin incision. The pneumoperitoneum is achieved using CO2 at a maximum pressure of 8 mm Hg. Other authors have used pressures of only 3 mm Hg and even make insufflations without manometric control with ambient air.31,32
Tolerance of this method is optimal, and the peritoneal cavity can be revised after biomaterial implant so that its behavior can be directly and sequentially followed. During the procedure, videos and photographs are taken for subsequent analysis of the adhesion formation process. To complete the laparoscopic study, a macroscopic assessment of the implant is made at the established time point.
Adhesion formation is assessed using an in-house protocol
33
in which we undertake a qualitative and quantitative morphometric analysis of the implanted biomaterial. Using transparent polyethylene templates of the same size as the implants, we trace the zones of adhesions formed to each implant at the given time points. Adhesions are then quantified through image analysis of the templates (Image J. NIH;

Other authors have described several classifications of adhesion formation depending on their origin, anatomical location, or consistency.35,36 One of the most used is that of Diamond et al., 37 in which different adhesion scores were assigned according to the percentage coverage of the prosthetic mesh surface (0%: 1, <25%: 2, <50%: 3, <75%: 4, >75%: 5).
Tissue incorporation
Once a prosthetic material is implanted, an inflammatory reaction is induced in an attempt to remove it or isolate it from the host tissue. After this initial response, a cellular response takes place that gives rise to the start of the process of integration of the biomaterial within the host tissue. Morphological, immunohistochemical, and molecular biology studies provide information on the events that regulate this process, and are the most useful techniques to analyze the progression of the implant and the neoformed tissue.
Morphological studies
Once the established implant time has been reached, first of all an exhaustive macroscopic evaluation of the mesh implant and host tissue is performed to compile data on the host tissue incorporation of the different biomaterials. Observations relative to whether the biomaterial becomes encapsulated, shrinks, shows dehiscence, or seroma forms etc., provide useful information regarding the prosthetic material's biocompatibility.
Following this macroscopic evaluation of the implant, microscopy studies can be conducted through standard light microscopy and scanning electron microscopy procedures. These observations are made on fragments of mesh containing the biomaterial/host tissue interface retrieved from the experimental animal. These two techniques complement each other and allow for the study of how the biomaterials become integrated into the host tissue. In the case of intraperitoneal implants, they also provide information about the mesothelial lining and can be used to determine the thickness of the neoperitoneum, defined as the distance between the implanted biomaterial and newly formed mesothelium.
Immunohistochemical studies
To detect specific cells and proteins at the implant site, monoclonal antibody labeling techniques based on immunohistochemistry and immunofluorescence are used for the evaluation of the inflammatory response by examining macrophages and lymphocytes, markers of the repair process such as TGFβ, metalloproteinases, and collagens.33,38–40 or to evaluate the proliferation state of cells forming the neoformed tissue 41 or even possible cellular damage. 42
For our research group, both assessment of the macrophage response to implants and of the progression of neoformed scar tissue are important routine techniques, since they provide useful information on the behavior of a biomaterial and its tolerance by the organism. To assess the macrophage response to the implanted biomaterial produced in the host animal, the monoclonal antibody anti-RAM-11 against rabbit macrophages is used (Dako, Glostrup, Denmark).
In the extracellular matrix of the neoformed connective tissue, one of the most important fibrillar components also routinely studied by our group is collagen. For the tissue repair of a damaged area constantly subjected to tensile forces such as the abdominal wall, optimal collagenization is an extremely important factor. The proper deposition and organization of mainly collagen type I in the neoformed scar tissue will condition the mechanical strength and compliance of the repair zone and thus possible hernia recurrence. 43 The collagen component of the implants is assessed by immunofluorescence using anticollagen type I (Sigma-Aldrich) and type III (Medicorp, Montreal, Quebec, Canada) monoclonal antibodies. Samples are examined using a confocal microscope Leica SP5 (Leica Microsystems, Wetzlar, Germany) that belongs to the platform ICTS “NANBIOSIS” (Confocal Microscopy Service, U17) of the facility Networking Biomedical Research Center on Bioengineering, Biomaterials, and Nanomedicine (CIBER-BBN) at the University of Alcalá, Madrid, Spain.
Gene expression
The above information regarding protein expression in tissue healing can be complemented with molecular level analyses (RT-PCR, microarray).43,44 Gene expression is the process by which genetic information is converted into a protein product, using an intermediate molecule RNA, which is transcribed from DNA and used as a template. Genetic expression studies are an important tool for analyzing how the genetics of the organism allows it to function and respond to its environment, quantifying the level of expression of a gene of interest.
In our laboratory, tissue fragments are obtained from the implant area comprising the given biomaterial and ingrown neoformed host tissue and stored at −80°C until use. Total RNA is extracted and complementary DNA is synthesized by reverse transcription. The cDNAs are amplified using different primers and iQ SYBR Green Supermix (Bio-Rad Laboratories, Hercules, CA). In our group, collagen 1 and collagen 3 gene expressions are usually analyzed. 43 Anti- and proinflammatory factors have also been evaluated to check the inflammatory reaction in full-thickness abdominal wall repair. Gene expression is then normalized against the expression recorded for the constitutive gene glyceraldehyde 3-phosphate dehydrogenase.
Biomechanical studies
Biomechanical tests are considered optimal to determine the mechanical properties of any material. There are several tests to determine the properties of a prosthetic material, such as, for example, mechanical tensile strength, shear resistance, or resistance to deformation. These tests include suture retention, tear resistance, uniaxial/biaxial, and ball burst tests.45,46
Once the biomaterial has been implanted in the abdominal wall, the most frequent tensiometric tests are uniaxial, shear stress, and ball burst tests. To analyze the mechanical behavior of the implant site, we designed a protocol in which crosswise strips of the implant are cut of width 1.5–2 cm, depending on the initial implant size that include the two lines of suture used to fix the implant to the host tissue. These strips can be used to assess the mechanical resistance to breakage of the different implanted biomaterials. For the tensile strength measurements, we use an INSTRON 3340 tensiometer (Instron Corp., Norwood, MA). The device offers computerized analysis of break forces and elasticity of the different prosthetic materials before and after their implant. In our experimental design, test speed is set to 2 cm/min and the distance between the two grips to 5–7 cm, depending on the initial implant size (Fig. 5). Results are expressed in Newtons (N).

There are other tests that are used to determine the stability of the fixation elements (sutures, tackers, tissue adhesives) of the prosthetic materials to the abdominal wall or how the tissue is integrated with the biomaterial. Among others, these include the T-peel tension loading test and the lap shear stress test.47,48 For these tests, we position the samples so that the upper edge of the mesh peels away from the abdominal wall and is inserted between the instrument's clamps such that the top clamp grips the mesh and the bottom clamp clasps the abdominal wall 1 cm from the lower fixation point of the mesh. 43
Distension tests calculate strength or stiffness by applying a constant load to the sample perpendicular to it using a spherical load applicator.41,49 These tests are used to determine implant compliance and how variations in intra-abdominal pressure during coughing, sneezing, or jumping may affect the properties of the biomaterial. 50
Information Gained from Selected Models
In our animal models, special attention has been given to the formation of seroma. This is one of the main early clinical complications of hernia repair using meshes and in its most severe forms may jeopardize the clinical outcome of surgery. 51 Our longstanding experience has shown us that during the first days of implant of a prosthetic material, whether seroma forms or not, is closely related to the material's structure. Thus, its appearance is more common for laminar materials (polymer or biological) and composites compared with reticular materials.
In laminar materials seroma can arise at the biomaterial/subcutaneous tissue interface, whereas in composites, depending on their structure, it may be observed at the biomaterial/subcutaneous tissue interface, between the different mesh components, or even at the composite/parietal peritoneum interface (Fig. 6).
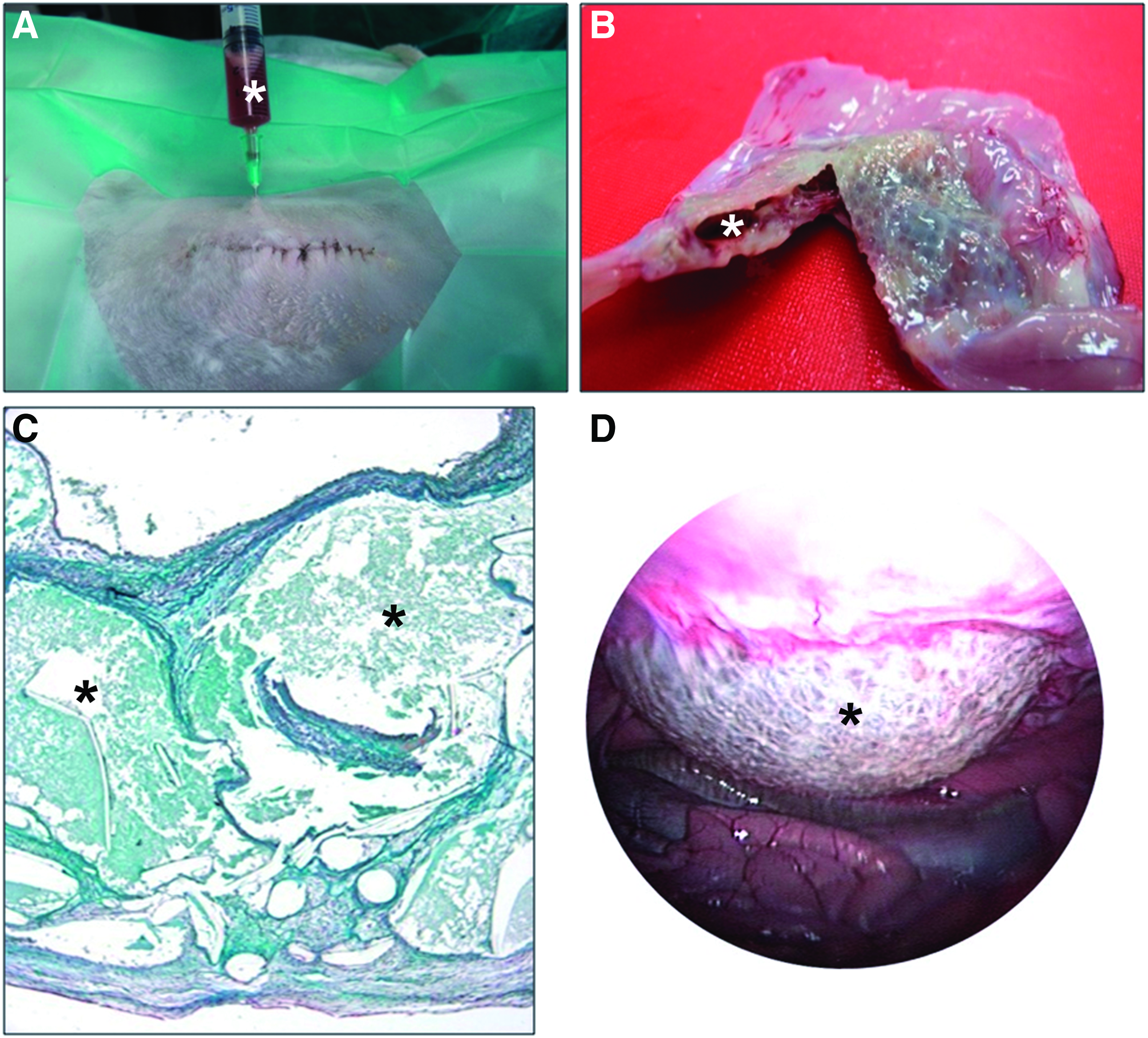
Seroma (*) formation at the different interfaces.
Laparoscopy: adhesion formation
Using intracavity models, we have assessed adhesion formation by sequential laparoscopy. It has been possible to establish that adhesion formation is a phenomenon that takes place early after implant (at 3 days) and progresses over the first week, stabilizing thereafter from days 7 to 14.14,31,33
We have noted differences in the distribution and percentage of adhesions depending on mesh structure. In general terms, reticular mesh shows marked adhesion formation across its surface irrespective of pore size. When reticular prostheses are implanted, the displacement of the intestine over the prosthesis could lead to the appearance of small microtraumas in the visceral peritoneum, leading to the accumulation of fibrin deposits that could lead to adhesion formation. These adhesions involve both the omentum and visceral peritoneum and are usually of the loose or firm type in initial stages, but may transform into integrated type adhesions over the course of study.
In contrast, laminar materials, whether polymer or biological, and composites behave better at this interface as they induce fewer adhesions which are mainly restricted to the fixation zones of the mesh to the host tissue (Fig. 7). The smoother surface of the laminar materials determines that the intestine can easily slide across the prosthesis, reducing or avoiding the damage to the visceral peritoneum. 52

Sequential laparoscopy images taken of different types of implant. Color images available online at
Tissue integration
In terms of tissue ingrowth in the implant area, significant differences have been made evident in our preclinical models depending on the properties of the implanted prosthetic material.
Reticular polymer
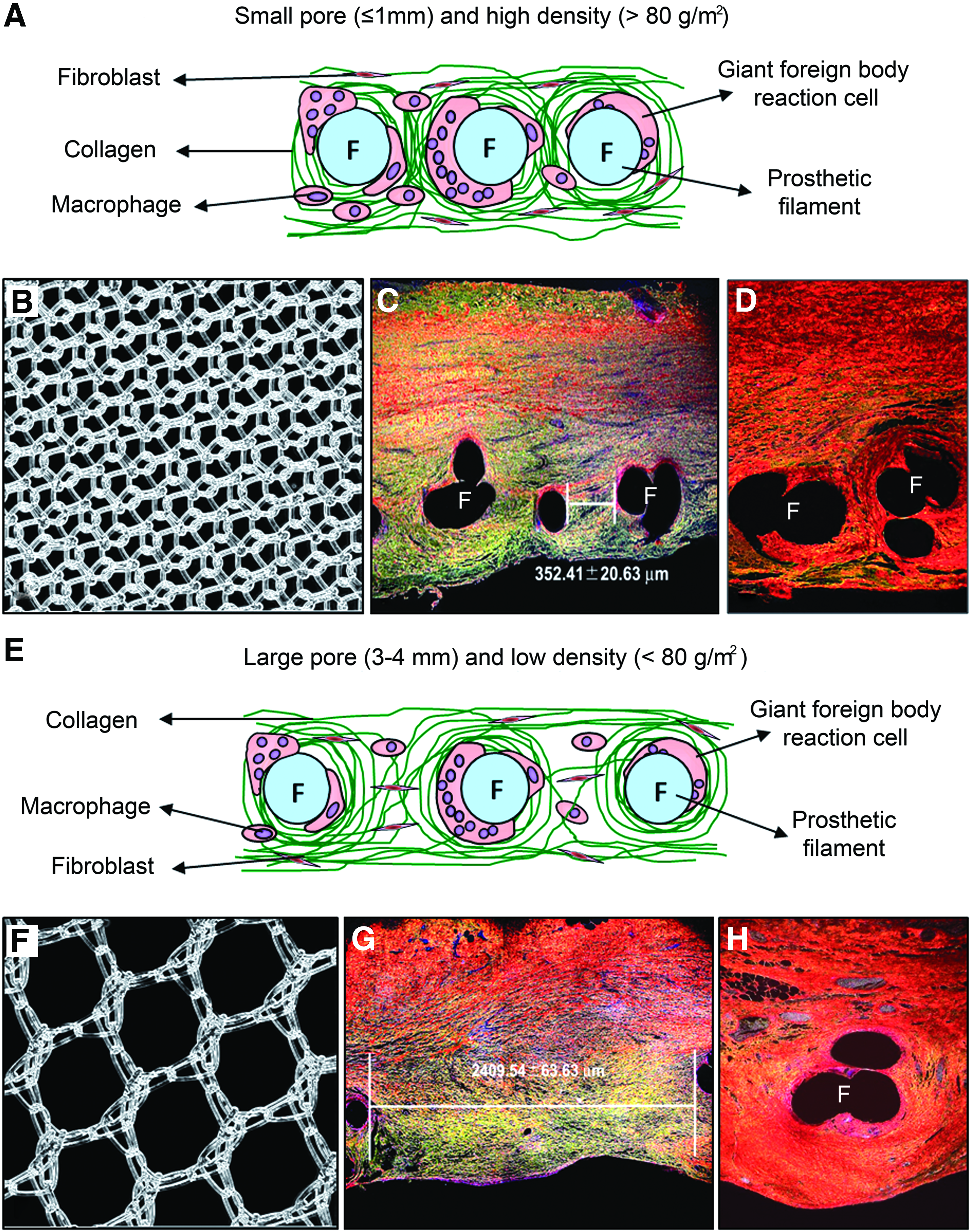
In the early stages postimplant (14 days) reticular materials with small pores become fully infiltrated by a loose connective tissue with the abundant presence of collagen type III fibers arranged concentrically around the prosthetic filaments. Among collagen fibers, fibroblasts and white blood cells may be observed, along with small- and medium-caliber blood vessels. As time advances (30–180 days postimplant), more cells are found around the mesh filaments and connective tissue acquires a more dense consistency predominated by collagen type I.
In some cases, when pore size is larger, there may be a slight delay in neoperitoneum formation and mesothelial cover, which in the long term appears as on the meshes with smaller pores (Fig. 8). Mesothelial cover on reticular materials is interrupted in zones showing adhesions.
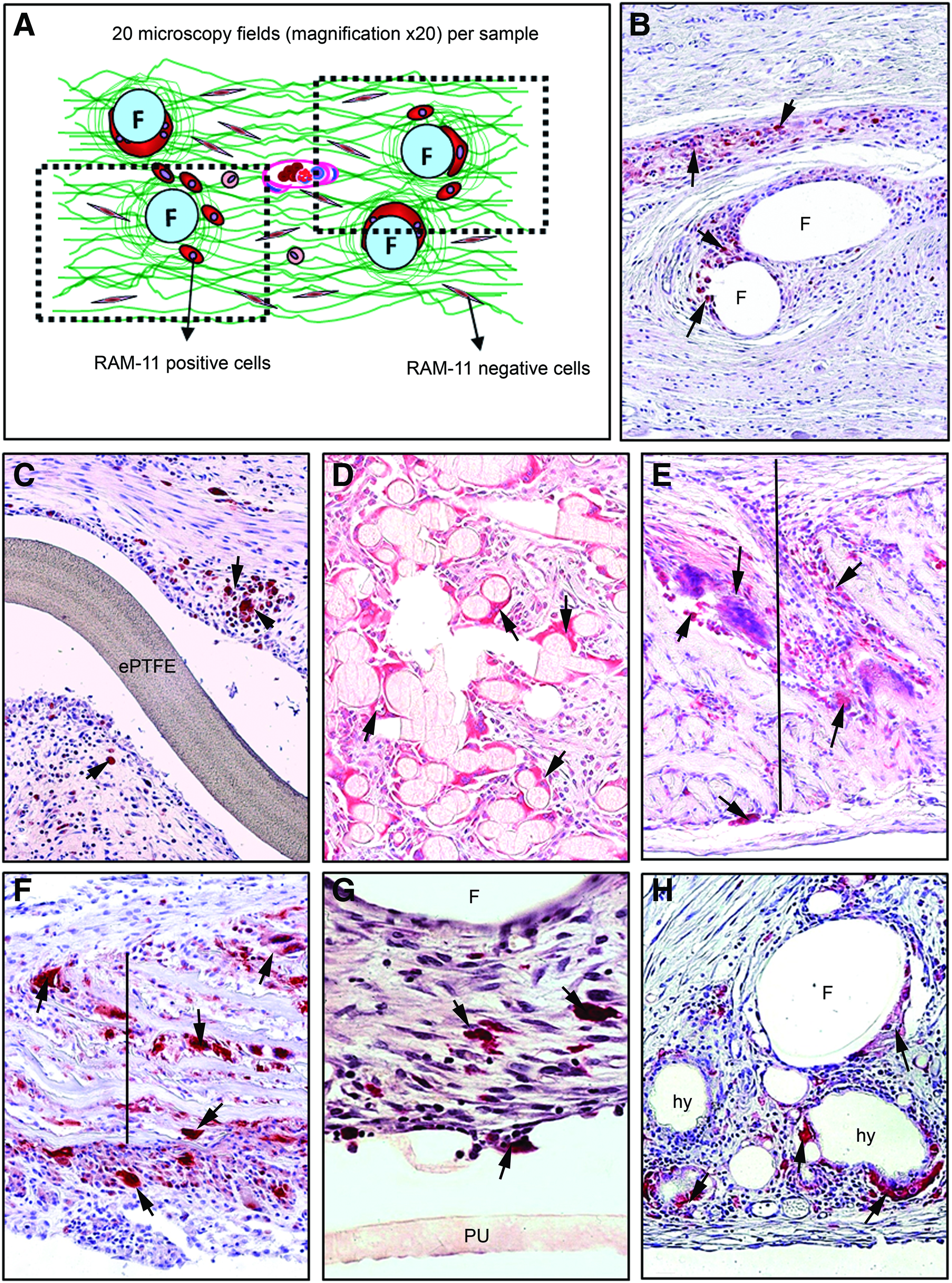
For these materials, the macrophage response is greater after 14 days of implant and diminishes gradually after this time point. Labeled cells occur around the prosthetic filaments, including isolated macrophages and giant foreign body reaction cells throughout the implant (Fig. 9A, B).
Laminar polymer
These materials characteristically induce the formation of a fibrous connective tissue capsule that envelops the prosthetic material and can be seen soon after implant. The connective tissue fibers are arranged parallel to the material and are accompanied by a barrier of inflammatory cells. These materials are not susceptible to cell colonization or tissue ingrowth throughout their structure, because of their microporous or nonporous surface, which makes their host tissue incorporation difficult.
Absorbable laminar biomaterials (polyglycolic acid:trimethylcarbonate) become surrounded by loose connective tissue in the short term and show the presence of collagen type III and inflammatory cells. Subsequent to this, the area occupied by the biomaterial is gradually replaced with connective tissue and collagen type I until it becomes fully absorbed after 180 days.
These materials, whether or not absorbable, show in the short term deposited mesothelial cells of secretory appearance and zones where the cell monolayer is not yet completely consolidated. At later time points, the mesothelial cover has a continuous stable appearance, similar to that of the native tissue (Fig. 10).
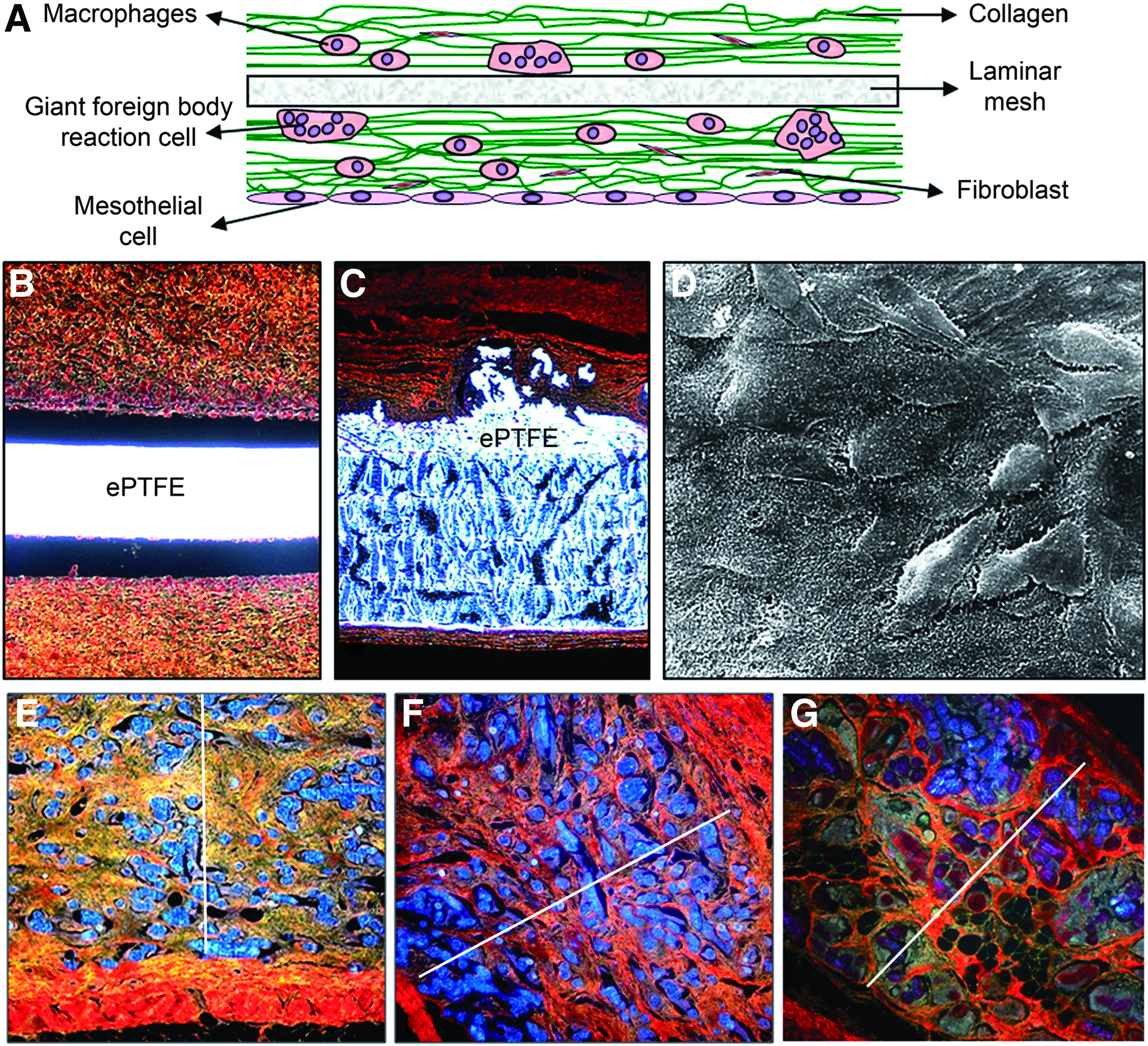
These materials appear surrounded by an inflammatory reaction showing a barrier of macrophage and giant foreign body reaction cells. The macrophage response progresses in time as for the reticular biomaterials, that is, more intense at early time points and diminishing in the long term (Fig. 9C, D).
Biological meshes
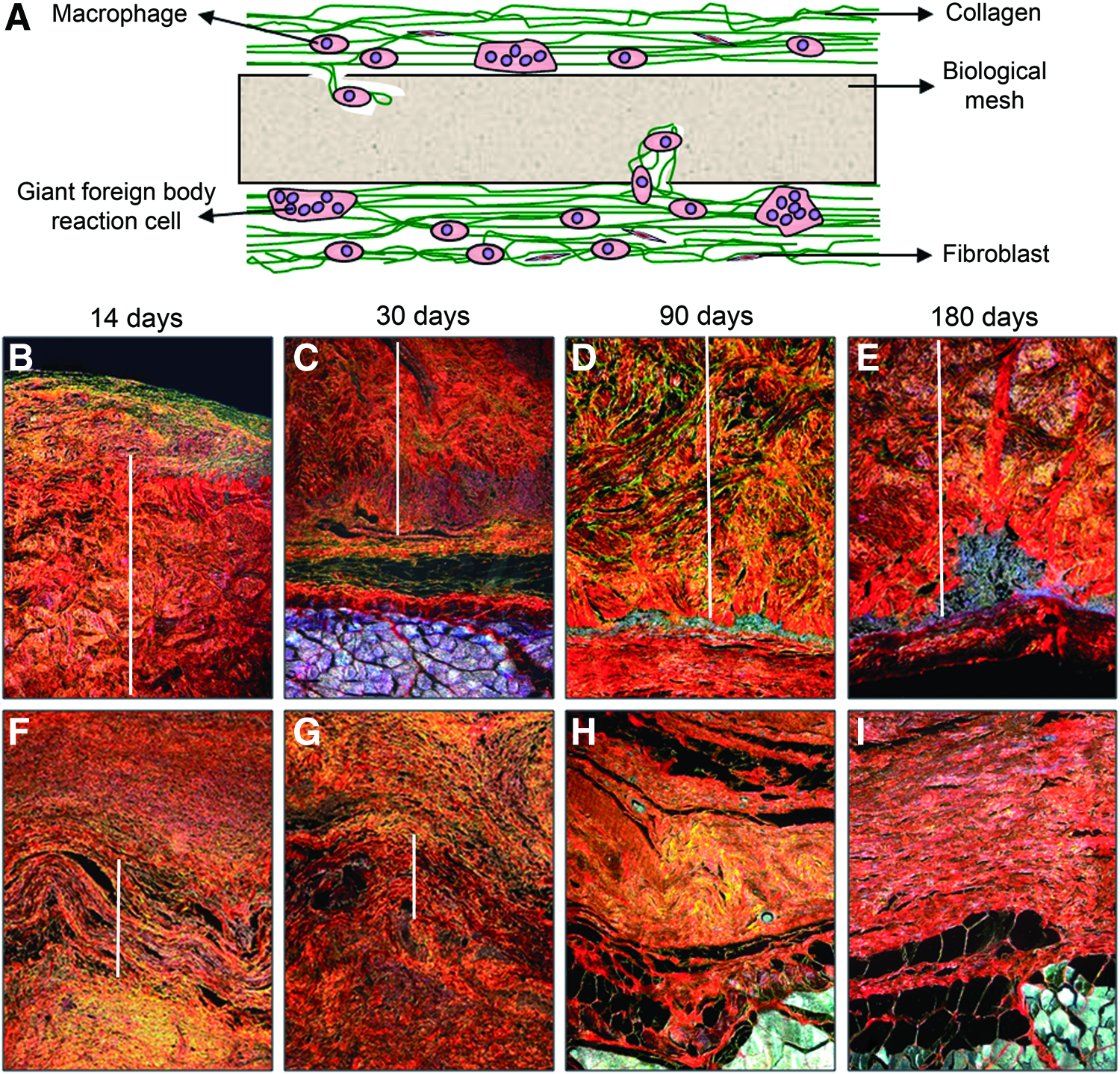
Biological meshes tend to become encapsulated by a fibrous-looking connective tissue and inflammatory cell barrier similar to the laminar polymer meshes. However, it may be observed that the cells and connective tissue gradually penetrate from the upper and lower surfaces of the host tissue, and from the anchored borders, leading to the formation of small blood vessels inside the biological material and collagen type III deposition in the tissue surrounding the implant.
The absorption of these materials over time varies according to their thickness and the presence or not of crosslinks in their structure. Generally speaking, absorption will be faster for noncrosslinked materials, although not all these biomeshes show this behavior. In the case of crosslinked biomeshes, the time of absorption is much slower, and their total absorption has not yet been confirmed. An appropriate mesothelial deposit showing a behavior similar to that of laminar materials has been confirmed (Fig. 11).
A macrophage response is observed around the implanted mesh itself forming a barrier similar to that produced around the laminar polymer mesh. However, infiltration by macrophages and giant foreign body reaction cells occurs from the margins of the material toward its interior. These materials are more reactive than polymer biomaterials and feature a larger number of cells showing positive labeling for macrophages during earlier time points that decreases in the long term (Fig. 9E, F).
Composites
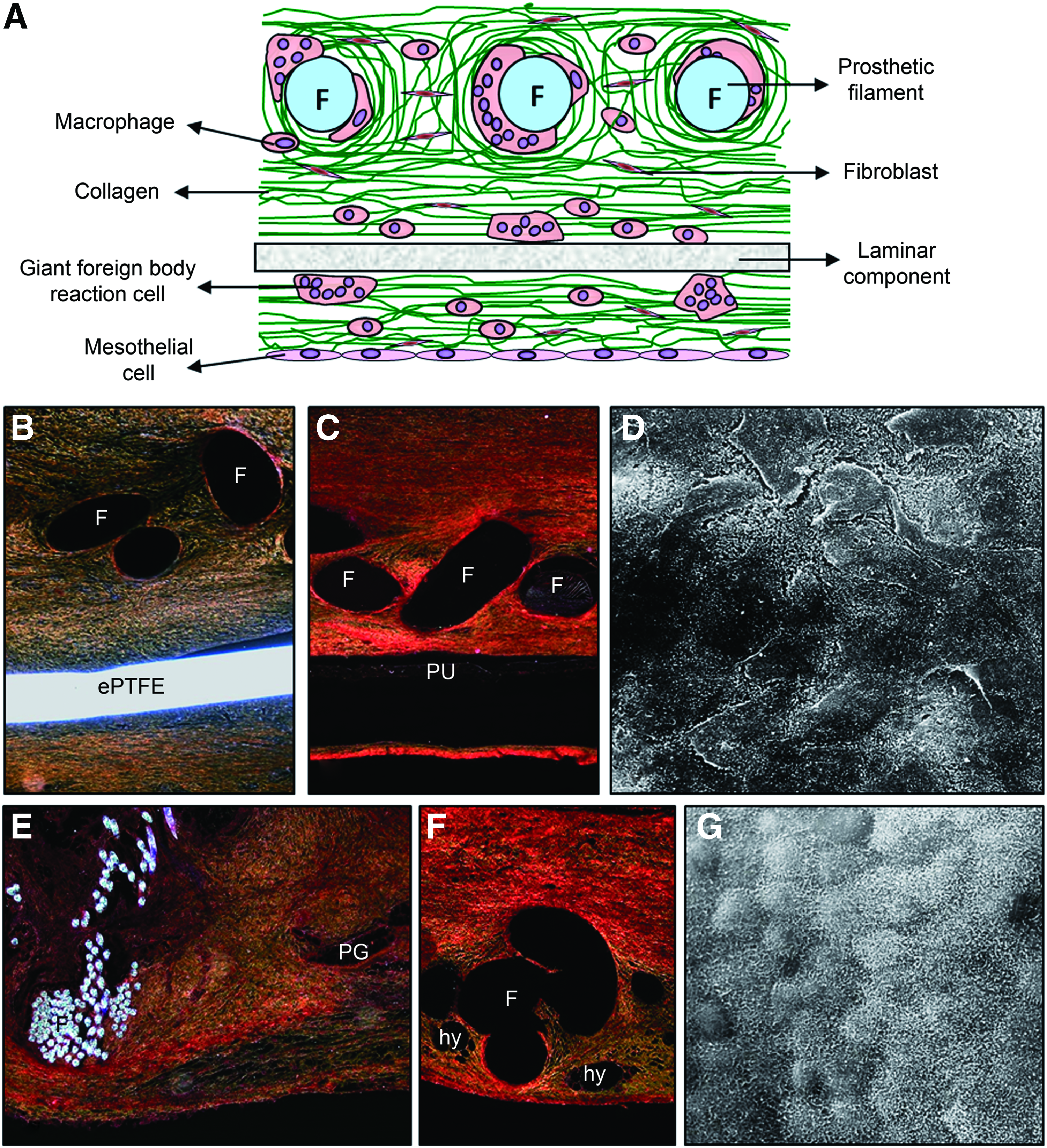
The first component of these implants, generally of the reticular type, shows very similar behavior in terms of host tissue incorporation and collagen deposition to that observed for the reticular meshes mentioned above. In the latest generation composites, this part of the biomaterial may be partially degradable.
The behavior of the second laminar component of these prosthetic materials varies according to its composition. Nonabsorbable components just like laminar polymer meshes lack porosity and thus prevent the cell colonization of their structure. In contrast, in the case of absorbable films, the sheet is gradually degraded by inflammatory cells and giant foreign body cells, determining their absorption over periods that vary according to the material used.
As in the cases above, these materials show adequate mesothelialization (Fig. 12).
Composite materials induce a macrophage reaction in which their structural components intervene. On one hand, the reticular component elicits a reaction similar to that described for the reticular materials, and on the other, the smooth laminar component contributes in greater or lesser measure depending on its composition. When there is a nonabsorbable component, the reaction provoked is similar to that shown by a laminar implant. Otherwise, an absorbable component will induce a macrophage response depending on its composition which will determine its time of absorption (short, mid, or long term) and its reactivity in the host tissue, thus giving rise to a smaller or greater proportion of macrophages (Fig. 9G, H).
Biomechanical resistance
Our biomechanical studies of the different implants have revealed that after 3 months, reticular mesh implants show a similar tensile strength regardless of their pore size and the presence of absorbable components in their structure.
In the case of laminar meshes, biomechanical behavior is similar although tensile strengths are around half the strengths observed for reticular materials.
Composites show similar strengths to reticular meshes, although there is some variation according to the components comprising each composite material.
Discussion
Preclinical animal experimental studies are necessary and useful to test the array of biomaterials we have available for the treatment of abdominal wall defects. Biocompatibility standards developed by the International Organization for Standardization, ISO 10993-6, “Biological evaluation of medical devices: Tests for Local Effects after Implantation,” represent the factors that must be taken into account when performing implant studies. Among other factors, they mention the selection of species and the evaluation of biological responses. Although ISO 10993-6 mentions different experimental animals like rats or mice, the rabbit, because of its size and easy handling, has long been the animal of choice for implant testing. With regard to assessment of the biological response, the objective of the test methods available is to characterize the course and progression of the tissue response after implantation of a biomaterial in direct contact with living tissue, including its final incorporation or absorption/degradation, as has been considered and reported in each and every one of our animal models. 53 Models in the New Zealand White rabbit have provided us with excellent information on the behavior of the different mesh implants at the abdominal wall, and helped improve our understanding of what occurs in human clinical practice.
Among the different biomaterials available, our research group has defined four broad groups in terms of their similar implant behavior essentially determined by their physical structure: reticular, laminar, biological, and composite.
The process of integration of the biomaterial within host tissue is directly related to its structure. It is the presence of porosity that modulates tissue integration, cellular penetration in the different interstices of the prosthesis, and facilitates angiogenesis.
Broadly speaking, reticular polypropylene mesh shows optimal behavior at the host tissue/tissue interface where integration is optimal. The drawback of this material is, however, its poor behavior at the peritoneal interface in intracavitary models. At this location, reticular mesh can give rise to adhesions or even to other complications such as intestinal obstruction, intestinal fistula, or implant migration to other organs as mentioned in the introduction. The basis for this behavior is that the open reticular structure of this biomaterial determines irregular mesothelial layer deposition. This means that it is the structure and not the chemical composition of a biomaterial that modulates its behavior at the peritoneal interface. 52
Conventional reticular mesh of small pore size has undergone several modifications that have given rise to a prosthetic material with larger pores and the reduced spatial organization of its filaments. Using the terminology employed by Schumpelick's group,54,55 this material is large-pore, low-density polypropylene mesh, also described as lightweight. The integration within host tissue shown by this mesh is ideal and it also induces early collagen deposition. 56 Its main benefit over the conventional small pore mesh is that it avoids excessive fibrosis given its large pores and thus interacts better with host tissue, maintaining in some measure its elasticity.57,58 In the long term, its mechanical strength is similar to that of conventional polypropylene mesh. 43
Such lightweight meshes besides consisting of a nonabsorbable material may also have an absorbable component giving rise to the so-called hybrid meshes. 59 The final objectives of these implants are essentially to minimize the amount of foreign material left in the host while trying to avoid compromising the mechanical strength of the mesh. 60 Although initially the foreign body reaction to hybrid mesh is greater than to fully nonabsorbable mesh, the idea of reducing the final amount of foreign material is an indisputable benefit, especially in young patients. In these patients, the biomaterial will remain embedded in the wall tissue for a long time period and it is still not known what changes it may undergo or reactions it may elicit after many years of implant.
Currently, new designs of reticular-type prostheses pursue alternative materials to employ in a conventional manner (polypropylene and polyester) such as ePTFE or polyvinylidene fluoride. In other designs a substance is incorporated in the filaments (titanium) to avoid adhesion formation. 61
Laminar mesh prostheses generally show deficient integration within host tissue and essentially become encapsulated by host tissue. The main benefit of laminar mesh is its easy mesothelialization when placed in contact with the visceral peritoneum in intracavity models. 62
Among the laminar materials available, the most representative is ePTFE, 63 which has undergone severe structural modifications. Initial models took the form of a patch, and evolved into a multiperforated patch with the aim to offer improved biomechanical resistance, but without success.64,65 Out of the last generation ePTFE arose the laminar implant in which tissue incorporation was achieved by its superficial side and no cell ingrowth was produced on its peritoneal side. To improve its tissue incorporation a rough surface was created. However, mechanical strength in the repair zone remained unchanged with respect to initial designs. Among its modifications, we should highlight its impregnation with a silver/chlorhexidine solution to avoid bacterial adhesion in the initial postimplant stages. Several studies have shown the benefits of this pretreatment.66,67
Another laminar polymer, but made of absorbable material, consists of polyglycolic acid:trimethylcarbonate. This mesh is reabsorbed within 90–180 days of implant. In preclinical studies, its behavior has proved similar to that of biological materials 68 showing greater adhesion formation at the peritoneal interface in intracavity animal models than laminar ePTFE.
Biological meshes are made of natural materials, usually collagens of animal or human origin.69,70 These bioprostheses or biomeshes are generated from tissues removed from their natural environment, and with or without modification act as a scaffold for cell colonization in the host tissues accommodating the implant. The goal of these biomaterials is to achieve, besides repair, tissue regeneration. Over time, these bioprostheses should become degraded in the host tissue acting as a temporary support for tissue repair.71,72 The pretreatment of these bioprostheses with different substances (glutaraldehyde, hexamethylene diisocyanate, etc.) favor the creation of covalent bonds, crosslinks that confer stability of these materials, extending their residence time in an environment in which they would be degraded by collagenases. 73 Biomeshes that are not crosslinked show a faster absorption time than crosslinked materials. 74 Their behavior at the tissue/tissue and peritoneal interface is similar to that of laminar mesh given their similar sheet structure.
These materials require strict control given their animal origin (pig or cow). Their use has been mainly restricted to hernia repair in contaminated settings.75,76 Although they have been recently approved for this purpose by the FDA, 77 they still generate some controversy. 78
When repairing a massive hernia, basically the abdominal wall has to be reconstructed and there is practically no supporting tissue. In this situation, a prosthetic mesh has to be placed in direct contact with the visceral peritoneum. For this purpose, composite type meshes have opened a wide range of possibilities, their main objective being to offer good behavior at every interface. 79
Composite prostheses have two components: one is usually the main or first component to which a second component may be added to fulfill the specific function not fulfilled by the first. Thus, the design of these prostheses is such that the first component should adopt the role of tissue incorporation while the second component should show good behavior when in direct contact with the visceral peritoneum in intracavity models avoiding adhesion formation. Both components are bound together with an acrylic adhesive, sometimes heat sealed, or sutured.80,81
The biomaterials forming the first component are usually of the reticular type, either polypropylene or polyester. The second component is usually laminar and may be absorbable or nonabsorbable. Due to the characteristics of the second component, these materials are referred to as prostheses with physical and/or chemical barriers. In the former, the second component will be nonabsorbable and in the latter it will be absorbable.46,82–85 In fact, there is not much difference between the behavior of the different barriers. Physical barriers have the drawback that more foreign material remains in the host meaning that chemical barriers are slightly more popular. 86
In summary, the New Zealand White rabbit model offers sufficient biological material for a complete battery of tests on implant specimens taken at several time points. This preclinical experimental animal also allows for procedures such as laparoscopy providing useful information on the behavior of different biomaterials at such a delicate interface as is the peritoneal. Our intra- and extracavity models have also enabled us to assess the behavior of a wide variety of prosthetic materials at different implant sites and thus determine the most suitable materials for each particular interface.
Overall, through the use of the experimental animal models described in this study, we have been able to accurately assess the behavior of a wide array of biomaterials used to repair abdominal wall defects. The reproducible qualitative and quantitative data obtained from these models have useful implications for human clinical practice.
Footnotes
Disclosure Statement
No competing financial interests exist.