
Abstract
Meniscus injuries represent one of the most-common intra-articular knee injuries. The current treatment options include meniscectomy and allograft transplantation, both with poor long-term outcomes. Therefore, there is a need for regenerative techniques to restore meniscal function. To preclinically test scaffolds for meniscus replacement, large animal models need to be established and standardized. This review establishes the anatomical and compositional similarities between human and sheep menisci and provides guidance for implantation and evaluation of such devices. The ovine meniscus represents a scaled-down version of the human meniscus, with only slight structural differences that can be addressed during device fabrication. Implantation protocols in sheep remain a challenge, as the meniscus cannot be visualized with the arthroscopic-assisted procedures commonly performed in human patients. Thus, we recommend the appropriate implantation protocols for meniscus visualization, ligamentous restoration, and surgical fixation of both total and partial meniscus replacement devices. Last, due to the lack of standardization in evaluation techniques, we recommend a comprehensive battery of tests to evaluate the efficacy of meniscus replacement implants. We recommend other investigators utilize these surgical and testing techniques to establish the ovine model as the gold standard for preclinical evaluation of meniscus replacement devices.
Introduction
T
Large animal models play a crucial role in the exploration of new strategies and clinical translation of novel techniques. 8 According to Madry et al., 8 the general requirements for large animal model experiments in translational orthopedic research are that the model needs to be comparable to the human species, comparative data must be available, the results must be transferable, and the surgery must be technically feasible. Several animal models (goat,9,10 dog,11,12 and pig13,14) have been utilized for testing both reparative and regenerative approaches to restore the original shape and function of the meniscus, 15 with sheep being the model most used.16–21 While studies have compared sheep and human menisci with regard to anatomy,22,23 physiology, 24 biological composition, 25 or structural mechanics26,27 individually, in this study, we synthesize the literature and opinions from our extensive hands-on experience to establish the sheep as the appropriate animal model for meniscus tissue engineering studies. Moreover, the United States Food and Drug Administration (FDA) provides guidance documents regarding cartilage 28 and ligament 29 replacement, but no such document exists for meniscus. Therefore, after establishing the utility of the ovine model, we provide guidance recommending the proper implantation and analytical techniques for preclinical evaluation of tissue-engineered meniscus devices in this large animal model.
Meniscal Anatomy
The anatomy of the meniscus is relatively well conserved between sheep and humans (Table 1). Sheep represent the best anatomical models for the human meniscus. 30 The medial and lateral menisci are semilunar, fibrocartilaginous discs with a triangular cross section, localized between the articular surfaces of the tibiofemoral joint. Due to the increased incidence of injury to the medial meniscus, 31 we recommend meniscus tissue engineering should focus on the medial meniscus in preclinical studies. These tissue engineering approaches are applicable to the lateral meniscus, provided the significant differences in anatomy, 22 kinematics, 32 and mechanics 33 are taken into account. The geometrical size of the ovine stifle is approximately two-thirds that of the human knee (Fig. 1 and Table 1). The femoral intercondylar ratio (intercondylar width divided by the epicondylar width) and tibial aspect ratio (medial-lateral dimension divided by the anterior-posterior dimension) are extremely similar, 23 indicating proportional scaling down of the joint. The average ovine meniscal width in the anterior and central regions and the slope of the superior articulating surface are comparable to the average human meniscus. 22 The meniscal length and width, proportional to the tibial plateau width, are also very comparable between humans and sheep. 30

Medial menisci of the
Mean (±SD).
Sources for dimensions are provided.
SD, standard deviation.
The gross anatomy of the medial meniscus is also similar between species. It is attached to the tibial plateau through anterior and posterior meniscotibial ligaments (or root attachments). The anterior and posterior meniscotibial ligaments connect the horns of the medial meniscus to the medial intercondylar eminence, anterior to the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) attachments, respectively. 39 However, while the anterior intermeniscal ligament directly connects the anterior horns of the lateral and medial menisci in humans, this structure is lacking in sheep. 39 In addition, unlike the separation seen in the human knee, the body of the ovine medial meniscus is strongly attached to the medial collateral ligament (MCL), which must be taken into careful consideration during implantation in the ovine model. 40
A few noteworthy dimensional differences exist and should be taken into consideration. The anterior-posterior length, the circumference of the outer margin, and the meniscal volume are different between sheep and humans. 22 In addition, the width of the posterior region is significantly greater compared with the anterior region in humans; the ovine meniscus, in contrast, is more symmetrical. To fill a gap in the literature regarding percent coverage, defined as the meniscal area divided by the underlying tibial plateau area, we imaged 12 sheep menisci (4–6 years old and 71.9 ± 9.5 kg) and 6 human cadaveric menisci (17–59 years old and 77.6 ± 20.8 kg), and used a custom MATLAB program to calculate the area of the meniscus, area of the tibial plateau, and percent coverage. The percent coverage of the ovine medial meniscus (67.97% ± 3.70%) was statistically greater (p < 0.001) than the coverage of the human meniscus (53.52 ± 3.13). These dissimilarities in size, shape, and coverage must be addressed during scaffold fabrication. The ovine posterior tibial slope is also greater in sheep, making biomechanical testing more challenging.37,40 The proximal tibial cortex is denser and thicker in sheep compared to human, 23 potentially altering osseous surgical fixation strategies.
Knee joint kinematics
There are also similarities and key differences in joint kinematics between species. The ovine knee has relatively restricted knee extension with an average range of motion of 40–146° compared to 2.5–137.5° in the human knee, meaning the ovine knee is permanently in flexion. 37 As a result, the anterior portion of the medial meniscus in sheep is loaded to a lesser extent than in humans, while in full extension. However, the differences in range of motion partially compensate for biomechanical differences caused by the increased tibial slope in the ovine knee (Table 1). 41 In the stance phase, the primary stabilizers are quite similar, although the human knee has more structures involved in secondary stabilization (handling of <5% of the total load). In addition, the applied axial force in the stance phase in the human knee is about 500 N, while it is about 300 N in sheep. 24 Interestingly, in the swing phase, there are fewer similarities between the two species. The total force in the ovine knee is ∼100 N, while the force in the human knee is about double that. In addition, there are few similarities in primary and secondary stabilizers of the knee in the swing phase. 24
It should be noted that the forces experienced within the joint reach much higher loads. Human peak femorotibial force has been estimated to range from 2.1 to 2.7 × body weight (BW) (or 1440–1850 N for a 70 kg individual) during walking and 4.2 × BW (or 2880 N for a 70 kg individual) for jogging.42,43 Ovine peak femorotibial force was found to be 2.27 × BW (or 1560 N for a 70 kg animal) during walking, comparable to humans. 44 In both species, the large majority of the force is transmitted through the medial compartment. 24 Thus, even though the sheep is a quadruped with slight differences in joint motion, the ovine knee presents an appropriate, proportionally scaled-down model of the human knee with comparable joint forces.
Meniscal Composition and Biomechanics
The sheep and human menisci also display similar compositional characteristics. For a thorough review of the composition and biomechanics of the human meniscus, the reader is directed to a review article by Fox et al. 45 The water content of human meniscus (72% 46 ) is comparable to that of ovine meniscus (68% 47 ), with the remaining dry weight being composed of primarily collagen (75%). Both sheep and human menisci exhibit type I collagen throughout the tissue, with type II collagen detected primarily in the inner half. 25 The extracellular matrix (ECM) organization is remarkably similar between sheep and humans in both the inner and outer half of the meniscus, as shown in Figure 2. One notable difference between sheep and human menisci are the relative glycosaminoglycan (GAG) contents, with sheep menisci displaying a deeper Safranin O stain (Fig. 2B), consistent with the literature 25 and with biochemical analyses.48–50 Both human and sheep menisci show a similar trend with regard to regional variation of GAG, with a deep concentration in the inner half and relatively no GAG in the outer half. The superficial lamellar layers of both human and sheep menisci are 40–65 μm thick. Cellularity is also similar between human and sheep menisci, 25 with a complex fibrochondrocytic phenotype throughout the tissue. The adult sheep meniscus also displays a high degree of structural similarity to the human meniscus, considering the cross sectional area (25.6 and 37.4 mm2 in sheep and humans, respectively) and vascular penetration (11.2% and 14.4% in sheep and humans, respectively). 25
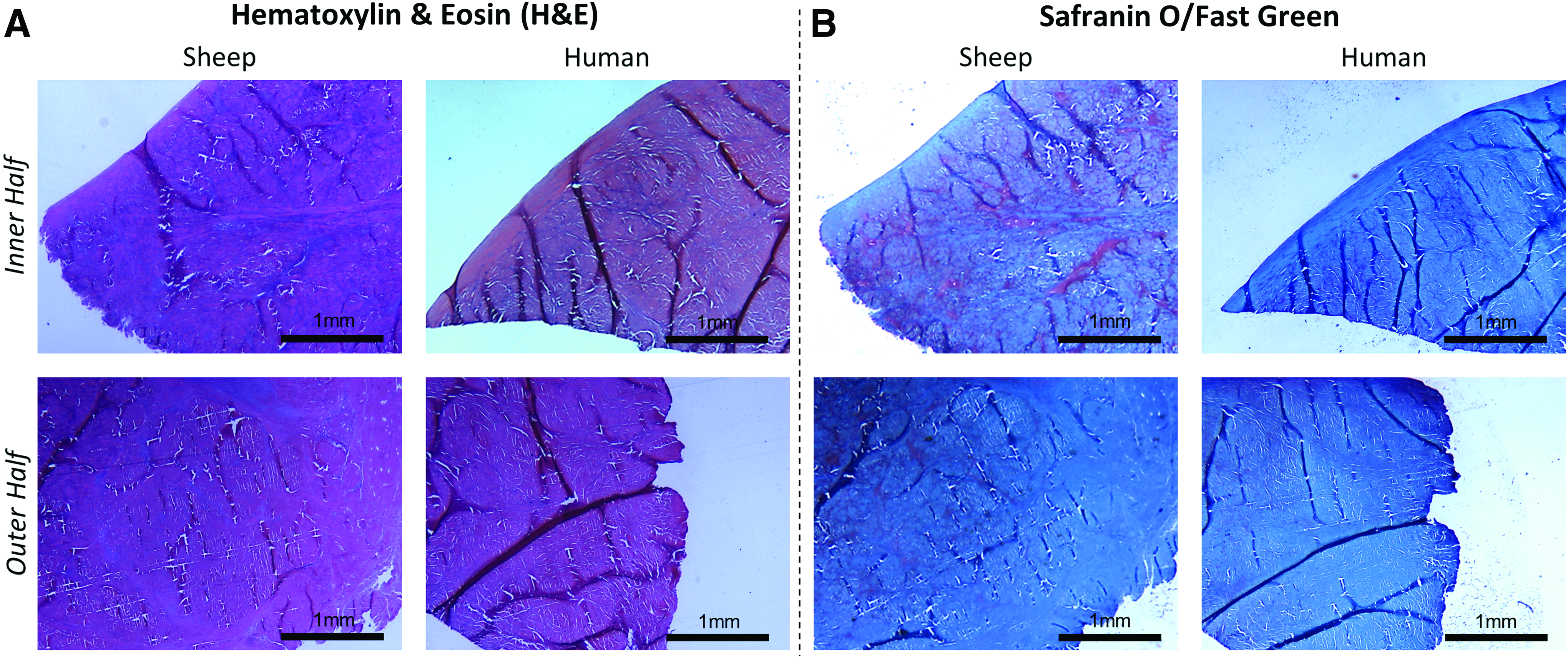
Histological sections of sheep and human menisci stained with
The functional biomechanics of the meniscus in both species are a result of its gross anatomy and ultrastructure. The curvature of the proximal surface conforms well to the femoral condyle and, therefore, effectively redistributes transmitted loads. 51 When axial compressive load is applied from the femur to the tibia, the wedge-shaped meniscal profile displaces a portion of the load radially. To resist extrusion or rupture, circumferentially aligned collagen bundles convert the radial stress into circumferential hoop stresses, transmitted into the tibia through the root attachments. Thus, both compressive and tensile properties are integral to meniscus function in both sheep and humans.
The compressive behavior of the meniscus is well described by Mow's biphasic theory, differentiating the viscoelastic tissue into a fluid phase and solid phase. 52 The solid phase consists of the collagen-proteoglycan matrix and the fluid phase consists of the interstitial fluid found within the solid matrix. 53 When loaded in compression, the interstitial fluid of the meniscus is forced to slowly flow out over time. The frictional drag force of this water displacement and its associated hydraulic pressure are the major mechanism for load support and provide the time-dependent compressive properties of the tissue. 54 The sheep meniscus was found to have the aggregate modulus and permeability most similar to humans, compared to several other animal models (monkey, canine, bovine, and porcine). 26 With regard to tensile properties, we performed circumferential tensile testing (10 mm/min to failure) on the body region of four cadaveric human menisci and compared the tensile stiffness and ultimate tensile load to previously established ovine meniscus values. 17 There was no significant difference in either ultimate load (p = 0.61) or tensile stiffness (p = 0.44). Tensile and compressive mechanical properties of human and sheep menisci are shown in Table 2.
Mean ± SD.
Citations for each value are given in parentheses.
To produce a functional tissue-engineered meniscal scaffold, the initial properties must exhibit comparable compressive and tensile values to the native meniscus to prevent rupture or extrusion in both partial and total implants. These properties are also crucial to provide the cells within the scaffold with the appropriate mechanical cues to differentiate toward the correct phenotypes.
Facility, Budgetary, and Behavioral Considerations
In addition to the anatomical and compositional considerations, other variables exist that further validate the ovine model. Anesthesia equipment, agents, and protocols are mostly similar between humans and many of the large animal models. Early research was performed in the canine model due to the ease of handling, but it has become increasingly unpopular due to ethical concerns regarding terminal research in companion animals. Even though sheep (50–75 kg) are much larger than the commonly used canines (15–30 kg), they remain relatively easy to handle, and intravenous access through the jugular or brachial vein is possible without premedication. The drastically larger size of adult bovine and equine subjects (750–900 kg) requires significant investment in large, specialized surgical tables, holding facilities, and handling equipment. Domestic porcine breeds are relatively inexpensive ($200–500 ea) and routinely available, but they grow extremely quickly and are in the 300–500 kg range at skeletal maturity (18–24 months). Miniature pig (>100 kg at skeletal maturity) and micro-pig breeds are available, but only through specialized vendors. Micro-Yucatan pigs have a slower growth rate through sexual maturity compared to miniature breeds, but the sizes of the breeds converge at skeletal maturity (2–4 years). The availability of these animals can be limited and prices are much higher ($2500–4000). In addition, swine are relatively difficult to handle and restrain, making postoperative care more complicated. Last, the Yucatan miniature swine lacks genetic diversity, raising concerns about the legitimacy of using these animal models. On the other hand, crossbred sheep are readily available and provide good genetic diversity, which is especially important for translational research.
While the caprine model represents an affordable, anatomically accurate alternative to the ovine model, behavioral factors limit its use due to rehabilitation concerns. In human patients, a toe-touch weight bearing recovery period would allow for adequate healing time. Unfortunately, animal models are limited in terms of rehabilitation. Sheep and goats are both quadrupeds, but sheep are grazers, while goats are browsers. Therefore, sheep generally remain on all fours, while foraging, but goats often stand on their hind legs to reach well above their heads. Thus, sheep are much less likely to bear their full weight on the newly operated knee, significantly reducing the likelihood of early damage to meniscal implants. To our knowledge, there has only been one report of using Achilles tenotomy to reduce weight bearing on the surgical leg for a time. 56 However, this has not been repeated, perhaps due to ethical issues, confounded results, or instability during the postoperative period. We see reasonable stability in our sheep within a few days, which allows them to be group housed relatively quickly. The relative expenses, size, ease of handling, and other considerations for various large animal models are depicted in Table 3.
+, easy handling; −, difficult handling.
Surgical Approach and Scaffold Fixation
Human arthroscopic procedure
Meniscal tissue engineering is not well established in humans; so total meniscus implantation techniques should be guided by those developed for allograft transplantation. Arthroscopically assisted procedures for allograft transplantation are well described and thoroughly tested.57,58 Arthroscopy possesses a number of advantages compared with arthrotomy, including decreased operative time, decreased risk of infection, and shortened postoperative recovery times.
40
There are two important considerations for a successful implantation:
(1) Proper visualization of the intraoperative site, allowing for anatomical positioning of the implant. (2) Adequate surgical fixation (either partial or total replacement).
In clinical use, three arthroscopic portals are created, anterior medial, anterior lateral, and posterior medial, to visualize the medial joint compartment. For implant insertion, the anterior-medial portal size is adjusted to the size of the implant, allowing for safe placement of the scaffold into the joint. The joint space may be increased through the utilization of an external joint distractor or the partial release of the MCL. Unfortunately, in sheep, there is limited arthroscopic visualization of the posterior compartment, compounded by the tightness of the joint, which limits access to the meniscus. Although ACL tissue-engineered devices can be implanted arthroscopically in sheep, 59 in our experience, the meniscus cannot be visualized properly; so the only feasible procedure for meniscal implantation in sheep is an open surgical approach.
Ovine arthrotomy procedure
Proper visualization of the meniscus is integral to anatomically position the tissue-engineered scaffold. However, the restoration of kinematics and ligamentous function is also crucial to outcomes, and a balance between access and invasiveness is needed. Two acceptable approaches are a modified medial parapatellar arthrotomy or combined medial and lateral parapatellar arthrotomy. The first technique described by McNickle et al. is the most commonly performed, but requires the MCL to be released. 60 It should be noted that the MCL is the primary stabilizer during swing phase in the sheep. 24 Improper reattachment of the MCL can cause gait disturbances and instability after surgery, and can also lead to synovial and chondral pathologies. Thus, the mechanism of MCL release is extremely important, with three major techniques existing in the tissue engineering literature (Fig. 3). Direct MCL release (Fig. 3A) with subsequent suture repair is less invasive than other release protocols,9,19,61,62 but can deteriorate MCL kinematics, leading to instability with failure rates of 6% found in human ligament reconstruction studies. 63 Epicondylar osteotomy (Fig. 3B), which involves cutting and reattaching bone with the femoral MCL attachment, allows for compartment access to a greater degree, the advantages of rigid bone fixation, preservation of native ligament function, and typically heals well if fixed properly.16,60 A 15 × 15 × 5 mm tissue section (centered around the MCL attachment) is cut with an oscillating bone saw, except for the inferior cut, which must be made with a narrow osteotome to prevent injury to the MCL. The bone block is detached from the femur, allowing for visualization of the medial compartment. Following implantation, the bone block is reduced and fixed using a cortical bone screw. 60 Medial condylectomy (Fig. 3C) provides the greatest access to the meniscus 18 and preserves the native MCL function, but the invasive procedure may result in poor bone healing and disturb cartilage continuity.
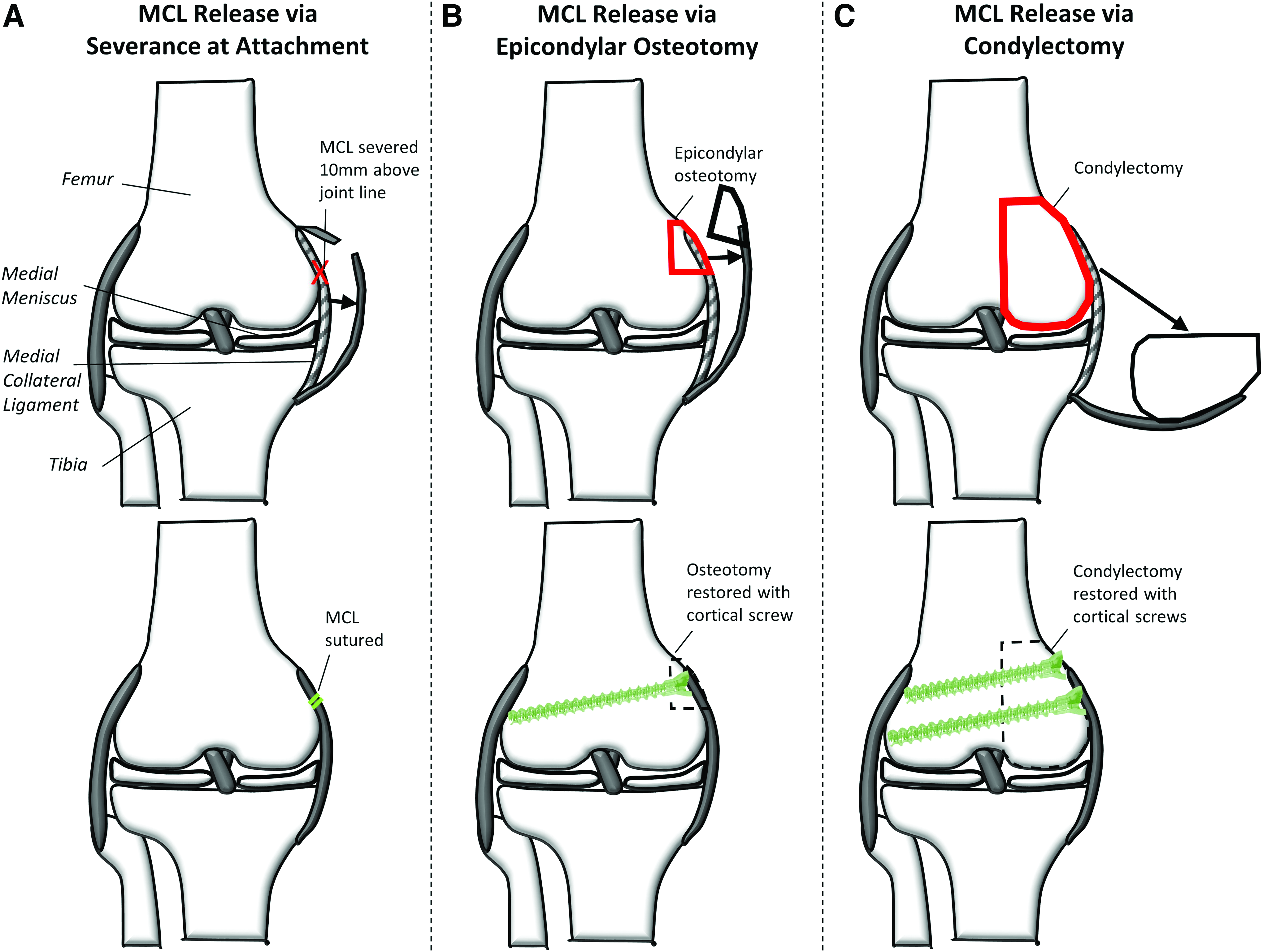
MCL release techniques by
The second surgical technique is the combined medial and lateral parapatellar approach, 18 allowing for better visualization of the posterior compartment and preservation of the MCL. However, this approach is more extensive and it requires an osteotomy of the tibial tuberosity together with distal patellar tendon attachment, increasing the risk of infection and complicating the rehabilitation process. Therefore, the medial parapatellar arthrotomy with epicondylar osteotomy provides the best balance between compartment access, restoration of joint mechanics, and invasiveness. A sham procedure should be utilized as a control group to evaluate changes in the knee resulting from the surgical approach itself.
Surgical fixation: total meniscus replacement
Total meniscal device implantation is modeled after allograft implantation techniques, which involve a total meniscectomy followed by replacement with an appropriately sized graft. The most crucial factor for success of the procedure is the appropriate placement and fixation of the meniscal roots. The fixation should be strong enough to avoid extrusion and restore the ability to dissipate hoop stress. Three fixation techniques have been utilized: suture, bone plug, and bone trough. In suture fixation, the graft is cut at the root attachment sites, the attachment sites are sutured, and the sutures are pulled through transosseous tunnels and secured using a cancellous bone screw. 64 Alternatively, in bone plug and bone trough fixation, the allograft is harvested with the attachment sites, allowing for rigid bone-to-bone fixation. Several studies have shown that bone fixation of medial meniscal allografts better restores contact mechanics and protects from extrusion compared to suture fixation.58,65
With regard to tissue engineering devices, some groups have attempted to suture the implant to the meniscotibial ligaments after total meniscectomy with multiple instances of extrusion and failure. 19 Others have passed sutures through intraosseous tunnels and either tied the ends together around the tibia or secured with an endobutton, with limited success.9,11,16 Merriam et al. described a unique technique for the implant fixation, where extended tails were pulled through intraosseous tunnels and fixed using interference screws. 66 This method of fixation resulted in strong adherence and the prevention of extrusion, likely due to increased stiffness and healing within the bone tunnels. Thus, we recommend total meniscus replacement scaffolds be fixed through bone tunnels (Fig. 4A) to maximize hoop stress function and minimize extrusion.

Total and partial meniscus fixation strategies.
Partial meniscus fixation
For partial meniscal scaffolds, suture fixation has been widely utilized and has shown to be clinically adequate in humans. The arthroscopic procedures following partial meniscectomy for implanting collagen meniscus implant and Actifit include the debridement of the meniscus to the red-red zone, measurement of the circumference of the meniscectomized tissue, implant trimming to approximately the same geometry, placement of the implant into the defect using a press-fit technique, and fixation to the remaining meniscus using vertical mattress sutures.67,68 Tissue-engineered partial meniscus implants should be similarly inserted into the defect and fixed.62,69 Sutures should connect the implant to the meniscal rim as well as to the anterior and posterior meniscal remnants (Fig. 4B). Typically, 2-0 Ethibond vertical mattress sutures are utilized and provide adequate biomechanical properties.70,71 However, if resorbable sutures are desired, 2-0 Vicryl and 0 PDS II can provide suitable fixation. 71 Adequate fixation is required to prevent separation of the implant from the remaining meniscus, ensuring proper force transmission and protection from cartilage damage.
Postoperative Care
Postoperative care remains a hurdle in all forms of orthopedic tissue engineering. There have been a few attempts by various investigators to prevent full weight bearing in sheep following orthopedic surgery. The use of trapeze-style slings to support much of the animals' BW following PCL replacement was found to adversely affect the normal healing process. 72 A plaster cast can be used to temporarily immobilize the surgical leg, making the leg stable enough to prevent full weight bearing during the postoperative period. 73 While both slings 9 and casts19,61 have been used in meniscus tissue engineering as well, these techniques require significantly increased costs and unpredictable risks of falls or other injuries. Achilles tenotomy has also been investigated to provide a nonweight bearing period, but in addition to ethical concerns, researchers have proven it to be ineffective. 74 Most researchers simply restrict movement by singly housing the animals in small cages (4 × 4 ft) for up to 1 week.18,66,75 Ideally, there should be a physical barrier, such as a grating or set of bars that allows visual and even “nose-touch” communication between animals to prevent anxiety. Following ∼3–5 days, at which point animals achieve slight weight bearing, pair housing and group housing in larger spaces are recommended as healing permits.
Evaluation of Implant Efficacy
Toward the standardization of the ovine model for meniscus tissue engineering studies, in addition to the implantation technique and surgical fixation, we recommend a battery of functional evaluation techniques to determine the efficacy of the implant. This section details, based on the literature and our experience, a standardization of meniscus and joint assessment protocols, with recommendations for which tests are considered mandatory (must be done), highly recommended (should be done), and suggested (could be done) (Table 4). Specifically, emphasis will be placed on mechanical and biological properties of the explanted neo-meniscus tissue, as well as quality of the articular cartilage and synovium. It is also important to note that the identical battery of tests should be performed on the contralateral, nonoperated knee for comparison.
GAG, glycosaminoglycan; H&E, hematoxylin & eosin; MRI, magnetic resonance imaging; PR, Picrosirius Red; OARSI, Osteoarthritis Research Society International; SafO, Safranin O.
Joint analysis and gross observations
Before sacrifice and retrieval of the animal joints, there are several analyses that can be performed on live animals. First, gait analysis can give great insight into weight bearing,76,77 using pressure-sensitive walkways to determine lameness or favoring. Moreover, imaging modalities can provide a nondestructive evaluation method of the knee joint. Magnetic resonance imaging offers visualization of the joint space,9,16 allowing the observation of meniscal, cartilaginous, and ligamentous pathologies. However, this technology is both expensive and not readily available, making their use suggested, but not required. On the other hand, X-ray is less sensitive and specific for detection of intra-articular pathologies, but is relatively inexpensive and more available. X-ray allows for the indirect observation of cartilage damage through the evaluation of the joint space narrowing, osteophyte formation, and changes in subchondral bone quality by comparing experimental time points to time zero. In the event that gait analysis and imaging are not possible, joints should be evaluated qualitatively against nonoperated contralateral knees for flexion, crepitus, and stability. 78
Immediately after the animal is sacrificed, and just before knee dissection, synovial fluid can be collected and tested for particulate wear debris and various inflammatory cytokines (e.g., IL-1, IL-6, TNF-α, and IFN-λ). Elevated levels of these cytokines may be indicative of joint damage and osteoarthritis that often result from improper meniscal function.79,80 After the operative knee joint is opened, gross observations must be made of the synovium, the cartilage, bone, and the meniscal implant site. Photographs of these sites can be used to document the state of the knee joint, and to quantify the dimensions of the neo-meniscus tissue, as detailed in Table 1. An easily attainable parameter not commonly evaluated is percent coverage,81,82 the meniscal area divided by the underlying tibial plateau area, using an image processing software such as MATLAB or ImageJ. Percent coverage is important to characterize the size and shape of explant tissue, for both partial and total meniscus replacements that may remain anatomically intact or may extrude, shrink, degrade, or wear with time.
Mechanical properties of explants
Before the mandatory compressive and tensile testing, we recommend performing nondestructive contact stress analyses on explants. The contact profile (peak stress, average stress, and contact area) on the underlying cartilage can be determined and compared among various conditions (explants, contralateral control, meniscectomy, allograft, etc.), providing functional insight into the explants' in vivo load-distributing capabilities.83,84 This can be accomplished with pressure-sensitive strips placed under the meniscus in conjunction with joint movement simulation, when available, or through uniaxial loading of the knee joint at various angles.85,86
To determine compressive mechanical properties, both instantaneous and time-dependent (stress relaxation or creep) analysis must be performed, because the meniscus is a viscoelastic tissue, like cartilage, and the FDA cartilage guidance document 28 and associated ASTM standards 87 mandate these characterizations. Confined creep testing with Mow's biphasic theory 52 allows for calculation of aggregate modulus and permeability. Likewise, the Kelvin–Voigt model can be used on creep data to obtain a Young's modulus and viscosity for further characterization of viscoelastic properties. 49 Both moduli relate to the ability of the ECM to resist loads, while the permeability and viscosity relate to time-dependent fluid flow, an integral function of the meniscus. Data from these biphasic models may demonstrate a large degree of variability; so we highly recommend that compressive testing be performed on multiple samples per explant. In addition, as multiple studies have shown differences between anterior, central, and posterior regions, samples must be taken from each region to account for this effect.17,49
While investigators routinely obtain compressive mechanical properties, tensile testing is very rarely performed in meniscus tissue engineering trials. The ability to resist circumferential hoop stresses is integral to the function of both total and partial meniscus replacements. Unfortunately, tensile testing of entire explants limits their use in other assays; thus, taking circumferential, dog bone-shaped, or expanded-tab segments (∼1 mm thickness) of meniscus tissue provides a suitable alternative.49,88,89 Dimensions should be obtained to normalize the structural properties (ultimate tensile load and stiffness) into material properties (ultimate tensile strength and elastic modulus). These parameters directly determine the ability of an explant to remain intact and resist extrusion. For partial meniscus replacement, additional samples should be taken in the radial direction to allow for quantitative analysis of integration mechanics between the explant and remaining meniscus, in addition to semiquantitative histological observations.61,62
Explant biology
In addition to mechanical analyses, tissue-engineered devices must be evaluated biologically through histological and immunostaining techniques to determine their ability to promote neo-meniscus tissue formation. These methods are typically performed on radial slices; however, researchers should also analyze circumferential sections when attempting to analyze circumferential alignment of fibers (with hematoxylin & eosin [H&E], Picrosirius Red, or confocal microscopy). 89 For both radial and circumferential analyses, H&E is the most widely utilized histological stain, providing necessary insight into cellular concentration and morphology, ECM deposition and organization, inflammatory response, and vascularity.18,62,90–92 Picrosirius Red is also highly recommended, allowing for visualization of collagen structure, and polarized light can be utilized to measure fiber alignment.18,89,90 Safranin O/Fast Green25,92,93 or Toluidine blue staining90,91 should be used to visualize proteoglycan content, integral to the osmotic properties of the meniscus, and assess any calcification or cyst formation. 94 Last, immunofluorescence or immunohistochemistry is highly recommended for determining the spatial distribution of type I and II collagen.18,90,92 The above staining on slices should focus on variations between not only the inner and outer zones but also regional variations that have been noted in previous studies.17,47 Partial meniscus replacements should also be evaluated for integration. The integration analysis may be performed on radial H&E sections, typically accompanied by a semiquantitative scoring system.95,96 Last, biochemical content analysis is recommended, specifically to characterize collagen and GAG content that are typically lacking initially in synthetic meniscus tissue engineering scaffolds.17,92
Analysis of joint cartilage
The most important assessment of the efficacy of a meniscus implant relates to its ability to protect the joint cartilage from deterioration. Macroscopically, the articular surfaces (femoral condyle and tibial plateau) should be analyzed for location and area of damage, by using the International Cartilage Repair Society mapping scheme. Using the same mapping scheme, cartilage indentation testing could be performed on the femoral condyle with a relatively inexpensive Shore A durometer, 97 to nondestructively evaluate the hardness of the cartilage. In addition, India ink staining is a common method to stain for gross cartilage degradation11,98; however, this may complicate subsequent histological techniques for cartilage analysis. The remainder of the analyses follows the Osteoarthritis Research Society International (OARSI) histopathology initiative for assessment of osteoarthritis in sheep and goats, with three independent observers for each analysis. 99 The four articular surfaces of the knee (medial and lateral, femoral condyle, and tibial plateau) should be graded macroscopically for gross articular damage and osteophyte development. Next, three medial-lateral slices (anterior, central, and posterior) of the femoral condyle should be taken and stained with either Safranin O/Fast Green9,11,17 or Toluidine blue. 90 The resulting sections should be divided into three regions (medial, central, and lateral), to obtain nine images per condyle. Low and high magnification images of each must be randomized and graded. The OARSI cartilage microscopy score 99 (also known as a modified Mankin) provides a semiquantitative scoring system and is based on structure, chondrocyte density, cell cloning, proteoglycan stain, and tidemark. This scoring scheme (0–25) allows for better differentiation of damage than the traditionally used Mankin score (0–14). 100 The histology and scoring of joint cartilage provide an in-depth analysis to the cartilage health that is not readily apparent macroscopically. The health of the cartilage is directly related to the function of any meniscus replacement scaffold, and thus must be thoroughly evaluated.
Additional understanding of joint health can be obtained by analysis of the synovium.61,91,101 Specifically, the synovium can be analyzed macroscopically for discoloration, fibrillation, and vascularity, and microscopically with H&E for particulate wear debris, intimal hyperplasia, inflammatory cell infiltration, subintimal fibrosis, and vascularity. 99
Other experimental considerations
The previous section provided a battery of tests, including mandatory, highly recommended, and suggested analyses, summarized in Table 4. These analyses can be applied to meniscus tissue engineering in the ovine model and other large animal studies. Some overall considerations for the ovine model are sacrifice time points, experimental conditions, and controls. The more commonly used short-term time points are 12 weeks9,18,102 and 24 weeks,11,47,102 and long-term time points include 12 months17,19 and 24 months. 11 In most large animal meniscus studies, animals do not achieve full weight-bearing until 4–6 weeks postoperatively9,66; thus, at least 12 weeks, it is recommended to allow sufficient time for the meniscus device to bear significant mechanical loads. Moreover, due to synthetic polymer mechanical strength loss that typically occurs between 12 and 24 weeks,47,103,104 the intermediate time point of 24 weeks is recommended. Long-term time points of 1 year and beyond are also required to determine efficacy after the implant is largely degraded and tissue has remodeled, and these time points are similar to follow-ups in clinical trials.105,106 Thus, future large animal work should be conducted at those short-term, intermediate term, and long-term time points to allow comparison of data between different research groups.
In addition to experimental groups, there are three possible control groups (nonoperated contralateral, meniscectomy, and sham surgery) that should be analyzed. The contralateral joints of experimental animals should serve as positive controls for all mechanical, histological, and joint health analyses. Total or partial meniscectomy (depending on the type of implant studied) can be performed as a negative control,11,66 as it is the current clinical gold standard. Last, as mentioned previously, sham procedures should be included to characterize any adverse effects of the arthrotomy and MCL release surgical procedures.9,21
In large animal studies, the number of animals per group (per time point) is often controlled by budgetary and institutional limitations and, unfortunately, may not be consistent with n values recommended by statistical analyses. In previous ovine studies, this number has ranged from three to eight per experimental group,9,16,47 whereas the meniscectomy and sham groups typically contain less animals, usually two.16,61,66 We recommend at least six experimental and two meniscectomy animals at each time point with two sham animals at the longest time point. Given the common constraints of a limited budget or a fixed number of animals in a study, the lower number of meniscectomy and sham animals allows for increased number of animals in the experimental group.
Conclusions
Numerous meniscus tissue engineering studies have been published in the past 10 years, with a variety of animal models used. The purpose of this review was to establish the ovine model as an appropriate model for meniscus tissue engineering and give guidelines for implantation and evaluation. The ovine model has anatomical and compositional similarities to humans, serving as a scaled-down version of the human knee. The few differences in anatomy, most notably the asymmetrical shape in humans, can be addressed during scaffold fabrication. Ligamentous attachments are similar, although proximity to the MCL and tibial cortex differences need to be addressed during implantation. Compositionally, sheep and human menisci are extremely similar, with the one major difference being GAG content. For this reason, experimental analysis of GAG content should include contralateral meniscus controls. With regard to both compressive and tensile biomechanics, the sheep meniscus was shown to be nearly identical to the human meniscus, further validating the ovine model for meniscus research.
Surgical approaches were also discussed, recommending a medial parapatellar approach with epicondylar osteotomy as a balance between joint invasiveness and return of MCL stability. Fixation method is also integral, with the suggestion of interosseous fixation for total meniscus replacement and suture fixation to the remaining meniscal rim for partial meniscus replacement. Considerations of expenses, facilities, and handling concluded that the ovine model provides one, if not the best, option. Postoperative management was also found to vary between previous research studies, and should be considered in the experimental design. Finally, we provided comprehensive strategies to determine implant efficacy to further advance the field of meniscus tissue engineering. Joint analyses before sacrifice, including gait analysis and imaging, can provide insight into joint function. The explanted neo-meniscus tissue must be characterized both mechanically and biologically, in different orientations and regions. Last, cartilage should be evaluated both macroscopically and histologically, with a blinded scoring system.
Currently, there is no FDA regulatory guidance document for preclinical evaluation, surgical implantation studies, or efficacy testing for meniscus implants. This review can serve as a template for future standardization of the ovine surgical model and the battery of analytical tests required to determine the efficacy of tissue-engineered meniscus implants in this large animal model.
Footnotes
Disclosure Statement
The meniscus device described in this manuscript has three issued patents (US 8,623,085; US 9,078,756 B2; US 9,579,212 B2). The technology has been licensed for product development (MeniscoFix, NovoPedics, Inc.). J.M.P. serves as a consultant for NovoPedics. C.J.G. serves as interim president and owns stock in NovoPedics. M.G.D. serves as interim secretary and treasurer, and owns stock in NovoPedics.