
Abstract
Delayed wound healing and the potentially resulting chronic wounds are a challenging clinical problem. Available therapeutic strategies are limited in both number and efficacy. For developing and establishing novel treatment approaches appropriate clinically relevant animal models are essential. The aim of the study was to establish a reliable and reproducible delayed wound healing model, which simulates the clinical scenario of compromised vascular tissue perfusion (hypoxia/ischemia). Therefore a standard rodent ischemic flap model was modified by challenging the tissue with ascending degrees of ischemia using different surgical approaches (minimal, mild, moderate, and severe ischemic invasive approach). Then a full-thickness circular wound was excised in both the non-/hypoperfused flap area and in the normally perfused contralateral region serving as an internal control. Wound healing progress was compared. Superficial tissue perfusion was measured by Laser Doppler imaging technique, which showed persistent ischemia in the moderate and severe invasive surgical approaches 7 days after wounding. Wound closure assessed by planimetric analysis occurred significantly slower in the ischemic wounds compared to the contralateral nonischemic wounds in the moderate invasive approach. Histologic evaluations in this approach showed signs of tissue necrosis and impaired angiogenesis in the ischemic wounds. Therefore, it can be concluded that this clinically relevant animal model is suitable to study mechanism in ischemia-impaired wound healing. Furthermore, it allows evaluating the efficacy of therapeutic strategies for impaired wound healing and comparing the results with an internal control wound.
Introduction
I
A broad spectrum of experimental animal models focus either on acute wound healing 10 or on impaired wound healing using different model setups such as chronic pressure ulcer models,11–14 metabolic pathologies, including but not limited to diabetic wound healing models, 15 immunosuppressive strategies applying glucocorticoids, radiation, 16 or chemotherapeutics, 17 blood vessel ligation flap models, 6 rat dorsal flap models, 18 rabbit ear excision models, 19 and hind limb models. 20 However, most models are complex and demanding in the surgical technique, often time consuming or necessitate a high number of control animals. In face of the multiplicity of experimental models, there are only a few roughly recapitulating the clinical hallmarks of delayed or chronic wound healing. Requirements to an optimal experimental in vivo setup to best converge the clinical features of chronic wounds are discussed to involve disturbances in oxygenation, venous insufficiency, neuropathy, the microbiota of the wound, patients' and wounds' age, the immune system, obesity, systemic metabolic diseases, and the anatomical wound location (partly reviewed in Ref. 21 ). However, considering the complexity, as well as the heterogeneity of delayed or chronic wounds in humans, none of the mentioned models is efficient to completely mimic each of the clinical settings. Aggravating this intricacy in any way, application of the relevant therapy is often found to be difficult in these iatrogenic induced wounds.
The present study aimed at establishing a reliable, reproducible, and simple delayed wound healing model caused by insufficiency in arterial, venous, and nervous supply. The application of different therapeutic topical approaches should be feasible during the wound healing process. A standard epigastric flap model was modified by inducing ischemia in an ascending manner by different surgical approaches (minimal, mild, moderate, and severe). Two circular wounds within the flap were excised, thus creating both an ischemic and a contralateral nonischemic wound. Wound healing progress was investigated in ischemia disturbed wounds in comparison to the nonischemic contralateral wounds (corresponds to an internal control) to elaborate the appropriate degree of ischemia to accomplish delayed wound healing, but avoiding tissue necrosis.
Materials and Methods
Establishing of an ischemia disturbed excisional wound healing model
The local ethics committee on animal experiments, Vienna, Austria, approved all experimental in vivo procedures before study initiation. The study individuals were treated according to the policies, procedures, and responsibilities for the care and use of laboratory animals within the Ludwig Boltzmann Institute for Experimental and Clinical Traumatology, Vienna, Austria. Animals were caged in pairs in stainless steel type 4 cages with an enriched environment (nestlets, wooden sticks) in open housing conditions at a mean room temperature of 18°C ± 2°C with 50% ± 10% humidity on a 12-h light/12-h dark cycle. All animals (n = 13) had water ad libitum and free dietary access. For preoperative preparation, male Sprague-Dawley rats weighing 300–350 g were initially anesthetized in an inhalation box provided with isoflurane (2.5 Vol%), oxygen (300 mL/min), and air (3 L/min). Anesthesia was maintained by intraperitoneal injection of 110 mg/kg ketamine hydrochloride (Pharmacia & Upjohn, Germany) and 12 mg/kg xylazine (Bayer, Leverkusen, Germany). Thereafter, the abdominal region was shaved and depilated in all animals irrespective of surgical intervention. Surgery was done using aseptic technique.
Optimization of ischemia by ascending degree of surgical invasiveness
The study aimed at developing an ischemia-impaired wound healing model with one circular wound in an ischemic insufficiently perfused, but not necrotic, area, as well as an internal control in a regularly perfused area in the same individual's abdomen. In all experiments the unilateral inferior epigastric bundle was ligated to induce primary ischemia. To optimize the model for our purposes, different surgical procedures with an ascending degree of invasiveness and consequently severity of secondary ischemia were performed (Fig. 1). Thereafter, standardized circular wounds (diameter of 1.5 cm) were excised within the ischemic and the vital area comprising skin and panniculus carnosus muscle, but leaving the underlying fascia intact. All different described experimental approaches were done in different animals.

Illustration of the surgical approaches in the experimental setup. (1) An inguinal incision (1 cm) was performed in the minimal invasive approach followed by a ligation of the unilateral inferior epigastric bundle. (2) Bi-horizontal incisions were made in the mild invasive approach, and the inferior epigastric bundle was ligated by the inferior incision. The transversal incisions should avoid collateral vessel growth (cranial and caudal lines). (3) An entire abdominal flap (severe invasive approach) was elevated. The unilateral inferior epigastric bundle was ligated before suturing the flap back (caudal, cranial and lateral lines). (4) In the moderate invasive approach the same procedure was done as in (3) but leaving the caudal side intact. *Two circular wounds, including epidermis and dermis but leaving the muscular fascia intact, were created in the ischemic and vital area in all experiments.
Model optimization
Minimal invasive approach
In a first experiment (n = 2), an incision of 1 cm was created in the left or right inguinal region according to a randomization protocol. The branch of the inferior epigastric bundle, including artery, vein, and nerve, was prepared by blunt surgical technique. After ligation of the inferior epigastric bundle with two single knot sutures the bundle was dissected between these sutures to assure a completely blocked blood flow and to avoid reanastomosis. Thus, a hypoperfused area of the corresponding abdominal side occurred. The incision was closed with interrupted sutures. Then, the circular wounds were created in the hypoperfused area, as well as in the contralateral nonischemic region (Fig. 1/1).
Mild invasive approach
Additional to the procedure in the minimal invasive approach, two horizontal 8 cm incisions were made caudally (inguinal) and cranially (xiphoid) until the muscle fascia level in two further animals. This excludes perfusion from the collateral vessels from proximal and distal, hence increasing the degree of hypoxia in the created wound area. Incisions were closed using interrupted sutures. The circular wounds were performed as described above (Fig. 1/2).
Moderate invasive approach
In the third experiment (n = 7), a standard abdominal flap measuring 8 × 8 cm was created but leaving the caudal base intact. In brief, a horizontal cranial incision (xiphoid) and two longitudinal lateral incisions (at the distinct conversion from the thin ventral to the coarse dorsal skin) were made. The flap was then harvested along the abdominal muscle layer from proximal to distal. The inferior epigastric bundle was ligated in the same manner as in the other experiments. The flap was then sutured back to its anatomical configuration, and circular excision wounds were created accordingly (Fig. 1/4).
Severe invasive approach
In this study, the same procedure in two additional animals was performed as done for the moderate invasive approach, but including the caudal base. Finally, an entire abdominal flap was harvested supplied by an unilateral epigastric bundle. After suturing the abdominal flap, the excisional wounds were created according to the standard protocol (Fig. 1/3).
Analgesic regimen and postsurgical treatment
As an analgesic treatment, rats received 1.25 mg/kg BW butorphanol and 0.15 mg/kg BW meloxicam 5 mg/mL subcutaneously (s.c.) on the day of surgery and on the three consecutive post-OP days. Perioperatively, animals received 10 mL Ringer solution s.c. for fluid resuscitation. At day 7 post OP the animals were euthanized by an intracardial overdose of barbiturate (Thiopental®, 150 mg/kg BW).
All excision wounds irrespective of group allocation were covered with a transparent film dressing (Opsite, Smith and Nephew, United Kingdom) and fixed with a second dressing (Fixomull-stretch, Beiersdorf, Germany). Bandages were changed on days 1 and 3 after wound creation or replaced when necessary. For this procedure animals were initially anesthetized in an inhalation box provided with isoflurane (2.5 Vol%), oxygen (300 mL/min), and air (3 L/min) and maintained by inhalation mask anesthesia with isoflurane (1.5 Vol%), oxygen (150 mL/min), and air (1.5 L/min).
Tissue perfusion measurement
The Laser Doppler imaging (LDI) (Moor Instruments Ltd., Devon, United Kingdom) system was used to evaluate flap and excision wound perfusion. A two-dimensional image of tissue perfusion was created by scanning the rat abdominal skin by a low-intensity laser light beam (2 mW, wavelength 632.8 nm). The change in laser frequency by moving blood cells was measured. The color-coded image represents the perfusion of the scanned area with blue areas reflecting low perfusion and green, yellow, or red reflecting ascending perfusion.
The abdominal skin was divided into three distinct areas: a vital area with the intact epigastric bundle, an ischemic area with the ligated epigastric bundle, and a borderline zone between the abovementioned areas. These areas were marked on the abdominal flap before measurements. Wounds were located in the vital and ischemic areas. The individual abdomen was scanned preoperatively, postoperatively, and at days 1, 3, and 7 postoperatively. The color-coded image was then divided according to the marked areas, and the perfusion of each area was measured using the measurement software tool provided with the LDI system (Moor Instruments Ltd.). Scans in the vital area were set to 100%, and the scans in the ischemic area were expressed as percentage of the vital area.
Planimetrical analysis
Planimetric analysis was performed to measure the wound size at different time points and to follow the rate of wound closure to compare wound healing progress between the vital and ischemic area. Excision wounds were traced on a transparent acrylic sheet postsurgery and at day 1, 3, and 7. The sheets were photographed and wound size was analyzed using a planimetric software tool (Lucia G1, Version 4.8; Laboratory Imaging Ltd., Czech Republic). The planimetric results were referred to the total postoperative wound surface area ( = 100%) and expressed as percentage.
Histological analysis and immunohistochemical analysis
Histological analysis was performed to evaluate ischemic and control nonischemic healing on a cellular level. At day 7 postOP the animals were euthanized in deep anesthesia by an intracardial overdose of barbiturate (Nembutal®, 150 mg/kg bodyweight). After animals were euthanized the entire wound, including the underlying muscle, was excised. The tissue was fixed in 4% formaldehyde for 24 h, passed through an ascending ethanol series (50%, 70%), and embedded in paraffin. For standard histology, sections were cut and stained with hematoxylin and eosin (H&E) using standard techniques.
Immunohistochemical staining of smooth muscle actin (SMA) was used to visualize mature functional vessels. Tissue was cut in 1.5 μm thick tissue sections. Slides were warmed to 60°C for 30 min and then deparaffinized by washing with xylene twice for 10 min, with ethanol in increasing concentrations (50%, 70%, 99%, and 100%) for 5 min each, and finally with phosphate-buffered saline (PBS) buffer for 2 min. Pronase type XXIV (Sigma Chemicals, MN) 0.1% in PBS buffer was used for pretreatment of slides for 10 min and endogenous peroxidase (1% H2O2 in methanol) for 15 to 30 min, both at room temperature. Primary SMA antibodies (mouse anti-human; Dako A/S, Denmark), diluted 1:2000 in antibody reagent solution (Dako A/S), were incubated for 60 min at room temperature. Secondary antibodies [HRP mouse (ENV); ChemMate Dako Envision, Denmark] were added and incubated for 30 min at room temperature. Reaction with detection substrate AEC chromogen (Dako A/S) was carried out for 5 min and then stopped in PBS.
Statistical analysis
Analysis of variance with Bonferroni's t-test was used to compare the data between the groups using Prism 5.01 software (GraphPad Software). Data are expressed as mean ± SD. p-Values of <0.05 were considered to indicate statistical significance. Statistical analysis has only been done in the moderate invasive approach. Due to ethical issues we did not perform more than two surgeries on animals in the minimal, mild, and severe group, as we were already able to see insufficient results on that basis.
Results
Concomitant increased compromised tissue perfusion with surgical invasiveness assessed by LDI
LDI was performed to evaluate flap perfusion and to reveal ischemia in the ligated area (Figs. 2 and 3).
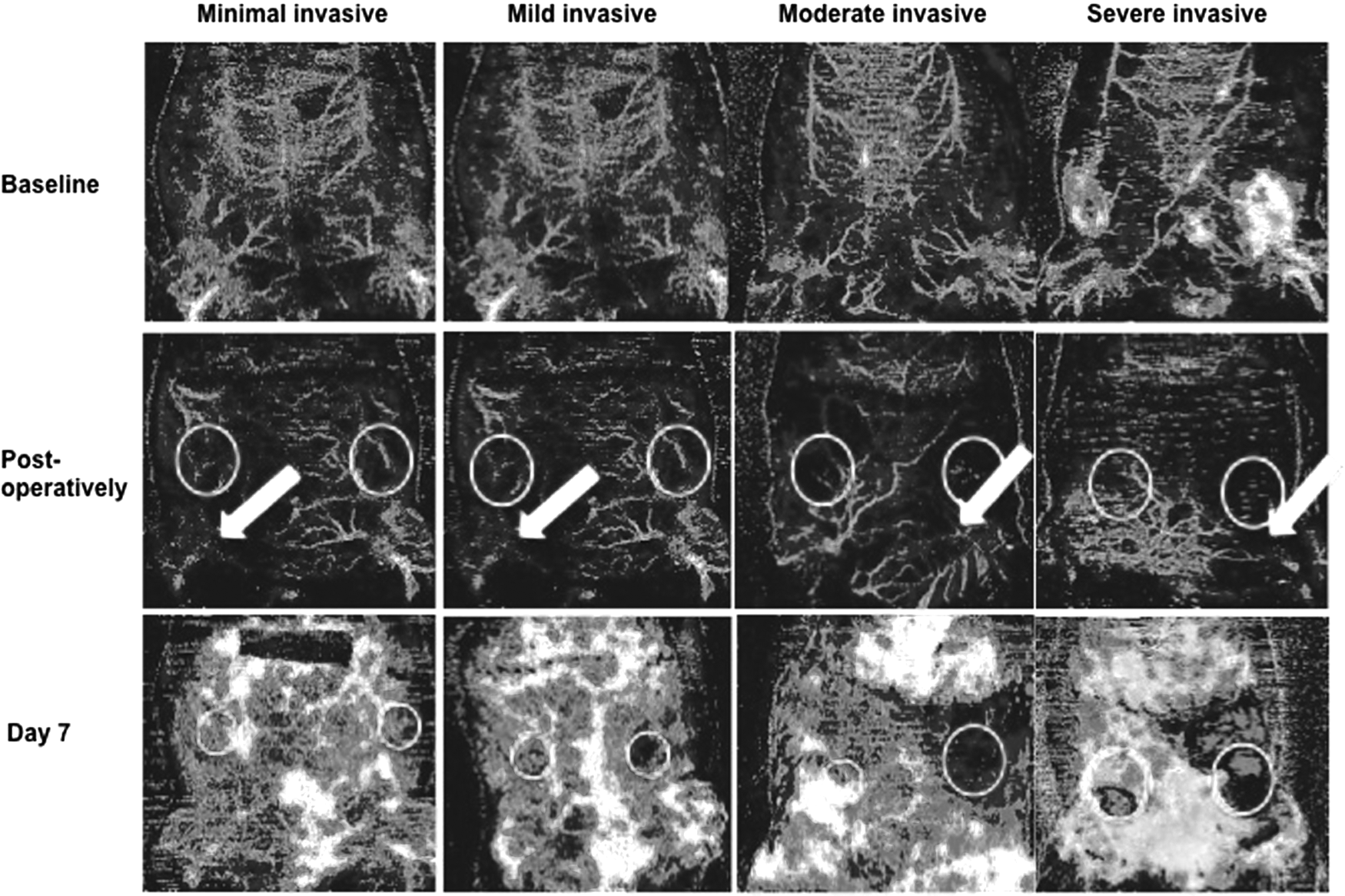
Representative Laser Doppler images at different time points showing tissue perfusion. Light colors indicate well to good perfusion, while regions colored dark colors reflect low perfusion. Circles indicate location of excisional wounds, arrows indicate ligation side. Minimal invasive approach: Ligation of the right inferior epigastric bundle led to initial lower perfusion, but equal perfusion after 7 days compared to the contralateral nonischemic side. Mild invasive approach: Ligation of the right inferior epigastric bundle with additional bi-horizontal incisions led to lower perfusion in the ischemic area postoperatively but again similar perfusion after 7 days compared to the contralateral nonischemic area. Moderate invasive approach: By elevating an abdominal flap, ligating one inferior epigastric bundle (left) and leaving the caudal side intact compromised perfusion of the ligated wound area achieved over 7 days. Severe invasive approach: In the most invasive experiment the entire flap was harvested leaving only an unilateral epigastric bundle intact (left); severe persistent ischemia was observed leading to extended tissue necrosis. White areas in the day 7 image correlate with green, yellow, and red color in the background.
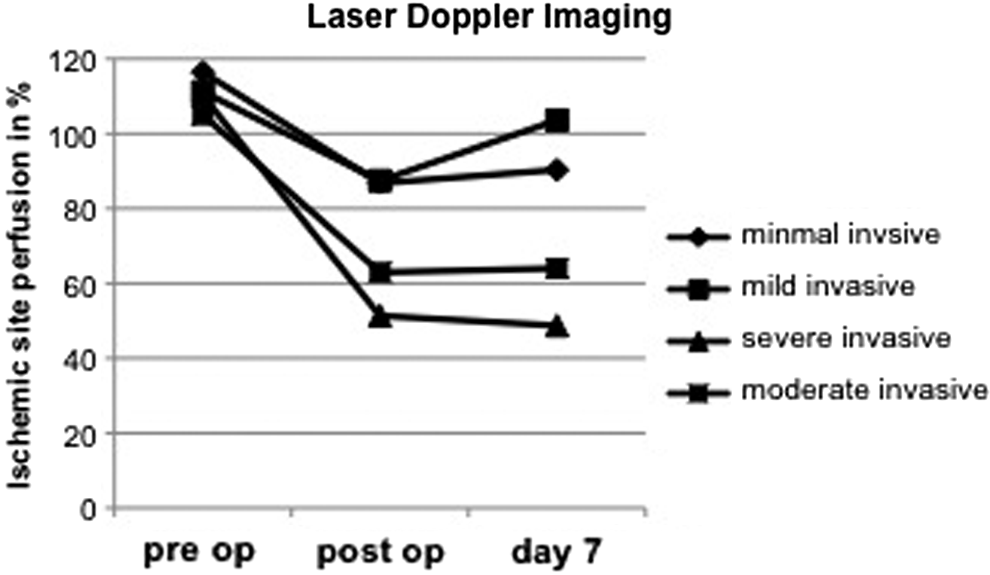
Laser Doppler imaging: perfusion of the ischemic area compared to the nonischemic area in percent. Pre op = before ligation, post op = after ligation, day 7 = after 7 days. Postoperatively and on day 7 we found lowest perfusion in the severe approach followed by the moderate approach. Minimal and mild approaches show insufficient disturbance in blood flow for decreased wound healing. Interestingly, the mild approach shows a slight increase of perfusion on day 7.
Minimal and mild invasive approach
The minimal experimental setup led to an initial lower perfusion in the corresponding hypoxia challenged area (116% perfusion before ligation and 86% thereafter), but insufficient differences in perfusion between ischemic and vital area in the follow-up (90% after 7 days).
Using the mild surgical approach the perfusion showed an initial ischemia in the ligated area (before and after ligation, 111% and 87%, respectively), but insufficient ischemia in the follow-up (103% after 7 days).
Moderate invasive approach
All ischemic areas had lower perfusion compared to the vital contralateral areas. Before ligation perfusion in the later ischemic area was 104.9% ± 7.3% compared to contralateral perfusion. After ligation the LDI value in the ischemic area was 62.9% ± 2.6% compared to nonischemic vital area. Over 7 days insufficient perfusion persisted in the ischemic area and remained at 64% ± 9.9% compared to the contralateral nonischemic area.
Severe invasive approach
In the most invasive experiment the entire flap was harvested leaving only an unilateral epigastric bundle intact. Severe persistent ischemia was observed over the entire study period, thus leading to extended macroscopic tissue necrosis with black appearance and hairless in conjunction with induration and loss of skin elasticity. Values of perfusion were 110% before ligation, 51% after the ischemic impact, and 48% after 7 days following ischemia.
Planimetrical analysis showed disturbed ischemic excisional wound healing
Wound size was evaluated on day 1, 3, and 7 postoperatively and expressed as percentage of the total postoperative wound surface area (Figs. 4 and 5).
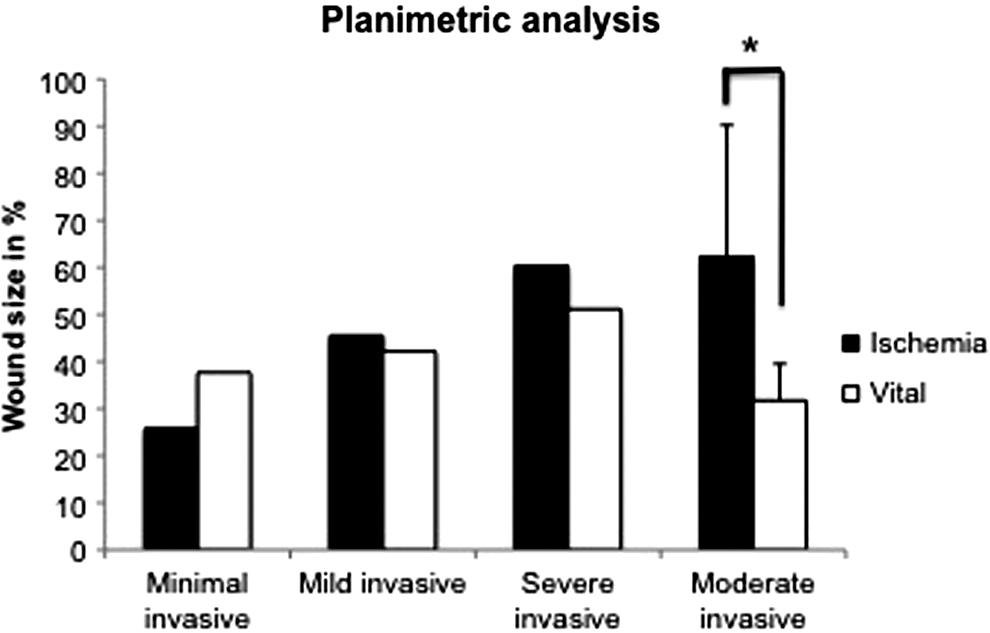
Wound size assessed by planimetric analyses on day 7 postwounding. No clinical impairment of healing could be detected between ligated and contralateral nonligated wound areas after 7 days in the minimal and mild approach. The severe approach resulted in larger wounds in the ligated ischemic and nonischemic area compared to the minimal and mild invasive approach on day 7 with similar wound sizes in both areas. Significantly larger wound size was found in the ischemic area compared to the vital area after 7 days (*p < 0.05; mean ± SD; n = 7) in the moderate approach.
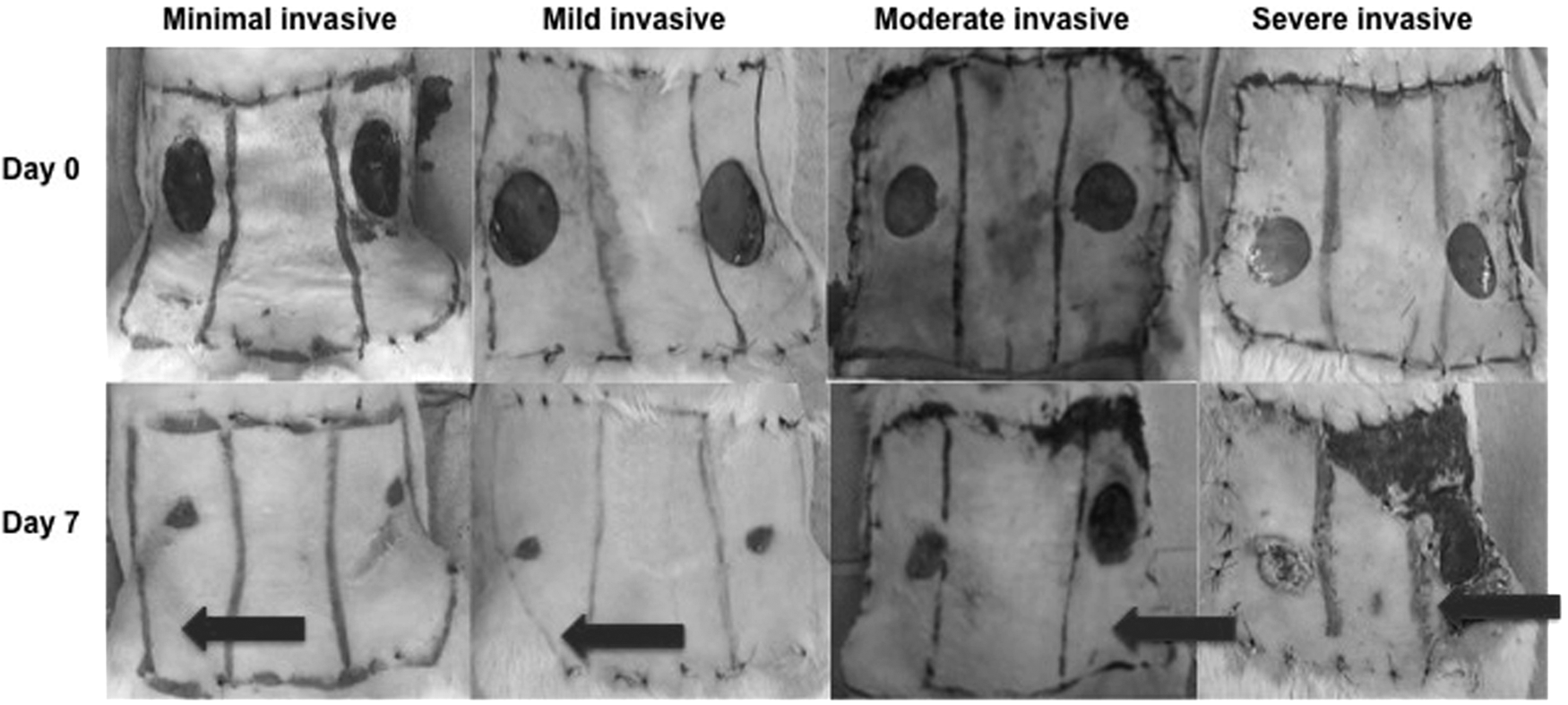
Representative images of the incisional wounds: postoperatively (day 0) and after 7 days. Arrows indicate side of ligation (ischemia). Markings on the rat abdomen indicate ischemic (ligation site), borderline (middle), and nonischemic (contralateral site) area. Minimal and mild approach show similar wound sizes after 7 days. The moderate approach shows significantly smaller wounds in the vital area compared to the ischemic area. Wounds in the severe approach were larger compared to the other approaches, without relevant differences between the wounds with large necrosis in the ischemic area.
Minimal and mild invasive approach
No clinical impairment of healing could be detected between ligated and contralateral nonligated wound areas after 7 days as reflected by similar wound size in both approaches (25.8% wound surface area in the ischemic area vs. 37.7% in the nonischemic area in the minimal approach; 45.5% wound surface area in the ischemic vs. 42.1% in the nonischemic area in the mild approach).
Moderate invasive approach
After 7 days the dimension of all excision wounds decreased compared to day 0 ( = baseline), irrespective of the presence of ischemia. However, wound healing in the ischemic areas occurred slower in comparison to the wounds in the vital areas with significant differences on day 7 postsurgery (31.7% ± 7.9% vs. 62.3% ± 27.9%, respectively; p < 0.05).
Severe invasive approach
Wounds in the ligated ischemic but also nonischemic area were larger with lower healing tendency compared to the minimal and mild invasive approach on day 7 with similar wound size in both areas (60.3% wound surface area in the ischemic part vs. 51.2% wound surface area in the vital part).
Histological analysis
Histological analysis with H&E staining was performed to evaluate differences in regeneration between normal nonischemic and ischemic wounds. Due to the meaningful results in all other parameters, the histological analysis focused on the most relevant moderate invasive approach. Under nonischemic conditions the wounds showed signs of inflammation with partially hyper-/parakeratosis. In the area of the excision extended granulation tissue could be discriminated without organization. Angiogenesis within the granulation tissue could be observed as evidenced by multiple vessel structures. The muscle layer beneath was also mildly infiltrated by inflammatory cells, and some fibers displayed signs of partial necrosis recognized by intramyofibrillar mononuclear cells. However, under ischemic conditions, the epidermis showed hyperplasia at the border of the excision wound, covered with a thick keratinized layer showing apoptotic bodies. Within the granulation tissue infiltration of inflammatory cells was visible. Several degenerative vacuoles could be observed as a sign of tissue necrosis. However, angiogenesis was less seen compared to the nonischemic control tissue. The underlying muscle showed disorganization, invasion of mononuclear cells, and degenerative vacuoles (Fig. 6).
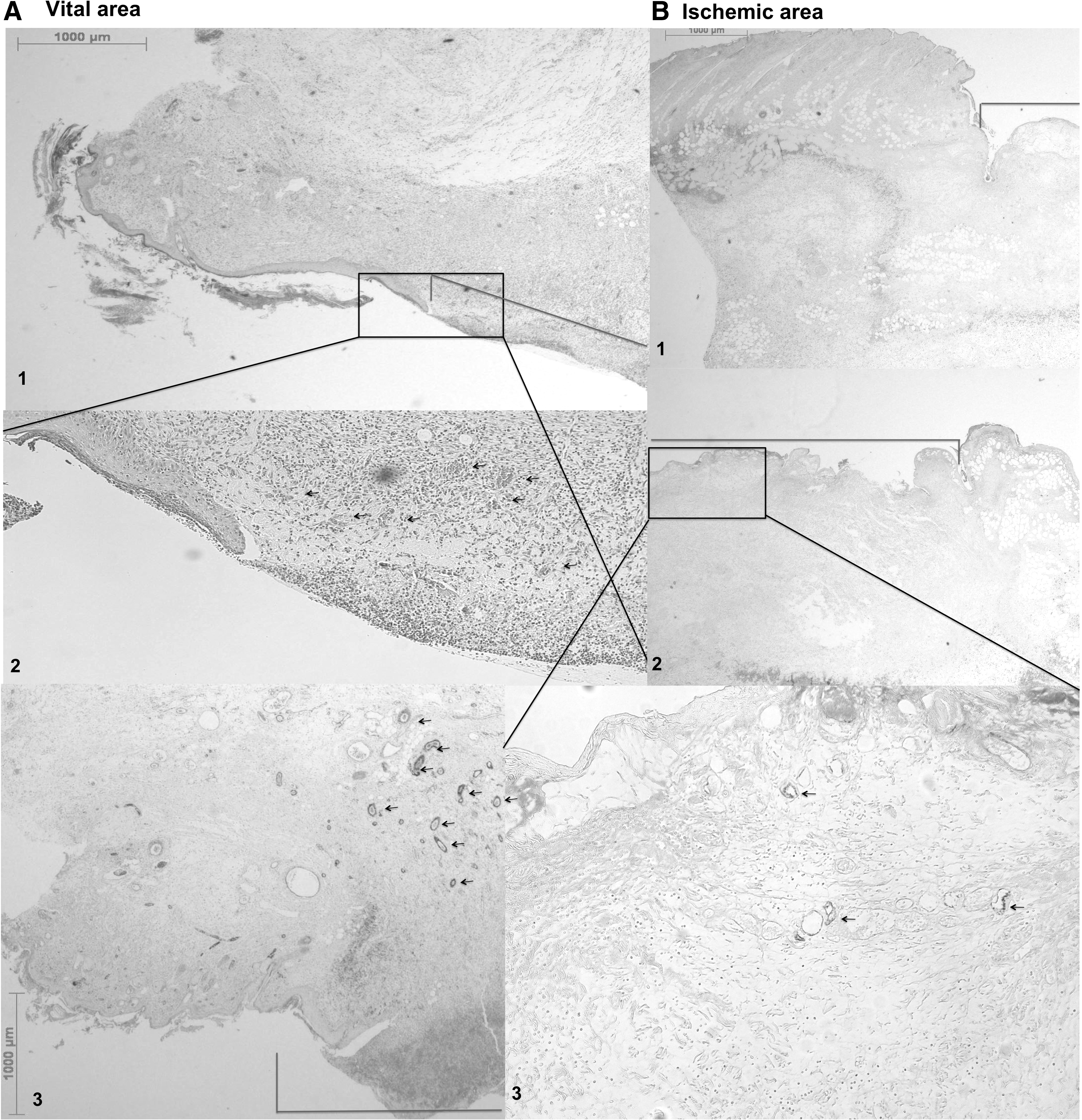
Representative histological images of wound areas in the moderate invasive approach. Bars depict wound area, arrows indicate vascular structures.
Immunohistochemical staining clearly showed mature vessels in the granulation tissue in the nonischemic side. Contrary, in the ischemic wounds only few vessels were found, showing impaired tissue perfusion resulting in disturbed wound healing, but avoiding extended tissue necrosis (Fig. 6).
Discussion
Impaired wound healing due to insufficient vascular supply is a common and severe clinical problem still lacking satisfying therapeutic approaches. For the development of new treatment strategies, appropriate animal models are essential. The aim of the present study was the establishment of a delayed wound healing model evoked by insufficient perfusion.
By creating two circular wounds in an ischemic and nonischemic area in a rodent epigastric flap a reliable ischemia impaired wound healing model was established. The wounds in the ischemic area were of significant larger size compared to the nonischemic intern control wounds after 7 days in the moderate approach. Thus, the clinical situation of impaired wound healing by insufficient perfusion of the wound area (e.g., in peripheral arterial diseases) is imitated. 22
Animal models mimicking clinically relevant diseases are crucial for the development of novel therapeutic approaches. There are several experimental studies on impaired wound healing using various model setups: Chronic pressure models simulating pressure ulcers,11–14 metabolic defects like diabetic wound healing models, 15 immunosuppressive strategies using glucocorticoids, radiation, 16 or chemotherapeutics, 17 ligation flap models, 6 rat dorsal flap model, 18 rabbit ear models, 19 and hind limb models. 20 Most of them are complex, demanding in surgical technique and often time consuming. Contrary, the surgery of the present model is simple and time efficient, and the reproducibility of ischemic wound healing behavior was high. Different surgeons performing the procedure achieved comparable outcome of evaluated parameters. However, one of the biggest strengths of the model is the possibility to test different treatment approaches in both an ischemic wound area and a healthy normally perfused contralateral internal control wound. Thus, differences in the wound healing process can be elucidated in one animal excluding certain bias evident in different individuals.
Another advantage of the model is that healthy animals were studied only compromised by regional ischemia without long-lasting preconditioning such as Streptozotocin treatment to achieve pathological healing conditions, thus reflecting time and cost improvement. However, in later studies diabetic or aged animals can be used in this model to combine both the clinically relevant comorbidity of diabetes, age associated systemic alterations, and peripheral vascular diseases.
The ligated epigastric bundle includes the artery, the vein, and the nerve which all supply the unilateral epigastric area. Currently, the influence of venous stasis, a yet not experimentally reproduced clinical entity, 10 and neuropathic changes that lead to an insensate area, are included in the model. In further studies, we thus have the possibility by ligating a single structure—artery, vein, or nerve—to focus on healing disorders emanating by each of them.
Trujillo et al. recently modified a rat dorsal flap model by placement of two silicon sheets beneath the wound to prevent revascularization from the recipient bed and to reduce contraction during wound healing. 18 In our model, we did find wound contraction to a certain degree in both the ischemic and the nonischemic region, as it is natural for wounds in rodents. Nevertheless, we found accelerated healing progress in wounds created in the vital area compared to the ischemic wounds then examining histologic specimen in the moderate invasive surgical approach (enhanced granulation tissue growth and improved reepithelialization). Therefore, we believe that the present model using the moderate invasive strategy is suitable to study wound healing in an insufficiently perfused area concomitantly comparing to an internal healthy control. Furthermore, applying different treatment modalities, various other parameters can be easily performed, including but not limited to immunohistology and biomolecular variables. In the present study, we only realized standard histology, since our primary focus was to identify the optimal degree of ischemia to establish an efficient delayed healing model.
As mentioned, different therapeutic regimens considering recombinant growth factors, gene therapy or stem cell therapy, injected alone or delivered locally by matrices need to be tested first in a relevant preclinical model. The excision wounds can be covered by the growth factor/biomatrix composition, thus sealing the wound and promoting the healing by the local growth factor stimulus. More general, this wound configuration enables to apply local delivering scaffolds of different constitutions like gel matrices, collagens, fibrin, or treatments comprising powder structures. Furthermore, different application methods can be tested, like the injection of therapeutics in the wound area, the plane application of sealant and powder, or the application of meshes. Already clinically established but mechanistically yet not fully understood therapeutic approaches like extracorporeal shockwave therapy 4 can be studied to investigate associated pathways in healthy and disturbed wound healing conditions.
In this study we used LDI and computed planimetrical analysis to monitor ischemia in the ligated area and to follow up wound size over 7 days. The animal model design, especially the superficiality of the area of interest and the appropriate wound size, allows several further methods for analyses. In earlier studies we used fluorescence imaging to follow labeled fibrin degradation over time and luminescence imaging to detect transfected cells. 23 Our model seems especially suitable for both methods. If specific techniques are not available, the wound size can be easily measured using transparent acrylic sheets. LDI can be exchanged for other perfusion measurement techniques. Postoperative histologic analysis with different staining and immunohistochemical methods, as well as histological measurements, 24 offers further options to display wound healing progress and therapy outcome.
In this study, we have established a novel excisional wound healing model disturbed by ischemia, showing significant wound healing alterations compared to nonischemic internal control wounds. The model proved to be reliable and highly reproducible, thus making it suitable to study and to develop different therapies and application forms. In further studies we intend to test the influence of various growth factors delivered locally from scaffolds such as a fibrin biomatrix.
Footnotes
Acknowledgments
Funding of this research project was provided by Angioscaff (NMP-2007-2.3-1). The authors thank Alexandra Meinl for support in histologic evaluation and Ilse Jung for statistic analysis.
Disclosure Statement
No competing financial interests exist.