
Abstract
While clinical vascular grafting uses an end-to-side surgical method, researchers primarily use end-to-end implant techniques in preclinical models. This may be due in part to the limitations of using small animal models in research. The work presented here provides support and evidence for the improvement of vascular graft implant techniques by demonstrating the successful implantation of experimental grafts into both large and small animal models. Specifically, models of aortoiliac baboon (Papio anubis) bypass and common carotid rabbit (Oryctolagus cuniculus) bypass were used to test vascular grafts for thrombosis and vascular healing after 1 month using an end-to-side anastomosis grafting procedure. Patency was evaluated with ultrasound or histological techniques, and neointimal growth was quantified with histology. In the development of this procedure for small animals, both an end-to-end/end-to-side and an end-to-side/end-to-side configuration were tested in rabbits. One hundred percent of rabbit implants (2/2) with an end-to-end/end-to-side configuration were patent at explant. However, with the end-to-side/end-to-side configuration, 66% (6/9) of rabbit implants and 93% (13/14) of baboon implants remained patent at 1 month, suggesting the importance of replicating the end-to-side method for testing vascular grafts for clinical use. This study describes feasible preclinical surgical procedures, which simulate clinical vascular bypass grafts even in small animals. Widespread implementation of these end-to-side surgical techniques in these or other animals should improve the quality of experimental, preclinical testing and ultimately increase the likelihood of translating new vascular graft technologies into clinical applications.
Impact Statement
Most animal models to date study bypass grafts using end-to-end surgical techniques. This article describes the feasibility and importance of using an end-to-side approach when examining preclinical performance of vascular grafts. Researchers demonstrate and evaluate a more clinically relevant method of end-to-side grafting in both large and small animal models. Efforts to incorporate these methods into future studies should improve clinical translatability.
Introduction
V
To address a lack of development in this field, Zilla et al. 2 wrote a provocative opinion article in 2007 criticizing the approaches that scientists were using to study vascular graft healing. Unfortunately, over a decade later, few researchers have heeded Dr. Zilla's advice. Specifically, in vivo vascular graft studies need to use longer grafts with an end-to-side implant model to examine the clinically relevant flow conditions observed by the native tissue with this type of anastomosis. A current review of vascular graft implant studies yielded 96 relevant publications in which animal implants have been performed since 2007 (Fig. 1). Of these, only four used an end-to-side implant method,3–6 and five were implanted as an arteriovenous graft.5,7–10
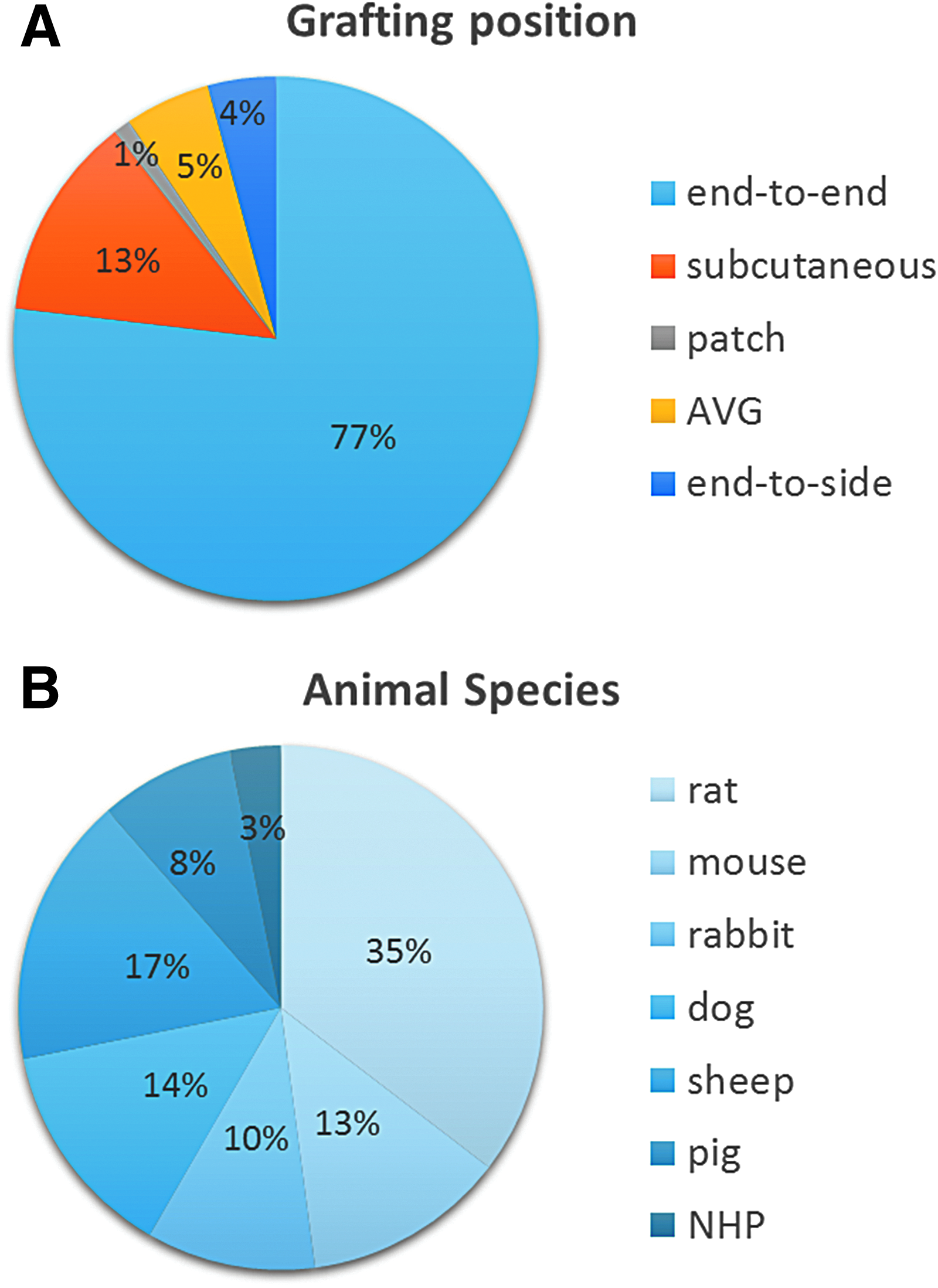
Survey of methods from 96 animal implants in the past 10 years.
Certainly, initial small animal work with interpositional grafts or subcutaneous implants to examine biocompatibility is important; however, even in large animals, researchers continue to use models that do not represent physiologic conditions or clinically relevant applications, where nearly all vascular grafts have end-to-side anastomoses. Previous work has laid the groundwork for performing end-to-side anastomoses in small animals by performing arterial/venous anastomoses using native tissues,11–13 but almost no researchers have translated this work into tissue engineering or biomaterials research. One notable exception is the work by Assmann et al. 6 who implanted a decellularized allograft into a rat infrarenal aorta in an end-to-side configuration, but arguably anastomosing a synthetic or tissue-engineered vascular graft in small animal is more challenging due to a need to match the thickness and the caliber of the graft and the vessel. New techniques are needed to enable the end-to-side anastomoses of engineered biomaterials in small animal models.
The lack of appropriate animal models plagues new research and may explain why very few developments have been observed clinically in vascular grafts. Dacron and ePTFE (expanded polytetrafluoroethylene) remain the clinical gold standards for artificial vascular materials when autologous grafts are not available. These materials have been available for decades, and yet have limitations due to low long-term patency at small diameters. Tissue engineering has attempted to fill this market by using cell-based approaches to develop small-diameter vascular grafts but has yet to bring a clinically useful device to market. The dearth of success in this field is likely attributed to the lack of good animal models that give a solid understanding of what will provide clinical translatability.
This article addresses the need for clinically relevant animal models, by validating surgical methods that can be applied to a variety of animal species. Our previous work has primarily focused on implanting 4 mm ePTFE vascular grafts into the aortoiliac position of a nonhuman primate model to provide the most clinically relevant approach3,14–21; however, we also demonstrate how this can be translated to smaller animals. Specifically, by implanting 2 mm ePTFE grafts with end-to-side anastomoses and poly(vinyl alcohol) grafts into the right common carotid artery (CCA) of rabbits with two different techniques: the end-to-end (proximal)/end-to-side (distal) anastomoses and the end-to-side for both proximal and distal anastomoses, we show the ability to evaluate small-diameter vascular grafts in a small animal model.
In small animal models, one challenge to studying a straight tube vascular graft with an end-to-side anastomosis is finding large vessels. To accommodate this challenge we developed an end-to-end/end-to-side implantation model in the rabbit carotid that allows a straight tubular graft to be implanted into an unbranched vessel. The aim of this work was to demonstrate that end-to-side grafting is feasible in a small animal model, and we hypothesize that the end-to-side/end-to-side configuration in the rabbit will demonstrate a more clinically relevant animal model compared with end-to-end/end-to-end configurations, and thus more closely reflect the previously developed and clinically validated baboon bilateral aortoiliac implant model.
Materials and Methods
Baboon surgery methods
Vascular graft implants in juvenile, male baboons (Papio anubis, 16.6 ± 3.2 kg) were performed at the Oregon National Primate Research Center (ONPRC) at Oregon Health & Science University (OHSU). Studies were approved (# IP00000049) by the Institutional Animal Care and Use Committee according to the “Guide for the Care and Use of Laboratory Animals” prepared by the Committee on Care & Use of Laboratory Animals of the Institute of Laboratory Animal Resources, National Research Council (International Standard Book, No. 0-309-05377-3, 1996). The ONPRC facility is fully accredited by the American Association for Accreditation of Laboratory Animal Care (AAALAC), and has an approved Assurance (#A3304-01) for the care and use of animals on file with the Office for Protection from Research Risks at the National Institutes of Health (NIH).
Bilateral implants of 4 mm inner diameter (ID), 5–7 cm in length, ePTFE (W.L. Gore & Associates, Inc.) were implanted in an aortoiliac position in seven animals. The proximal anastomoses were performed to the abdominal aorta. Construction of the distal anastomoses was performed at the iliac artery bifurcation (Fig. 2) in seven animals. After anesthesia was administered as ketamine (10–20 mg/kg intramuscularly) or Telazol (3–5 mg/kg intramuscularly), followed by 1–3% isoflurane delivered at 1–2 L/min in 100% oxygen, and animals were clipped and aseptically prepared.

Surgery began with a midline incision into the abdomen. The abdominal contents were packed away to expose the abdominal aorta in its length to the bifurcation. The iliac arteries were also dissected out to the level of the iliac bifurcation. The abdominal aorta was partially clamped with atraumatic microvascular clamps after a heparin bolus (100 IU/kg), to facilitate the proximal anastomoses of the grafts. For each proximal and distal anastomosis, the artery was opened longitudinally using a #11 blade, and the arteriotomy extended using a 30° Potts forward cutting scissors. Graft ends were spatulated to 45° angles. End-to-side anastomoses were constructed using a combination of continuous and interrupted 7-0 polypropylene sutures. This closely mimics clinical surgical practice. 22 Each graft was then anastomosed distally to the common iliac artery on that side above the bifurcation of the iliac into its external and internal branches. The common iliac artery proximal to the distal anastomosis was ligated with a silk suture. No additional antiplatelet therapies were given during or after surgery. For terminal experiments, at 4 weeks postimplant, animals were given ketamine (20 mg/kg), followed by phenobarbitol (25 mg/kg) and exsanguination for euthanasia. Samples were explanted by pressure fixing with 10% formalin. After full fixation, sections were embedded in paraffin, and stained with hematoxylin and eosin (H&E) using standard histological procedures. Intimal hyperplasia was quantified as described previously. 3 In brief, the immunohistological midpoint sections of both the proximal and distal anastomoses were selected and imaged. Using ImageJ, a trained, blinded analyzer traced a 2 mm arc length distance starting at the anastomotic junction. The tracing was extended into the graft region to quantify the neointimal surface area on the vascular graft material. Filling the area, ImageJ quantified the total pixels in the IH area. Knowing the scale of the image, pixels were converted to surface area and presented as an area of ingrowth for that 2 mm distance.
Rabbit surgery methods
Vascular graft implants in male New Zealand White rabbits (Oryctolagus cuniculus, 3.7 ± 0.2 kg) were performed at the Center of Animal Facility (CAF) at the University of Waterloo. Studies were approved (#AUPP 16-09) by the Animal Care Committee according to the Canadian Council on Animal Care's Guidelines, the requirements of Province of Ontario's Animals for Research Act, and the University of Waterloo's Guidelines for the Use of Animals in Research and Teaching. CAF was accredited by the Ontario Ministry of Agriculture and Food and Rural Affairs with accreditation number 0079-01, and was certified by the Canadian Council on Animal Care to have a Good Animal Practice.
Enrofloxacin (10 mg/kg; Baytril) was administered intramuscularly as antibiotic 24 h before surgery. Ketamine (35 mg/kg) and xylazine (5 mg/kg) administered intramuscularly, followed by 1–3% isoflurane through inhalation. Animals were intubated after induction of anesthesia with ketamine and xylazine. Heparin (200 IU/kg) was administered intravenously before arterial clamping. In the event of vasoconstriction or spasm of the arteries, 5–10 mL of warm (37°C), sterile saline solution was applied topically on the constricted vessel. If vasodilation was not observed, a few drops (0.3–0.5 mL) of papaverine (a vasodilator) were applied topically on the vessel.
End-to-end/end-to-side anastomosis in rabbit model
An end-to-end/end-to-side implantation method was performed in two animals, each having one polyvinyl alcohol (PVA) graft implanted at the right CCA (Fig. 3A, C). Straight PVA graft (outer diameter = 2 mm, length = 1.49 cm) ends were precut perpendicularly for end-to-end anastomosis and obliquely (45°) for end-to-side anastomosis using a straight mayo scissors. The rabbit's right CCA was exposed using four to six round wire handmade retractors, secured with four to six mosquito clamps at the end of each retractor. Two size-3 vascular clamps were used to clamp the CCA at distal and proximal positions. The thyroid artery branch, which was located in between the two clamping sites, was then ligated. The CCA was cut in between the clamps using a straight microscissors.

Implant schematic for
To make an end-to-end anastomosis, the PVA graft end (perpendicular cut) was aligned with the open vessel end (proximal). Using 8-0 Ethilon Polyamide 6 suture (Ethicon), the graft was stitched onto the vessel with 8–10 interrupted sutures starting with 1 suture on each lateral and medial side (180° apart), followed by 3–4 sutures on each of the ventral and dorsal sides. To make an end-to-side anastomosis, a hole was made at the CCA (distal) by creating an interrupted suture at the vessel wall, and then cutting away the sutured section using the microscissors. Like before, one suture was placed on each distal and proximal side, followed by three to four interrupted sutures on each lateral and medial side. The opened end of the CCA (distal) was then tied off, and clamps were released for leak testing.
End-to-side/end-to-side anastomosis in rabbit model
The end-to-side/end-to-side implantation method (Fig. 3B) was performed in nine animals with seven animals receiving PVA grafts (Fig. 3D) and two animals receiving ePTFE grafts (Fig. 3E); each having one graft implanted into the right CCA. PVA (1.8 mm ID, 1.9 cm long) or ePTFE graft (2 mm ID, 1.9 cm long) was precut in an oblique manner to make angled (45°) anastomoses using a straight mayo scissors. The right CCA of the rabbit was exposed using four to six round wire handmade retractors, secured with four to six mosquito clamps at the end of each retractor. The thyroid artery branch was then ligated. Two size-3 vascular clamps were used on the CCA at distal and proximal positions.
To make an end-to-side anastomosis, a hole was made at the CCA by placing an interrupted suture at the vessel wall, and then cutting away that sutured section using a microscissors. Using 8-0 Ethilon Polyamide 6 suture (Ethicon), the graft was stitched onto the vessel with 8–10 interrupted sutures starting with 1 suture on each distal and proximal side (180° apart), followed by 3–4 sutures on each of the lateral and medial sides. After finishing the second end-to-side anastomosis, the CCA between the two anastomoses was tied off with two sutures to prevent blood from flowing through the original CCA, and the clamps were released.
Ultrasound Doppler
To assess patency of the implanted grafts, Doppler ultrasound imaging of blood flow was done on day 12 for end-to-end/end-to-side and on day 16 for end-to-side/end-to-side. Both days 12 and 16 were chosen to represent the graft patency close to the midpoint of the 1-month implant duration; that is, day 15. The presence of a moving fluid in the probed area was indicated on the Doppler ultrasound image. Measurements were performed using SonixTouch (Analogic Ultrasound, Peabody) with a 10.0 MHz probe. The rabbit was put under 1–2% of isoflurane before performing ultrasound measurement.
Histology of the excised grafts
Heparin (500 IU) was administered into the blood circulation before euthanization with sodium pentobarbital (100 mg/kg). The graft, CCA, and surrounding tissues were excised, rinsed with saline, and fixed in 4% paraformaldehyde for 72 h. Tissue embedding was done using Paraplast (Leica), and tissue sections were stained with H&E.
Statistical analysis
Baboon IH data were analyzed using a one-sided t-test with 95% confidence interval to determine equivalency, where statistical equivalence was defined as an area change of 0.06 mm2 or less.
Results
Baboon surgery results
At 4 weeks, 93% of the implanted 4 mm diameter ePTFE grafts were patent (13/14 grafts from seven animals). For the neointimal analyses, 12 grafts from six animals were analyzed. The patent graft that was paired with the occluded graft was omitted due to the significant alteration in flow conditions in the graft after occlusion (all aortic blood flow was then going through the single graft). Representative histology and IH quantification (Fig. 4) illustrate statistical equivalence between proximal (0.18 ± 0.10 mm2) and distal (0.20 ± 0.12 mm2) anastomoses (p = 0.038). At this 28-day time point, the neointima is generally thickest along the suture line at the interface of the native artery and implanted graft. The IH tapers down along the length of the graft away from the anastomosis.
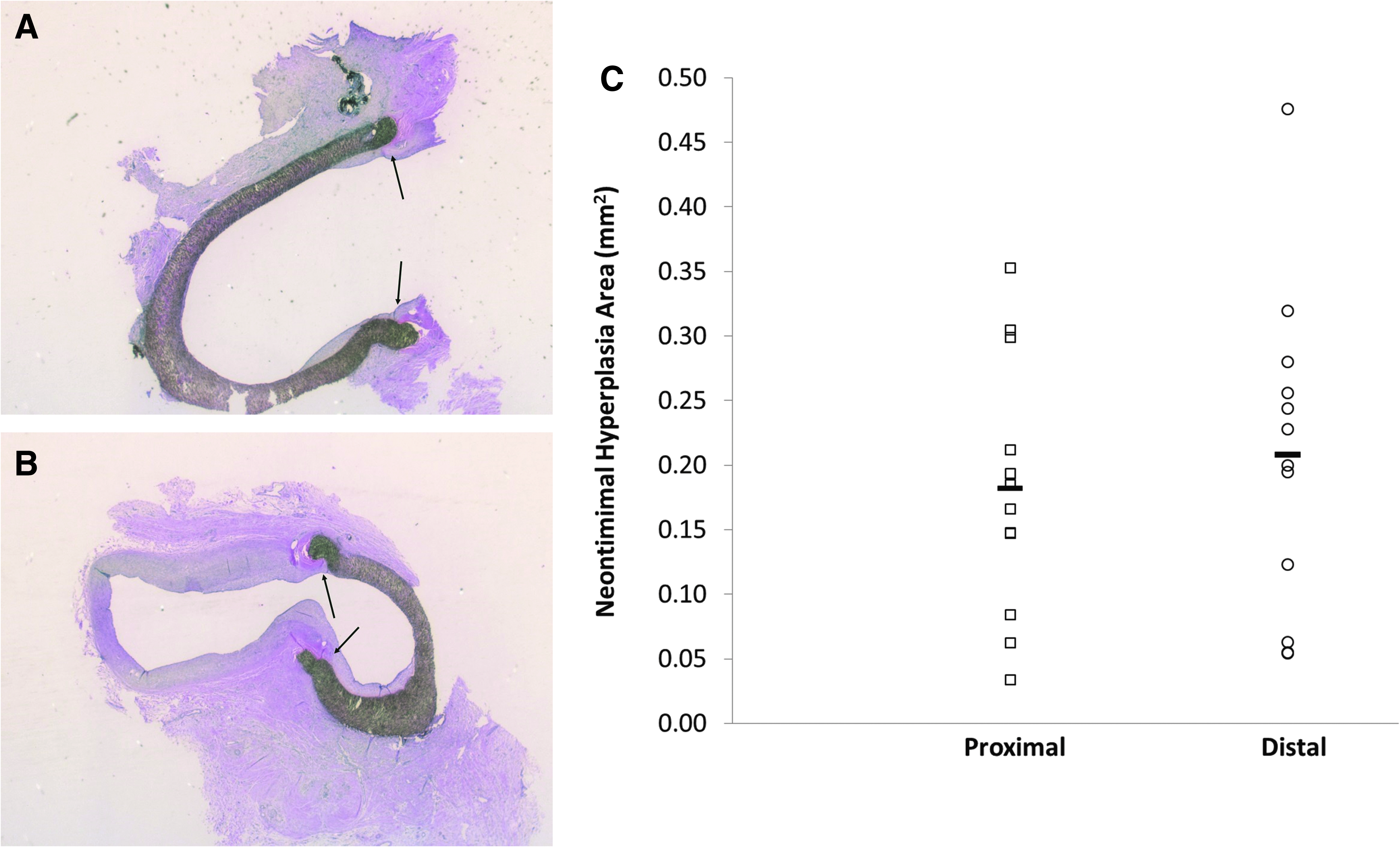
Histological analysis of end-to-side implanted 4 mm diameter ePTFE in juvenile male baboons. Representative H&E staining of
Rabbit surgery results
Figure 3 illustrates the successful implantation of a 1.8 mm diameter PVA vascular graft using end-to-end (Fig. 3A) or end-to-side (Fig. 3B) methodology, and 2 mm diameter ePTFE graft using end-to-side methodology (Fig. 3C). All grafts remained patent at days 12 or 16 as measured with the Doppler ultrasound at the midsection of the grafts (Fig. 5A–C). Furthermore, all rabbits survived until the endpoint (day 30). Two of two PVA grafts with end-to-end/end-to-side anastomoses were patent (100%) at the endpoint. Subsequent PVA and 2 mm ePTFE implants using end-to-side/end-to-side configuration showed patency in 5/7 grafts (71%) and 1/2 grafts (50%), respectively, after 28–30 days of implantation. Figure 5C–E shows the H&E histological analysis of the grafts implanted with end-to-end/end-to-side anastomoses and end-to-side/end-to-side anastomoses. Results showed the presence of mild thrombosis in the end-to-end/end-to-side implant (Fig. 5C) as well as neointima formation in the end-to-side/end-to-side implant (Fig. 5D, E). There was no neointima formation and less thrombosis observed in the first anastomoses configuration, indicating the greater challenge in end-to-side anastomoses. Attempts to quantify the graft IH in the rabbit surgery per the baboon methods were inconclusive due to native tissue that likely shifted during the ligation step. The recommended method for future implants is to ligate farther from the anastomosis site.
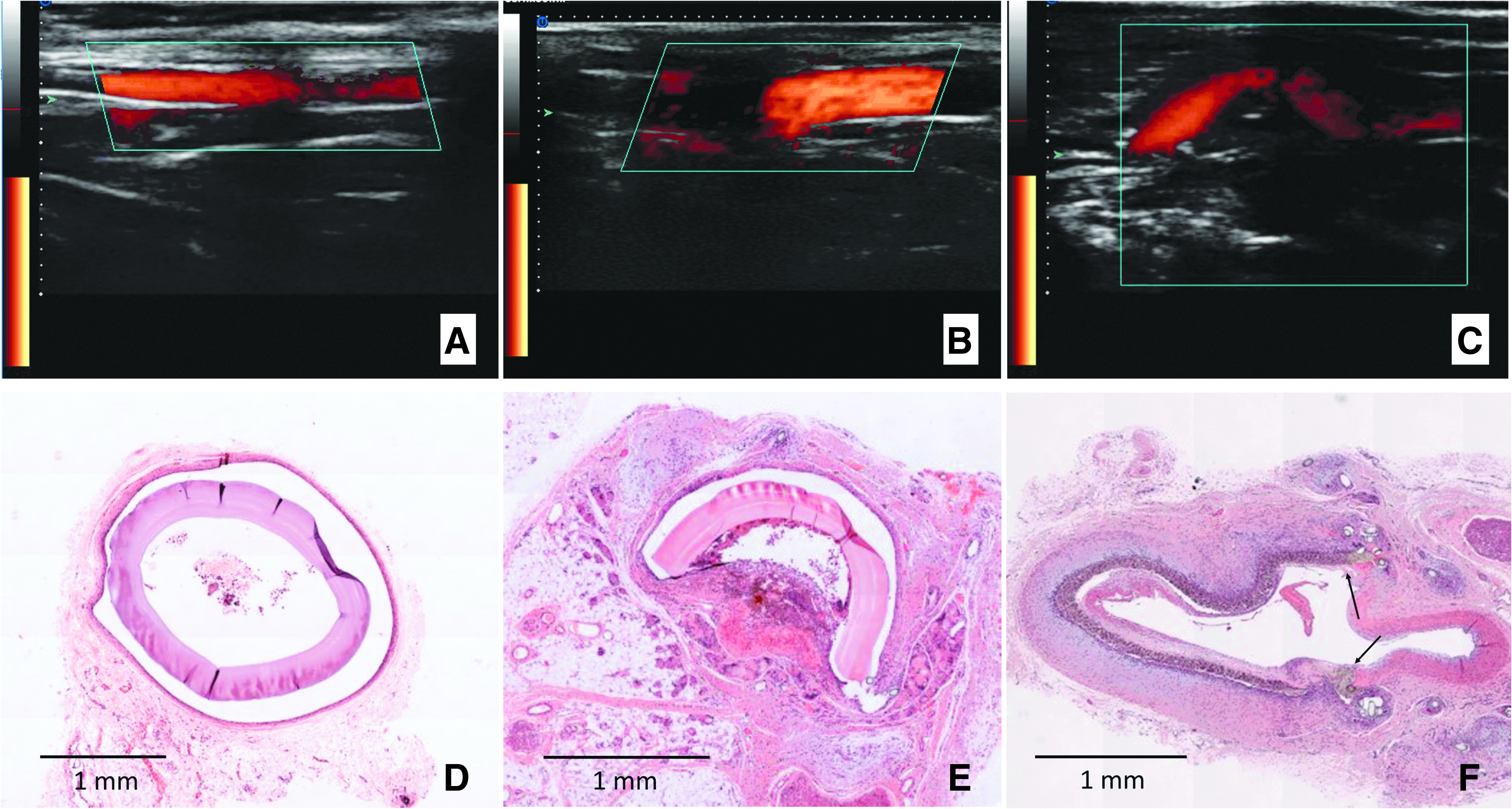
Doppler ultrasound measurements were taken at
Discussion
This study demonstrates the importance of end-to-side grafting when testing biomaterials for vascular graft implantation, and describes the methodology to support its use by showing successful implantation of multiple materials in large or small animals. Small animal models for preclinical testing are less costly and raise fewer ethical concerns than large animal models. However, due to size limitations, vascular graft implantations are often done in an end-to-end manner,23–25 which is not representative of the actual use of the grafts in a clinical setting and has led to the lack of translation from successful preclinical graft results into clinical studies. Comparing the end-to-end/end-to-side and end-to-side/end-to-side implant configurations in the rabbit, it was clearly demonstrated that the end-to-side/end-to-side configuration, which was also presented in the baboon, is the more challenging and clinically relevant implant model. Research that continues to use end-to-end grafting may be biasing results to better patency than would actually be experienced in a clinical setting.
Previous work described the variations in flow dynamics associated with varying graft angles in an end-to-side anastomosis, and found that an anastomotic angle of <30° reduces flow disturbances. 26 Clinically, surgeons strive to minimize these disturbances, but even a low angle is dramatically different than the end-to-end, interpositional grafts that are common in preclinical testing of new technologies. The difference between the two types of anastomoses (end-to-end and end-to-side) can be dramatic as the end-to-end anastomosed artery does not experience the significant wall shear stress variability as that observed in an end-to-side anastomosis.27,28 It is not uncommon to have turbulent and oscillating flow in an end-to-side anastomosis, which is known to contribute to neointimal formation. 28 Taking these complications into consideration, a graft that is patent when implanted in an end-to-end manner may not be patent when implanted in an end-to-side manner due to these differences in neointimal growth. This limits the clinical translatability of these grafts.
While the work presented here illustrates that end-to-side grafts are feasible even in smaller animal models, it is critical to understand the importance of a skilled surgeon to perform the surgeries in either a small or large animal model, to prevent inaccuracies with suture positioning, vascular misappositions, puckering, and blood loss. Clinically, these procedures would be performed by an experienced surgeon, with >2 years of experience in performing microvascular anastomoses. Our expertise suggests that rapidly performed and clean anastomoses are less likely to develop thrombosis or IH, and provide consistent results between animals. The best results would likely be obtained by a vascular surgeon who performs a minimum of 30 procedures with some regularity and a surgical assistant. This may present a significant hurdle to many research groups in improving vascular graft animal studies, particularly with small ID vessels and grafts, which require microsurgical skills. However, veterinary staff with surgical skills have been trained in this procedure by using bench top vascular surgery skills kits and anastomosis training using fresh, vascular-rich tissue beds. Veterinary staff for the small animal work were able to obtain sufficient practice through cadaver anatomy practice and a workshop on vascular anastomoses and microsurgery. Veterinarian surgeons wishing to learn this procedure would likely benefit from mentoring by an experienced vascular, clinical surgeon and should obtain the necessary skills with significant practice.
This work focused on examining the patency and IH of vascular graft anastomoses; however, when preclinical studies are performed, additional characterization may be desirable to better understand the graft's potential for success or failure. Other valuable imaging modalities could be used to visualize and quantify responses to the implant, such as magnetic resonance imaging, computed tomography, optical coherence tomography, intravascular ultrasound, and angiography, where these facilities are available. These could be used to further characterize the anastomotic shape and luminal diameter, and gain a deeper understanding of the healing potential of the graft.
The type of animal model used and the graft anastomosis configuration has implications in the endothelialization of the implanted grafts. Many researchers have found better endothelialization rates in animal models, which do not translate to clinical outcomes. Previous work found that our baboon, aortoiliac model will endothelialize a nonporous graft ∼0.5 cm in 1 month and 0.8 cm in 3 months. 17 Care must be taken to have a graft long enough to avoid spontaneous endothelialization not observed clinically. The use of a larger animal is a strong step toward avoiding this problem, but so potentially is the use of a longer graft. End-to-end grafts in small animal models tend to be only ∼1 cm long, whereas end-to-side grafting allows for substantially more length. This is particularly critical when evaluating grafts for peripheral artery disease. It is possible that to achieve the lower flow rates observed in peripheral artery grafting, a large animal is required. Despite these limitations, end-to-side anastomoses in relatively small animal models provide clinically relevant information on the in vivo healing response.
All animal models have advantages and limitations. 29 Nonhuman primates are strong candidates for vascular graft animal models because of their similarity to human genetics,30,31 hemostasis,32–34 and mechanical properties.35–38 It is also advantageous that probes and assays developed for human tissues can be used for studies on nonhuman primates. While we and others 5 have found success with this model, it has limited availability and high cost. The rabbit is a small animal model that has resemblance to human cardiovascular system; it is often used as a model in atherosclerosis39,40 and cardiac disease studies.41,42 Through this work, we successfully evaluated a working method for small-diameter (4 and 2 mm), artificial vascular bypass graft with an end-to-side implant method. We believe that these methods can be applied to other small or mid-sized animal models, and should definitely be used with large animals, such as sheep or pigs. Efforts to use these methods in preclinical testing should promote translation of new graft technologies into clinical use.
Footnotes
Acknowledgments
This work was supported by National Institutes of Health Grants R01HL130274 and R01DE026170. We gratefully acknowledge the staff at ONPRC and CAF, specifically the critical technical assistance of Ms. Jennifer Johnson, Ms. Barbra Mason, and Ms. Jean Flanagan. We appreciate W.L. Gore for supplying ePTFE graft material for scientific study. We thank the technical ultrasonography assistance of Dr. Adrian J.Y. Chee, Mr. Billy Y.S. Yiu, and Prof. Alfred Yu from LITMUS. For the surgical procedures, we thank Dr. Marek Kukumberg and Dr. Howard Song for helpful advice on developing the procedures. Finally, we thank Ms. Erica Sharp and Yim laboratory members for technical support, and Mr. Kyle Hart from OHSU Biostatistics Design Program and Mr. Matt Hagen for their assistance with equivalency testing.
Disclosure Statement
No competing financial interests exist.