
Abstract
Purpose:
To test the technical aspects and feasibility of seeding a combination of meniscus cells isolated from a rapid digestion protocol and mesenchymal stromal cells (MSCs) (20:80 ratio) into a meniscus scaffold for the development of a one-stage arthroscopic procedure for meniscus regeneration.
Methods:
A cadaveric study was performed using nine fresh frozen human cadaveric knee joints. Two different arthroscopic cell-seeding methods were applied to the Collagen Meniscus Implant (CMI®) as carrier scaffold: either (1) seeding before arthroscopic surgical implantation of the scaffold or (2) after implantation of the scaffold. The cells were injected inside the scaffold, using fast green-stained fibrin glue as carrier, to macroscopically visualize the amount of fibrin glue. Macroscopic pictures and confocal microscopy analyses were used to determine cell distribution and viability. In addition, the DNA content in the cell-seeded scaffold was determined. In addition, different concentrations of Liberase were examined to find the optimal concentration for rapid digestion of meniscus tissue.
Results:
Macroscopically, seeding before implantation showed a better distribution of fast green-stained fibrin glue carrier than seeding the scaffold before surgical implantation. In addition, it resulted in significantly more cells and a better cell distribution compared with seeding the scaffold after arthroscopic implantation. Both seeding methods did not affect cell viability. After rapid digestion, 0.0125% Liberase resulted in the highest cell isolation efficiency.
Conclusions:
This study demonstrates that living human meniscus cells can be isolated efficiently, combined with MSCs in 20:80 ratio, and uniformly delivered into a currently available meniscus scaffold. This scaffold can then be arthroscopically implanted, creating a one-stage solution for partial meniscal deficiency.
Impact Statement
Meniscus injury remains the most common indication for orthopedic surgery, but loss of functioning meniscus tissue is strongly correlated with development of early osteoarthritis. However, current clinical options for tissue engineering of the meniscus are limited. This study demonstrates the feasibility of combining human meniscus cells with mesenchymal stromal cells to enhance a meniscus scaffold for meniscus regeneration in a one-stage solution for partial meniscal deficiency.
Introduction
Meniscus injuries are very common, especially in young and active patients. Approximately 15% of all knee injuries involve a tear of the meniscus. 1 The main functions of the menisci are load transmission, shock absorption, and stability of the knee. 2 These native functions are impaired when an injury occurs causing a meniscus tear. This meniscus deficiency can result in excessive forces and abnormal loading of the articular cartilage, leading to osteoarthritis (OA).2,3 Meniscus tears in the nonvascularized zone have limited healing capacity, and currently the most frequently used surgical treatment involves (partial) removal of the damaged meniscus, 2 contributing even further to the early development of OA.4–7 To potentially prevent postmeniscectomy arthritis and treat postmeniscectomy syndrome, options such as implanting a porous meniscus scaffold have been introduced. Currently, a commercially available scaffold fabricated from bovine type I collagen will degrade within 1–2 years after implantation. 8 These porous scaffolds have shown promising clinical results up to 12 years follow-up, by demonstrating less pain, higher subjective scores using patient reported outcome measures, and a higher activity level than a partial meniscectomy control group.3,9 Ideally, healing may occur by surrounding resident meniscus cells and cells from synovial lining engraft the CMI, thereby forming meniscus-like tissue, while the biomaterial slowly degrades. However, this process is very slow, and long-term MRI demonstrates that <10% of the patients have a meniscus regenerate size similar to the native meniscus. 10
Therefore, this process potentially could be accelerated and improved by seeding the porous artificial meniscus with cells, as shown by Martinek et al. in a goat study. 11 Specifically, a combination of autologous meniscus cells and allogeneic mesenchymal stromal cells (MSCs) is promising, as these cell types could be seeded during a one-stage surgical procedure, thereby avoiding a costly two-stage autologous cell expansion. In addition, allogeneic MSCs have been proven to be safe and a viable cell source for implantation with autologous chondrons for regeneration of knee cartilage.12–14 Finally, biochemical and histological analysis of in vitro coculturing of MSCs and meniscus cells demonstrated excellent matrix production of glycosaminoglycans (GAGs) and type I collagen, especially in the ratios where a higher percentage of MSCs (up to 90%) was used. 15
For this one-stage surgical procedure to become clinically feasible, meniscus tissue digestion and uniform delivery of the cells into a meniscus scaffold need to be optimized. Specifically, a rapid digestion protocol 12 for meniscus tissue is needed to harvest sufficient meniscus cells to combine with allogeneic MSCs within the time frame of one surgery. These cells would then be delivered to a commercially available meniscus biodegradable scaffold. For optimization of seeding the meniscus scaffold with cells, two seeding methods are possible in clinical practice: (1) seeding before surgical implantation of the scaffold, or “dry seeding” (as the meniscus scaffold is still dry outside the knee at the time of seeding), or (2) seeding after surgical implantation in a fluid arthroscopic knee environment, or “wet seeding” (as fluids present in the knee at the time of implantation are already taken up by the scaffold). In both methods, the cells are injected inside the scaffold, using fibrin glue as a carrier for the cells to ensure local delivery. Therefore, the purpose of this study was to test the technical aspects and feasibility of seeding a combination of meniscus cells and MSCs (20:80 ratio) into a meniscus scaffold, using a rapid digestion protocol to isolate meniscus cells, for the development of a one-stage arthroscopic procedure for meniscus regeneration.
Methods
Study outline
To evaluate the feasibility of combining a commercially available meniscus scaffold (Collagen Meniscus Implant (CMI®); Stryker, Kalamazoo, MI) with autologous meniscus cells and allogeneic MSCs in a 20:80 ratio 15 during a one-stage arthroscopic procedure, a laboratory and cadaveric study on human knee specimens were performed.
Donors
Meniscus tissue was obtained as redundant material from four patients undergoing total knee arthroplasty. The anonymous use and collection of this material was performed according to the Medical Ethical regulations of the University Medical Center Utrecht and the guideline “good use of redundant tissue for research” of the Dutch Federation of Medical Research Societies.16,17 For the MSCs, bone marrow biopsies were obtained from the iliac crest during total hip replacement after written informed consent was obtained (Medical Ethical Committee, University Medical Center Utrecht).
Nine postmortem fresh frozen human legs were provided by the anatomy department of the University Medical Center Utrecht. These were graciously donated by people who signed written informed consent during lifetime for postmortem donation of their entire body for educational and research purposes.
Cell isolation
For a one-stage surgical application, it would be desirable to complete the isolation of autologous meniscus cells from the debrided meniscus tissue within 40 min, yielding enough cells for 20% meniscus cells (for a 2.5 cm defect a total of 2,000,000 cells are used 14 ) of the total seeded amount. Therefore, different concentrations of Liberase (Roche, Germany) were examined to find the optimal protocol for rapid digestion of meniscus cells.
For the cadaveric study, the entire meniscus of four donors was cut in pieces of 2 × 2 mm, washed in phosphate buffered saline (PBS) and digested in 0.15% collagenase type II (Worthington, Lakewood, NJ) dissolved in Dulbecco's modified Eagle's medium (DMEM; Life Technologies, Bleiswijk, The Netherlands) with 1% penicillin/streptomycin (1% pen/strep; 100 U/mL/100 μg/mL; Invitrogen, Life Technologies) overnight at 37°C on a shaker plate.
In addition, meniscus cells were acquired from four different donors using adapted versions of the rapid digestion protocol from Bekkers et al., 12 where concentrations of 0.05%, 0.025%, and 0.0125% of Good Manufacturer Practice (GMP)-grade Liberase (Roche, Germany) in DMEM with 1% pen/strep were used for the digestion of 100 mg of meniscus tissue with duration of 40 min at 40°C on a shaker plate. Afterward, for both digestion methods, the suspension was filtered through a 100 μm cell strainer (BD Biosciences), spun by centrifugation for 5 min at 300 g, resuspended in DMEM supplemented with 1% pen/strep and 10% fetal bovine serum (FBS; HyClone, Logan, UT), counted with an automated cell counter 1:1 diluted in trypan blue (Biorad) to detect dead cells (TC20™ Bio-Rad, Herclues, CA). The meniscus cells for the cadaveric study were cultured up to passage 3 or 4, whereas for evaluation of the rapid digestion protocol, the total cell count and viability were corrected for the weight of the tissue. To exclude the erythrocytes from the count, only cells larger than 6 μm were considered meniscus cells.
Human MSCs (hMSCs) were isolated from bone marrow biopsies as described previously 18 and were expanded in α-minimal essential medium supplemented with 10% FBS, 1% l-ascorbic acid-2-phosphate (Sigma-Aldrich), and 1% pen/strep to be used at passage 5 or 6.
Preparation of the fibrin glue containing cells
To seed and seal the meniscus cells and hMSCs inside of the meniscus scaffold, a commercially available clinical grade fibrin glue kit (Tisseel, Baxter) was used, consisting of two components: fibrinogen and thrombin used 1:1. When fibrinogen or thrombin is mentioned, it concerns specifically one of the two components, whereas fibrin glue refers to the complete product. Fastgreen (Merck, Germany) was dissolved in PBS with a concentration of 0.4 mg/mL and filter sterilized. Cells were trypsinized, spun by centrifugation for 5 min at 300 g, and resuspended in this solution in combination with the fibrinogen and stored in a syringe with a final cell concentration of 3.0 × 106 cells per 1 mL of fibrin glue, meaning 6.0 × 105 meniscus cells and 2.4 × 106 MSCs/mL.
The 20% meniscus cells and 80% MSCs was chosen based on previous cocultures of meniscus cells and MSCs. 15 Production of tissue, most comparable with native meniscus tissue, was shown using the combination of meniscus cells and MSCs in this ratio. Besides, 20% meniscus cells is a clinically feasible percentage for performing a one-stage procedure.
Surgical procedure
Arthroscopy of nine fresh frozen knee joints was performed by two orthopedic surgeons, using standard instrumentation and technique with routine anterolateral and anteromedial portals, creating a full thickness meniscus defect both on the medial and lateral side with a defect size between 2.5 and 3 cm. A rim of the meniscus, the anterior, and posterior roots were preserved for attachment of the meniscus scaffold during implantation. The meniscus scaffold was fixed to the rim of the meniscus using two inside-out 2-0 FiberWire® Meniscus Repair Needles (Arthrex, Naples, FL). In each knee joint the two different cell-seeding procedures were performed, meaning that both procedures were executed four times on both lateral and medial sides.
Two methods of cell seeding were applied in this study:
Dry seeding: after measuring the defect size, the meniscus scaffold was trimmed to the appropriate size and the first 0.5 mL of the fibrinogen (containing the cells as described previously) component was injected into the scaffold followed by injection of the thrombin component, both using a 23-gauge needle. Afterward, the seeded meniscus scaffold was transferred to the portal, by using a clamp and sutured to the meniscus rim, without stopping the saline flow (Fig. 1A–C). Wet seeding: for this procedure the meniscus scaffold was first surgically implanted and sutured as described earlier, and the cells were injected afterward. To prevent the cells from washing out, the flow of saline from the arthroscopy was stopped during the injection of the cells. Three different locations (to distribute the cells throughout the complete implant) were chosen to inject the cells with a 18-gauge spine needle (6.00IN 1.2 × 152 mm; Becton, Dickinson and Company, Franklin Lakes, NJ) through the contralateral portal of the meniscus defect, where the 0.5 mL cell suspension in fibrinogen was injected, the needle was left at the final injection location, and the syringe was changed to one containing 0.5 mL of thrombin, which was also injected at the three locations (Fig. 1D–F).
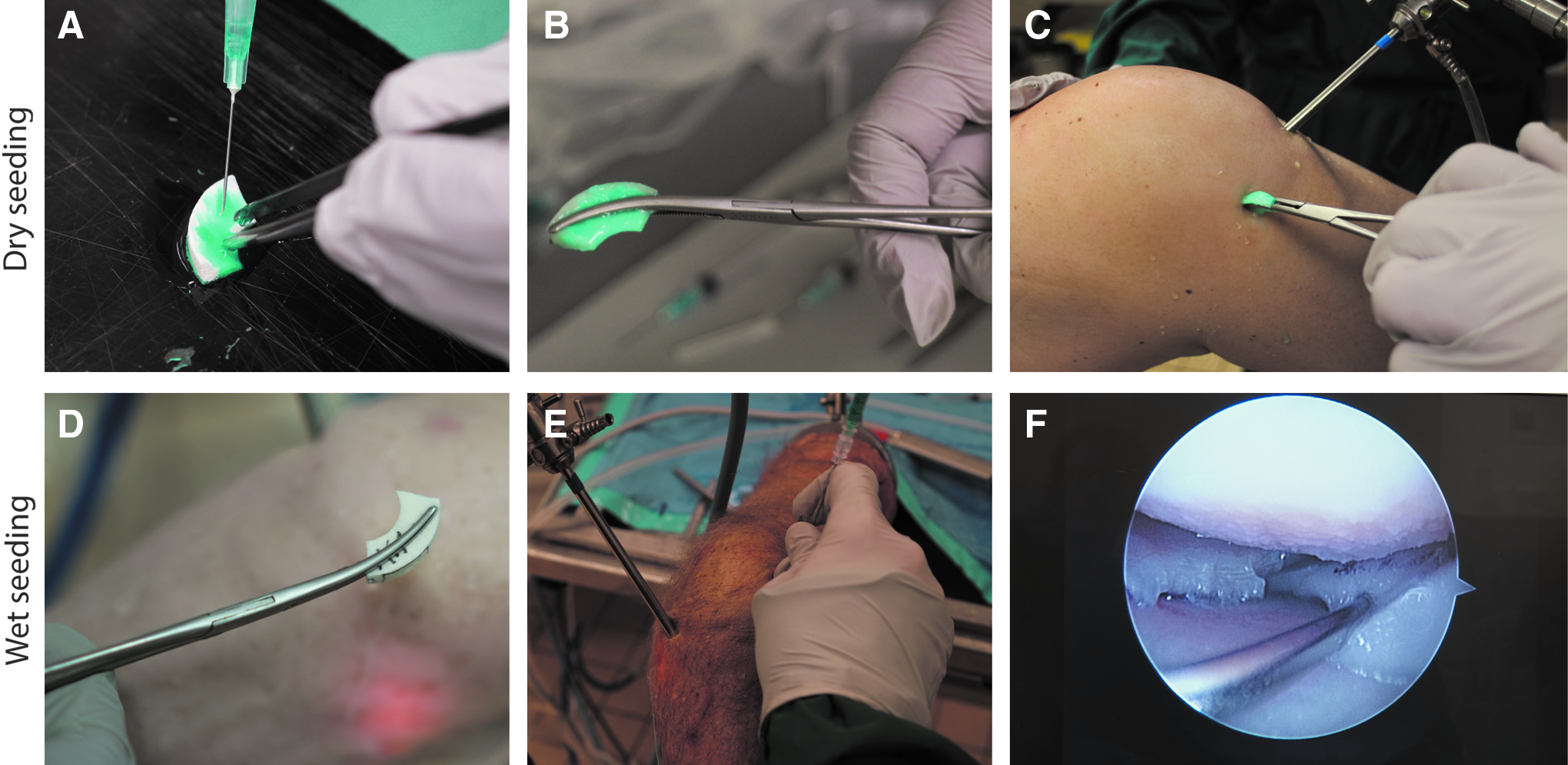
Different seeding methods. Dry seeding was performed by injection of the fibrinogen, which contained the cells, and was stained with fast green
Assessment of macroscopic pictures
After the two procedures were performed, the knee was opened and macroscopic pictures of the joint with the implants were taken. Because the fibrinogen component of the fibrin glue was stained with fast green, it was possible to macroscopically visualize the amount of leakage and distribution of the fibrin glue.
Cell distribution and viability
Visualization of the cell distribution throughout the meniscus scaffold and measurement of cell viability between different seeding methods was performed by creating three-dimensional (3D) images acquired from a Leica SP8 confocal microscope. For three scaffolds per seeding method, the scaffold was cut in the sagittal plane in six pieces and imaged with the microscope, to include both the core of the scaffold, as well as the superficial zone. LIVE/DEAD assay was then performed to stain the cells present in the scaffold after the arthroscopic procedures. The six even pieces were incubated for 30 min with 0.5 μL/mL Calcein AM (Molecular Probes) and 1 μL/mL Ethidium homodimer-1 (Molecular Probes) in PBS. After washing with PBS, the pieces of meniscus scaffold were stained for 4 min with 100 ng/mL 4′,6-diamidino-2-phenylindole and washed again in PBS. Merged 3D images from the Leica confocal microscope with a mean depth of 178 μm (range 86.7–238.7) were analyzed using ImageJ to calculate the ratio of live and dead cells per image.
Assessment of cell amount after seeding
After confocal imaging the meniscus scaffold pieces were digested overnight at 60°C in papain. Before the picogreen DNA assay (Invitrogen), ethanol (EtOH) precipitation of DNA was performed on the papain samples to wash out the fast green. And then 25 μL 3 M sodium acetate and 725 μL 100% EtOH were added to 250 μL papain digestion and stored at −20°C overnight. The samples were then centrifuged for 30 min, the EtOH was removed, and the pellets were washed two times in 75% EtOH. Picogreen DNA assay was used according to the manufacturer's instructions to determine the DNA content of the meniscus scaffold after implantation into the knee. λDNA was used as a standard reference to calculate the DNA content at an excitation measured at 480 nm and emission set at 520 nm.
Surgical implantation evaluation
Feedback of the surgeons on their experience and the feasibility of the different procedures were reported after each surgical implantation.
Statistical analysis
The sample size, based on preliminary in vitro results of the different seeding methods, was calculated with nQuery Advisor® version 7.0. When using the mean difference and a significance level of 5% and a power of 80%, the required sample size was five procedures per seeding method. A paired Student's t-test was performed on the picogreen assay to compare the amount of DNA in the meniscus scaffold after the two different seeding methods. A one-way analysis of variance was used to calculate the amount of cells after digestion with different concentrations of Liberase. A p-value of <0.05 was considered significant.
Results
Optimal rapid digestion protocol for isolation of meniscus cells
After comparison of the three different concentrations of Liberase for digestion of meniscus tissue within 40 min at 40°C, there was no significant difference between the total amount of cells after digestion for the four different donors (mean 2.18 × 106 cells per gram tissue, range 2.17 × 105–5.23 × 106). The 0.05% Liberase group resulted in significantly more living cells than 0.025% (p = 0.0179). However, when compared with 0.0125%, there was no significant difference (Fig. 2). The percentage of living cells was the largest for the 0.0125% group, with no difference in cell number.
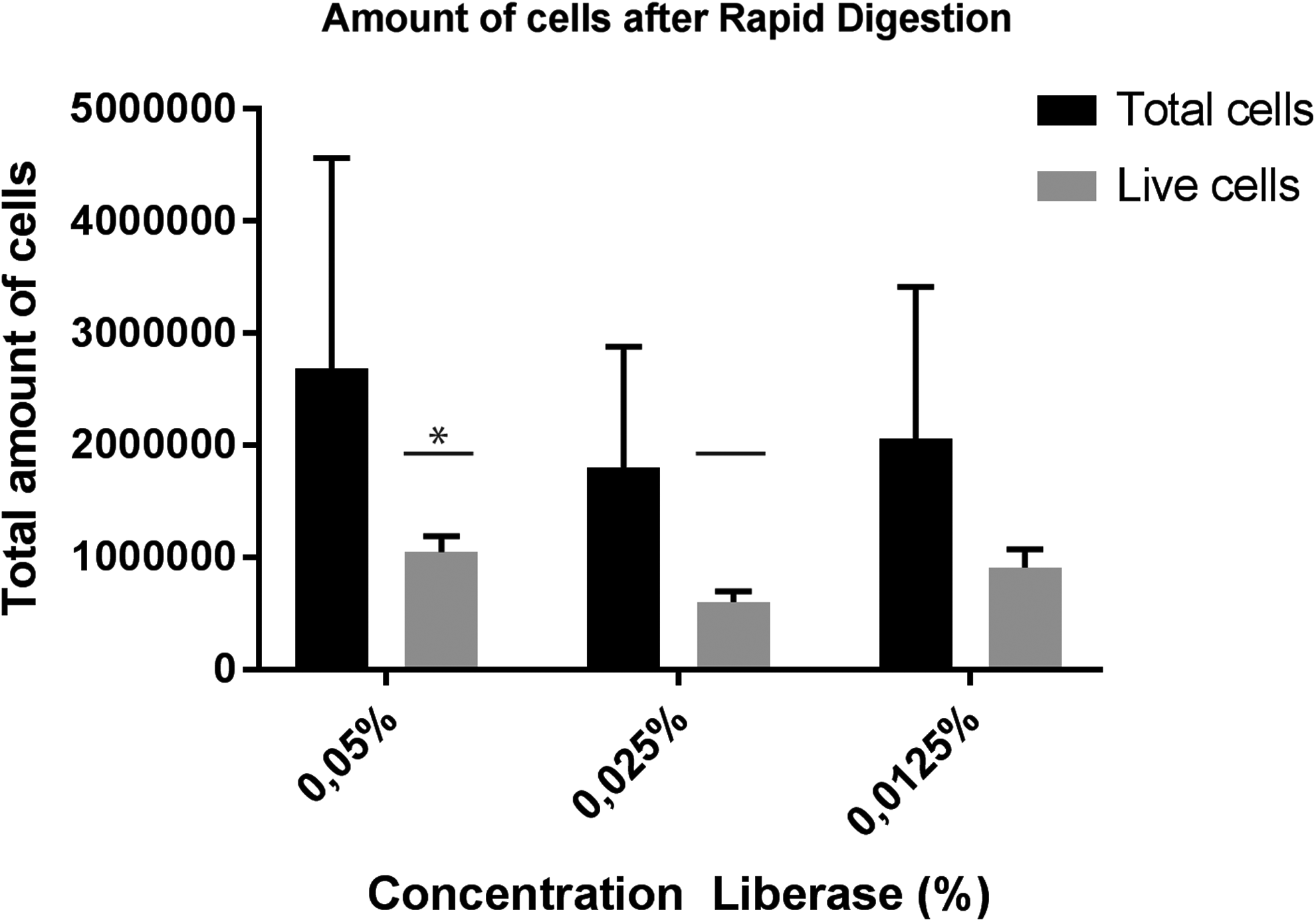
Cell counting after rapid digestion of meniscus tissue using 0.05%, 0.025%, and 0.0125% Liberase showed a significant difference in living cells between 0.05% and 0.025% Liberase, but not compared with 0.0125%. A significant difference with a p-value <0.05 is shown with asterisk.
Best seeding method for MSCs and meniscus cells in a CMI
In the macroscopic images of the human knees, the amount of fibrin glue, containing the cell suspension of 20% meniscus cells and 80% MSCs, inside the meniscus scaffold is shown by the amount of fast green staining (Fig. 3). Dry seeding shows a brighter staining of the fast green in the meniscus scaffold and a more homogenous distribution (Fig. 3A, C) than wet seeding (Fig. 3B, D). After injection of the fibrin glue in the wet seeding method, Figure 3D shows leakage of the fibrin glue into the joint instead of the meniscus scaffold. A clear difference in fast green staining was observed in the sagittal planes of the meniscus scaffolds for dry (E) and wet (F) seeding. Macroscopically, the dry seeding method demonstrated a higher amount of fibrin glue throughout the entire construct.
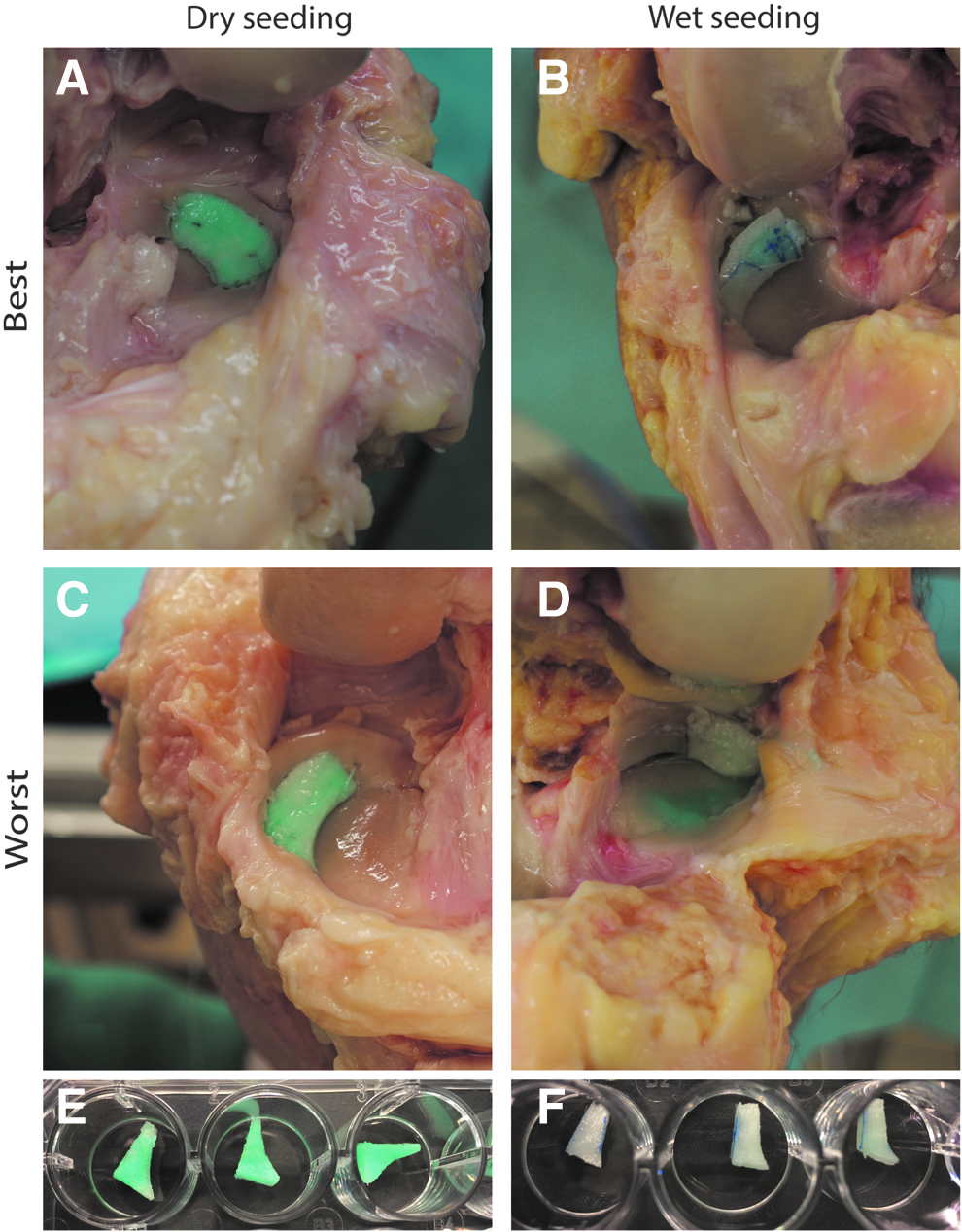
Pictures showing a meniscus defect replaced with the CMI in a human cadaveric knee with the most efficient seeding after both dry
After EtOH precipitation of DNA on the papain-digested tissue, the picogreen assay (as quantification for the amount of cells) showed a significant difference between the amounts of DNA in the two seeding methods (p = 0.0096), in favor of dry seeding (mean 4800 ng, standard deviation [SD] 1935) compared with wet seeding after implantation (mean 2928 ng, SD 1223) (Fig. 4).
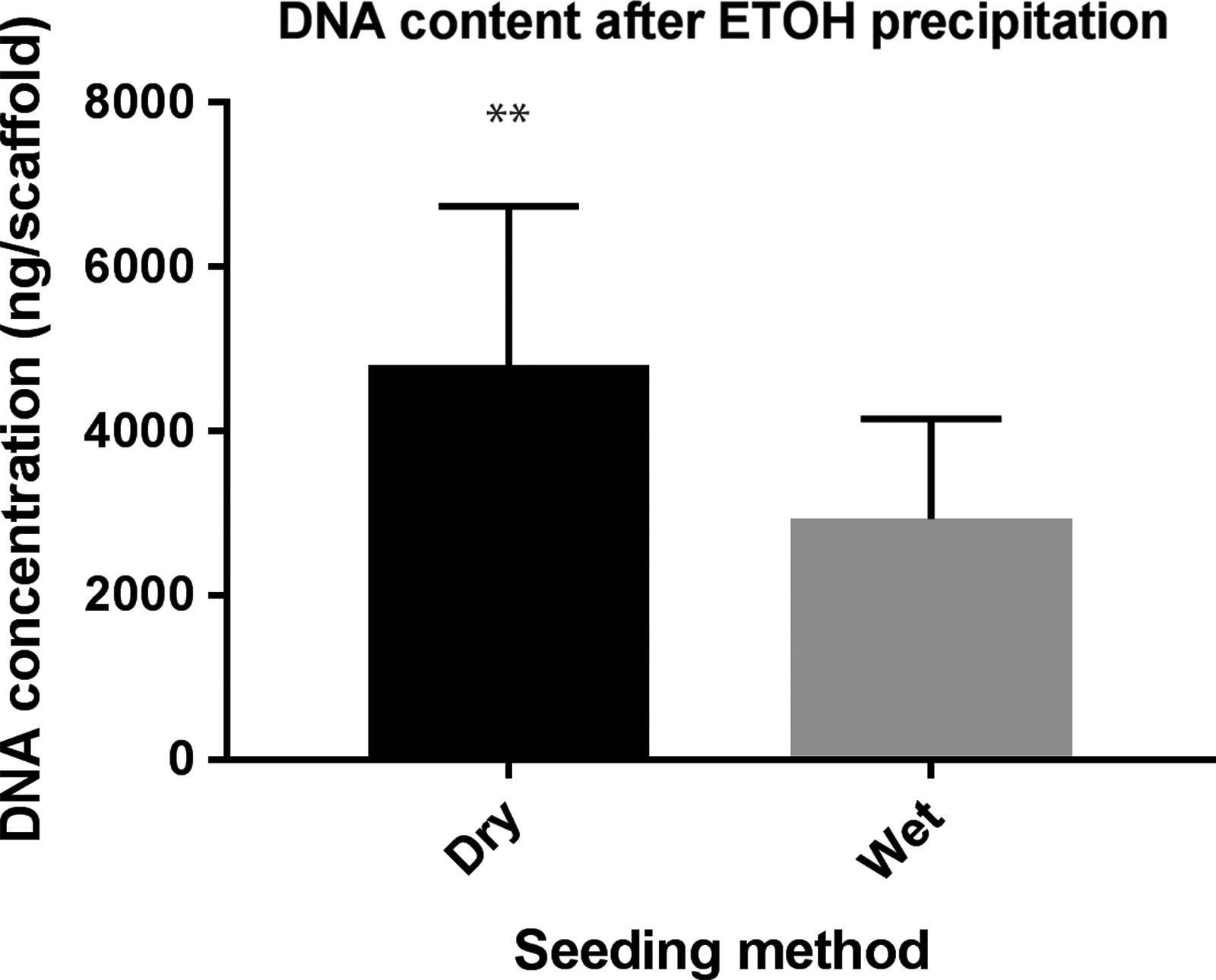
Picogreen assay showed a significant higher DNA content in the preseeded CMIs than in the CMIs seeded after implantation after EtOH precipitation (p = 0.0096). A significant difference with a p-value <0.01 is shown with **. EtOH, ethanol.
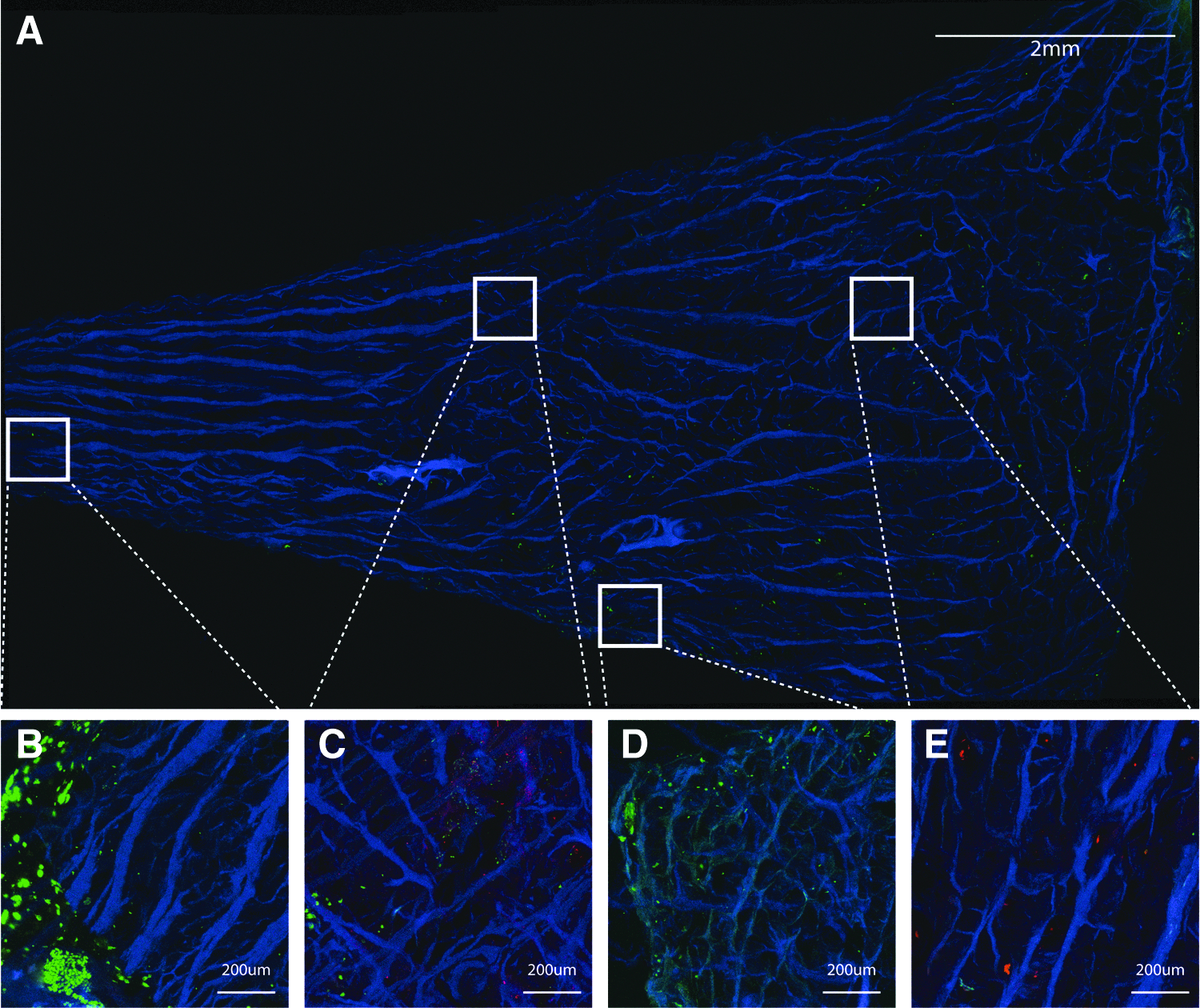
Confocal imaging of the meniscus scaffolds after implantation showed even distribution of the cells throughout the meniscus scaffold when dry seeding was used (Fig. 5A). Some areas contained fewer cells than other, but the overall distribution was acceptable (Fig. 5B–E). Around the meniscus scaffold, a layer of fibrin glue containing cells was formed. In contrast, the cell distribution was less homogenous for wet seeding (Fig. 6A, B, D, E), and damage of the meniscus scaffold was observed at the location of needle injection (Fig. 6C). When processing the confocal images with ImageJ (z-stacks of 270 μm), dry seeding demonstrated 305.8% more cells than the wet seeding, with 99.3% and 99.5% living cells, respectively.

Merged confocal image after preseeding of the CMI. The CMI is stained with DAPI (blue) and the cells for live/dead assay, showing the cell distribution throughout the CMI
Merged confocal image of the CMI seeded after implantation. The CMI is stained with DAPI (blue) and the cells for live/dead assay, showing the cell distribution throughout the CMI
Discussion
This study demonstrated the feasibility of combining recycled autologous meniscus cells and allogeneic MSCs in a meniscus scaffold during an arthroscopic one-stage procedure for meniscus regeneration. Rapid digestion of meniscus tissue with 0.0125% Liberase resulted in sufficient living cells for a 20:80 ratio with allogeneic MSCs during a one-stage procedure. Both seeding methods did not affect cell viability, but dry preseeding of the meniscus scaffold resulted in more cells, and a better distribution of the cells in the scaffold, than wet seeding after arthroscopic implantation.
Feedback of the surgeons suggested the surgical procedure of dry seeding to be more feasible in clinical practice. The structure of the meniscus scaffold does not seem to change after seeding; therefore, the implantation of a seeded meniscus scaffold is not different from the implantation of an unseeded scaffold. Moreover, it is relatively easy to seed the cells inside of the meniscus scaffold outside of the knee in a dry environment, and no additional damage is administered to the scaffold during the dry seeding procedure, compared with the wet seeding.
However, logistically, for a single-stage procedure, dry seeding is less efficient than wet seeding. After performing the partial meniscectomy, the tissue will be subjected to enzymatic digestion and washing steps to isolate the meniscus cells and mix them with “off-the-shelf” allogeneic MSCs in fibrin glue, which takes about 90 min in total, 60 min between start of the operation and seeding of the cells. In the interim, the surgeon can implant the meniscus scaffold in the defect and seed afterward, when using wet seeding, which will lead to a time of 50 min between start of the procedure and injection of the cells. In contrast, when applying dry seeding, the surgeon must wait until the cell mixture is prepared before continuing the surgery.
However, a disadvantage of seeding the scaffold after implantation is the saline present in the knee joint, preventing a good distribution of cells throughout the scaffold because of its sponge-like character. It is possible to completely drain the knee from saline to inject the meniscus scaffold in a nonaqueous environment, but the visibility for the surgeon will be suboptimal, making it less suitable to inject the cells reproducibly. Even when the flow is paused to prevent washing out the cells, it is difficult to determine whether the needle is inside of the scaffold, or already in the outer rim of the meniscus.
To date, an optimal cell density for regenerative medicine is not yet described. The total amount of cells seeded into the meniscus scaffold was based on the IMPACT trial (NCT02037204) 13 and in autologous chondrocyte implantation (ACI) for cartilage defects, 19 where ∼2.0 × 106 cells/cm2 are used. Both ACI and the IMPACT trial have demonstrated good results for cartilage regeneration using this cell concentration of either chondrocytes, or the combination of chondrons and hMSCs.13,14,19 Other cell-based treatments for meniscus regeneration show a wide variance in number of cells used, depending on the strategy to accomplish meniscus regeneration. 20 In small and large animal models, 0.5–5 million and 15–150 million cells were used, respectively. However, most of these methods included intra-articular injections, which seem to require a larger number of cells than local application with seeding a scaffold with the cells.
In animal models, meniscus regeneration methods in which a scaffold was used, cell concentrations ranged between 1.0 × 106 and 10.0 × 106/mL.21–24 A CMI seeded with meniscus cells and cultured in vitro for 3 weeks was implanted in sheep by Martinek et al., 11 with a seeding density of 10.0 × 106 cells per 3.25 cm CMI. Baker et al. 25 used a cell concentration of 5.0 × 106/mL for seeding a poly(ɛ-caprolactone) scaffold with human meniscus cells in vitro. Thus, even for the application of meniscus cells combined with a scaffold, cell concentrations vary widely and there is no consensus on the effect of a higher number of seeded cells. Furthermore, a higher cell concentration may not translate to a higher cell density after seeding. Equally high seeding efficiencies were shown by Weinand et al. 26 for cell concentrations of 1.0 × 106 and 2.0 × 106/mL compared with 5.0 × 106/mL when oscillating seeding of the Vicryl scaffold was used.
Nevertheless, this study showed a significant difference in seeding efficiency between the two different seeding methods, using the same cell concentrations, resulting in 99% living cells inside of the scaffold. A 20:80 ratio of meniscus cells and MSCs were used, which is clinically feasible as enough autologous cells can be isolated. For a defect of 2.5 cm, 0.65 g of tissue can be harvested (data not shown) resulting in ∼600,000 meniscus cells. A 2.5 cm defect is comparable with 30% of the meniscus scaffold, meaning 2.0 × 106 cells in total and 400,000 meniscus cells are needed. Overall, this indicates that the current cell yield after rapid digestion is sufficient for this procedure. The combination of the 20% autologous meniscus cells with 80% allogeneic MSCs makes this procedure suitable for a one-stage operation. First, there is no additional operation needed to harvest and expand autologous MSCs from bone marrow of the patients, making it a two-step procedure and increase costs considerably. 27 Second, we think that using allogeneic MSCs instead of autologous will lead to better tissue regeneration by the secretion of trophic proregenerative factors and anti-inflammatory factors.14,28,29
For this study, a standard fluid arthroscopy of the knee was performed. Carbon dioxide (CO2)-insufflated arthroscopy is also described for the knee, and could be used during the seeding procedure after implantation of a meniscus scaffold.30,31 Vascellari et al. 30 described the combination of a standard arthroscopy for the debridement of the cartilage defect, and preparation of the graft for matrix-induced autologous chondrocyte implant followed by a CO2-insufflated arthroscopy for implantation of the graft using fibrin glue. 27 No adverse events or complications related to the surgery were observed during the surgical procedure and follow-up period. In addition, the visualization during CO2 arthroscopy is similar compared with arthroscopy with saline inflow. This indicates CO2-insufflated arthroscopy could be safe and might be an option for seeding cells after fixation of the meniscus scaffold. However, during injection of the scaffold after implantation, it was not only difficult to inject the meniscus scaffold with cells due to the sponge-like character after soaking in saline, it was also difficult to determine whether the needle was in the scaffold or already in the outer rim of the meniscus. This problem would not be solved by using CO2-insufflated arthroscopy.
Rapid enzymatic digestion of meniscus tissue is performed on manually minced pieces of meniscus with an approximate size of 1 to 2 mm2. Automated mincing of the meniscus tissue is faster, could possibly lead to a higher cell yield, and could shorten digestion time because the smaller pieces would allow the Liberase to further penetrate the each fragment of tissue and improve the digestion effectivity. 32 Therefore, automated mincing could potentially accelerate the time needed for the one-stage procedure for meniscus regeneration. To the best of our knowledge, there is nothing known on combining automated mincing of tissue with enzymatic digestion for cell isolation.
Limitations
Several limitations to this study could be identified. First, the number of cells after rapid digestion was calculated per 1 g of meniscus tissue. However, the amount of tissue retrieved from partial meniscectomy was not standardized. Nevertheless, when 2.0 × 106 cells/cm2 were used, such as during ACI, 1.2 × 106 meniscus cells are needed to fill a defect comprising an entire meniscus scaffold. The amount of fibrin glue and number of cells are proportional to the percentage of scaffold used for the defect. This target should be reached, even when accounting for the lowest amount of received tissue during partial meniscectomy. Likewise, there was a broad range in the number of isolated cells within the same concentration of Liberase. This could be due to quality of meniscus tissue, which we received from patients undergoing a total knee arthroplasty.
Second, the fibrinogen and thrombin for this study were added consecutively instead of simultaneously through the DuoSet device, which is advised for the usage of fibrin glue. When injecting the fibrin glue inside of the meniscus scaffold, more pressure is needed than when injecting it on a surface. This is especially relevant for the 18-gauge spine needle, as when the two components are mixed inside of the needle, it will clog, making it impossible to inject the two components at the same time. To be able to compare the different seeding methods, dry seeding was performed using the two components consecutively as well. Moreover, in in vitro studies this method of cross-linking is often used and validated. 33 Therefore, we assume this injection method of fibrin glue will not affect the cross-linking process of the fibrin glue inside of the meniscus scaffold.
Finally, in this study, only the procedure of implanting and seeding a meniscus scaffold was examined, but the knees were not stressed with mechanical loads or motion. Therefore, we have no information on the (sheer) force in the fibrin glue containing the cells in the scaffold. However, since the treatment after closure of the knee was the same in both seeding methods, this was not relevant to the results of this initial study.
In conclusion, this study demonstrates that living human meniscus cells can be isolated efficiently, combined with MSCs in 20:80 ratio, and uniformly delivered into a currently available meniscus scaffold. This scaffold can then be arthroscopically implanted, creating a one-stage solution for partial meniscal deficiency.
Footnotes
Acknowledgments
The authors thank Smith&Nephew for research funding and providing the arthroscopy tower and devices, Stryker for research funding, Arthrex and iMove Medical for providing research material, and Simon Plomp for his kind assistance at the anatomy department.
Disclosure Statement
M.H.H., L.A.V., and D.B.F.S. received research funding from Smith&Nephew and Stryker for this study, and materials were provided by Stryker, Arthrex, and iMove Medical.