
Abstract
Pneumatic extrusion-based three-dimensional (3D) printing can be used to fabricate custom-made scaffolds to restore irregular bone defects. During the 3D printing process, therapeutic agents can be added to the scaffolds. This study aimed to develop a polycaprolactone (PCL) scaffold loaded with Ag3PO4 to prevent infections and lidocaine for pain relief by one-step 3D printing. We hypothesized that the drug release could be controlled by varying the filament diameter of the 3D printed scaffolds. To this end, PCL slurry mixed with different amounts of silver phosphate and lidocaine was printed via differently sized nozzles. The obtained cylindric scaffolds displayed a porous interconnected microstructure with high fidelity. The Ag3PO4 and lidocaine were distributed homogeneously. The lidocaine release could be controlled by adjusting the filament diameter while the silver release is correlated with the Ag3PO4 loading amount. The released medium from silver-loaded scaffolds exhibited an obvious inhibition zone against Staphylococcus aureus and Escherichia coli upon loading with 1% Ag3PO4 for up to 6 days and with 3% Ag3PO4 for at least 7 days. Cytotoxicity of all scaffolds was screened by cell assay. In conclusion, the pneumatic extrusion-based 3D printing provides a practical technique to fabricate drug-loaded scaffolds. The Ag3PO4 and lidocaine loaded PCL scaffolds showed the potential for infection prevention and pain relief.
Impact Statement
The manuscript describes the possibility to incorporate bioactive agents, that is, Ag3PO4 and lidocaine, into polymeric scaffolds via a novel three-dimensional (3D) printing technique. Lidocaine release can be controlled by adjusting the filament diameter of the scaffolds while silver release is correlated with the loading amount. The released lidocaine reached concentrations far above the therapeutic threshold within 4 days, the released silver can prohibit bacterial growth for more than 6 days. These results indicate that the pneumatic extrusion-based 3D printing provides a practical way to fabricate bioactive scaffolds. This work will be interesting to researchers working to fabricate bioactive tissue engineering scaffolds.
Introduction
The restoration of the maxillofacial defects is a challenge because of the complicated pre-existing anatomy of the skull. 1 Recently, the advance in three-dimensional (3D) printing with computer-aided modeling techniques has enabled to create accurate scaffolds that contour to the patient's anatomical parts based on the 3D reconstruction of computed tomography (CT) scanning data.2,3 Based on the baseline technology, type of machine architecture, and the material transformation physics, 3D printing can be classified into five categories, that is, vat polymerization, powder bed fusion, material extrusion, material jetting and direct energy exposition. 3
The pneumatic extrusion method, a sub-category of material extrusion, is attractive for biomedical application as it requires only a small amount of materials, that is, in a few milligrams compared to a few hundred grams for other technologies. 3 Furthermore, it does not require an elevated temperature during the process, which is beneficial for the incorporation of biomolecules. During the 3D printing process, a viscous or semisolid slurry, made by mixing a solvent and polymer, for example, alginate, polycaprolactone (PCL), polyglycolic acid, polylactic acid and their copolymer poly (lactic-co-glycolic acid), is loaded into the syringe. 4 The applied pneumatic pressure can continuously extrude a microfilament from the viscous slurry via a fine nozzle. After the 3D reconstruction file is loaded to the 3D printer, the object can be precisely printed via controlling the movement of the syringe (x-, y-, z- motion). The printability of the slurry is controlled by parameters such as the slurry viscosity, nozzle diameter, the speed of nozzle movement and the pneumatic pressure. 5 The final architecture of the scaffold can be characterized by the shape of the micro-filament diameter, pore size and shape, total porosity, and pore interconnectivity, etc. 6
Such 3D designed polymeric scaffolds have the potential to restore and regenerate bone defects. The influence of 3D printed scaffolds on mineralization of the osteoblasts and osteogenic differentiation of stem cells has been studied previously.7–9 For instance, after culturing human adipose-derived stem cells on the 3D printed PCL scaffolds in osteogenic medium for 14 days, minerals were deposited throughout the pore spaces and along the filaments. 9 Similarly, after the 14-day culture of the preosteoblasts (MC3T3-E1) on the scaffolds, calcium deposition was observed.7,8 Furthermore, in vivo studies showed bone regeneration capacity of the 3D printed PCL-based scaffolds using animal models of calvarial defects.10–12
However, maxillofacial bone defects often originate from or are associated with infection, accompanied by bacterial colonization and inflammation. 13 Despite radical surgical debridement, removal of the infected area is often incomplete. 14 Consequently, the residual bacteria may attach to the restorative materials to form a biofilm, which are difficult to eradicate. 15 Over the past decades, attempts have been made to prevent and cure infections by incorporating antibiotics into the materials during either primary or revision surgery.16,17 However, the long-term patient exposure to low doses of antibiotics has a high risk of inducing antibiotic resistance. Alternatively, chemical agents such as silver have been used due to the much lower tendency to give rise to resistance. 18 For instance, silver phosphate (Ag3PO4) has been incorporated into polyurethane composites through an in situ forming method and exhibited strong antibacterial effects with satisfactory cytocompatibility. 19 To eradicate the organisms from infected surrounding tissues usually requires the release of effective antibacterial drugs for 3 to 4 days including a high initial burst release during the first 2 days. 20
In addition to the infection, postoperative pain is an unavoidable symptom. During the first postoperative 24 h, ∼40% of the patients reported moderate to severe postoperative pain. 21 Although the pain decreased with time, the management of the postoperative pain can be important at home as it will last longer than 24–48 h. Currently, the patients usually are administered strong pain killers, like opioids, to relieve the pain. 22 Although being effective, a large intake of opioids can induce respiratory depression, nausea, and vomiting. Therefore, multimodal analgesic regimens, such as local anesthetic-opioid combinations, have been proposed to control postoperative pain. 23 Particularly, continuous postoperative application of lidocaine longer than 24 h can have a preventive effect on the postoperative pain and reduce opioid consumption.24,25
For the above-mentioned reasons, it can be advantageous to incorporate both antibacterial and analgesic drugs in a bone scaffold to release drugs above the therapeutic thresholds. 3 In a microscale polymeric drug delivery system, the drug transport is primarily driven by diffusion. 26 Therefore, an important way to control the drug release is the alteration of the diffusion distance.27,28 Since the diffusion distance can be easily adjusted by modulating the filament diameter of the printed scaffolds, we hypothesize that the drug release rate can be changed by varying the filament diameter of the 3D printed scaffolds. However, no research work on this topic can be found in literature until now.
In this study, we aimed to develop a PCL scaffold loaded with Ag3PO4 to prevent infection and lidocaine for pain relief by one-step 3D printing. PCL was selected due to its biocompatibility and printability by a pneumatic extrusion method.5,29 The scaffold morphology, drug release profiles, antibacterial efficacy, and cytotoxicity were further evaluated.
Materials and Methods
Slurry preparation for printing
The slurries for printing were prepared by mixing PCL (Mn = 80,000 g/mol, Tm = 60°C; Shenzhen Esun Industrial Co, Shenzhen, China), lidocaine (Sigma-Aldrich, St. Louis, MO) and Ag3PO4 (Strem Chemicals, Newburyport, MA) in dichloromethane (Kelong Chemical Reagent Factory, Chengdu, China). All chemical reagents used in this research were of analytical quality. The sample groups were named as Drug0, L2, L4, Ag1, Ag3, and Ag3L4 based on the drug (lidocaine and Ag3PO4): PCL weight ratio (Table 1). Materials were dissolved for 2 h and stirred in a fume hood until a filament of around 20 cm in length could be extruded. The shear viscosity of the slurry was further determined by a viscometer (NDJ-9S digital viscometer; Vetus Electronic Technology, Hefei, China) at a rotation speed of 1.5 rpm at 25°C. A proper shear viscosity of the slurry for the extrusion of filaments had to range from 0.25 to 0.35 Pa·s.
The Composition of the Slurry for Printing in Different Groups
PCL, polycaprolactone.
Scaffold fabrication
The scaffolds were printed using a pneumatic extrusion-based 3D printer (Regenovo 3D Bioprinter, Hangzhou, China). The 3D printer was composed of a nozzle-connected printing head (syringe), pneumatic pressure controller and three-axis (x, y, z Cartesian coordinates) linear motion controllers. A digital file of a disc model (15 mm in diameter and 1.5 mm in thickness) was transferred to the printer, as the designed shape for the 3D printed samples. During the printing process, the slurries were delivered through a nozzle (0.21 or 0.41 mm in diameter) at a speed of 4 mm/s with a constant pressure of 450 kPa. The slurries were laid down in a layer-by-layer manner to form the scaffolds, which were further labeled with 0.21 and 0.41, respectively. A degree of 90 was set between the lower and upper layers to generate a latticed pattern. The 0.41 scaffolds were printed with an x- or y-motion step of 0.7 mm and a layer thickness of 0.2 mm (z-motion), while the 0.21 scaffolds were printed with an x- or y-motion step of 0.5 mm and a layer thickness of 0.1 mm. The printing was conducted under ambient conditions. After printing, all scaffolds were further dried in the fume hood overnight and then vacuum-dried for another 12 h.
Morphological characterization
The morphology of the scaffolds was assessed by scanning electron microscopy (SEM, JEOL 6500LV; JEOL, Tokyo, Japan). All samples were sputter-coated with a thin layer of gold before observation. The diameter of the filaments was quantified from four different SEM images at 35 × using Fiji software (NIH, Bethesda, MD). The scaffolds were cross-sectioned to further observe the drug status in the filaments. Energy Dispersive X-ray spectroscopy (EDX) (Oxford Instruments, Abingdon, United Kingdom) was applied for analysis of elemental composition of the filaments. The 3D structure was reconstructed following micro-CT scanning (μCT40; Scanco Medical, Brüttisellen, Switzerland). The samples were scanned at 45 kV and 175 μA with a slice increment of 19 μm. The 3D images were reconstructed from a series of serial 2048 × 2048 bitmap images using Software CTAn and CT Vol Realistic 3D Visualization (Bruker microCT, Kontich, Belgium).
Drug release
Disk samples (n = 5 of each type) were weighed and placed into 15 mL Falcon™ conical centrifugal tubes containing 10 mL phosphate buffer saline (PBS; Gibco™, Invitrogen Corp., Paisley, Scotland). The tubes were incubated at 37°C with gentle agitation. At each predetermined time point, that is, after 1, 2, 6, 24, 48, 96, and 168 h, all supernatants were collected for further analysis and the tubes were refreshed with 10 mL PBS.
The concentration of lidocaine was detected by reverse-phase high-performance liquid chromatography (HPLC) according to a previously reported method. 30 The HPLC system consisted of a L-2130 pump (Hitachi, Tokyo, Japan), a L-2400 UV detector (Hitachi), a L-2200 autosampler (Hitachi), and a LiChrospher RP-18 endcapped HPLC column (125 × 4 mm, particle size 5 μm; Sigma-Aldrich). For lidocaine detection, the used mobile phase was acetonitrile: ammonium acetate (0.0257 M), pH 4.85 (adjusted with acetic acid) in the ratio of 60/40 (v/v). The injection volume was 20 μL with a flow rate of 0.5 mL/min. The concentration of lidocaine was quantified at 254 nm using a standard calibration curve in the concentration range between 4 and 1000 μg/mL.
The silver concentration in the collected supernatants was determined by atomic absorbance spectroscopy (AAS, SpectrAA 220FS; Varian, Palo Alto, CA). The collected supernatant was acidified using 65% nitric acid (Aladdin, Shanghai, China) to a 1% nitric acid solution before AAS analysis. A standard calibration curve was prepared with silver concentrations ranging from 8 to 1000 ng/mL.
Antibacterial property
Disk samples (n = 3 for each type) were immersed in 1.5 mL of PBS with gentle agitation at 37°C. The supernatants were collected daily for 7 days and stored respectively. Then 1.5 mL fresh PBS was added. Filter papers, 6-mm in diameter, were immersed into the collected supernatants for 30 s and subsequently air dried for further use. A zone of inhibition test (modified Kirby–Bauer test) was adopted to evaluate the antibacterial property of the filter papers against Staphylococcus aureus (ATCC® 25923™, Manassas, VG) and Escherichia coli (ATCC 25922™). Standard tablets containing 30 μg of cefoxitin were used as positive control. In brief, a bacterial suspension was prepared by mixing bacterial colonies with sterile saline (0.85% w/v NaCl in water) to an optical density (OD) value of 0.090 and further diluted for 10 times. The bacterial suspension was smeared evenly on nutrient agar plates (Jiangmen Caring Trading Company Limited, Jiangmen, China). Subsequently, three filter papers from different disk samples were distributed on each agar plate. After incubation for 20 h at 36°C, the diameters of the transparent zones of inhibition (ZOI) were measured.
Cytotoxicity
The cytotoxicity of the membranes was evaluated by the Cell Counting Kit-8 (CCK-8) assay.
31
All experiments were done by following national guidelines for working with human materials (Dutch Federation of Biomedical Scientific Societies, human tissue and medical research: code of conduct for responsible use. Available at
Human foreskin fibroblasts (HFFs, isolated from foreskin specimens from a healthy donor by following national guidelines for working with human materials) and MC3T3-E1 osteoblastic cells (ATCC) were cultured in αMEM cell culture medium (Gibco®) supplemented with 10% fetal bovine serum (Sigma F7524, Taukirchen, Germany) and 1% penicillin/streptomycin (Gibco) under a 5% CO2 atmosphere at 37°C.
The cells were seeded onto a 24-well plate with a cell density of 20,000 cells per well. After 24 h, the culture medium in the plate wells was replaced with the collected supernatants or 5% dimethyl sulfoxide (DMSO) groups (positive control) to start the evaluation. Again, 20 h later, the culture medium was refreshed with 1 mL culture medium containing 10 v/v% CCK-8 dye to measure the metabolic activity of the cells. After 2 h of incubation, a 100 μL aliquot of the metabolized medium from each well was transferred into a 96-well plate in duplicate and the absorbance was measured at 450 nm in a Synergy HTX multimode reader (BioTek Instruments, Winooski, VT).
Statistics
All data were reported as mean ± standard deviation. The data were analyzed by a two-way analysis of variance followed by a Tukey's multiple comparisons test using GraphPad Prism 5.0 (GraphPad Software, Inc., San Diego, CA). Furthermore, an independent t-test was performed to compare the cytotoxicity of drug-loaded groups to negative controls. Differences were considered as statistically significant at p < 0.05.
Results and Discussion
The fabrication of the scaffolds
To illustrate the pneumatic extrusion-based 3D printing, a cylindrical plate provided with a pillar was designed and printed (Fig. 1). All scaffolds, as used in the various assays, could be without any problems printed using a nozzle of 0.21 or 0.41 mm in diameter at a speed of 4 mm/s and a constant pneumatic pressure of 450 kPa under ambient conditions.
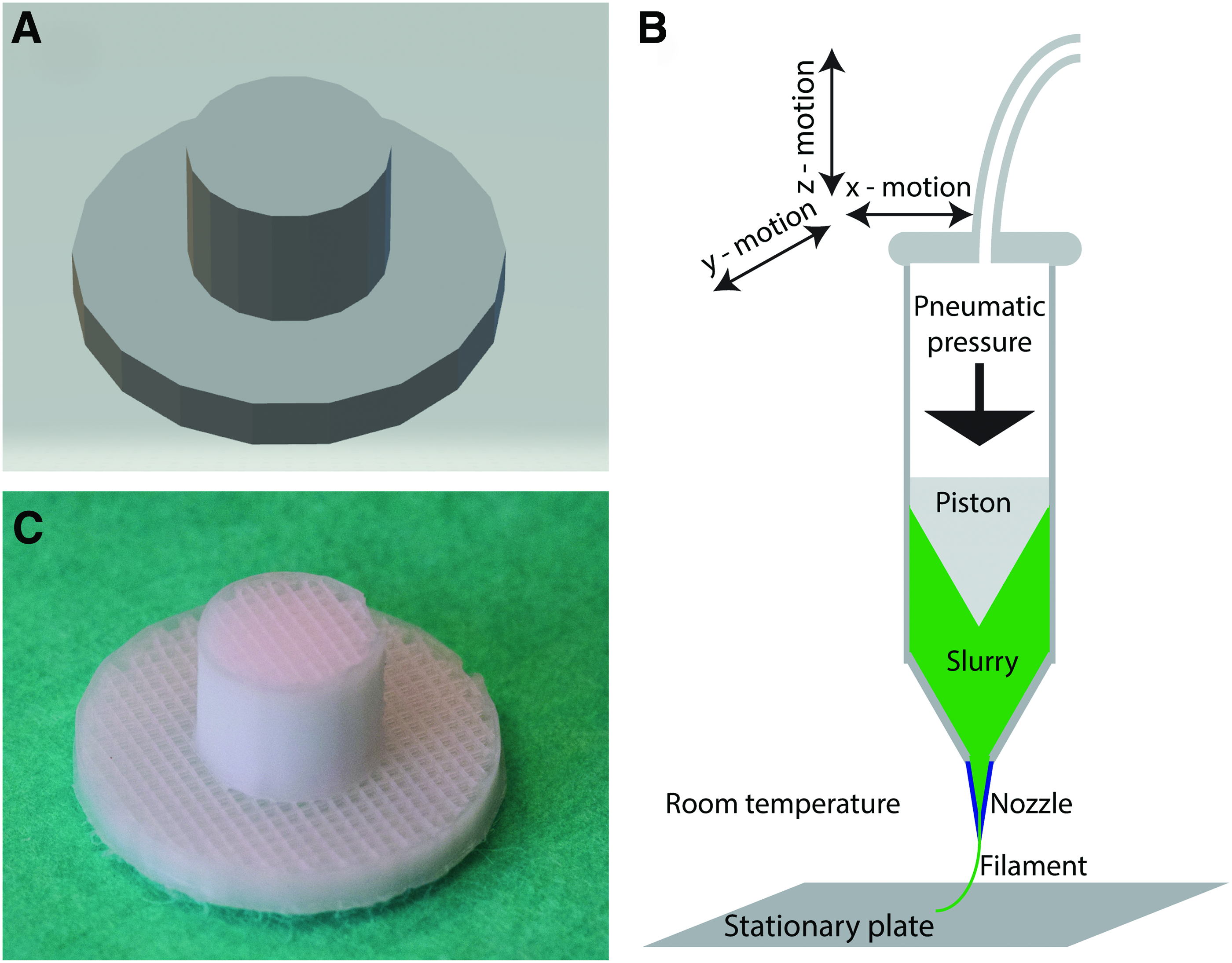
Schematic representation of the direct digital manufacturing process using an air pressure extrusion based additive manufacturing system.
Morphology of the scaffolds
Figure 2 shows the 3D structure of the scaffolds after micro-CT reconstruction. The scaffolds displayed a porous interconnected structure formed by microfilaments. The scaffolds prepared with the nozzle of 0.21 or 0.41 mm could easily be discerned from each other on basis of the filament diameter (Fig. 2). Further quantification of micro-CT data demonstrated that the surface area-to-volume ratios of the scaffolds from 0.21 to 0.41 groups were identical, both around 0.15/pixel.
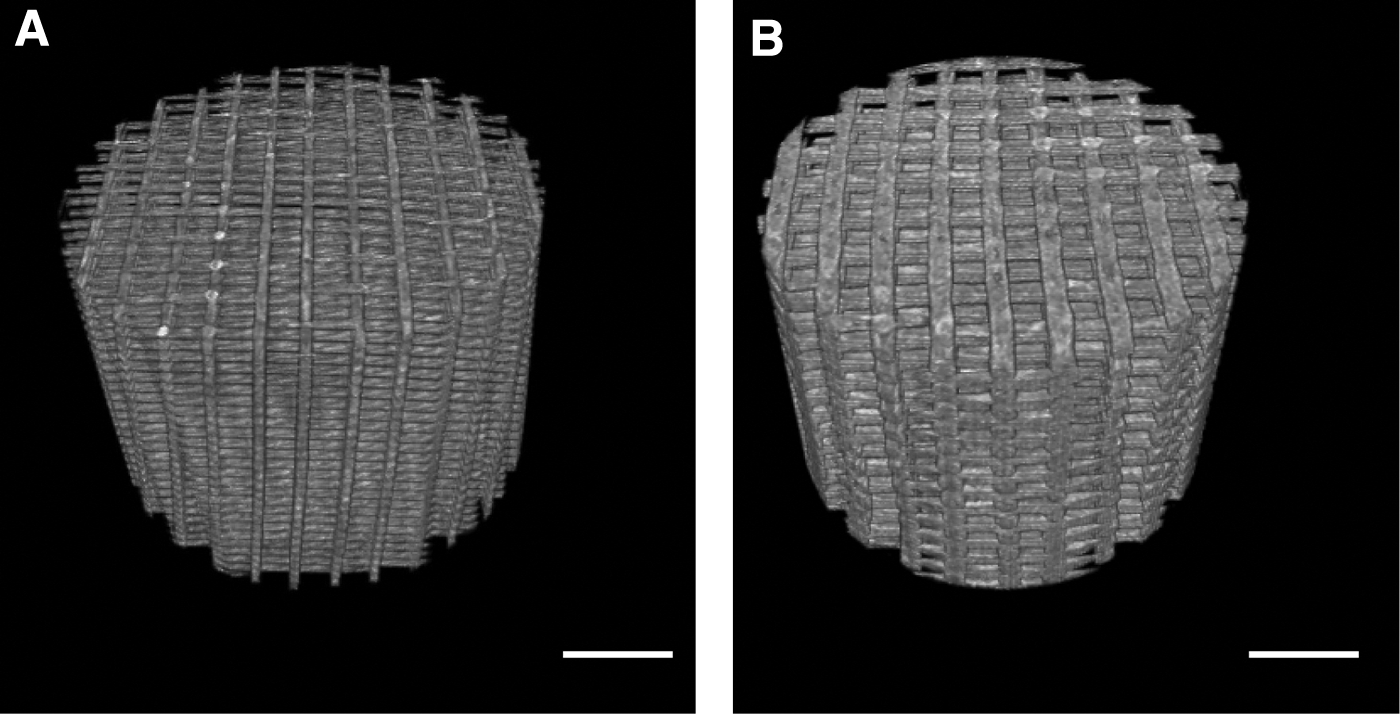
The structure of 3D printed scaffolds.
Since drug release is primarily driven by diffusion, the comparable surface areas of the scaffolds formed a sturdy basis for the further comparison on the effect of the filament diameter. The quantification of the filament diameter from SEM images (Table 2) confirmed that: (1) filament diameter of the 0.21 and 0.41 scaffold group was indeed different, that is, ∼73 and 144 μm, and (2) no significant differences existed in filament diameter among the different drug loaded groups printed with the nozzle of the same size. The observed discrepancy between filament diameter and the internal diameter of the nozzles may be due to the fluidal characteristics of the dissolved polymer. As soon as the polymer slurry leaves the tip of the nozzle, it will flow to a wider diameter till the solvent is completely vaporized and the polymer is stabilized again. This flow can even become increased by the constant pneumatic pressure in the delivery of the slurry.
The Filament Diameters of Scaffolds from Different Groups
The distribution of the lidocaine and Ag3PO4 throughout the filaments was analyzed by SEM-EDX, which confirmed that filaments contained silver (in red) and nitrogen (in green, indication of lidocaine). Elemental mapping demonstrated an even, spot-like distribution of the silver and lidocaine over the filaments (Fig. 3). The cross-section of the scaffolds (Fig. 4) showed that Ag3PO4, confirmed by EDX, embedded in PCL as microparticles, which still existed after 7-day immersion in PBS. No lidocaine particles were found in the lidocaine groups (Fig. 4B), indicating that lidocaine was dissolved by the organic solvent and dispersed in the filaments.

The morphology of the scaffold and the elemental distribution of lidocaine and Ag3PO4. The nitrogen was mapped in green to represent the lidocaine and the silver was mapped in red to represent Ag3PO4. Scale bar: 250 μm. Color images are available online.
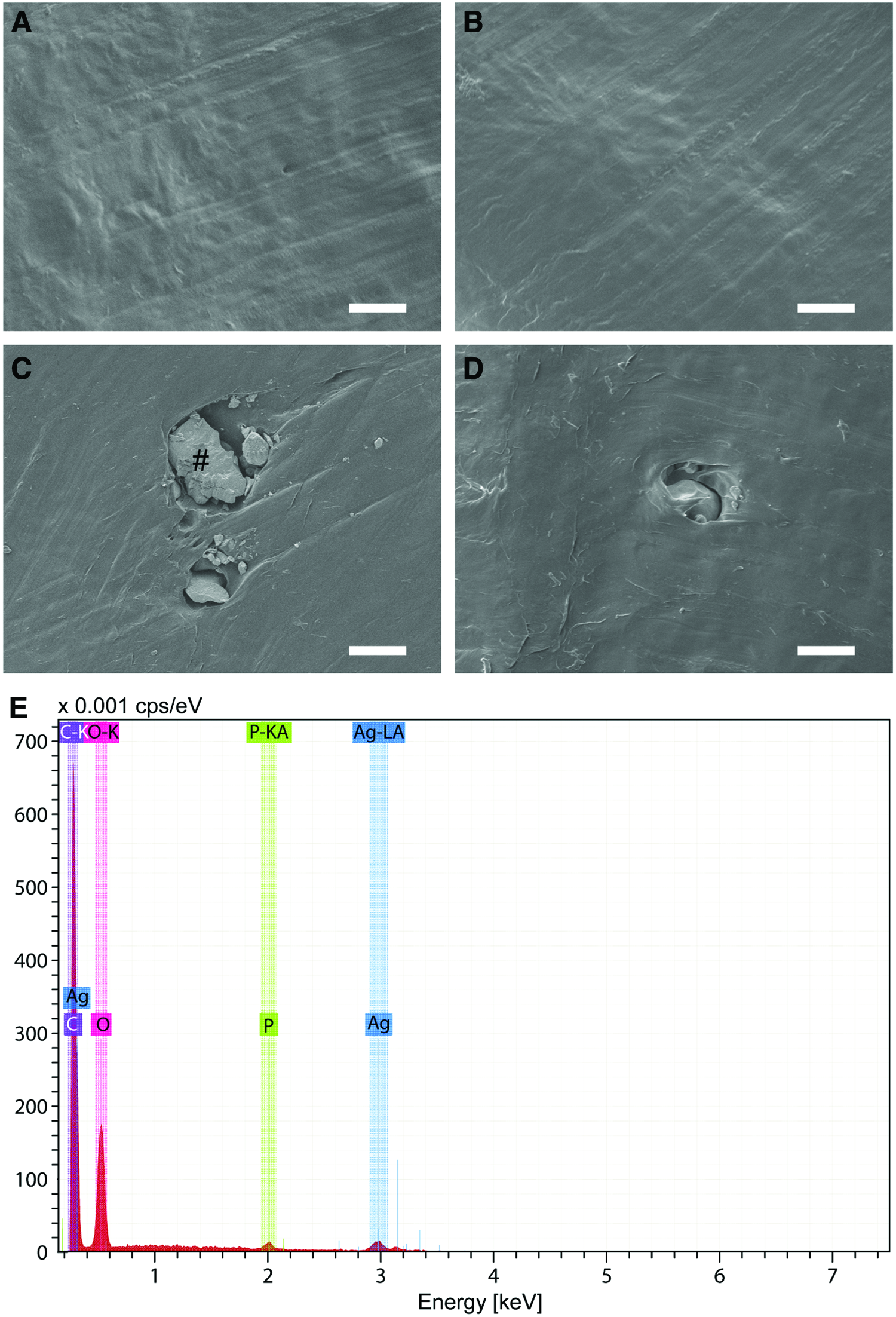
The cross-section of filament from
The drug release profiles
Figure 5A and B shows the release profile of the lidocaine from the various scaffolds. When the scaffolds were loaded only with lidocaine, the majority of the lidocaine was released in 6 and 24 h from 0.21 groups (0.21L2 and 0.21L4) to 0.41 groups (0.41L2 and 0.41L4), respectively. These results corroborate with the principles of diffusion-driven drug release. A decrease in filament diameter reduces the diffusion distance of the drugs. Notably, the dual loading of lidocaine and Ag3PO4 resulted in a delayed release of lidocaine at 48 and 96 h for the 0.21Ag3L4 group and the 0.41Ag3L4 group, respectively. This effect may be due to the increased diffusion distance as the embedded lidocaine needs to bypass the Ag3PO4 particles.

The release profiles of the lidocaine
Since the postoperative pain is greatest during the first 24–48 h and will decrease with time 21 and the lidocaine-loaded scaffolds displayed a controlled release of lidocaine within 4–7 days, these scaffolds may well be a candidate to control postoperative pain. As the diameter of the nozzles, used in this study, did have the most commonly used nozzle diameters, that is, 0.2 to 0.4 mm, for pneumatic extrusion, 32 it is possible to further control and optimize the lidocaine release by using larger custom-made nozzles. Such larger tip diameters may also be beneficial to deliver other bioactive compounds for biomedical applications.
The silver release profiles are displayed in Figure 5C and D. Generally, the silver showed a sustained release pattern for all silver-loaded groups. The sustained silver release profiles indicate that the Ag3PO4 loaded scaffolds can work as a depot to release silver ions in a long-term, that is, at least 7 days, which may be paramount to exert long-term antibacterial functions. Comparing the 0.21 with 0.41 groups, that is, 0.21Ag1 versus 0.41Ag1 and 0.21Ag3 versus 0.41Ag3, no significant difference was found. This suggests that filament diameter did not play a key role in the silver release. Instead, comparison of the scaffolds with different Ag3PO4 amounts, the Ag1 groups (0.21Ag1 and 0.41Ag1) showed a significantly faster release rate than the Ag3 groups (0.21Ag3 and 0.41Ag3) but fewer silver amounts were released from the Ag1 groups than from Ag3 groups.
Moreover, the Ag3 groups (0.21Ag3 and 0.41Ag3) showed a similar release profile with Ag3L4 groups (0.21Ag3L4 and 0.41Ag3L4). This result indicates that the further incorporation of lidocaine did not affect the silver release. Therefore, the data indicate that the silver release is correlated with the initial amount of Ag3PO4 as loaded in the scaffolds instead of the filament diameter. This discrepancy between lidocaine and silver release may be attributed to the different status of the drugs in the filaments, that is, lidocaine was dispersed as molecules while Ag3PO4 was embedded as microparticles in the filaments (Fig. 4). When the scaffolds were immersed in the release medium, lidocaine molecules are ready to be spread out, but the release was limited by the diffusion distance, which is related to the filament diameter. In contrast, the silver ions need to be firstly dissolved from Ag3PO4 particles and then diffused out of the filaments. The dissolution of silver ions from the Ag3PO4 particles is slow 19 and thus dominated the silver release. As such, the silver release was mainly correlated with the Ag3PO4 loading amount instead of the filament diameter.
In this study, PBS was used as the release medium considering that PBS is the most simple and common medium for the release kinetics studies. However, the scaffolds will be subjected to completely different conditions when implanted into the body tissues, where the released drug is continuously diluted and undergoes protein binding. As a consequence, different drug release behavior and performance can occur under in vivo conditions than observed in the in vitro release studies. 33 Therefore, despite the promising drug release profiles, data must be interpreted with care and in vivo studies are necessary to confirm the obtained data and prove the clinical potential of the designed scaffolds.
The antibacterial efficacy
S. aureus and E. coli are two representatives of common gram-positive and gram-negative bacteria in infected wounds. The results of the zone of inhibition test against these two bacteria are shown in Figure 6. Only the samples containing silver showed a transparent (Fig. 6A). The ZOI against S. aureus was larger than against E. coli, which indicates that silver has a stronger effect against gram-positive bacteria than gram-negative bacteria (Fig. 6B, C). This is confirmed by Taglietti et al., who reported that the extra thick peptidoglycan layer of the cell wall in the gram-positive bacteria prevents the penetration of silver. 34 No significant differences in antibacterial effect were found between the silver-loaded groups (Fig. 6B, C).

The antibacterial results.
In addition, the comparable antibacterial efficacy of Ag3 and Ag3L4 groups (Fig. 6B, C) indicates that the loading of lidocaine did not affect the antibacterial efficacy of the silver-loaded scaffolds. Furthermore, the release media of Ag1 and Ag3 groups were further evaluated to 7 days (Fig. 6D, E). No significant difference was found between 0.21 and 0.41 groups. As expected, the Ag3 groups showed a larger zone of inhibition than Ag1 groups. At day 7, the released medium from Ag1 groups lost its antibacterial efficacy, while the Ag3 groups remained effective. Evidently, the silver-loaded scaffolds proved that the clearance of organisms from infected tissues usually requires the sustained release of effective antibacterial drugs for 3–4 days. 20 Therefore, under the current experimental conditions, the antibacterial properties of the silver-loaded scaffolds seem suitable to prevent infections.
The cytotoxicity of the scaffolds
Since higher concentrations of silver can induce cytotoxicity, 18 cytotoxicity of the samples was further tested. The cytotoxicity of the scaffolds was evaluated by the CCK-8 assay to evaluate the metabolic activity of HFFs and MC3T3 cells. Drug0 and 5% DMSO groups were set as negative and positive control, respectively. The results are shown in Figure 7. The 5% DMSO group resulted in a significant lower OD value for both cell types than the Drug0 group, which validated the test. No significant difference in cytotoxicity was found between 0.21 and 0.41 groups. Regarding the drug loading amounts, the lidocaine- or silver-loaded groups did not separately show any significant difference in cytotoxicity compared to the negative control, which indicates that the released lidocaine and silver ions after 24-h immersion did not reach the toxic threshold to HFFs as well as MC3T3 cells.

The cell metabolic activity test of the scaffolds.
The therapeutic threshold of lidocaine is around 1.5–6.0 μg/mL.35,36 Based on the release study, the released lidocaine from the L4 group was estimated to be around 800 μg/mL, which is far higher than the therapeutic threshold and thus implies the potential to control pain. In contrast, the Ag3L4 groups had a significant cytotoxic effect on the MC3T3 cells but not on HFFs. We hypothesize that this cytotoxic effect of Ag3L4 scaffolds to MC3T3 cells is because the released lidocaine and silver ions can increase the osmotic pressure of the culture medium and the accumulation of lidocaine and silver ions from Ag3L4 groups reached a tolerant hypertonic threshold to MC3T3 cells, but not to HFFs. This hypertonic condition is unlikely to happen in vivo due to the continuous flow and circulation of body fluids. Therefore, in vivo studies can now be designed to further elucidate the appropriate doses to achieve an appropriate antibacterial effect to prevent infections as well as analgesic efficacy to control the postoperative pain, and to further evaluate their effects on bone regeneration.
Conclusion
The technological breakthrough of computer and information technology facilitates the fabrication of custom-made products based on computer-assisted design. Ag3PO4 and lidocaine loaded PCL scaffolds were printed using a pneumatic extrusion-based 3D printing. The scaffolds showed a porous structure with high fidelity. The delivery of lidocaine could be controlled by adjusting the filament diameter while that of silver release is correlated to the Ag3PO4 loading amount. The lidocaine was release in a controlled manner during 4–7 days and resulted in a concentration far above the therapeutic level of lidocaine. Moreover, the Ag3PO4 incorporation showed a sustained silver release profile and enhanced the antibacterial properties of the scaffolds for at least 6 days. Although the Ag3L4 scaffolds showed a toxic effect to MC3T3 cells, which can be due to the hypertonic effects of the dual-released lidocaine and silver, the lidocaine or Ag3PO4 loaded scaffolds alone did not evoke cytotoxicity to HFFs and MC3T3 cells. Therefore, pneumatic extrusion-based 3D printing can provide a practical way to fabricate drugs loaded scaffolds. In vivo explorations can now be performed to validate the clinical efficacy and safety of the scaffolds.
Footnotes
Acknowledgments
This work was supported by the NutsOhra Foundation [project no.: 1303-024], the China Scholarship Council (project no.: 201406220180), and the Erasmus+ funding programme (reference no. IV/2017/14014). The author would like to thank Ms. Quanjing Mei for her help with the antibacterial test.
Disclosure Statement
No competing financial interests exist.