
Abstract
Objective:
To investigate the preclinical feasibility of using bio-airbrush technology for the fully arthroscopic treatment of cartilage defects with a combination of cells and biomaterials.
Design:
A combination of in vitro, ex vivo, and cadaveric in situ experiments was performed, to evaluate the preclinical feasibility of using bio-airbrush technology for cartilage repair. Cartilage matrix production after airbrushing cells was evaluated. Subsequently, the influence of different spray parameters on successful defect fill was studied. Finally, the surgical feasibility of using bio-airbrush technology was evaluated in situ in cadaveric knees.
Results:
The most important findings of the presented study are that the matrix producing capacity of the cells was not hampered by airbrushing, air pressure and defect location were important parameters to consider, and using the bio-airbrush was found to be surgically feasible in a CO2-insufflated arthroscopic procedure in cadaveric knees.
Conclusions:
Bio-airbrush using CO2 arthroscopy would facilitate fully arthroscopic application of (cell laden) two-component in situ gelating biomaterials to cartilage defects, as a treatment for cartilage repair. This would shift the conventional procedures, which are commonly performed using a (mini-)arthrotomy, toward arthroscopy.
Impact Statement
This study shows that a bio-airbrush can be a clinically feasible instrument for the use in cell transplantations to repair knee cartilage defects. This technology would enable a shift from cartilage repair procedures, which are mostly performed using an arthrotomy, toward a fully arthoscopic approach. In addition, the technology presented could possibly be translated to other fields of research where controlled in situ deposition of cells is required, such as treatment of burn wounds/ulcers/others. Our research has shown that the use of an airbrush is safe, without harming cell viability and performance.
Introduction
Treatment of articular cartilage defects in knees of young patients is focused on providing a solution that is suitable for their high-demanding lifestyle. Briefly, defects larger than 2–2.5 cm2 require cell-based treatment or osteochondral auto/allograft transplantation.1–5 Both mono- (autologous chondrocyte implantation [ACI]) and cotransplantations of chondrocytes and human multipotent mesenchymal stromal cells (MSCs) are being used in cell-based cartilage repair procedures.6,7 However, these treatment options are mostly performed using a (mini-) arthrotomy approach, which is more invasive compared to an arthroscopic approach. Furthermore, arthrotomy is more painful for the patient compared to arthroscopic surgery and may cause localized bleeding, which can be harmful for the implanted chondrocytes. 8 In addition, arthroscopic ACI is challenging, as it was shown that cell viability is severely hampered when it is performed arthroscopically, due to the required manipulation of the implant through the arthroscopic portal.9,10
In situ gelating biomaterials, such as fibrin glue, have been widely used as a scaffold for cell-based treatment.11–14 These biomaterials can be applied directly to the defect, without any need for manipulation of the implant through an arthroscopic portal. Several one-stage, fully arthroscopic procedures have been proposed in which a defect is treated with a cell-based or cell-free, in situ gelating biomaterial.12,15 However, there have not been any large advancements in instrumentation used in these arthroscopic procedures during the past years. Standard injection needles are used to apply an in situ gelating biomaterial, which can be challenging especially when cartilage defects present at a slope that is not oriented horizontally.
Recently, the arthroscopic airbrush was proposed as an innovative technology that allows for in situ co-delivery of a combination of a two-component biomaterial and cells, to rapidly fill complex tissue defects.16,17 This would facilitate fully arthroscopic filling of cartilage defects with cell-laden in situ gelating biomaterials. However, the arthroscopic environment is challenging, as it is associated with a limited working distance and limited maneuverability. In addition, while cell viability has been shown to not be affected by the spraying process, 17 it is still unknown if the spray application is not influencing the regenerative capacities of the cells.
Previous academically-driven, not industry-driven, research has resulted in a clinically relevant custom-made instrument, the bio-airbrush,12,17 with the length of an arthroscopic probe, a thickness of ±4.5 mm, and a 30° angled tip to provide sufficient maneuverability in the knee. The aim of this study was to study the preclinical feasibility of using this technology for the fully arthroscopic treatment of cartilage defects with a combination of cells and biomaterials. To study this extensively, a combination of in vitro, ex vivo, a study in a three-dimensional (3D)-defect model, as well as cadaveric in situ experiments, was performed.
Methods
Cell isolation and expansion
Cartilage for cell isolation was obtained from redundant material from patients that underwent total knee arthroplasty. The anonymous collection of this material was performed according to the Medical Ethical regulations of the University Medical Center Utrecht and the guideline “good use of redundant tissue for research” of the Dutch Federation of Medical Research Societies 18 (Federa, Rotterdam, The Netherlands). Articular chondrocytes were isolated using a previously described protocol, using type II collagenase (Worthington Biochemical). 19 Cells were expanded in chondrocyte expansion medium (DMEM [Gibco], 10% fetal bovine serum [FBS; Hyclone, Logan, UT], and 1% penicillin/streptomycin (P/S; Gibco, 100 U/mL/100 μg/mL)), passaged at subconfluency and maintained in expansion medium until passage 2, when they were harvested for experiments.
Human bone marrow MSCs (BM-hMSCs) were isolated from bone marrow aspirates according to a previously described protocol. 20 Bone marrow aspirates were taken from the iliac crest of patients receiving total hip arthroplasty, after their informed consent and according to a protocol approved by the local Medical Ethics Committee (University Medical Center Utrecht). Cells were separated on Ficoll-Paque (GE-Health care), and the mononuclear fraction was plated for culture in MSC expansion medium (aMEM [Gibco], 10% FBS, 1% P/S, and 0.2 mM L-ascorbic acid-2-phosphate [AsAp; Sigma-Aldrich]). BM-hMSCs were selected based on plastic adherence, as previously described. 21 Cells were passaged at subconfluency and maintained in expansion medium until passage 3, when they were harvested for experiments.
In vitro culture of sprayed cell-laden constructs
To study the capacity of sprayed cells to produce cartilage tissue, fibrin glue (Tisseel, Baxter) constructs were made containing chondrocytes (n = 3 donors) and BM-hMSCs (n = 1 donor). Constructs were made with monocultures of chondrocytes (100% chondrocytes) and cocultures of both cell types in a ratio of 10:90 (10% chondrocytes, 90% BM-hMSCs) because the current cell therapies for cartilage defect repair consist of these cells and cell combinations (cultivated chondrocytes: MACI, ChondroCelect, and Spherox; combination of chondrocytes and MSCs: IMPACT and Reclaim).6,7 Cells were dissolved in the fibrinogen component (diluted 1:15 in phosphate-buffered saline [PBS]; Gibco) at a concentration of 5,000,000 cells per mL of diluted fibrinogen. Subsequently, the cell-laden fibrinogen was applied simultaneously with the thrombin component (diluted 1:50 in PBS) at a 1:1 ratio. To make the constructs with sprayed fibrin glue, fibrin glue was sprayed using the custom-made bio-airbrush system (Fig. 1) with air supply (0.6 bar for cell survival) 17 in wells of a 48-well plate. To make the extruded control constructs, the bio-airbrush system was used without air supply, so the components dripped out of the system in wells of a 96-well plate. The fibrin glue in the multiwell plates was incubated for 20 min at 37°C to allow complete gelation. Subsequently, the constructs were transferred to 24-well plates and cultured for 28 days in redifferentiation medium (DMEM, 2% insulin–transferrin–selenium [ITS]-X [Invitrogen], 0.2 mM AsAp, 2% human serum albumin [Sanquin Blood Supply Foundation Amsterdam, the Netherlands], and 1% P/S). Culture medium was refreshed thrice per week and collected for biochemical analyses with every medium change. For biochemical analyses, four technical replicates of the constructs were made per condition per donor, for histology and immunohistochemistry two replicates.
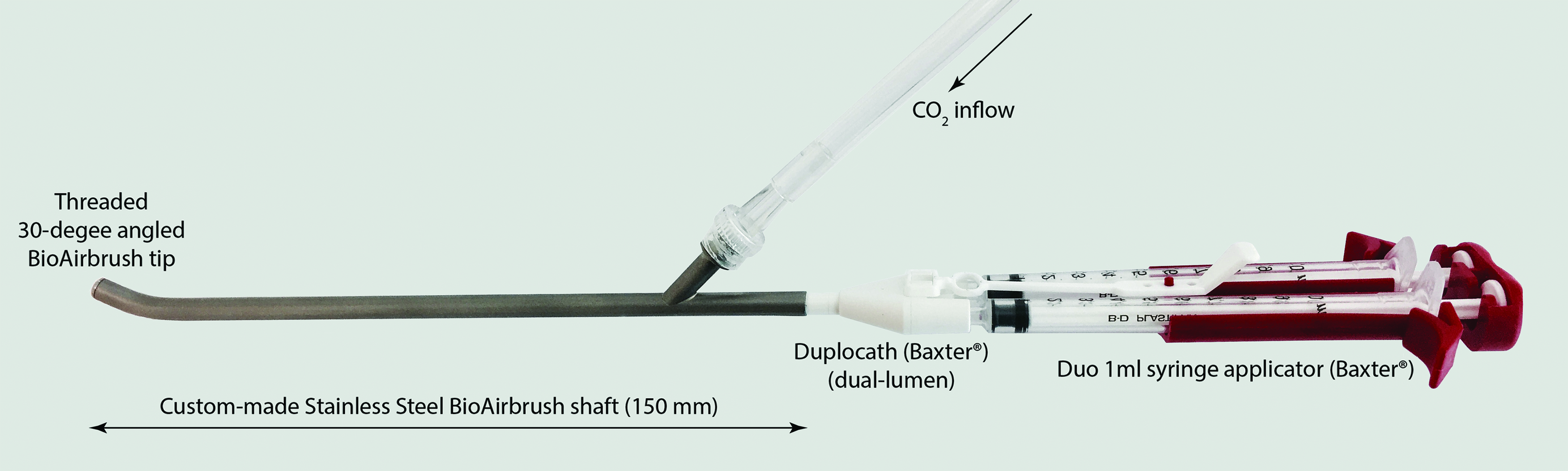
Bio-airbrush instrument design. The dual syringe applicator is used to manually apply the cell-laden fibrin components simultaneously. CO2 inflow is controlled using a foot pedal, at a variable pressure set at the DuploSpray pressure regulator (Baxter). Color images are available online.
Biochemical analyses
Cartilage tissue formation was evaluated using a combination of quantitative biochemical analyses of cartilage matrix components. Proteoglycan content was evaluated by quantification of the sulfated glycosaminoglycan (sGAG, further referred to as GAG) content (in the constructs), release (in the culture medium), and total GAG (content+release). Collagen content was evaluated indirectly by quantification of the hydroxyproline content. 22 DNA content (quantified by PicoGreen assay) was determined to normalize the production of matrix components to the amount of DNA in the constructs.
Briefly, after 28 days of culture, constructs were digested overnight at 60°C in a papain digestion solution (250 μg/mL papain [Sigma-Aldrich], 0.2 M NaH2PO4, 0.1 M EDTA, and 0.01 M cysteine-HCL). Digests (content) and culture medium (release) were used for quantification of the GAG content with a dimethylmethylene blue assay with an absorption ratio of 525/595 nm in a spectrophotometer and chondroitin-6-sulfate (Sigma-Aldrich) as a standard.
For the hydroxyproline assay, papain digests were lyophilized, subsequently hydrolyzed overnight in 0.4 M NaOH at 108°C, and finally 1.4 M citric acid was added, before performing the assay. Hydroxyproline (Sigma-Aldrich) was used as a standard. For the hydroxyproline assay, samples were incubated with chloramine-T (in 2-propanol and stock buffer) for 20 min at room temperature, then dimethylaminobenzaldehyde (in 2-propanol and perchloric acid; Merck) was added and again incubated for 20 min at 60°C. Plates were read out at 570 nm in a spectrophotometer. The total amount of collagen was calculated based on the assumption that 13.5% of collagen consists of hydroxyproline. 22
DNA content in the papain digests was determined using a PicoGreen DNA assay (Invitrogen) according to the manufacturer's instruction.
Feasibility in a 3D cartilage defect model
The surgical feasibility of using the bio-airbrush for arthroscopic knee cartilage repair was first studied in a 3D printed cartilage defect model. Three-dimensional models of knee cartilage defects were modeled based on patient data using computer aided design (CAD, Blender software) and subsequently produced by 3D printing (Fig. 2L). To test the surgical feasibility, the bio-airbrush system was used to apply sodium alginate (1.2%; Sigma-Aldrich), simultaneously with 204 mM CaCl2 (Sigma-Aldrich), resulting in cartilage defects filled with cross-linked alginate. For visibility, alginate was colored with yellow food dye, which did not affect gelation capacity. Studied variables were air pressure and defect location. For the variable defect location, an air pressure of 0.6 bar was used. To ensure no influence of defect model position, the models were positioned similarly for each experiment. This position was based on leg positioning during arthroscopic surgery, which was evaluated in the laboratory using a femorotibial sawbone model as a guide (Fig. 2J, K). The success of cartilage defect filling was assessed (three independent observers) by scoring macroscopic photos of the filled defects, according to a modified version of a previously described scoring method.16,23 Outcomes were (1) % of defect outline covered, (2) % of defect fill, and (3) % of gel outside the defect. Outcomes were given a score between 1 and 5, as shown in Table 1.

Macroscopic images of defect fill in 3D defect models. Mean results are shown for parameters air pressure in the range of 0.4–1.0 bar
Modified Macroscopic Scoring System
Percentage of full circumference that has contact with the surrounding cartilage rim.
Percentage of total cartilage defect that is covered with gel.
Percentage of gel located outside the defect area.
The score that matches the percentages is given between the parentheses.
Cell distribution and survival
To evaluate cell distribution and survival, a LIVE/DEAD Viability Kit (Invitrogen) was used. Briefly, cell-laden constructs of fibrin glue (1 × 106 hMSCs per 500 μL construct, n = 5, see In Vitro Culture of Sprayed Cell-Laden Constructs section) were created in a fresh ex vivo focal cartilage defect, created in a part of a femoral condyle (redundant total knee arthroplasty material). Constructs were removed from the defect and subsequently incubated with 2 μM calcein-AM and 4 μM ethidium homodimer-1 in PBS, for 30 min in the dark at 37°C. Afterward, constructs were washed thoroughly and visualized under fluorescence microscopy. Cell survival was evaluated by evaluating the number of live cells compared to the number of dead cells. Cell distribution was evaluated by observing the distribution of cells within the constructs, focusing on the presence of cell agglomerations.
Preclinical in situ feasibility in the human knee
To test the preclinical surgical feasibility of the bio-airbrush, a controlled in situ feasibility study in human knees was performed in six different knee joints of three male and three female donors (mean age 66, range 56–78) in agreement with the guidelines of the local ethics committee. The fresh knee specimens were derived from bodies who entered the Department of Anatomy through a donation program. From these persons, written informed consent was obtained during their lifetime that allowed use of their bodies for educational and research purposes.
Each knee was tested on (visual) malalignment, stability, and range of motion (full extension and at least 80° flexion). Briefly, full-thickness cartilage defects were created using an open approach, after which the knee was closed and arthroscopy was initiated. First, an anterior midline incision through the skin and subcutaneous layer was made. A medial parapatellar approach through the joint capsule was used to enter the joint. Subsequently, the patella was everted to obtain access to the femoral articular cartilage. Cartilage defects were created with consistent size (2.0 cm2) on the medial lateral condyle, as well as the trochlea (facies patellaris), using a sharp spoon and an oval shaped defect punch as a template (Braun Aesculap Novocart 3D; 2.0 cm2); the articular cartilage and the underlying calcified layer were removed. In addition, the infrapatellar fat pad was removed. Subsequently, the knee was closed in three layers; the capsule, the subcutaneous, and the skin layer.
After closure, three arthroscopic portals were created; standard anteromedial, anterolateral, and superolateral (CO2 inflow), to initiate CO2-insufflated arthroscopy. When proper view of the defects was obtained, the defects were dried with cotton buds before application of the fibrin. The two-component holder of the fibrin glue (Baxter) was connected to the bio-airbrush system. For CO2 supply, the instrument was connected to a DuploSpray (Baxter) pressure regulator, which was used to apply CO2 flow using a foot pedal, to facilitate spraying.
The fibrin glue was stained with a blue food dye for visibility, without impairing gelation capacity, and applied to the three cartilage defects, using either the bio-airbrush system (n = 9 defects) or a standard Duo syringe system (Baxter) with a 18 gauge needle (n = 9 defects) utilizing CO2 insufflation. Afterward, the legs were subjected to several cycles of flexion and extension, to ensure proper placement of the cell product. Finally, the knees were reopened for macroscopic evaluation of defect fill. Digital photographs were made from each filled defect and the surrounding cartilage for macroscopic scoring.
The macroscopic images of defect fill were scored by four independent observers (blinded for the application method) using a modified macroscopic scoring system as described in the feasibility study in a 3D cartilage defect model (Table 1). To assess the reliability of the macroscopic scoring system, interobserver agreement was determined.
Statistical analyses
The biochemical data were statistically evaluated using two-tailed paired t-tests comparing mono- and cocultures and bio-airbrush versus extruded samples. Macroscopic scorings in the 3D defect model were compared using an ordinary one-way ANOVA with Tukey's post hoc multiple comparison test. The macroscopic scorings in the cadaveric study were compared using unpaired two-tailed t-tests comparing bio-airbrush versus needle extrusion. A p-value <0.05 was considered statistically significant. To evaluate inter-rater reliability of the macroscopic scoring system, the Fleiss-kappa κ was used. 24 κ was determined for each of the scoring parameters in both the 3D model (three observers), as well as the cadaveric study (four observers). A κ-value of <0.20 was considered to indicate slight agreement, 0.21–0.40 fair agreement, 0.41–0.60 moderate agreement, 0.61–0.80 substantial agreement, and 0.81–0.99 almost perfect agreement.24,25 All statistical analyses were performed using Prism 7 (GraphPad) and Excel 2010 (Microsoft).
Results
In vitro culture of sprayed versus extruded cell-laden constructs
Both sprayed and extruded cell-laden constructs were successfully cultured for 28 days without any disintegration of the constructs. Contraction of the constructs was observed in the first 3 days, after which construct size stayed constant. At day 0, no GAGs or collagen could be detected in the constructs (data not shown). After 28 days of culture, total GAG production and collagen content showed similar levels between sprayed and extruded constructs (Fig. 3). In addition, no differences could be observed among total GAG production, collagen content (either or not corrected for DNA content), and DNA content between monocultures and cocultures. Moreover, no differences were found in the amount of DNA between day 0 and 28 (data not shown). Overall, constructs made using the bio-airbrush or extrusion showed similar levels of matrix production (Fig. 3).
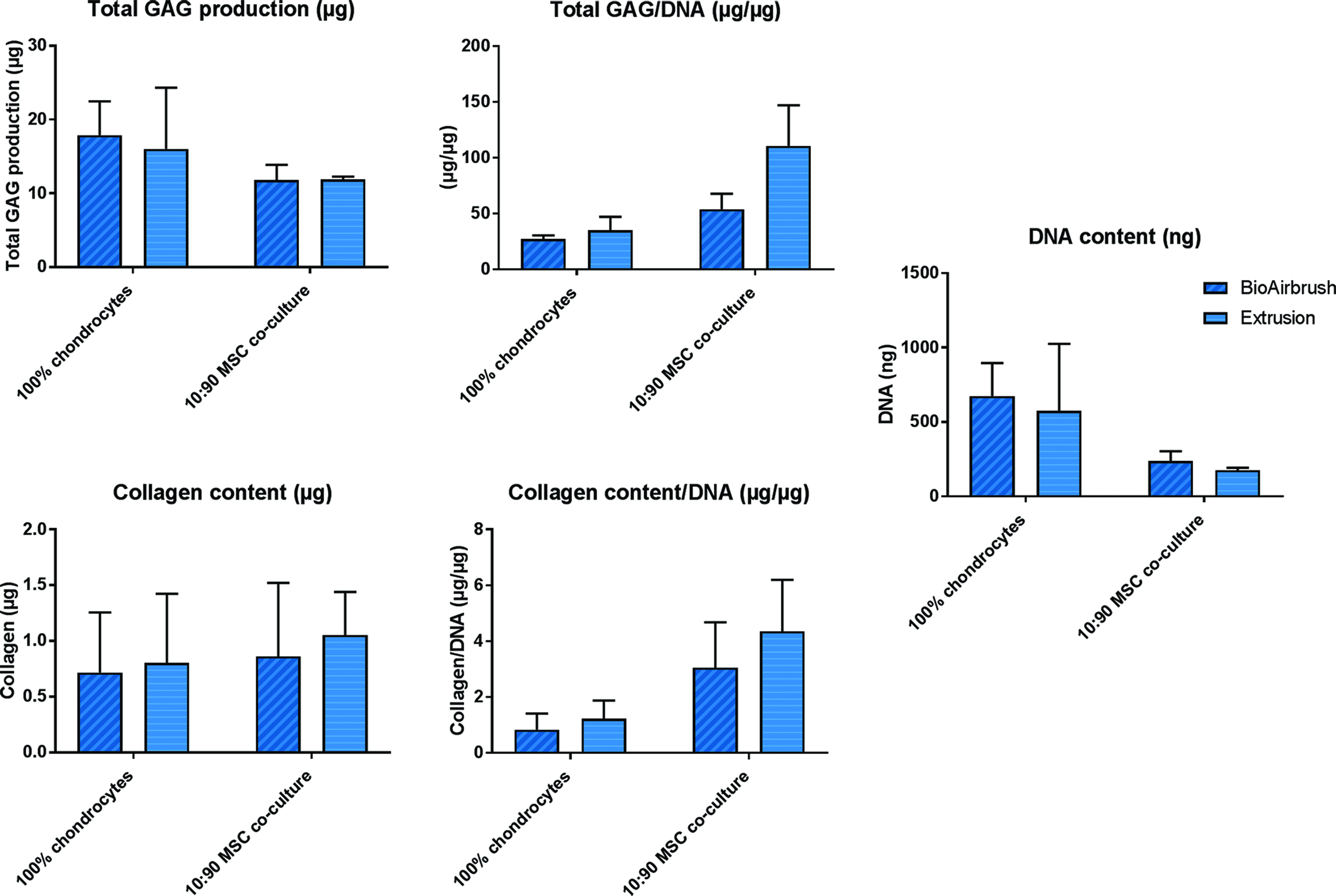
Biochemical analyses after 28-day culture of mono- and cocultures of chondrocytes and MSCs in bio-airbrushed versus extruded fibrin constructs. Total GAG production, collagen, and DNA content, as well as production normalized for DNA, are expressed as mean ± SD. GAG, glycosaminoglycan; MSCs, mesenchymal stromal cells. Color images are available online.
Feasibility defect fill parameters in 3D defect model
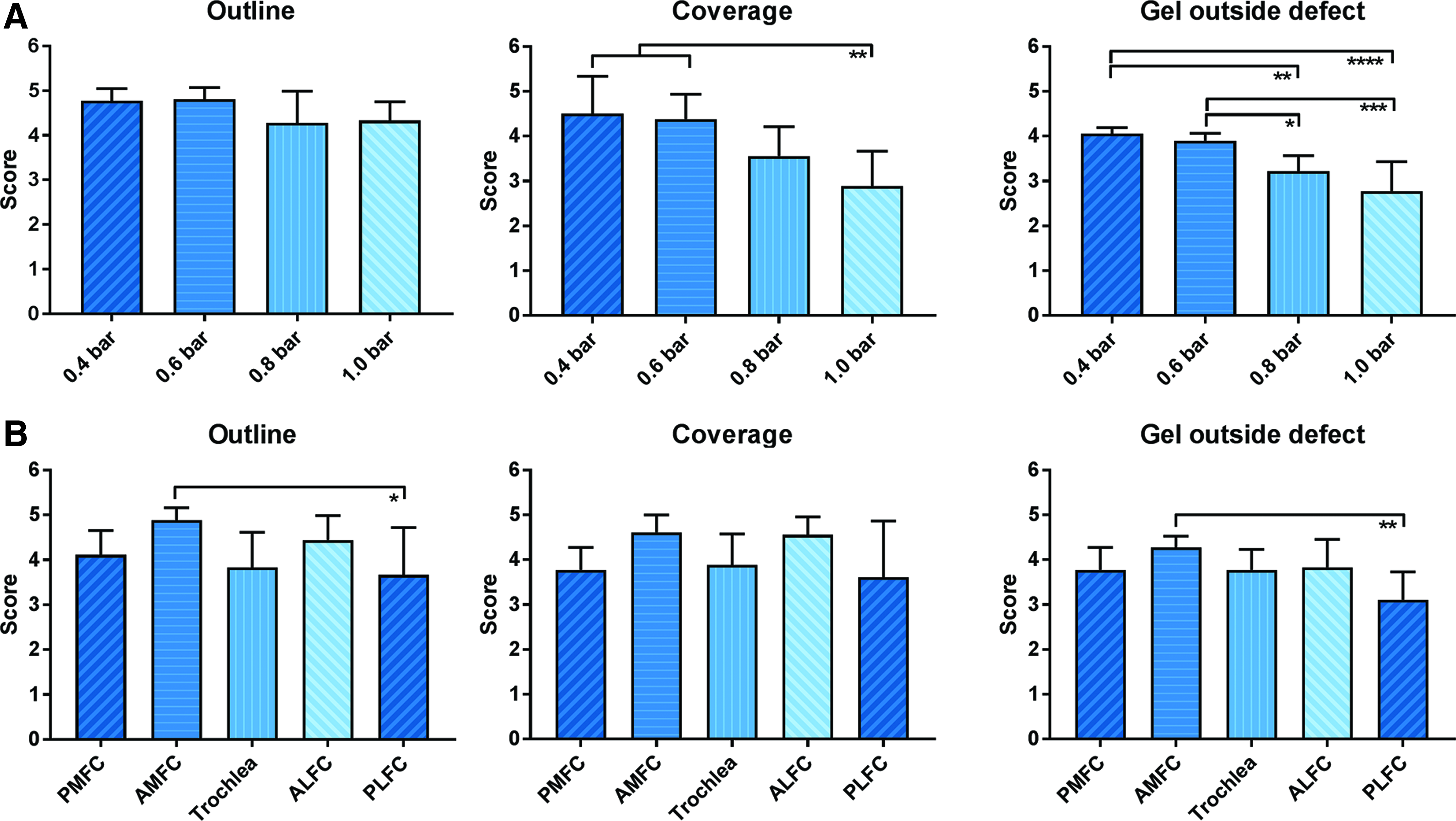
Use of the bio-airbrush allowed for easy delivery of a two-component gel into cartilage defects in 3D printed defect models. Mean outcome scores were used for graphical presentation of the results in Figure 4. Interobserver reliability testing with Fleiss-kappa κ showed a moderate-to-substantial agreement between observers. Fleiss-kappa κ-values were 0.52, 0.55, and 0.70 for outline, coverage, and gel outside defect scores, respectively, regarding the pressure variable. Fleiss-kappa κ-values for defect location were 0.57, 0.43, and 0.56.
Macroscopic outcome scores in 3D defect models (Fig. 2) for parameters air pressure
Use of pressures <0.4 bar did not result in spray formation. Defect outline outcomes were not significantly affected by a varying air pressure. However, defect coverage and gel outside of the defect outcomes were significantly decreased by use of an increasing air pressure ≥0.8 bar (Figs. 2 and 4A). Overall, use of a pressure of 0.4–0.6 bar resulted in the highest outcome score for all scoring parameters, which facilitated the best defect fill.
Considering the location of the femoral cartilage defect, a minor, nonstatistically significant influence on outcome scores was observed. However, a trend was observed toward higher outcome scores on all scoring parameters for defects located on the anterior part of the femoral condyle (Figs. 2 and 4B). Trochlear defects and defects located on the posterior part of the femoral condyle resulted in similar outcome scores, which were slightly lower compared to the anterior located defects. Differences between the laterally and medially located defects were nonexistent. Overall, average outcome scores were substantial (outline [range 3.67–4.89], coverage [3.61–4.61], and outside defect [3.78–4.28] on a range of 1–5) and indicated successful defect fill using the bio-airbrush.
Cell distribution and survival
Cell distribution and survival of hMSCs were evaluated in sprayed fibrin glue in a fresh cartilage defect. Upon microscopic evaluation (Fig. 5), homogenous cell distribution, as well as cell survival of >95% of the cells, was observed in all samples (n = 5).
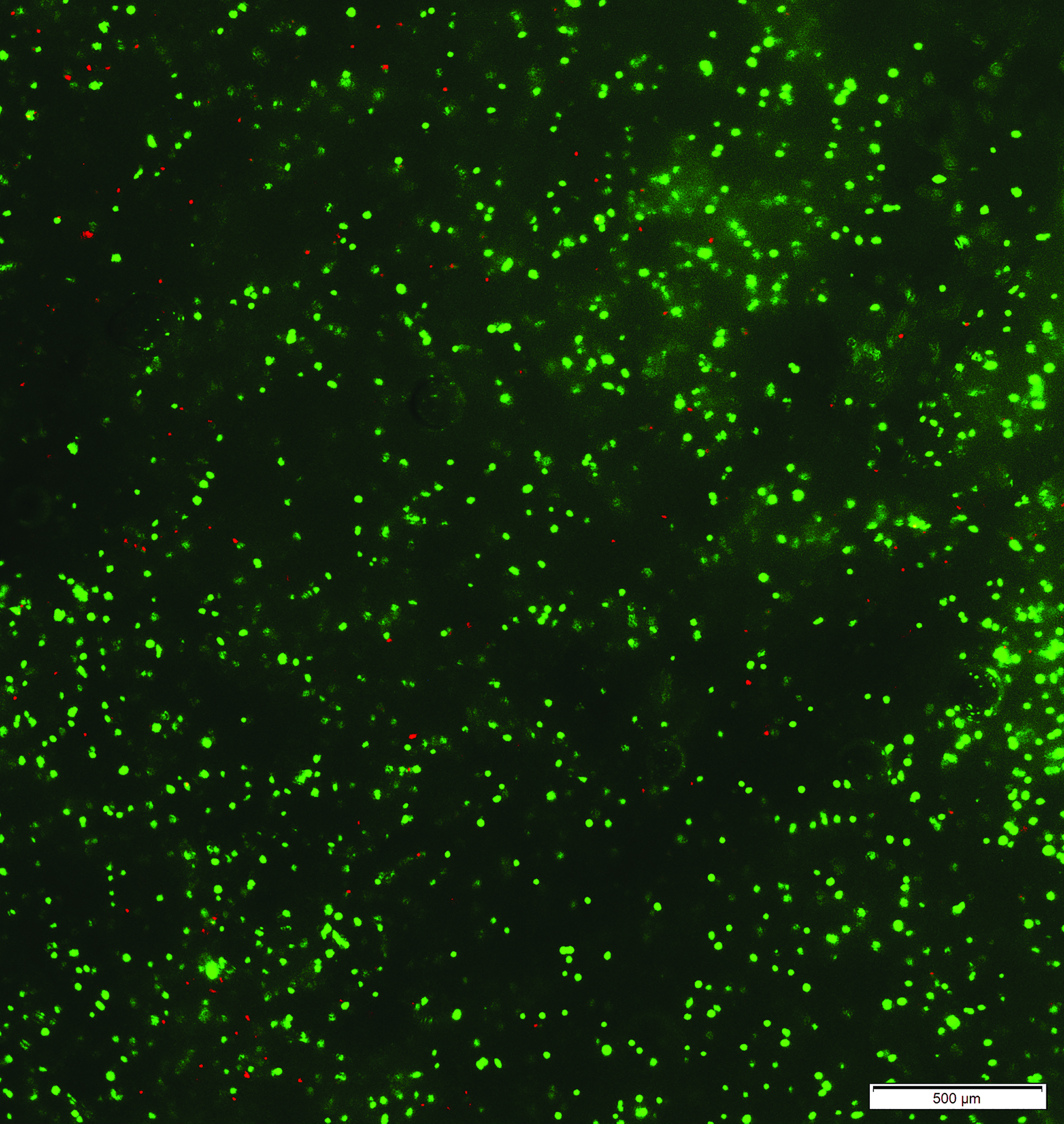
Cell viability of bio-airbrushed hMSCs in fibrin glue after application in an ex vivo cartilage defect (pressure 0.6 bar). Images were obtained directly after application, after staining with calcein-AM (live cells, green) and ethidium homodimer-1 (dead cells, red). Figure shows a representative image of n = 5 constructs. 10 × magnification. hMSCs, human mesenchymal stromal cells. Color images are available online.
Feasibility defect fill in cadaveric knees
Arthroscopic use of the bio-airbrush was shown a feasible and straightforward technique for the application of (cell-laden) fibrin glue in articular cartilage defects in cadaveric knees. CO2-insufflated arthroscopy was found to be a workable method for the creation of arthroscopic accessibility of the defects, which allowed for application of (cell-laden) fibrin glue using both the bio-airbrush and needle extrusion. A separate portal for CO2 insufflation is recommended as this allowed more stable pressure inside the joint, compared to using the arthroscope portal. Arthroscopic needle extrusion was found to be a more challenging technique due to gravity induced spill, premature gelation of fibrin, and undesirable adhesion of the fibrin glue to the soft tissues upon withdrawal of the needle.
Interobserver reliability testing with Fleiss-kappa κ showed a moderate-to-substantial agreement between observers. The Fleiss-kappa κ-values were 0.50, 0.48, and 0.60 for the outline, coverage, and gel outside defect scores, respectively. The mean outline, coverage, and gel outside defect scores were 3.22 ± 0.80, 3.47 ± 0.55, and 4.36 ± 0.81 (mean ± SD) for the bio-airbrush technique, compared to 2.48 ± 1.10, 2.95 ± 1.09, and 4.08 ± 0.68 (mean ± SD) for the arthroscopic needle extrusion (Fig. 7). Overall, a trend toward higher outcome scores for the bio-airbrush was found (p-values reported in Fig. 7).
Macroscopic images of the best, mean, and worst results in terms of successful defect fill for both techniques are shown in Figure 6. Overall, the best, mean, and worst case for the bio-airbrush techniques showed better defect fill compared to arthroscopic needle extrusion.
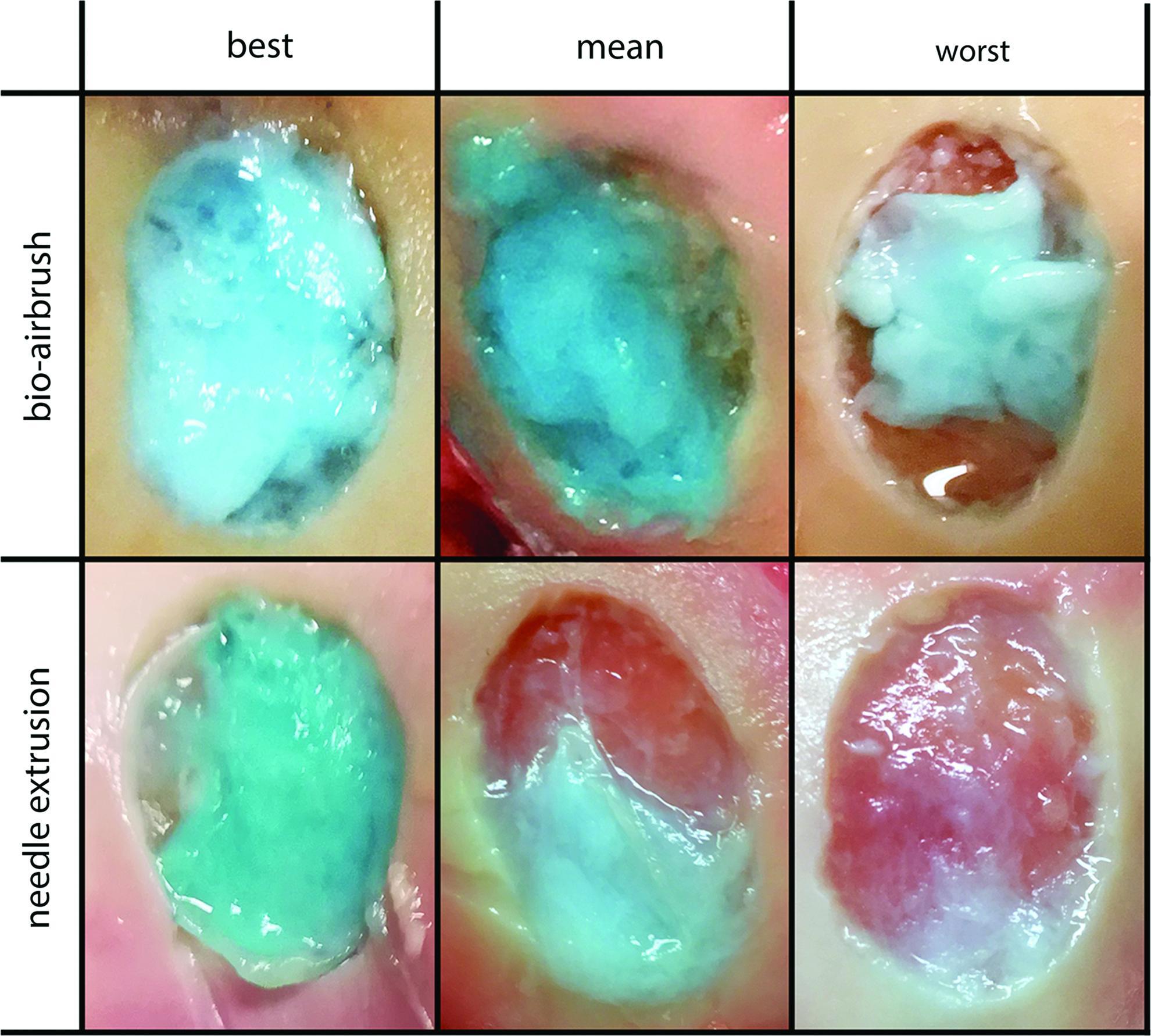
Images of best, mean, and worst defect fill in defects filled with the bio-airbrush and needle extrusion in cadaveric knees. Images were categorized as best, mean, or worst based on macroscopic scorings. Color images are available online.
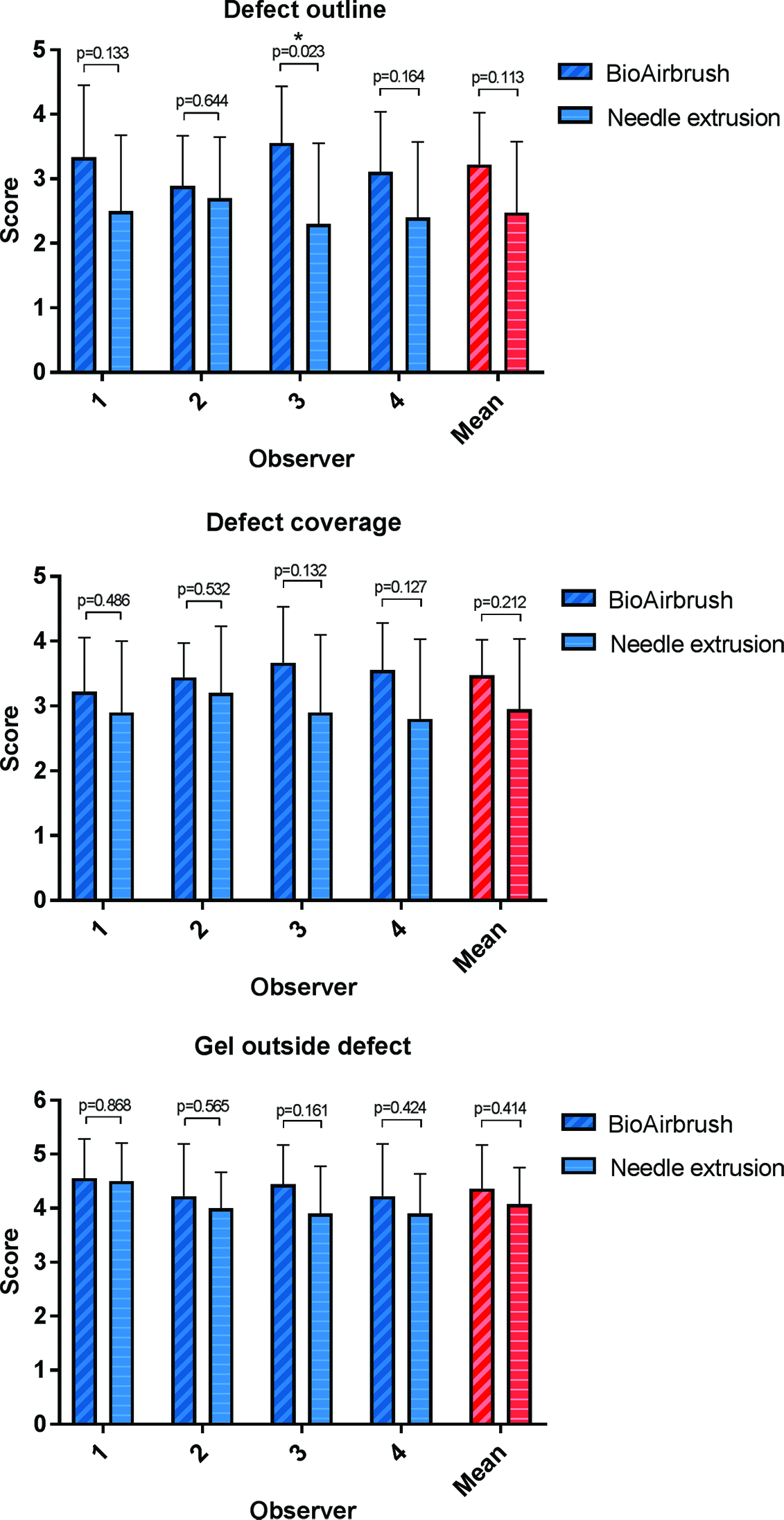
Macroscopic outcome scores for the cadaveric study (Fig. 6). Results are shown for each observer, as well as a mean for all observers, for both bio-airbrush and needle extrusion filled defects, expressed as mean ± SD. p-Values as a result of statistical evaluation of the difference between bio-airbrush and needle extrusion are reported in the graph. Color images are available online.
Discussion
This study has evaluated the feasibility of arthroscopic airbrush-assisted cell transplantations for cartilage repair using a variety of approaches. The most important findings of the presented study are that the matrix producing capacity of the cells was not hampered by airbrushing, that air pressure and defect location are important parameters to consider, and that use of the bio-airbrush was found to be surgically feasible in a CO2-insufflated arthroscopic procedure.
Airbrush-assisted cell transplantations are not only proposed for cartilage repair procedures. Recent examples of this technology have been presented in the field of organoids for intestinal regeneration, 26 sprayed cells for skin regeneration, 27 cell transplantations in tubular structures for tracheal reconstruction,28,29 application of stem cells to heart tissue, 30 and several others.31,32 The overall opinion about this technology is that this method is particularly suitable for locations that are difficult to reach, and it allows for controlled deposition of viable cell-laden biomaterials to facilitate tissue regeneration.16,28,33
In this study, use of the bio-airbrush did not hamper the matrix producing capacity of chondrocytes and cocultures of chondrocytes and hMSCs. It was already shown that chondrocytes and hMSCs retain gene expression of aggrecan and type II collagen after airbrushing. 17 Moreover, based on production of GAGs and collagen in this study, the most abundant matrix components of articular cartilage, airbrushed cells were shown capable of producing these components to similar levels as needle extruded cells. This confirms the hypothesis that cells not only survive the airbrushing process but also maintain their matrix producing ability. The current study showed the survivability of hMSCs after airbrushing. Previous studies have already shown viability of chondrocytes and cocultures of chondrocytes and hMSCs after airbrushing on tissue-culture plastic.16,17
Parameters that might affect defect fill using the bio-airbrush were studied in 3D printed articular cartilage defect models. Air pressure was shown to significantly affect defect fill on all scoring parameters. Use of pressures higher or equal to 0.8 bar resulted in crater formation due to the force of the airflow. Interestingly, this is the same cutoff as was found for the influence of air pressure on cell viability in a previous study. 17 This study showed that similar high pressures significantly decrease cell survival. Regarding these results, an air pressure of maximum 0.6 bar is recommended for spray application of cells in fibrin glue, which is in line with other studies.17,34
Defect location was also found to affect defect fill, presented by more successful defect fill in anterior located defects, compared to trochlear and posterior located defects. This can partly be explained by the influence of gravity that is more present in posterior located defects. This can however not explain the lower scores in trochlear defects, as this defect was almost horizontally oriented. Possibly the shape of the defect, which was slightly more elongated compared to the other defects, might explain this effect. Another limitation of the study is that the 3D defect models were made from polylactic acid (PLA) plastic, which provides a substrate difference from the subchondral bone in a cartilage defect. Even though subchondral bone and PLA show comparable elastic modulus, PLA: 3.5 GPa, 35 compared to femoral subchondral bone: 3.9 ± 1.5 GPa, 36 as a measure for stiffness, other material characteristics might have influenced defect fill. 37
An interesting finding was that this bio-airbrush system approach could also be adopted for use with other two-component in situ gelating biomaterials, which was shown with alginate in these experiments. Examples of other two-component in situ gelating biomaterials are, for example, based on alginate, 38 collagen, 13 dextran, 39 hyaluronan, 39 gelatin, 40 and others. 41 The universal character of the bio-airbrush instrument using standard 1 mL syringes allows for adaptation with different biomaterials, modification of gelation times, etc.
Important for successful cartilage regeneration when applying cell-laden fibrin glue are cell survival and distribution throughout the defect. 42 High cell survival (>95%) and homogenous cell distribution were found after airbrush-assisted application of cell-laden fibrin to a cartilage defect, with the subchondral bone as a substrate. Thus, bio-airbrush-assisted application of cell-laden fibrin to a cartilage defect can provide a stable, well-mixed fibrin scaffold, in which the cells survive and are homogenously distributed.
Apart from an extensive study into the method of application and performance of the cell product, an instrument feasibility study was performed in cadaveric knees. This study has shown that CO2 knee arthroscopy is a feasible technique for the arthroscopic application of (cell-laden) fibrin glue in articular cartilage defects using conventional needle extrusion and the bio-airbrush. Using this technique, several points are important to consider. The CO2 flow can influence the gel application process by interfering with the flow of the spray or extrusion. Therefore, CO2 flow was introduced through a separate superolateral portal, which provided stable intrajoint pressure and minimal interference with the gel application process. Drying of the defect area was shown to improve adherence of the gel to the defect. However, extensive drying of the cartilage surface can harm cell viability 43 ; therefore wetting of the surrounding cartilage with saline would be advised during CO2 arthroscopy.
In addition, defect characteristics were shown to influence successful defect fill. Most important for successful defect fill were properly debrided defect edges (90° angle with the defect area) and cartilage thickness at the defect edges. This study was performed in knees from relatively old donors, in which osteoarthritic thinning of the cartilage was present (upon macroscopic observation) in some specimens. This might have influenced the outcome scores of defect fill, which were overall slightly lower in the cadaveric study, compared to the study in a 3D defect model. Finally, a limitation of the study was the use of cadaveric knees, since the integration of the fibrin with the defect might be different in living tissue. Adherence of the fibrin to the defect area would be better in living tissue, 44 due to active binding to the subchondral bone. To evaluate adherence of the gel, the knees were subjected to several cycles of flexion/extension, before the knees were opened for macroscopic evaluation.
Conclusion
This study has shown that the matrix producing capacity by cells is not hampered by airbrushing. Furthermore, use of the bio-airbrush allows for arthroscopic application of cell-laden fibrin glue, as well as other biomaterials, in which cells survive and are homogeneously distributed throughout the hydrogel. Surgical feasibility was shown in a 3D defect model, as well as in a cadaveric study. Air pressure, defect location, and defect characteristics are important parameters to consider when using this technology. Use of the bio-airbrush using CO2 arthroscopy would facilitate fully arthroscopic application of (cell-laden) two-component in situ gelating biomaterials to cartilage defects, as a treatment for cartilage repair. This would shift the conventional procedures, which are commonly performed using a (mini-)arthrotomy, toward arthroscopy.
Footnotes
Acknowledgments
Financial support by the Dutch Arthritis Association is gratefully acknowledged by all authors. The authors thank Matthijs Wassink at the Medical Technology and Clinical Physiology department of the UMC Utrecht for his assistance in designing/producing the bio-airbrush, Smith & Nephew for providing the arthroscopy equipment and devices, and Xavier van Leening and Simon Plomp for their kind assistance at the Anatomy Department.
Disclosure Statement
No competing financial interests exist.