
Abstract
A novel animal experimental model of congenital bone defects without surgical intervention is needed to better mimic human alveolar cleft. We aimed to establish a new experimental model of human alveolar cleft using rat palatine fissures that are present in the central portion of the maxilla. The palatine fissures on the left and right sides are separated by the nasal septum. In this study, we examined potential bone repair by an autologous bone implant and beta-tricalcium phosphate (β-TCP) using rat palatine fissure as a model. The results of the implants were evaluated by micro-computed tomography and histological analysis. All 20 rats received a palatine fissure on the left side; they were then randomly subdivided into 3 groups: group 1 received an autogenous bone graft, group 2 received β-TCP, and group 3 received a blank defect with no implant at the implant site. Sixteen weeks postimplantation, new bone formation at the margins of the left palatine process of the maxilla was observed in all samples. To compare the effect of autologous bone grafts and β-TCP on bone regeneration, the bone volume and bone mineral density (BMD) of newly formed hard tissues were calculated. At 16 weeks, the bone volume and BMD were significantly higher in group 1 than in group 2. Histological examination revealed abundant woven bone ingrowth in groups 1 and 2. Alkaline phosphatase (ALP) staining revealed the presence of osteoblasts along the leading edges on the surface of the newly formed bone. Tartrate-resistant acid phosphatase (TRAP) staining revealed that a few multinucleated giant cells were present on the surface of the newly formed bone. Our model demonstrated that higher bone volume and BMD were achieved with autologous bone graft than with β-TCP. In conclusion, we have provided the first demonstration of the suitability of the rat palatine fissure as the implant site for bone graft materials to simulate the implantation of bone graft materials into human alveolar cleft. Thus, the palatine fissure can be considered as a congenital bone defect that is similar to the alveolar cleft conditions in humans.
Impact Statement
The rat palatine fissure is anatomically similar to human alveolar cleft. In this study, we examined potential bone repair by an autologous bone implant and beta-tricalcium phosphate (β-TCP) using rat palatine fissure as a model. Autologous bone chips or β-TCP granules were implanted into the rat palatine fissure. Our model demonstrated that higher bone volume and bone mineral density were achieved with autologous bone graft than with β-TCP. We have provided the first demonstration of the suitability of the rat palatine fissure as the implant site to simulate the transplantation of bone graft materials into human alveolar cleft.
Introduction
Cleft lip, palate, and alveolus is caused by incomplete fusion of the facial prominences during the 4th–10th weeks of gestation. Among these clefts, an alveolar cleft is a congenital malformation because of abnormal primary palate formation,1,2 which results in the collapse of alveolar segments; therefore, reconstruction is required to provide continuity and stabilization of the maxillary arch to close the oronasal fistula and to permit tooth eruption.3–5 Traditionally, the canine is erupted to the bone graft area, which results in an excellent dental arch using autologous iliac bone grafting before canine eruption. 6 More recently, harvesting cancellous autografts from the iliac bone has become the gold standard treatment for alveolar cleft reconstruction before eruption of the permanent maxillary canine or lateral incisor tooth.3,4,7,8 However, the major drawback of this procedure is the morbidity associated with harvesting (e.g., chronic pain, infection, scar formation, hematoma, and nerve injury). Therefore, various types of iliac bone substitute materials are currently used to repair an alveolar cleft, including hydroxyapatite,2,9 although it suffers from limitation of low solubility and slow in vivo resorption profiles. Alternatively, several beta-tricalcium phosphate (β-TCP) bone graft substitutes have been reported in animal and human studies. However, the ability of the β-TCP to successfully repair an alveolar cleft and the long-term effects have been uncertain. Therefore, searching for novel bone substitution materials is required for improving the clinical outcome in the surgical reconstruction of an alveolar cleft.
A suitable animal experimental model is essential for evaluating bone substitute materials because evidence of the ability to enhance bone repair is a precondition before their clinical application, which also allows for determining the reproducibility of results and comparability of the bone substitution outcome. One of the main prerequisites for an alveolar cleft model is to avoid the occurrence of spontaneous complete osseous regeneration of the created bone defects during the lifetime of the animals. To date, several animal experimental models have been developed to evaluate bone substitute materials for bore repair, which typically involve the creation of a so-called critical size defect by surgical resection of preexisting bone tissue.10,11 Historically, the induction of alveolar clefts in experimental animals has been achieved mainly by two methods. The first is the congenital induction of clefts by administering teratogens to pregnant mothers. However, the teratogens may also lead to other life-threatening anomalies.12,13 The other method involves the surgical creation of a defect that will not heal spontaneously. In general, compared with congenital induction of clefts, a surgically created bone defect seems better suited for applied research because the size and extent of the cleft can be accurately controlled, and can be reproduced with relative ease. However, the main disadvantage of such a model is that when the existing bone is removed to create the defect, extensive damage to the adjacent to bone is inevitable during this operation. This damage itself affects the bone repair process. Moreover, the artificially created bone defects are embryologically and anatomically different from a congenital bone defect of alveolar cleft. In particular, although the bone surrounding the congenital defect does not possess a self-repair property, preexisting bone does have inherent ability for bone regeneration. Therefore, spontaneous healing of created bone defects without implantation of materials can occur in these models, and the bone defects ultimately repair to some extent. In addition, artificial creation of a bone defect imposes artifacts because of the surgical intervention, which also affects the process and extent of bone regeneration. To date, no accurate reproducible congenital bone defect method has been developed to test the potential of the material as a bone substitute for alveolar cleft reconstruction. Accordingly, a novel animal experimental model of a congenital bone defect without surgical intervention is needed to better mimic human alveolar cleft.
Therefore, in this study, we established a new experimental model in which we use the palatine fissures of rats as a model of human alveolar cleft. The palatine fissure of a rat exists in the central portion of the maxilla in the oral cavity (Fig. 1A, B). The palatine fissures on the left and right sides are separated by nasal septum. The palatine fissure can be considered as a congenital bone defect that is similar to the human condition of alveolar cleft. Furthermore, the palatine fissure does not become filled with the bone tissue, even in older rat, further suggesting that the palatine fissure can appropriately imitate alveolar cleft in human congenital bone defects. In this study, we examined the potential of the repair of autologous bone and β-TCP using the palatine fissure as a model. The results of the implants were evaluated by micro-computed tomography (micro-CT) and histological analyses. Confirmation of the suitability of this model could open up new avenues of research into the pathology of alveolar cleft and facilitate evaluations of new materials for reconstruction in clinical practice.
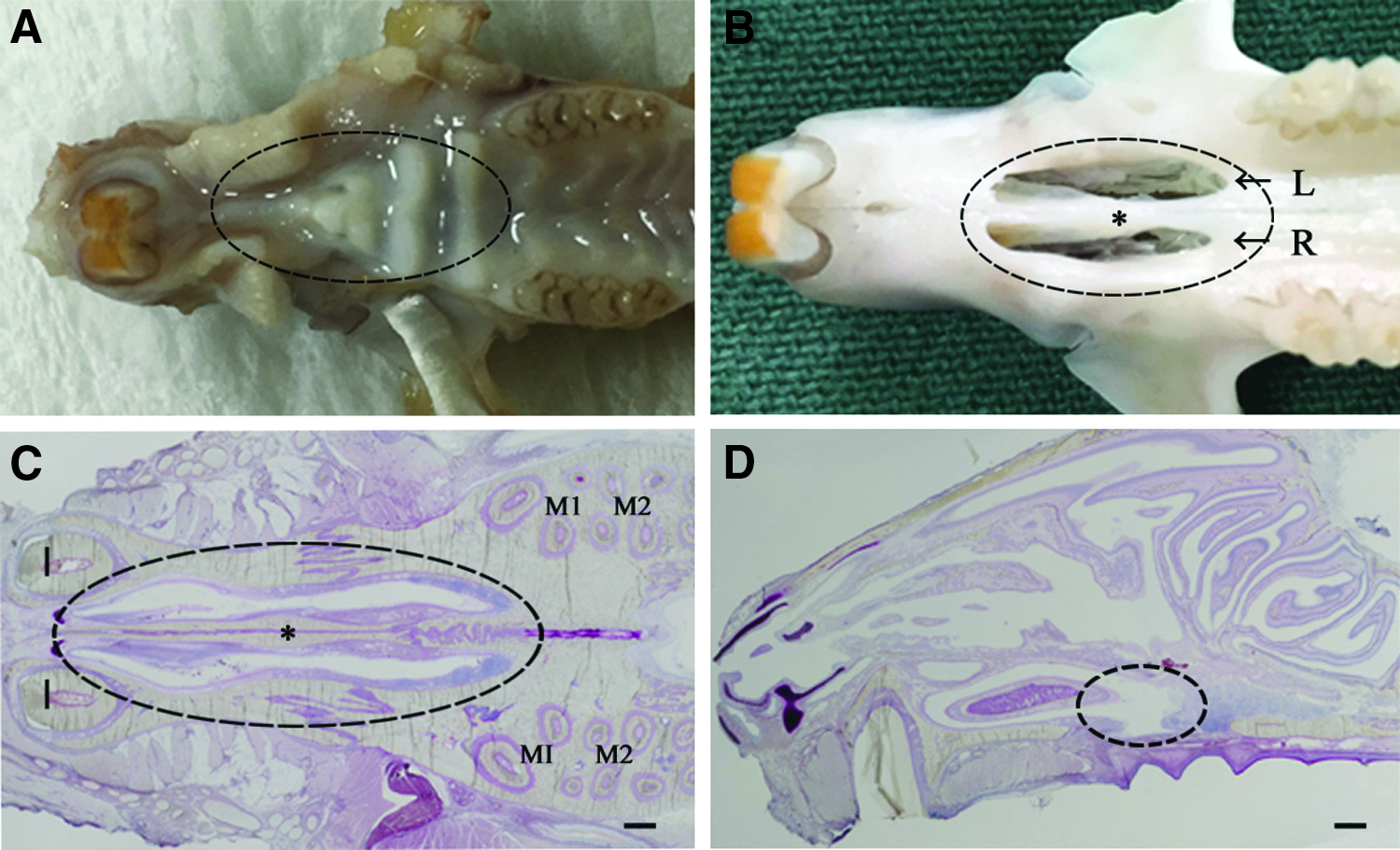
The congenital palatine fissure of a rat.
Materials and Methods
Animals and housing
All experiments were performed using 11-week-old healthy male Sprague-Dawley rats with a body weight of 350–400 g (Chubu Kagaku Shizai, Nagoya, Japan). All rats were kept at an animal experimentation laboratory under a standardized temperature and humidity environment with a 12-h day/night cycle at the Animal Research Center of Aichi Gakuin University. The study protocol was approved by the Aichi Gakuin University School of Dentistry Animal Research Committee (approval No. AGUD412) and the animal care and the experimental procedures were conducted in accordance with the animal care and use committee guidelines of the School of Dentistry, Aichi Gakuin University.
Preparation of implant site
The surgery was performed under sterile conditions after general anesthesia achieved by intraperitoneal injection with a 0.5 mL/100 g body weight of a combination anesthetic (0.3 mg/kg of DOMITOR®: Nippon Zenyaku Kogyo Co., Ltd., Fukushima, Japan; 4.0 mg/kg of midazolam: SANDOZ, Tokyo, Japan; 5.0 mg/kg of Vetorphale®: Meiji Seika Pharma Co., Ltd., Tokyo, Japan and 2.9 mL/kg of Otsuka Normal Saline: Otsuka Pharmaceutical Co., Ltd., Tokyo, Japan). A 10 mm longitudinal incision was made along the reflection between the body of the left incisive bone and palatine process of the left maxilla, and then an incision between the mucosa and periosteum was made to separate the oral mucosal flap and periosteum (Fig. 2A). After an incision was made under the periosteum of nasal septum, the periosteal flap between palatine process and nasal septum was elevated. Then, the occupied fibrous tissue in the left palatine fissure was removed to expose the palatine fissure (Fig. 2B). To prepare the implant site, the elevated periosteum including both the palatine process and nasal septum was pressed into the nasal floor (Fig. 2C). The implant site was surrounded by the two cortical bone surfaces and the two periosteum surfaces to best imitate a human congenital alveolar cleft (Fig. 3A). The materials were immediately placed on one side of palatine fissures after preparation of the implant sites (Fig. 3B). Thereafter, a releasing incision was made between the periosteum and the palatine process. After adequate hemostasis, the incision was closed using 4-0 silk sutures in a single layer. The right palatine fissure remained untreated. After the prescribed experimental period, the animals were killed and examined for gross anatomical changes, micro-CT imaging, and histological analyses. Postoperatively, the animals were fed a powder diet.
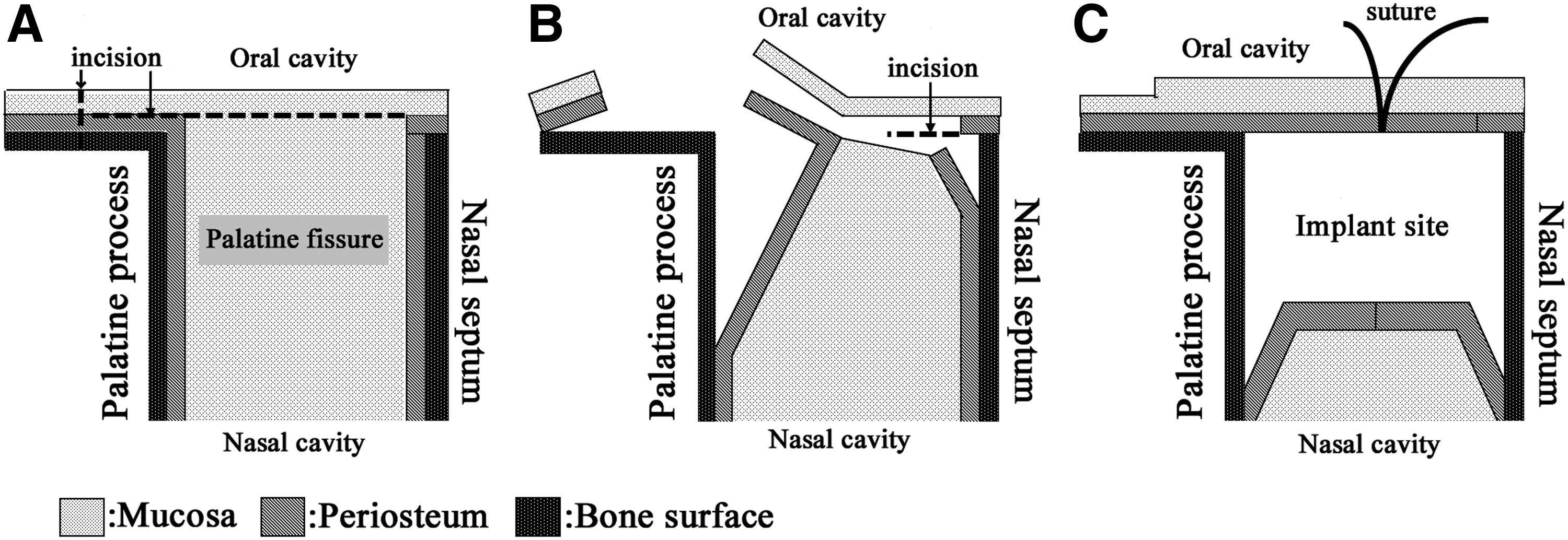
Schematic drawing of how to expose the palatine fissure and make an implant site. This schematic drawing is the palatine fissure of a rat in the frontal section.

The image of operative method of autologous bone graft.
Preparation of implants
After all 20 rats received a palatine fissure on the left side, they were randomly subdivided into 3 groups based on the implants administered: group 1 received an autogenous bone graft, group 2 received β-TCP (OSferion®; Olympus Terumo Biomaterials Corp., Tokyo, Japan), and group 3 received a blank defect in which no material was implanted in the implant site in the cleft palate on the left side. For group 1, autologous bone chips were collected from the tibia bone. In brief, a 10 mm skin incision was made along the inferior border of the tibia. The muscle and periosteum flap were elevated from the tibia. A 2 mg mixture of cortical bone with cancellous bone was cut with an osteotome (Fig. 3C). The autologous bone chips were stored in saline until implantation. After the muscle and periosteum flaps were repositioned, the skin incision was closed to ensure healing by primary intention. For group 2, commercial β-TCP was used as a representative bone substitute material. The granule size of β-TCP was 0.5–1 mm and the pore size was approximately 250–400 μm.
Micro-CT imaging and analysis of hard tissue formation
We divided 15 of the 20 rats into 3 groups for micro-CT analysis. In vivo X-ray micro-CT (Cosmo Scan GX; Rigaku Corporation, Tokyo, Japan) was used for imaging as previously described.14–16 The exposure parameters were 18 s, 90 kV, and 100 μA. The isotropic voxel size was 45 μm. Hard tissue regeneration images were obtained from each rat at 4, 8, 12, and 16 weeks after surgery. Bone volume was measured in the regions of interest (ROIs) from voxel images using the bone volume measuring software 3 by 4 viewer 2011 (Kitasenjyu Radist Dental Clinic i-VIEW Image Center, Tokyo, Japan). The ROI size was 1.8 × 2.7 × 0.9 mm, which covered the space used for implantation. The bone volume and bone mineral density (BMD) in the ROI were measured before surgery and at 4, 8, 12, and 16 weeks after surgery. The increases in bone volume and density in individual rats were then calculated by subtracting the value measured before implantation from the subsequent values measured at 4, 8, 12, and 16 weeks after surgery. 17
Histological analysis
We divided 15 of the 20 rats into 3 groups for histological analysis at 16 weeks after surgery. In addition, the other five rats were used for histological analysis at 12 weeks after surgery. The animals were killed in a CO2 bath and the harvested specimens were fixed in 4% neutral-buffered paraformaldehyde for 24 h, decalcified in 10% ethylenediaminetetraacetic acid disodium salt (Muto Pure Chemicals, Tokyo, Japan) for 8 weeks, dehydrated through a graded series of ethanol solutions, and then embedded in paraffin. Specimens were prepared as horizontal plane sections (5 μm thick) with a microtome (Leica RM2165; Leica Microsystems, Nussloch, Germany), and the paraffin sections were stained with hematoxylin and eosin (H&E). To observe the osteoblast and osteoclast, the paraffin sections were stained with alkaline phosphatase (ALP) and tartrate-resistant acid phosphatase (TRAP; Sept. Sapie Co., Ltd, Tokyo, Japan).
Statistical analysis
Data are expressed as mean and standard deviation for each group. Statistical analysis was performed using Excel Statistical File software (ystat2008.xls; Igakutosho-Shuppan Ltd., Tokyo, Japan). One-way analysis of variance with a Tukey–Kramer post hoc test was used for intergroup comparisons. p < 0.05 was considered statistically significant.
Results
Observation of palatine fissure in rat
Palatine fissures were not grossly visible in the oral cavity of the rat (Fig. 1A). However, when the palatal mucosa was removed, two congenital bone defects were visible in the maxilla. The size of one side of the palatine fissure was 10 × 3 × 5 mm in length, width, and depth, respectively (Fig. 1B). The left and right palatine fissures were separated by the nasal septum and connected to the nasal cavity as assessed by histological observations (Fig. 1C, D).
Clinical results
The operative procedures were well-tolerated by all rats. No wound dehiscence, severe inflammation, or swelling was observed in any of the samples throughout the experimental period. The animals showed no weight reduction during the healing time.
Micro-CT findings before and after implantation of materials to palatine fissure
The presence of both sides of the palatine fissures was easily confirmed in the maxilla using micro-CT images (Fig. 4). Either transplanted bone or newly formed bone formation at the margins of the left palatine process of the maxilla was noted on the radiographs of all samples in group 1 at as early as 4 weeks after transplantation. Three patterns of newly formed hard tissue were observed by 12 weeks after autologous bone chip transplantation, as given in Figure 4. The new hard tissue was observed in anterior (Fig. 4A), central (Fig. 4B), and posterior (Fig. 4C) of the left palatine fissure by 12 weeks. The transplanted bone chips clearly remained in the palatine fissure (Fig. 4A, B), but in one sample, were slightly observed radiologically in the left palatine fissure by 12 weeks (Fig. 4C). The bone union was observed between the nasal septum and left palatine process of the maxilla at 8 weeks after transplantation (Fig. 4C). In other samples, the bone union was observed between the nasal septum and palatine process only at 16 weeks after transplantation (Fig. 5A, B). However, the location of the bone union formed differed among the samples. Transplanted bone resorption was not yet completed at 16 weeks (Fig. 5A, B). When β-TCP particles were implanted into the palatine fissure, new bone was clearly deposited along the margins of the left palatine process as observed for the autologous bone chips. The bone union was observed in the anterior region of the palatine fissure at 16 weeks (Fig. 5C). Although a substantial amount of β-TCP particles remained in the palatine fissures at 4 and 8 weeks after implantation (data not shown), it was difficult to find remnant β-TCP particles on the radiographs at 16 weeks (Fig. 5C). In group 3, no newly formed hard tissue was visible in the left palatine fissure by 16 weeks in any of the samples (Fig. 5D).
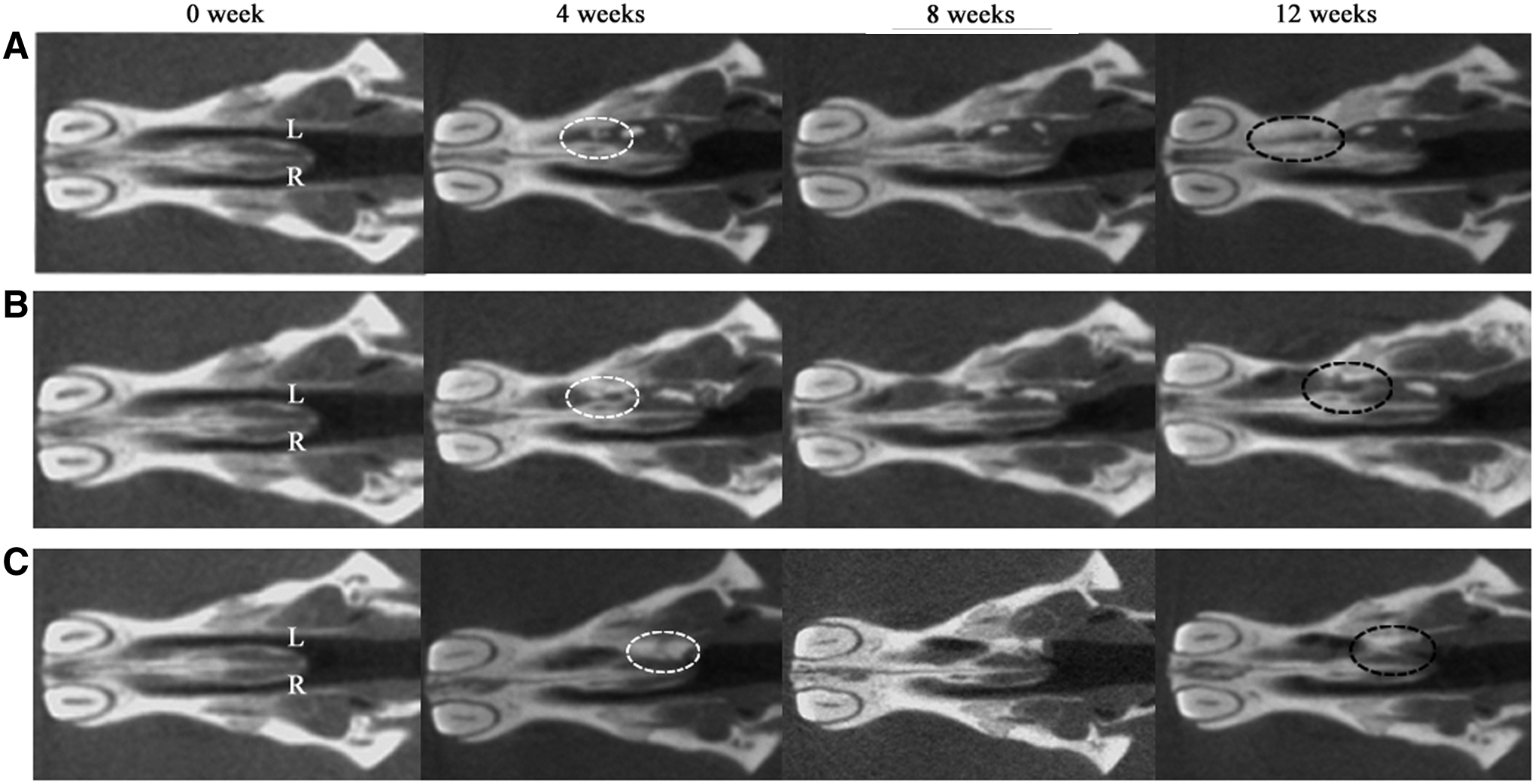
Micro-CT images of palatine fissures in the horizontal plane section. Each image is in group 1 rats before the transplantation and at 4, 8, and 12 weeks after the transplantation, respectively. The images show three of five rats in group 1. At 12 weeks after transplantation, the hard tissue (dashed line area) was visible in anterior site of the left palatine fissure
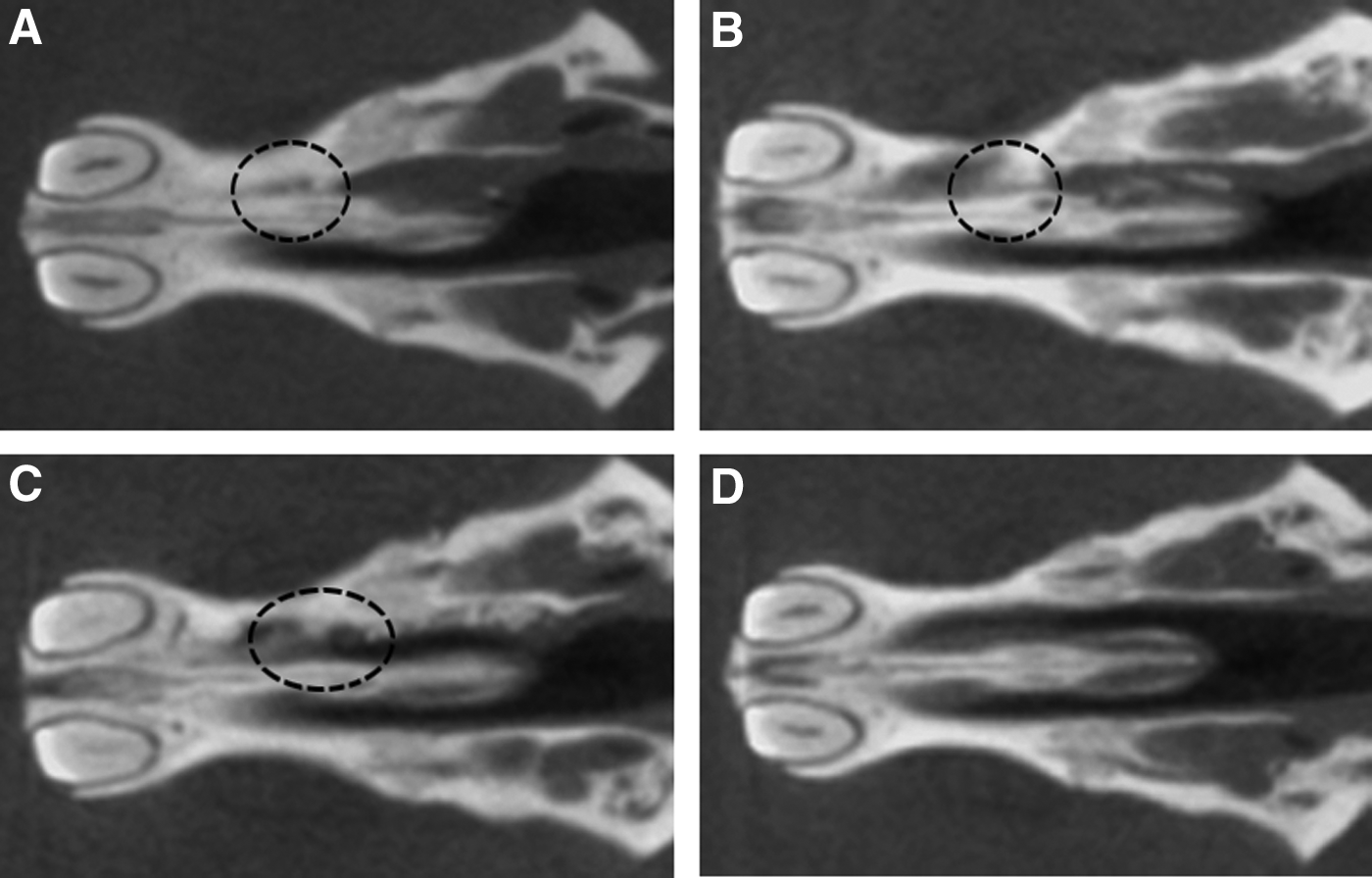
Micro-CT images of the palatine fissure at 16 weeks after operation.
To evaluate the autologous bone grafting, we calculated the bone volume and BMD of the implant sites at 4, 8, 12, and 16 weeks after operation. Bone volume was significantly decreased from 4 to 8 weeks after transplantation, but it was significantly increased from 12 to 16 weeks after transplantation in group 1. To evaluate the differences between autologous bone chip and β-TCP in bone formation, we calculated the bone volume and BMD of the implant sites. The bone volume and BMD in group 1 were significantly higher than those of the rats in group 2 at 16 weeks. There was no difference in the BMD of original cortical bone (729 mg/cm3) from that in group 1 (Fig. 6A, B).
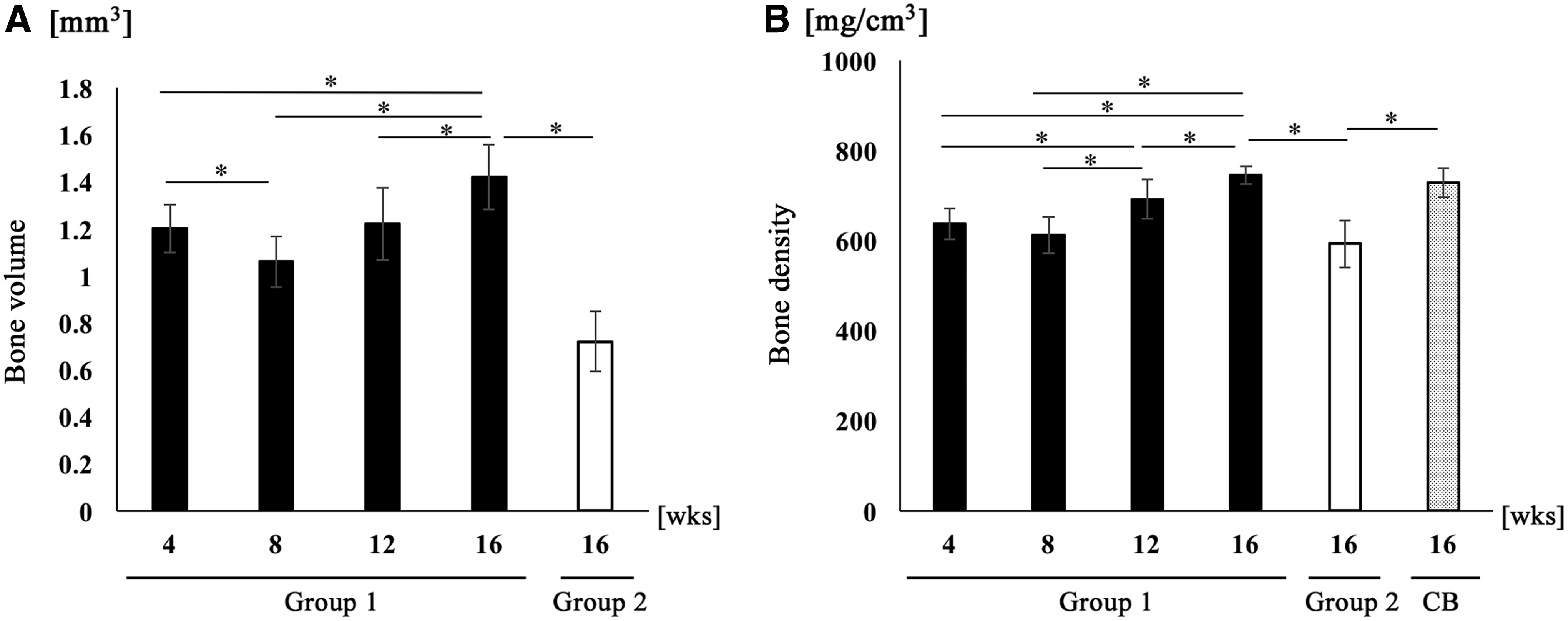
Micro-CT analyses of the palatine fissure at 4, 8, 12, and 16 weeks after operation.
Histological analysis
The left and right palatine fissures separated with the nasal septum were easily identifiable by histological observations (Fig. 1C, D). At low magnification, a large number of inflammatory cells were observed around the bone chips at 12 weeks in group 1 (Fig. 7A). At higher magnification (framed areas in Fig. 7A), the new bone formation was observed and the cells were recognized in the newly formed bone. On the contrary, bone lacuna without cells was observed in the bone. The boundary was unclear between the bone with cells and the one without cells (Fig. 7B). At higher magnification (Fig. 7B), many osteoblasts stained with ALP were noted along the surface of newly formed bone (Fig. 7C). There were also some multinucleated giant cells observed on the surface of newly formed bone. The cells stained with TRAP were located in Hawship's lacuna (Fig. 7D).
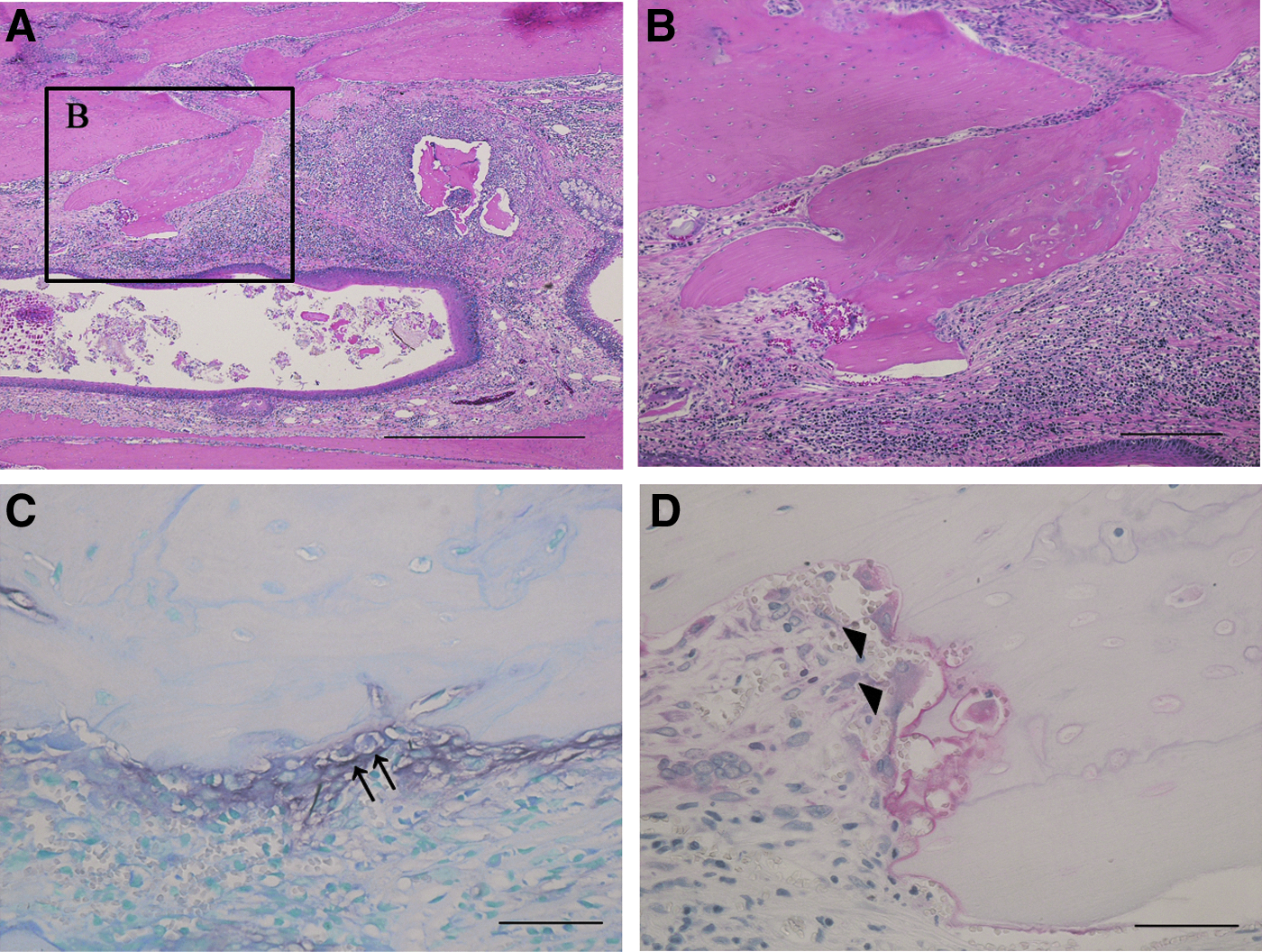
Histological images of rat palatine fissure in horizontal plane section at 12 weeks after implantation in group 1.
All samples obtained from both groups 1 and 2 contained remaining graft particles of bone and β-TCP, respectively, at 16 weeks after implantation (Fig. 8A, E). The histology showed direct bone deposition on β-TCP and a layer of woven bone that contained cells, a characteristic of new bone formation, in all samples (Fig. 8E). Higher magnification images (framed areas in Fig. 8A, E) showed abundant woven bone ingrowth in groups 1 and 2 (Fig. 8B, F). The border between the preexisting bone and the newly formed bone was clearly visible. Osteocytes in the lacunae were present in newly formed bone (Fig. 8B, F). At higher magnification (framed area in Fig. 8A, E), many osteoblasts were noted along the surface of newly formed bone and stained with ALP (Fig. 8C, G). There were also a few multinucleated giant cells observed on the surface of newly formed bone. The cells were located in Hawship's lacuna and stained with TRAP in both groups (Fig. 8D, H).
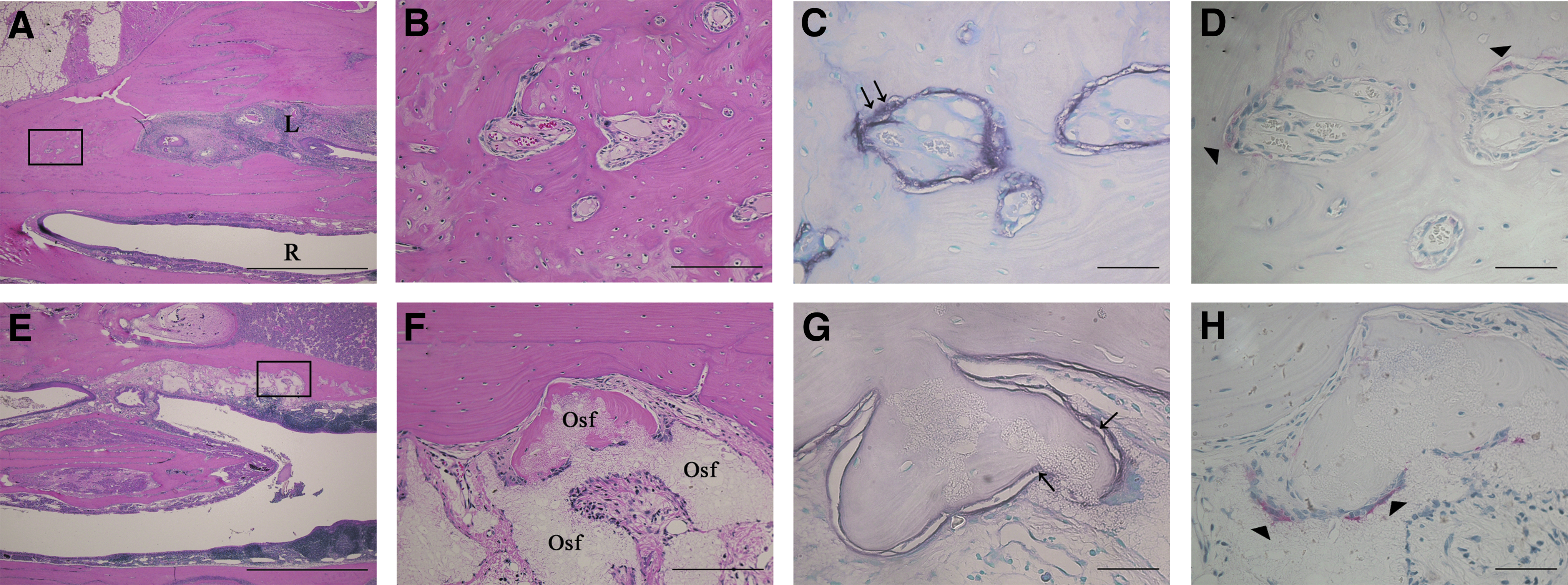
Histological images of rat palatine fissure in horizontal plane section at 16 weeks after implantation.
Of interest, there were substantial differences in the histological structure of the epithelium before and after operation in all groups. Before the operation, both the epithelium covering the nasal septum and that of the palatine process of the maxilla showed a pseudostratified ciliated columnar structure (Fig. 9A). The higher magnification view of the framed area in Figure 9A showed a large number of nasal glands (Fig. 9B, C). However, after operation, only with the periosteal elevation without the implantation of materials, the newly formed bone was covered with a stratified squamous epithelium on both sides (Fig. 9D). Higher magnification of the framed areas in Figure 9D showed connective tissue similar to the lamina propria under the stratified squamous epithelium on both sides (Fig. 9E, F).
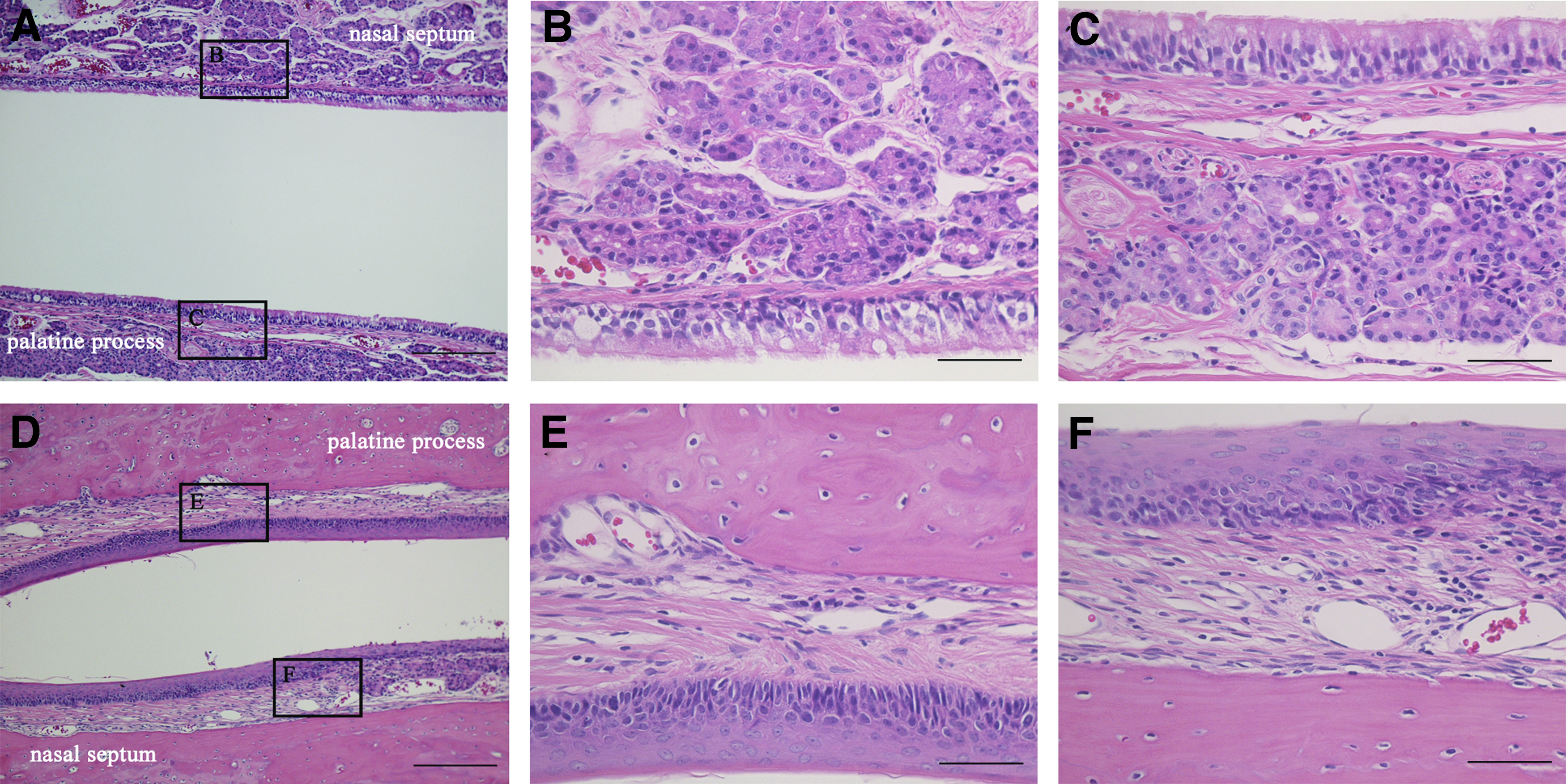
Histological images of the epithelium covering the nasal septum and palatine process in the horizontal section at 16 weeks after operation in group 3. The images show periosteal elevation changed the epithelial structure covering the nasal septum and palatine process.
Discussion
One of the most difficult challenges of a cleft palate–lip repair operation is reconstruction of alveolar cleft. Undoubtedly, an autogenous bone graft is the most commonly used reconstruction material for this purpose; however, this method has important drawbacks, including pain at the donor site, development of deformity, possible injury to adjacent anatomical structures, prolonged surgical duration, prolonged hospitalization, and loss of grafted bone.18,19 Thus, it is important to develop and evaluate candidate bone substitute materials to reconstruct an alveolar cleft while reducing or preventing these complications at donor site after an autologous bone graft. 20 In this study, we developed a novel and more suitable experimental model for evaluating new bone substitute materials and their bone formation potential that could more appropriately mimic human alveolar cleft.
In general, rats are favored as an appropriate animal model for alveolar cleft research as an accurate, stable, reproducible, and cost-effective animal model.17,21,22 Because the innate rat palatine fissure shows no bone continuation, and fibrous connective tissue interposes between the palatine process and nasal septum, we decided to utilize the palatine fissure as a model for testing a novel bone substitute material for alveolar cleft reconstruction. We focused on the palatine fissure for three main reasons. First, this is a congenital bone defect in the oral cavity. Second, the palatine fissure is surrounded by bone on two sides and the remaining two sides are covered with mucosal membrane of both the palatal membrane and nasal membrane. Third, the palatine process and nasal septum maintaining the space of the palatine fissure throughout the animal's lifetime. Taken together, we concluded that the rat palatine fissure anatomically imitates human alveolar cleft more closely than a surgically created critical sized defect. To our knowledge, this is the first article describing the similarities of the palatine fissure with human alveolar cleft.
We decided to test the possibility of the palatine fissure to imitate human alveolar cleft. We selected autologous bone chips and β-TCP granules as the graft materials. Autogenous bone is currently the gold standards for alveolar cleft treatment, and commercial β-TCP have already been used in oral and maxillofacial surgery such as for sinus floor augmentation and repair of deficient alveolar bone in implant therapy in clinical settings.20,23–28 However, the potential of β-TCP for reconstruction of human alveolar cleft is not well established. Owing to its high radiaopacity, it was not possible to assess the replacement of β-TCP by newly formed bone using micro-CT until 12 weeks. In our study, we found a significant difference in the newly formed bone quantity between the autologous bone graft and β-TCP graft group at 16 weeks. Specifically, there was less bone formation with β-TCP according to two dynamic parameters, bone volume and BMD. This result is in contrast with previous studies that have generally shown a similar effect regarding maxillary sinus augmentation or edentulous alveolar ridge augmentation using autogenous iliac bone or β-TCP grafts.29,30 The most likely reason to explain these discrepancies from previous results is the differences in the location of the implant site, including the maxillary sinus, edentulous alveolar ridge, and palatine fissure. The potential of bone repair in the maxillary sinus and alveolar ridge could be higher than that in the palatine fissure because the preexisting bone has a spontaneous healing potential when it is damaged, whereas the bone of the palatine process surrounding the palatine fissure has a poor repair property. Furthermore, β-TCP functions only during an osteoconduction process, whereas abundant growth factors for osteoinduction and osteoconductivity are expected to be present in autogenous bone. Their functional difference precisely matches the difference in the degree of new bone formation. Because the location of the rat palatine fissure better reflects the implant site of human alveolar cleft, this model is more suitable to evaluate new bone graft materials for alveolar cleft reconstruction. Namely, this study indicated that the palatine fissure is a feasible model to develop novel bone substitute materials as an alternative to an autogenous bone graft.
Various reports have shown that the degradation rate of β-TCP depends not only on its porosity and pore size but also on the implant sites.31–33 Although a small amount of β-TCP particles remained in the palatine fissures at 16 weeks after implantation in our study, previous study also reported that 55% of β-TCP was degraded after 24 weeks of implantation in a rabbit model. 34 The degradation of β-TCP in vivo is reported to involve two pathways: solution-mediated dissolution and a cell-mediated resorption process.35,36 Because multinucleated giant cells were found on the β-TCP, it is likely that a cell-mediated resorption process was the predominant cause of β-TCP degradation in the palatine fissures in our study.
Conclusion
We have provided the first demonstration of the suitability of the rat palatine fissure as the implant site for bone graft materials to simulate the implantation of bone graft materials into human alveolar cleft. This new experimental model does not require surgical creation of the defect, the size and extent of the congenital bone defect of this animal is standardized for all rats, and the anatomical structure matches that of human alveolar cleft. Using this experimental model, we demonstrated that bone volume and BMD from the implantation of an autologous bone graft was greater than that obtained with β-TCP. Further study is warranted using this model toward developing a novel bone substitute for alveolar cleft treatment.
Footnotes
Disclosure Statement
The authors confirm that there are no known conflicts of interest associated with this publication.
Funding Information
This work was supported by Japan Society for the Promotion of Science (JSPS) KAKENHI Grant Number JP16K11703.