
Abstract
Background:
Clinically available cartilage, such as large-volume tissue-engineered cartilage, is urgently required for various clinical applications. Tissue engineering chamber (TEC) models are a promising organ-level strategy for efficient enlargement of cells or tissues within the chamber. The conventional TEC technology is not suitable for cartilage culture, because it lacks the necessary chondrogenic growth factor, which is present in platelet-rich plasma (PRP). In this study, we added autogenous auricular cartilage fragments mixed with PRP in a TEC to obtain a large amount of engineered cartilage.
Experiment:
To prove the efficacy of this method, 48 New Zealand white rabbits were randomly divided into 4 groups: PRP, vascularized (Ves), PRP, PRP+Ves, and control. Auricular cartilage was harvested from the rabbits, cut into fragments (2 mm), and then injected into TECs. Cartilage constructs were harvested at week 8, and construct volumes were measured. Histological morphology, immunochemical staining, and mechanical strength were evaluated.
Results:
At week 8, PRP+Ves constructs developed a white, cartilage-like appearance. The volume of cartilage increased by 600% the original volume from 0.30 to 1.8 ± 0.1789 mL. Histological staining showed proliferation of edge chondrocytes in the embedded cartilage in the PRP and PRP+Ves groups. Furthermore, the cartilage constructs in the PRP+Ves group show mechanical characteristics similar to those of normal cartilage.
Conclusions:
Auricular cartilage fragments mixed with PRP and vascularization of the TEC showed a significantly increased cartilage tissue volume after 8 weeks of incubation in rabbits.
Impact Statement
Repair of defects of ear cartilage tissue has always been a huge challenge to plastic surgeons. In this article, a new method is presented to produce within 8 weeks auricular cartilage in a tissue engineering chamber without cell culture. Having such a method is a valuable step toward creating a large volume of functional cartilage tissue, which may lead to successful construction of normal auricular structure with minimal donor-site morbidity.
Introduction
Total and subtotal reconstruction of auricle defects remains challenging for plastic surgeons. Some surgeons have reported using rib cartilage, the current golden standard, to carve a neo-framework, resulting in aesthetically acceptable results.1,2 However, this procedure is inevitably associated with donor site morbidity. To address this issue, the field of cartilage tissue engineering has emerged in the last 30 years. For example, in 1997, Cao et al. engineered cartilage using a human auricle shape implanted into the back of nude mice; since then, many researchers have explored strategies for constructing tissue-engineered cartilage. 3
Cartilage is a type of avascular tissue, and chondrocytes were expected to be easily cultured in vitro. 4 However, although isolated chondrocytes survive and proliferate robustly in vitro during cell culture, after several passages of monoculture, cells lose their natural phenotype and undergo degeneration.5,6 In contrast, mesenchymal stem cells (MSCs), including adipose-derived stem/stromal cells, show great proliferation efficiency but exhibit a hypertrophic morphology after the induction of chondrogenic differentiation. 7 Therefore, coculture strategies have been developed to circumvent some of the limitations of utilizing chondrocytes or MSCs alone. However, the risk of contamination during cell culture has limited the clinical use of this approach.7–9
Yanaga et al. generated clinically available cartilage stacking cultured monolayer chondrocytes into multilayer structure and using platelet-rich plasma (PRP) as a scaffold and implanted these multilayered chondrocyte constructs into the abdomen. Subsequently, after 6 months of implantation, a mature cartilage block was formed with sufficient elasticity for use as auricular cartilage. 10 These findings demonstrated that multilayered chondrocyte constructs in combination with PRP can imitate the structure of cartilage, thereby promoting the regeneration of chondrocytes and consequently generating engineered cartilage bricks in vivo. In addition, Kawanabe and Nagata demonstrated that re-embedding sliced rib cartilage into the empty pocket of the perichondrium can stimulate the regeneration of cartilage; 6–12 months were required to regenerate cartilage tissue in the perichondrium pockets. 11 This finding suggests the possibility of using sliced cartilage as a cell source for cartilage tissue engineering.
As a follow-up of the above mentioned, organ-level tissue engineering strategies 12 and tissue engineering chambers (TECs) 13 were introduced to produce a clinically relevant amount of cartilage. However, these culture techniques still take too long and therefore lacks clinical application value. By introducing an intrinsic vascular component into a rigid chamber, TECs can stimulate the regeneration of cells 14 or tissues15,16 in the chamber. Our team previously used TECs to develop adipose flaps with a volume of over 80 mL in rabbits. 17
Consequently, PRP, which contains both chondrogenic and angiogenic factors, was introduced by us into the TEC as a method to optimize this technology for the production of a large amount of viable engineered cartilage.
Methods
Rectangular-shaped TECs, made of silicone rubber, were used. They had an inner length of 20 mm, forming a 3.2-mL wide space with a height of 8 mm. All chambers were perforated with side holes measuring 1 mm in diameter. The base had four suture holes for fixation, allowing the chamber to be anchored to the surrounding tissues.
Rabbits were used, as experimental animal, and anesthetized with 30 mg/kg of 3% pentobarbital. Lidocaine was applied to the operative area by multipuncture of 0.5 mL/site. The surgery process is shown in Figure 1. First, a 1 × 1 cm portion of auricular cartilage was harvested from both ears of a rabbit. The 1.5-cm incision was closed immediately using nylon sutures. The harvested cartilage was cut using a lancet into 1–2-mm3 blocks. Then, a moderate amount (10 mL) of whole blood was drawn through the marginal ear vein and centrifuged to prepare PRP, as reported by Wu et al., 18 and immediately transferred to sterile tubes containing heparin. Samples were centrifuged (Eppendorf) for 10 min at 215 g, resulting in three layers. Plasma layers were then removed and subjected to another 10-min centrifugation at 863 g to obtain platelet-poor plasma (PPP) and PRP. The PPP was discarded, while thrombin was added to the PRP to change it into a hydrogel state. Finally, PRP and diced cartilage were mixed and loaded into a 1-mL syringe.
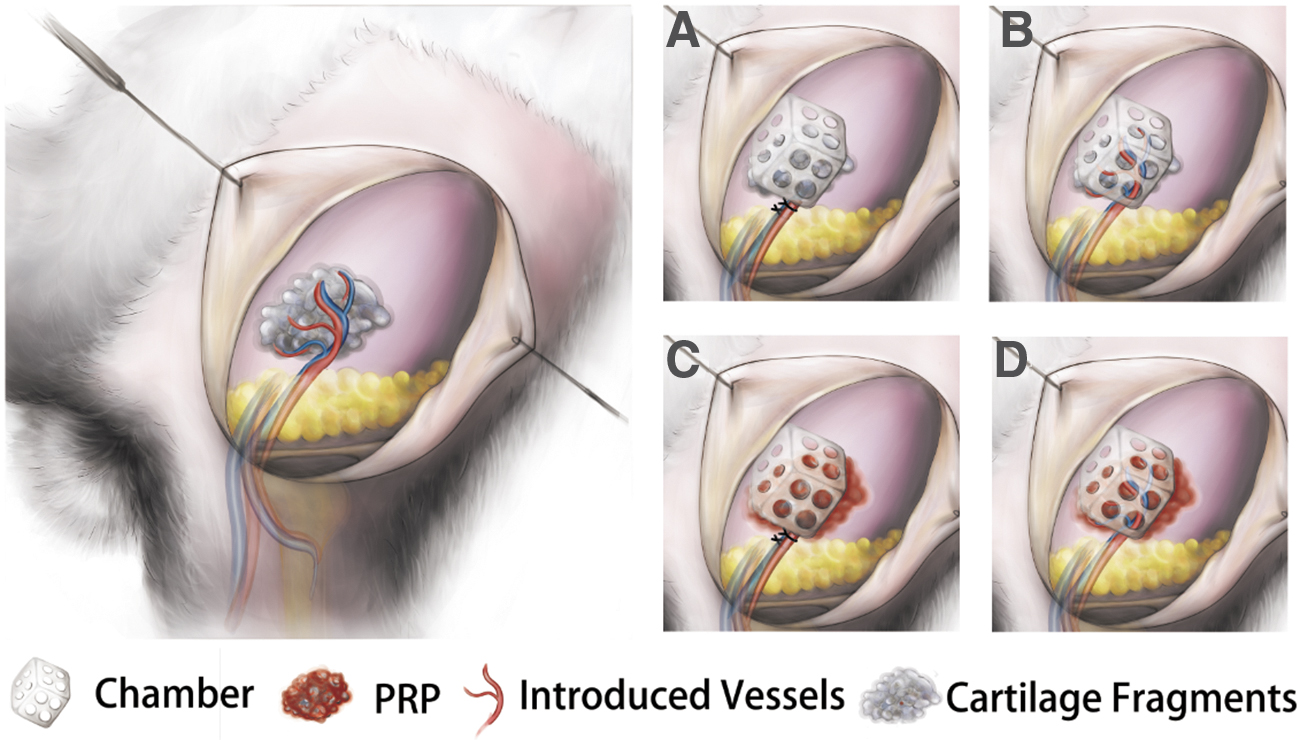
Schematic diagram of the experimental model of cartilage tissue engineering chamber. Left: the vessels we used and the surgical area.
Subsequently, a 3-cm incision was made in the skin of the inguinal area. A subcutaneous pocket was created around the incision, and the femoral artery bundles were recognized and isolated. Then, the perforated TEC was installed and fixed using 3-0 nylon for the isolated artery. Subsequently, cartilage with PRP was injected into the chamber through the base of the chamber. Finally, the wound was closed with 4-0 nylon. Postoperatively, penicillin was administered intramuscularly to prevent infection. After 8 weeks of implantation, rabbits were euthanized and the cartilage was harvested for further analysis.
Experiment
Experimental design
Animals
Forty-eight New Zealand white rabbits (weight: 2.5–3.0 kg, age: 3–4 months) were used in this study. All rabbits were purchased and housed at the Experimental Animal Center of Fujian Medical University. All experiments were performed with the approval of the Ethics Committee of our hospital and the Experimental Animal Center of Fujian Medical University (FJMU IACUC2018-0002).
After anesthesia, auricular cartilage of the ears of the rabbits was dissected and PRP was prepared and loaded with cartilage fragments according to the description in the Methods section. Then, subcutaneous pockets were created in the inguinal area and TECs installed. Subsequently, cartilage with or without PRP was injected into the chamber through the base of the chamber. Therefore, the rabbits were randomly divided into four groups as shown in Figure 1: (1) PRP group (1.0 mL PRP was mixed with 0.30 mL cartilage fragments and injected into the TEC), (2) Ves group (the femoral artery was dissected and left in situ in the TEC, which was injected cartilage fragments only), (3) PRP+Ves group (the femoral artery was dissected and left in situ in the TEC, which was injected with cartilage fragments mixed with PRP), and (4) Control group (cartilage fragments only were injected into the TEC).
Finally, the wounds were closed with 4-0 nylon. Postoperatively, penicillin was administered intramuscularly to prevent infection.
Tissue harvesting
Animals were euthanized at 8 weeks. Constructs were harvested and carefully removed from chambers via separation from the surrounding tissue. The volumes were measured by drainage after imaging with a digital camera. Harvested cartilage was placed in a 5 mL syringe, to which 3 mL saline has been added in advance. The volume measured by the syringe minus 3 mL is the cartilage volume. All samples were prepared for subsequent analyses.
Histological examination
All samples were fixed in 4% paraformaldehyde, dehydrated, and embedded in paraffin. Specimens were then sectioned serially (5-μm thickness) along the longitudinal axis. The sections were stained with hematoxylin and eosin (H&E), safranin-O, Verhoeff-Van Gieson, and Masson's trichrome stains or immunostained for Ki-67. Sections stained with H&E were used to determine chondrocyte viability, chondroid tissue status, and the structure of the surrounding tissues, whereas sections stained with Masson's trichrome stain were used to determine the collagen content of the construct tissue matrix (green color). Safranin-O staining was used to determine the proteoglycan content of the matrix (red color). Sections stained with Verhoeff-Van Gieson were used to assess chondroid tissue matrix metachromasia and the density of vessels. Ki-67 immunohistochemistry was used to identify the locations of chondrocyte proliferation in the specimen (brown deposits in the nucleus). In brief, the sections were treated with 0.3 vol% hydrogen peroxide in methanol solution, and blocked with 1 wt% bovine serum albumin in phosphate buffered saline for 30 min. Then, primary antibodies (ab15580; Abcam) were incubated overnight at 4°C. Following the incubation, the samples were treated with peroxidase-conjugated secondary antibody (ab6721; Abcam). The immunoreactions were visualized by DAB substrate in chromogen solution. The samples were counter stained with hematoxylin. All sections were assessed by microscopy (Olympus).
Histopathological analysis
The degree of cartilage fibrosis was calculated as a percentage of the stained area (not including the capsule area) divided by the total tissue area of the sections using ImageJ software (National Institutes of Health, Bethesda, MD). The microvessel density of the capsule was calculated as a percentage of the stained microvessel area divided by the total tissue area of the sections using ImageJ software and we took the five random areas with the highest blood vessel density section under the microscope, and express the microvessel density as the ratio of the area occupied by blood vessels to the visual field area. Cartilage-specific extracellular matrix (ECM) was calculated as a percentage of the stained area (Safranin-O staining and Verhoeff-Van Gieson staining) divided by the total tissue area of the sections using ImageJ. Cell proliferation was calculated as a percentage of the Ki-67 positive cells divided by the total cell number of the sections using ImageJ software.
Mechanical test
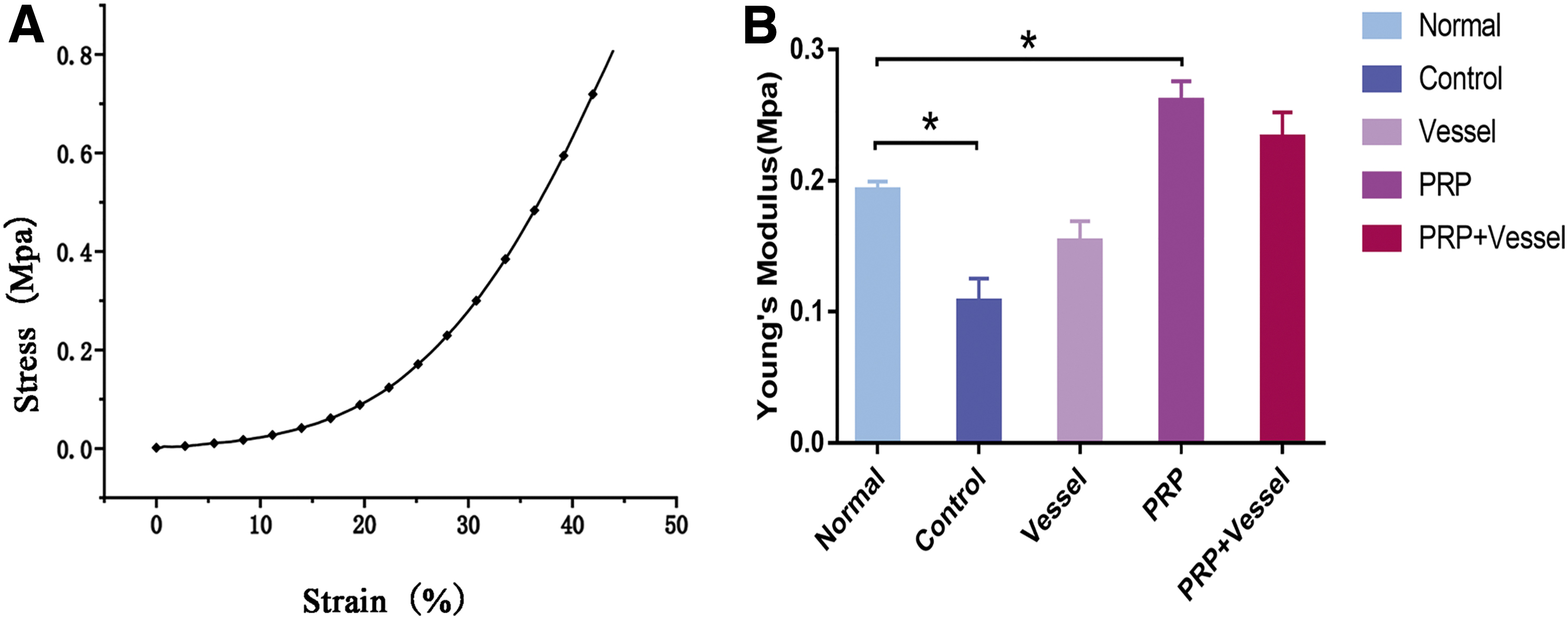
The biomechanical properties of the engineered cartilage were determined using a texture analyzer (Stable Micro System). The samples were processed to a rectangular shape by means of refinement; cylindrical samples had a 5-mm side length and 2 mm thickness. A constant compressive strain rate of 2.0 mm/s was applied until 80% of the maximum deformation was achieved, and a stress-strain curve was generated. The Young's modulus was calculated based on the slope of the stress-strain curve.
Statistical analysis
All quantitative data were expressed as means ± standard deviations. Statistical analyses were carried out with GraphPad Prism 7.0 software. Comparisons between groups were performed by random data two-way analysis of variance. Significance was established for differences with p-values of <0.05.
Experimental Results
Macroscopic observations
At the end of 8 weeks, every animal developed a vascularized double-layered fibrous capsule around the implanted engineered cartilage and the implanted chambers. Only the constructs in the PRP+Ves group filled the chamber and were shaped by the chamber into a square cube. The diced cartilage formed an integral tissue in all groups (Fig. 2). However, from the cross-section view, we could distinguish clear borders of the implanted cartilage in the control group. In contrast, the borders in the PRP and PRP+Ves groups were blurred compared with that in the control group. The femoral vessels in the Ves and PRP+Ves groups, which had been transplanted and fixed in the chamber, were fully incorporated into the capsule on the constructed tissue surface (Fig. 3A).

Tissue-engineered cartilage in the group of control, Vessel, PRP, and PRP + Ves under gross view and cross section. Color images are available online.
Cartilage volume increased in all groups
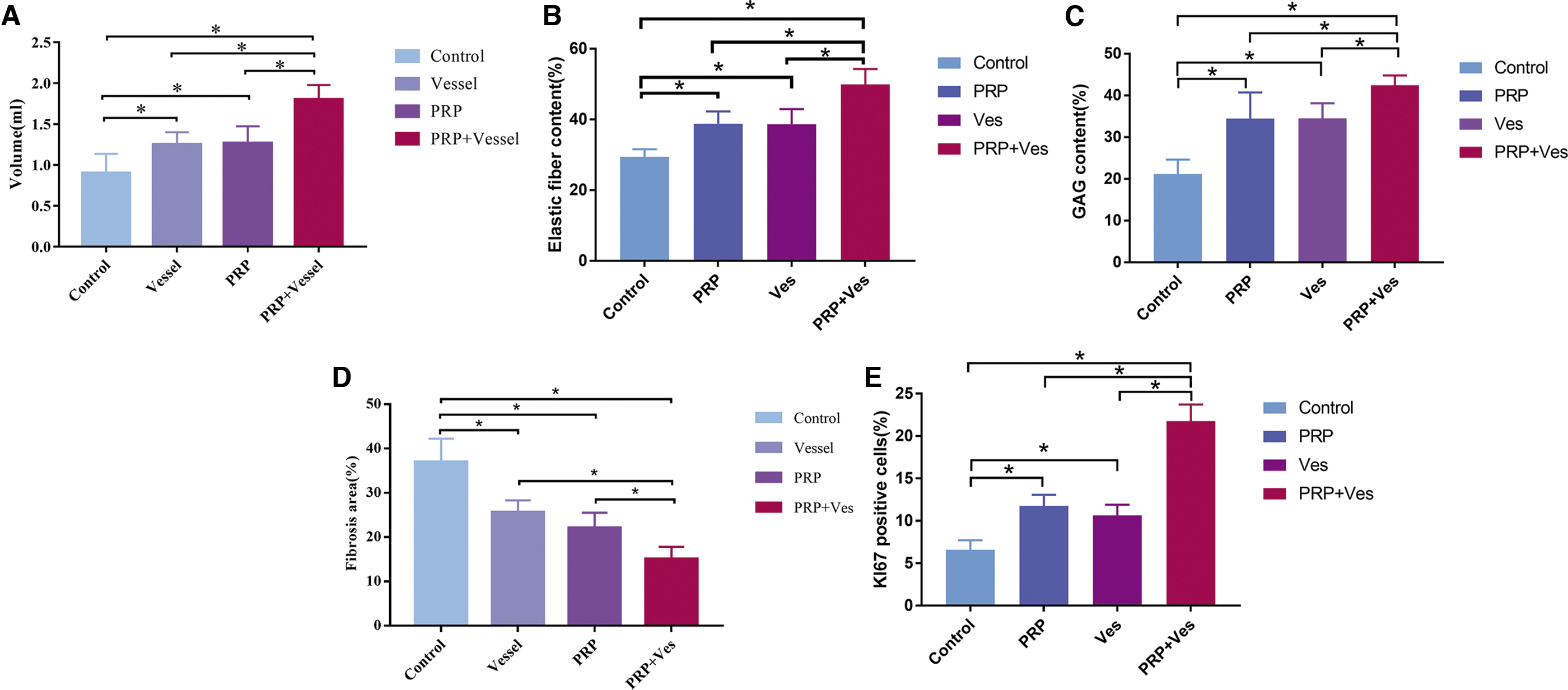
The initial volume of cartilage was 0.30 mL in each group. The volumes of all constructs were significantly higher than their initial volumes (p < 0.05). The volume in the PRP+Ves group increased by 600% to 1.80 ± 0.18 mL, and this volume was significantly higher than those in the other three groups (Fig. 4; p < 0.05). Moreover, the volumes in the Ves and PRP groups increased to 1.25 ± 0.15 and 1.26 ± 0.21 mL, respectively. Overall, the volumes in all experimental groups were significantly higher than that in the control group. However, there were no differences between the Ves and PRP groups in terms of the volume of engineered cartilage (p > 0.05; Fig. 4A).
The analysis of volume growth
Hematoxylin and eosin and Masson's trichrome staining of cartilage constructs
In cartilage sections for all groups, chondrocytes could be easily distinguished within the matrix. In the control and Ves groups, the embedded cartilage had clear borders by H&E staining. The original cartilage showed darker purple staining for the ECM, and the surrounding connective tissue was stained pink. Moreover, the border of original cartilage in the PRP and PRP+Ves group was blurred. On the border, the chondrocytes and collagen interdigitate with each other.
The different merging degree of the embedded cartilage and neo-tissue in all groups was confirmed by Masson's trichrome stain. Furthermore, we quantified the fibrous component according to Masson's trichrome stain using ImageJ (Fig. 4D). The control group had the highest degree of cartilage fibrosis, whereas the PRP+Ves group showed the lowest degree of fibrosis (15.02% ± 1.24%). Indeed, the control, Ves, and PRP groups showed increased blue staining (36.94% ± 2.37%, 25.61% ± 1.20%, and 22.05% ± 1.56%, respectively; p < 0.05) compared with that in the PRP+Ves group.
Safranin-O and Verhoeff-Van Gieson staining of auricle cartilage-specific extracellular matrix components
Both Safranin-O and Verhoeff-Van Gieson staining showed strong positive signals in the embedded cartilage matrix. The border of embedded cartilage and neo-tissue was clear in the control and Ves groups. Interestingly, both stains faded on the periphery of the cartilage in the PRP and PRP+Ves groups. We quantified the glycosaminoglycans and elastic fibers according to Safranin-O and Verhoeff-Van Gieson staining using ImageJ (Fig. 4C, D). The PRP+Ves group showed the highest degree of GAG content (42.48% ± 2.23%). The control, Ves, and PRP groups showed decreased GAG content (21.17% ± 1.55%, 34.5% ± 1.63%, and 34.49% ± 2.78%, respectively; p < 0.05) compared with that in the PRP+Ves group. Verhoeff-Van Gieson staining shows similar results, The PRP+Ves group showed the highest degree of elastin content (49.92% ± 1.95%). The control, Ves, and PRP groups showed decreased GAG content (29.42% ± 0.96%, 38.66% ± 1.89%, and 38.79% ± 1.56%, respectively; p < 0.05) compared with that in the PRP+Ves group.
The stainless ECM around the chondrocytes on the periphery indicated that these chondrocytes may be newly formed.
Ki-67 positive staining on the periphery of embedded cartilage revealed an outgrowth phenomenon
Ki-67 staining (Fig. 5) was positive on the periphery of embedded cartilage, demonstrating robust proliferation of chondrocytes in all groups except for the control group. Thus, Ki-67 immunohistochemical staining on the periphery revealed an outgrowth phenomenon, whereas the chondrocytes in the center showed negative staining. We quantified the Ki-67 positive cells using ImageJ (Fig. 4E). The PRP+Ves group has the highest amount of Ki-67 positive cells (21.75% ± 0.88%). The control, Ves, and PRP groups showed relatively small number of Ki-67 positive cells (6.59% ± 0.50%, 10.65% ± 0.56%, and 11.76% ± 0.59%, respectively; p < 0.05) compared with that in the PRP+Ves group.
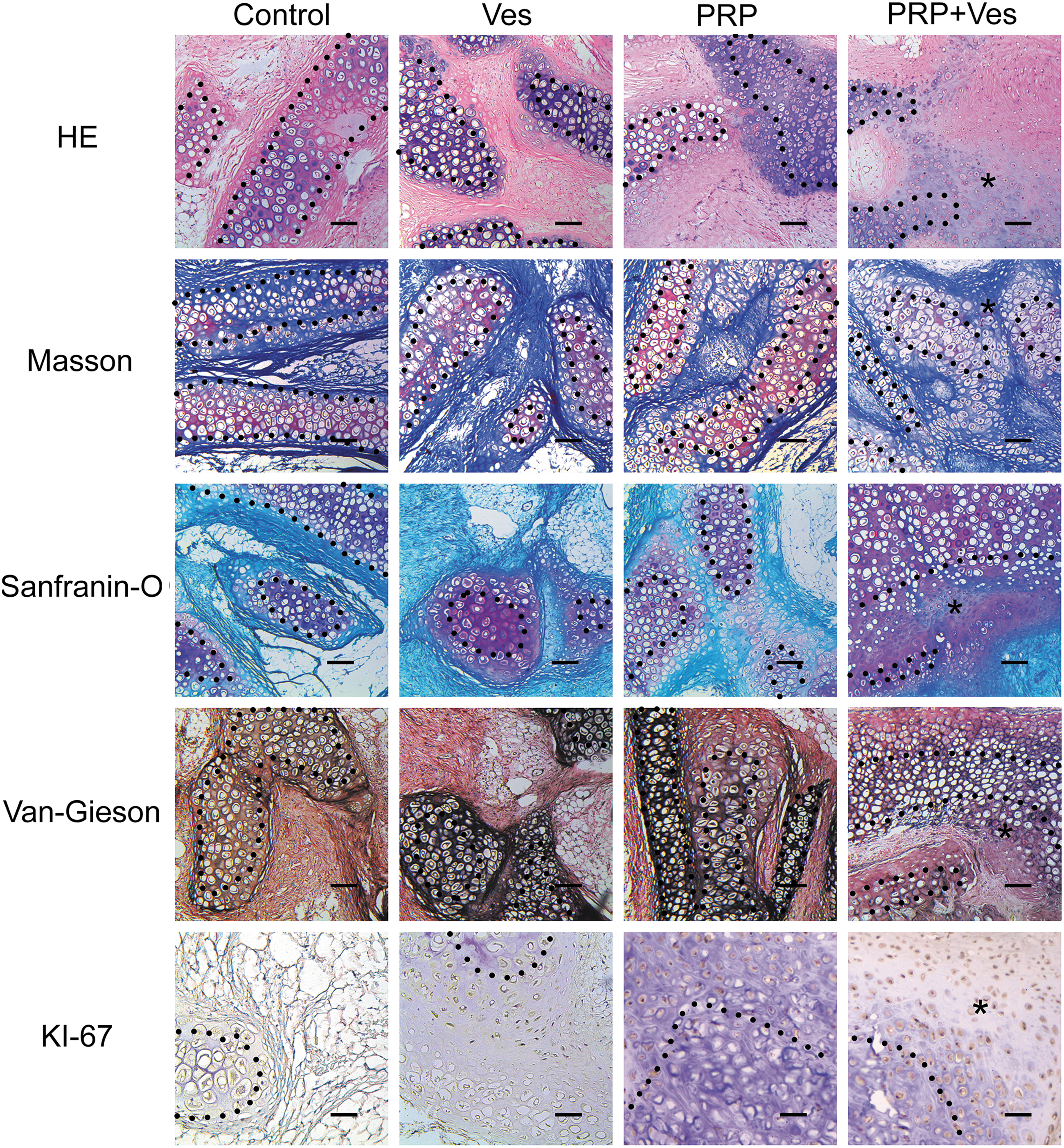
Histologic and immunohistochemical analysis of engineered cartilage tissue in each group after 8 weeks in vivo. The boundary of original cartilage block is shown by the dotted. Neocartilage formation (marked as “*”) is remarkable in P + V group. Scale bars = 100 μm. Color images are available online.
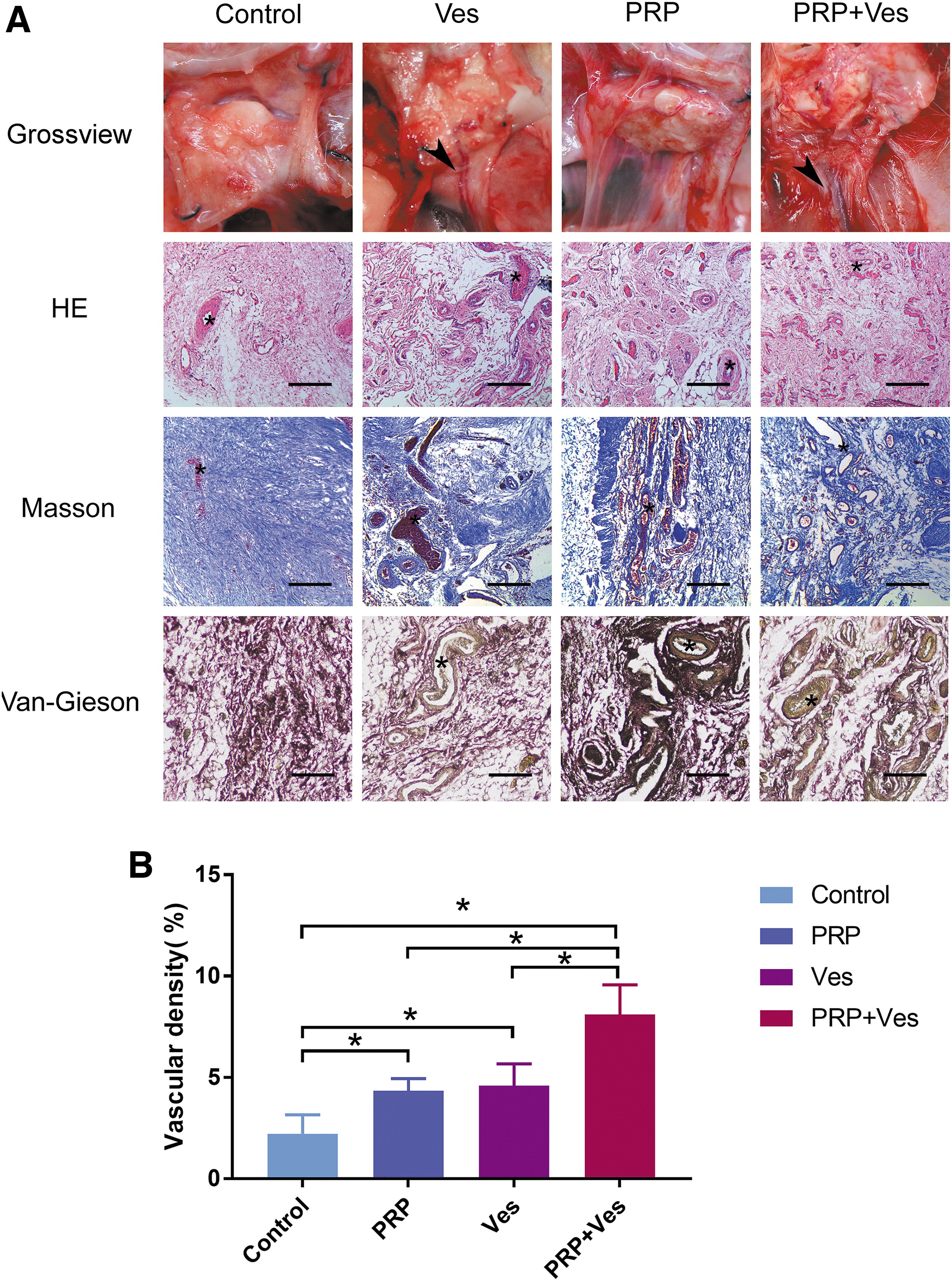
The fibrous capsule wrapping the cartilage showed vascularization
Capillary structures were more prominent in the Ves, PRP, and PRP+Ves groups than in the control group (Fig. 3A). ImageJ analysis showed that the microvessel density in the PRP+Ves group was significantly increased to ∼7.31% ± 0.92%, which was higher than those in the control, Ves, and PRP groups (2.41% ± 0.63%, 4.35% ± 0.48%, and 4.69% ± 0.64%, respectively; p < 0.05). Moreover, the microvessel densities in the Ves and PRP groups were significantly higher than that in the control group (p < 0.05). There were no significant differences between the Ves and PRP groups (Fig. 3B).
Biomechanical analyses
To further quantitatively evaluate the cartilage-like properties of the engineered constructs, biomechanical analyses were performed. The Young's modulus for samples in the Ves and PRP+Ves groups did not differ significantly from those in normal cartilage. The Young's moduli in the control and PRP groups were significantly lower than that in normal cartilage (Fig. 6B).
Discussion
Cartilage tissue engineering has recently emerged as a novel medical technology, and continuous efforts have been made to establish ear-shaped cartilage tissue engineering. 2 However, limited strategies are available for achieving clinically viable auricle reconstruction.17,19 One of the major challenges in such tissue engineering is obtaining a sufficient cell source. For cartilage tissue engineering, chondrocyte monolayer cultures tend to dedifferentiate or degenerate, 6 change phenotypically, and show altered ECM secretion. 20 Furthermore, chondrocytes from microtia cartilage showed inferior capacity to yield healthy ear chondrocytes. 21 Although many attempts have been made to slow dedifferentiation during passaging, including the use of hypoxic conditions, 22 three-dimensional (3D) bioscaffolds, 23 high-density culture, 24 growth factors, 25 and varying temperatures, 24 no efficient methods have been developed to overcome these problems. 20 Alternatively, MSCs may represent a promising cell source owing to the chondrogenic differentiation ability of these cells. 26 Chondrocytes obtained from MSC differentiation show hypertrophic morphology and expression of collagen X.4,27 Although strategies for coculture of MSCs and chondrocytes have been developed 1 to overcome the drawbacks of single cells alone, the complex procedures have made clinical use difficult owing to the necessity for optimization of coculture conditions and for increased product stability. 7
The regeneration potential of chondrocytes alone is sufficient for ear-cartilage tissue engineering. 10 Indeed, researchers have developed a two-stage strategy for ear reconstruction involving incubation of cartilage blocks. Yanaga used a multilayer culture technique involving reseeding of chondrocytes onto dedifferentiated chondrocytes under monolayer culture, causing the chondrocytes to redifferentiate again. Thus, such a multilayer structure resembling the natural structure of cartilage is crucial for the regeneration of chondrocytes. According to the study by Yanaga et al., we used auricle cartilage fragments, which maintained the natural structure of cartilage. Finally, we generated a cartilage block with a volume of ∼2 mL, which was about 600% the original volume. Histological assessment using Ki-67 staining confirmed an edge-outgrowth phenomenon. Furthermore, we found that the neo-cartilage was positive for both Safranin-O and Verhoeff-Van Gieson staining, demonstrating the auricle cartilage origin of the tissue.
After physically cutting the cartilage, small pieces of cartilage show outgrowth at the cutting edge in vivo 28 and in vitro.29,30 Although some researchers have shown limited outgrowth,31,32 no researchers have used scaffolds to optimize regeneration. Additionally, the reported observation times have always been <7 days, which is not sufficient for outgrowth. The regeneration of cartilage fragments may take more than 6 months, and the remodeling of regenerated cartilage is even sustained until 12 months, as demonstrated in a clinical study. 11 Moreover, the scaffold used for cartilage is a crucial factor determining the results of regeneration.33,34
In our study, we used PRP as the scaffold to carry cartilage fragments. PRP is an autologous extract that has low immunogenicity and some anti-inflammatory effects. 35 Recently, many studies have used PRP alone or in combination with other scaffold materials in cartilage tissue engineering.35–38 PRP is a carrier of multiple cytokines, PDGF, IGF-1, and FGF among them promoting the regeneration of chondrocytes and VEGF, TGF-1 and PDGF-BB promoting angiogenesis.39,40 Additionally, PRP forms a 3D porous fibrin structure, allowing diffusion of the surrounding components and supporting the differentiation of chondrocytes. 38 By using PRP as a scaffold, Yanaga et al. produced clinically applicable cartilage blocks. 10 Thus, we believe that PRP may be an ideal bioactive scaffold for cartilage tissue engineering.
In the PRP+Ves group, we observed merging of the neo-cartilage with the embedded cartilage. In the clinical setting, this merging is observed by about 10–12 months. 11 Thus, in PRP+Ves group, the regeneration process was accelerated. In our study, we used a TEC technique that introduced an intrinsic vessel into the constructs. 41 Although cartilage is an avascular tissue that contains chondrocytes alone, the exchange of oxygen and nutrients is required during regeneration. 42 In fact, the perichondrium is a well-vascularized tissue. Despite the observation that invasion of vessels into cartilage is a sign of aging, it is difficult to determine whether vessels can cause chondrocyte aging or whether hypotrophic chondrocytes cause the invasion of vessels. 43 von Bomhard et al. showed that without introducing blood vessels, the center of an embedded ear-shaped scaffold contained no vital cells, but instead exhibited large areas of necrosis. 44 Although we did not observe necrosis in our study, we believed that vessels are crucial for clinical applications of TECs. In the PRP group, we also observed that the capsule wrapping the cartilage was well vascularized. Indeed, PRP releases many proangiogenic cytokines, which could explain why the PRP group showed similar merging of cartilage fragments compared with the Ves and PRP+Ves groups. Furthermore, intrinsic vessels only formed a vascular capsule wrapping the cartilage without invading into the cartilage, as demonstrated by our histological findings.
There were several limitations in this study of ours, the exact process of the regeneration of chondrocytes was not clearly demonstrated. According to the Ki-67 result on week 8, the proliferation of chondrocytes on the outer layer of the embedded cartilage fragment was still robust, indicating that the regeneration process did not finish. Thus the long-term stability of the cartilage contruct was not clear. Furthermore, large animal study need to be done to fully explore the up-limit of contruct volume using TEC technique.
Conclusion
Using the TEC technique, we found that the addition of auricular cartilage fragments mixed with PRP and introduction of axial blood vessels promoted the growth of cartilage tissue, activated chondrocyte proliferation, and stimulated the secretion of cartilage-specific ECM. This approach enabled us to obtain clinically available tissue cartilage within a short time (8 weeks) while maintaining the morphology of the cartilage tissue.
Footnotes
Acknowledgment
We would like to acknowledge the help from Mr. Zhiming Zhang for the help with mechanical test.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Natural Science Foundation of China (81801931), the Scientific Research Foundation of National Health Planning Scientific Research Foundation-Joint Research Projects of Fujian Provincial Health and Education (2019-WJ-09), the Special Supported Funds of Fujian Provincial Finance Department (BPB-WB2019), the Young and Middle-aged Key Scholar Program of Fujian Provincial Health Commission (2019-ZQN-58), the Fujian Provincial Natural Science Foundation Program (2018J01154, 2018J01163).