
Abstract
Repairing mandibular bone defects after radiotherapy of the upper aerodigestive tract is clinically challenging. Although bone tissue engineering has recently generated a number of innovative treatment approaches for osteoradionecrosis (ORN), these modalities must be evaluated preclinically in a relevant, reproducible, animal model. The objective of this study was to evaluate a novel rat model of mandibular irradiation sequelae, with a focus on the adverse effects of radiotherapy on bone structure, intraosseous vascularization, and bone regeneration. Rats were irradiated with a single 80 Gy dose to the jaws. Three weeks after irradiation, mandibular bone defects of different sizes (0, 1, 3, or 5 mm) were produced in each hemimandible. Five weeks after the surgical procedure, the animals were euthanized. Explanted mandibular samples were qualitatively and quantitatively assessed for bone formation, bone structure, and intraosseous vascular volume by using micro-computed tomography, scanning electron microscopy, and histology. Twenty irradiated hemimandibles and 20 nonirradiated hemimandibles were included in the study. The bone and vessel volumes were significantly lower in the irradiated group. The extent of bone remodeling was inversely related to the defect size. In the irradiated group, scanning electron microscopy revealed a large number of polycyclic gaps consistent with periosteocytic lysis (described as being pathognomonic for ORN). This feature was correlated with elevated osteoclastic activity in a histological assessment. In the irradiated areas, the critical-sized defect was 3 mm. Hence, our rat model of mandibular irradiation sequelae showed hypovascularization and osteopenia.
Impact statement
Repairing mandibular bone defects after radiotherapy of the upper aerodigestive tract is clinically challenging. Novel tissue engineering approaches for healing irradiated bone must first be assessed in animal models. The current rat model of mandibular irradiation sequelae is based on tooth extraction after radiotherapy. However, the mucosal sequelae of radiotherapy often prevent the retention of tissue-engineered biomaterials within the bone defect. We used a submandibular approach to create a new rat model of mandibular irradiation sequelae, which enables the stable retention of biomaterials within the bone defect and should thus facilitate the assessment of bone regeneration.
Introduction
With 600,000
The exact pathophysiological mechanism of ORN has not been determined, although several hypotheses have been put forward. These include the “3Hs”—hypoxia, hypovascularization, and hypocellularity 3 —and the “2Is”—infection and ischemia. 4 In histological assessments, radiotherapy is seen to impair bone healing by damaging blood vessels, increasing intracellular damage and osteoclastic activity, and promoting bone marrow fibrosis. 5
Between 5% and 15% of treated patients will display ORN. Localized ORN is treated with drugs, 6 whereas the gold standard for extensive ORN is the microanastomosed free flap. 7 However, the latter procedure induces locoregional complications in the recipient (irradiated) area and sequelae in the donor area.
In recent years, the development of calcium phosphate biomaterials has provided new perspectives for mandibular bone reconstruction. The rat hind limb model previously developed in our laboratory has been used to study sequelae of bone irradiation. 8 However, this model is limited by its use of long bones and thus the difficulty of transposing the results to the jaw. Another model of mandibular irradiation sequelae is based on tooth extraction after radiotherapy. 9 However, the mucosal sequelae induced by radiotherapy often prevent the biomaterial from being stably retained within the bone defect.
Hence, the primary objective of this study was to develop a novel rat model of mandibular irradiation sequelae, to facilitate the assessment of radiotherapy's harmful effects on bone structure, intraosseous vascularization, and bone regeneration. We specifically chose a submandibular approach so that biomaterials could be stably retained in the resulting bone defect. The study's secondary objective was to determine the critical-sized defect in the irradiated jaw bone, that is, the smallest defect that would not heal spontaneously.
Materials and Methods
After 10 days of acclimatization, an 8-week-old inbred male Lewis 1A-haplotype RT1a rat was irradiated with a single 80 Gy dose to the jaws, using an XRAD225Cx irradiator (Precision X-Ray, Inc., North Bandfort, CT). General anesthesia was induced by inhalation of isoflurane (Isoflo®; Abbott France, Rungis, France) at a concentration of 4% for induction and 2% for maintenance. Next, the animal was placed in a feet-first prone position in the irradiator (Fig. 1). The target volume was the mandibular angle, and the field diameter was 10 mm at the isocenter. An irradiation time of 561 s (voltage: 225kVp; intensity: 13 mA) was required for an 80 Gy dose to the bone.

An animal in the feet-first prone position in the irradiator. Color images are available online.
Three weeks after irradiation with a single 80 Gy dose, a 0, 1, 3 or 5 mm diameter circular defect was created on each hemimandible to test tissue engineering strategies for mandibular regeneration after irradiation. Mandibular defects were created under general anesthesia, according to the protocol mentioned earlier. Under aseptic conditions, the masseter muscle was incised and retracted to expose the mandibular ramus. A full-thickness 1, 3, or 5 mm diameter circular defect was created in the mandibular angle on both sides of the body, using a high-speed drill and cooling with physiological saline solution. The muscle and skin lesions were closed with resorbable suture (Vicryl® 4.0; Ethicon, France).
Postoperative analgesia was provided by (1) buprenorphine (0.05 mg/kg, Buprecare®; Animalcare, York, UK) as a subcutaneous injection every 12 h for 4 days, and (2) meloxicam (1 mg/kg, Metacam®; Boehringer, Ingelheim Am Rhein, Germany) as a subcutaneous injection every 24 h for 5 days and then gavaged in sterile water on days 6 and 7. A 5-day course of antibiotic (marbofloxacin 3 mg/kg, Marbocyl®; Vetoquinol, Magny-Vernois, France) was initiated on the day of the surgery.
Experiment
Experimental design
Animals
Twenty 8-week-old inbred male Lewis 1A-haplotype RT1a rats were provided by a certified breeding center (Janvier Labs, Le Genest-Saint-Isle, France). The study protocol was approved by the regional Animal Care and Use Committee (reference: CEEA.201610272139518/AFAPIS 7387) and performed in accordance with European Directive 2010/63/EU. During a 10-day acclimatization period, the animals' health status, behavior, and food intake were examined daily. The rats were weighed twice a week throughout the experiment.
Experimental design
This study is summarized graphically in Figure 2.
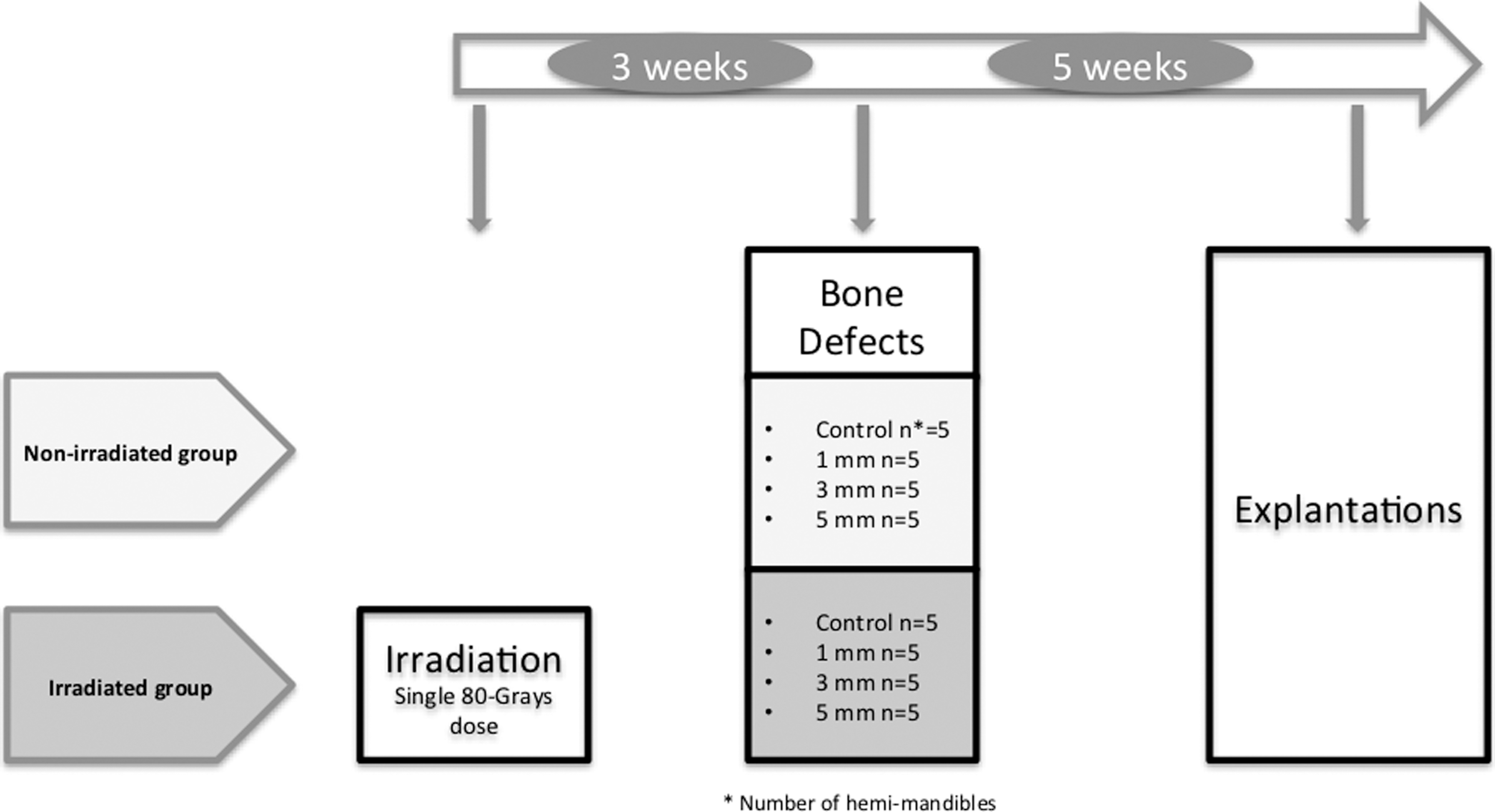
Study design.
On day 0, 10 animals were irradiated with a single 80 Gy dose to the jaw and 10 animals were used as controls. Three weeks after irradiation, mandibular bone defects were created on each hemimandible. For each of the 20 rats, two defects of different sizes (0, 1, 3, or 5 mm) were created in each mandibular angle. In each group of 10 rats (irradiated and nonirradiated), five animals had a 5 mm defect on one side and no defect (i.e., a “0 mm defect” of) on the other, and the other five had a 3 mm defect on one side and a 1 mm defect on the other. Hence, there were 10 defects of each size and 40 defects in total. Five weeks after the surgical procedure, the animals were euthanized.
Two rats from each of the four subgroups received an intravenous injection of contrast agent, so that vascularization could be studied. The mandibles were harvested for qualitative and quantitative analyses.
The irradiation procedure
The dose of radiation described in the Materials and Methods section was delivered at the Institut de Cancérologie de l'Ouest (Centre de Lutte Contre le Cancer René Gauducheau, Saint Herblain, France).
The surgical procedure
Mandibular defects were created 3 weeks after irradiation, as described in the Materials and Methods section. A full-thickness circular defect (diameter: 0, 1, 3, or 5 mm) was created in the bilateral mandibular angle.
Intracardiac injections of contrast agent and euthanasia
Five weeks after surgery, two rats from each of the four subgroups received an injection of contrast agent. Under general anesthesia with isoflurane, the abdominal cavity and the thorax were opened. A catheter was placed at the apex of the left ventricle and connected via a peristaltic pump to a container filled with warmed (40°C) contrast agent (50% barium sulfate (Micropaque®; Guerbet, Roissy Charles de Gaulle, France) in 50% phosphate buffered saline (PBS) with 1.5% gelatin (Sigma-Aldrich, St. Louis, MO)). After resection of the right atrium, ∼200 mL of contrast agent was injected into the bloodstream at a constant rate until all the animal extremities turned white. The animals died (under anesthesia) a few minutes after the start of the injection.
Animals that did not receive contrast agent were euthanized with an intracardiac injection of sodium thiopental (Dolethal®; Vetoquinol). Lastly, the mandibles were harvested and fixed in a solution of paraformaldehyde in 4% PBS for 6 days.
Micro-computed tomography image acquisition and analysis
All samples were imaged with a micro-computed tomography (Micro-CT) system (SkyScan 1272®; Bruker, Kontich, Belgium), with the following acquisition parameters: 0.5 mm aluminum +0.038 mm copper filter; resolution: 18 μm; voltage: 90 kV; amperage: 111 μA; rotation step: 0.8°. The images were processed offline with NRecon® (version 1.6.9.8), DataViewer® (version 1.5.1.2 64-bit) and CTAnalyser® (version 1.14.4.1) software (all from Bruker micro-CT), to create three-dimensional reconstructions and thus study new bone formation and intraosseous vascularization.
The percentage of new bone formation was defined as the bone volume/tissue volume (BV/TV) ratio in the volume of interest (i.e., the defect's initial volume). The vascular volume (in mm3) was quantified in a volume of interest of 5.4 mm in length (composed of 300 slices) starting immediately distal to the third molar.
Histological examinations
After the samples had been fixed, the two hemimandibles were separated for easier inclusion. Nondecalcified, explanted bone specimens were dehydrated with a graded series of ethanol-xylene solutions and then embedded in a methylmethacrylate resin (Technovit 9100; Kulzer, Weirheim, Germany) that hardens at low temperatures. After various pre-infiltration and infiltration procedures, the samples were embedded in the polymerization mixture at −20°C for 1 week. Serial 6 μm coronal sections were then prepared with a microtome for nondecalcified tissues (Polycut MEICA SM2500; Leica Microsystems, Wetzlar, Germany).
The bone sections were stained with Movat pentachrome. The tartrate-resistant acid phosphatase (TRAP) activity was also measured. Lastly, bone sections were observed with a digital slide scanner at a magnification of × 20 (NanoZoomer 2.0 HT; Hamamatsu, Hamamatsu, Japan).
Scanning electron microscopy and image analysis
Each bone sample was sanded, then carbon-coated on a Desk III (Denton Vacuum, Moorestown, NJ), and finally studied in backscattered electron mode in a scanning electron microscope (Leo 1450 VP; Zeiss, Oberkochen, Germany). Bone defects, bone contours, and bone formation were observed in 2D at the same cutting levels as the specimens for histological staining at magnification 50. The area of newly formed bone was determined by using image analysis software (ImageJ; U.S. National Institutes of Health, Bethesda, MD). The percentage of newly formed bone was the ratio between the bone area and the total area corresponding to the initial defect area.
Statistical analysis
Groups of animals were compared with regard to the bone and vascular volumes obtained from micro-CT and scanning electron microscopy (SEM) data, using the Mann-Whitney test. Statistical and graphical analyses were performed with GraphPad software (version 5.00; GraphPad Software, Inc., San Diego, CA). The threshold for statistical significance was set to p < 0.05.
Results
Animals and clinical observations
None of the animals died before the scheduled euthanasia. Both the irradiation procedure and the surgical procedure were well tolerated. A breakpoint in the weight curve was detected after irradiation and lasted for 1 week in the irradiated group. A similar breakpoint was observed after surgery in all groups (data not shown).
Five or 6 weeks after irradiation, the irradiated animals showed an area of depilation on the cheek.
Micro-computed tomography study
New bone formation
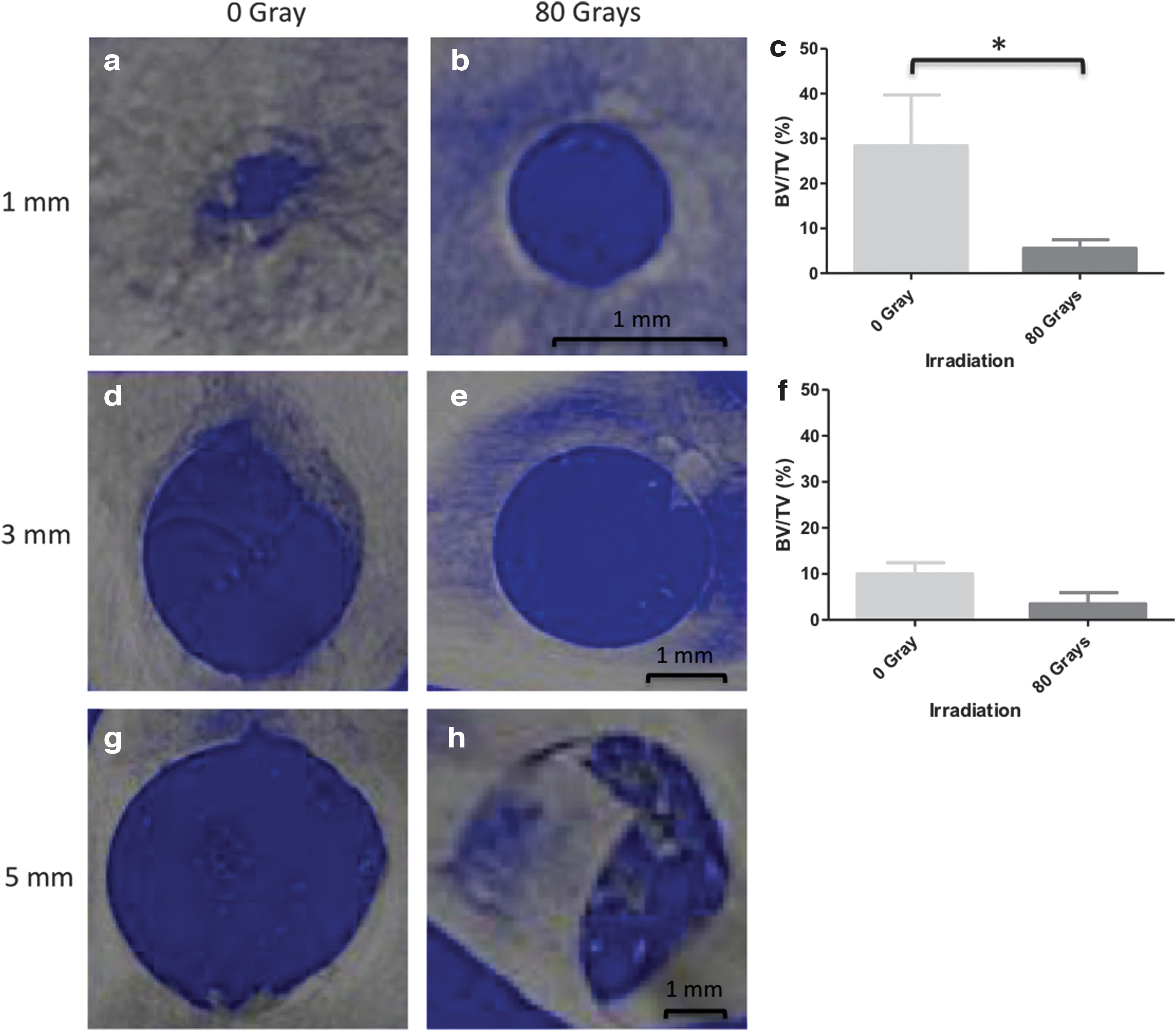
The micro-CT assessment evidenced centripetal bone regrowth in the 1 and 3 mm nonirradiated defects (Fig. 3a, d), whereas no bone regrowth was observed in the 5 mm defects (Fig. 3g). No mandible fractures were observed for 1 mm defects, and only one fracture was observed for 3 mm defects. In contrast, two fractures (40%) were observed for mandibles with a 5 mm defect. In the irradiated group, little bone formation was observed within the bone defects (Fig. 3b, e); jaw fractures were observed in all five animals (100%) with a 5 mm defect (Fig. 3h) and in three of the animals (60%) with a 3 mm defect.
Micro-CT 3D reconstructions of mandible defects in irradiated animals
We were able to analyze bony formation in 10 hemimandibles with a 1 mm defect, six with a 3 mm defect, and three with a 5 mm defect. The other samples were fractured, which compromised the observation of bone formation. The extent of new bone formation (expressed as BV/TV) tended to decrease as the size of the defect increased. The bone formation was significantly greater in nonirradiated 1 mm bone defects than in irradiated bone defects of the same size (p = 0.0317) (Fig. 3c). The difference was not significant for 3 mm defects (Fig. 3f).
Intraosseous vascularization and bone volume
Before euthanasia, four irradiated animals and four nonirradiated animals were injected with contrast agent. Macroscopically, major destruction of intraosseous vessels was not observed. To limit variations in BV, only hemimandibles with a 1 mm defect or without a defect were included in the qualitative micro-CT analysis. One rat from the nonirradiated group was excluded from this analysis because of poor injection quality. Hence, three mandibles from the nonirradiated group and four from the irradiated group were assessed. Bone and vessel volumes were significantly lower in the irradiated group than in the nonirradiated group (p = 0.0286) (Fig. 4).

Quantification of bone and vessel volumes in micro-CT reconstructions of the jaw.
SEM analysis
Qualitative SEM analysis
In the irradiated group, the SEM study revealed the presence of large, multilobed gaps (Fig. 5a) that were suggestive of Dambrain periosteocytic lysis. 4 There was no new bone formation in the defects, regardless of the size. The defects' edges were flat, with no convexity toward the center of the defect (Fig. 5c). In contrast, the bone microarchitecture was maintained in the nonirradiated samples (Fig. 5b). Likewise, the cortical bone in the nonirradiated samples was smooth, and all the defects contained newly formed bone with a medullary aspect (Fig. 5d, in yellow).

Quantitative SEM analysis
In the 1 mm defect group, two hemimandibles were excluded from the quantitative analysis because the section did not pass through the defect. Therefore, eight samples were included. In the 3 mm defect group, three irradiated mandibles were fractured and one section did not pass through the defect. In the nonirradiated group, one explant could not be used and so five were included in the analysis. All the 5 mm defects in the irradiated group were fractured, preventing an analysis of this size of defect. For 1 mm defects, the bone ingrowth ratio was significantly higher in nonirradiated bone than in irradiated bone (p = 0.0286) (Fig. 5e). The same type of difference was found for 3 mm bone defects but was not statistically significant.
Histological examinations
In the nonirradiated samples, newly formed bone (surrounded by a large number of medullar cells) was observed on the edges of the defect (Fig. 6a, b). The bone marrow showed high cellularity and was highly vascularized (Fig. 6c). The edges of the defects were smooth, and the TRAP activity was low (Fig. 6h). In the irradiated group, no bone regrowth was observed (Fig. 6d, e). The defects were filled with acellular, possibly fibrotic tissue. The bone marrow showed low cellularity. Multinucleated cells (possibly osteoclasts) were observed on the edges of the defects (Fig. 6f). Moreover, the level of TRAP activity was higher in the irradiated bone than in the nonirradiated bone. The level was particularly high in the multilobed gaps observed in the SEM study (Fig. 6g).

Histological assessments with Movat pentachrome staining in irradiated animals
Discussion
The histological and biomechanical effects of bone irradiation appear at doses above 60 Gy. As the last stage in bone tissue degradation, ORN is characterized by the occurrence of gaps, fibrosis, and necrotic areas. In our present laboratory, the sequelae of irradiation have typically been studied in the rat posterior limb model. However, this model is limited by the use of long bones (whose embryological origin differs from that of the jaw) and by the presence of a mixed ossification process. 10
Although several research groups11–13 have studied animal models of mandibular ORN induced by low-energy X-rays, the irradiation was usually diffuse; in this study, however, we used targeted irradiation. Other researchers have used the high-energy X-rays techniques 9 commonly used to treat patients in the clinic and that are believed to harm the bone less than low-energy X-rays do at an equivalent dose level. Likewise, a number of models have been based on the fractioned radiotherapy techniques used in the clinic,11–13 although implementation with animals is complicated by the need for general anesthesia and repeated transport—both of which can induce stress. Therefore, the results will vary according to the irradiation dose and protocol.
In an earlier model, 14 rats received a single 80 Gy dose to their hind limbs, and pathognomonic ORN lesions were observed. However, specific lesions (such as ORN) were not observed at a lower (50 Gy) dose—even though fractures were just as frequent. Hence, we chose to keep a single 80 Gy dose in this study.
The critical-sized circular defect in the mandibular angle is often used in experiments that do not involve irradiation.15–20 Another model involves segmental mandibulotomy stabilized by an internal fixator. A critical-sized defect will not heal spontaneously21,22 and so mandibular regeneration requires a therapeutic intervention. According to the literature, the critical size of the bone defect in a healthy jaw is around 4 or 5 mm. This model offers an ideal platform for testing the osteoconductive properties of bone substitutes 23 and membranes in the presence17–19 or absence of growth factors. 24
Lastly, it is known that trauma (especially tooth extraction) in an irradiated area can induce ORN. 25 Therefore, some models are based on molar extraction a few days or a few weeks after irradiation.9,26,27 However, the mucosal sequelae of irradiation prevent the defect from being filled with biomaterial in a lasting manner.
This study is the first to have assessed a rat model of mandibular irradiation sequelae with a circular submandibular defect in an irradiated area. This model avoids mucosal lesions and thus enables the evaluation of bone remodeling with tissue engineering techniques. We sought to model the adverse events associated with bone irradiation and so we observed the clinical and histological characteristics of ORN. Seven days after irradiation, we observed a break in the weight curve in the irradiated group—suggesting oral mucositis. Five weeks after irradiation, the irradiated area had shed its hairs.
A micro-CT analysis showed a loss of BV after 80 Gy irradiation and thus confirmed the direct impact on bone microarchitecture. Further, a large number of fractures were observed during the explantation and the micro-CT acquisitions. Fractures of the inferior mandibular border in nonirradiated areas have already been reported but were infrequent 17 ; this suggests that a critical defect in an irradiated area is smaller than a critical defect in a nonirradiated area. Likewise, Tchanque-Fossuo et al. 28 described a dose–response effect for the deterioration of the murine mandible's biomechanical properties after irradiation.
In this study, we found that bone regrowth decreased as the size of the defect increased. However, there were no significant differences between the defect conditions. In nonirradiated areas, almost no bone formed in 5 mm defects—confirming the critical-sized defect reported in the literature. Five weeks after surgery, partial bone regrowth was observed in nonirradiated 1 and 3 mm bone defects. Although this timeframe was short to observe complete healing, it was enough to observe bone regeneration. Our histological data showed increased osteoclastic activity in the irradiated area—suggesting that the various types of bone cell differ in their radiosensitivity. Osteoblasts appear to be the most radiosensitive, followed by osteocytes and then osteoclasts. 29
We showed a decreased intraosseous vascular network in the irradiated animals, in accordance with previous studies also using micro-CT8,30 or Doppler. 31 In vitro, Dudziak et al. showed that vascular endothelial growth factor expression, essential for neoangiogenesis, was decreased beyond an 8-Gy irradiation. 32 The pathologic effects of radiation are mediated in part through endothelial lesions of capillaries and distal vessels. It results in progressive obliterative endarteritis, leading to decreased blood flow and fibrosis. Mandibular bone is particularly prone to radiation damage due to its tenuous vascular supply from the inferior alveolar artery, limited collateral circulation, and compact bony structure.33,34 This set of anatomical features could explain the pathological fractures recorded in the study.
According to our micro-CT and SEM studies, a 1 mm defect appeared to be too small for accurate quantification of bone regrowth: It closed quickly after being filled with biomaterials. Therefore, a 3 mm defect appears to be a good compromise for a critical-sized defect: Bone regrowth was noted in a healthy jaw but not at all in an irradiated jaw.
This study had some limitations. First, the number of animals in each group was low; however, this was in accordance with current guidelines on reducing the use of laboratory animals. Second, we created a circular defect that does not resemble the naturally occurring bone loss induced by irradiation. Third, our follow-up period was limited to 5 weeks; clinically, the sequelae of bone irradiation develop over several months. However, rodent bone regenerates more quickly than human bone. Despite these differences, our model reproduced alterations in bone healing. From a cost perspective, a small animal model is an advantage. In the future, we, nevertheless, intend to develop a large animal model.
Our study also had several strengths. For example, we used several imaging techniques to assess bone remodeling. Scanning electron microscopy is the gold standard analytical technique in our lab.14,35,36 However, SEM measurements are limited to a single bone section, whereas new bone grows in all three dimensions. Micro-CT has a lower spatial resolution than SEM but seems to be of value in the assessment of bone healing in three dimensions.
Conclusion
This study highlighted the impact of radiation on the intraosseous vasculature and bone microarchitecture of the rat mandible. With a view to studying bone remodeling, the critical-sized defect in the irradiated jaw appears to be 3 mm. Despite practical and time constraints, we demonstrated that our model effectively reproduces the sequelae of irradiation of the jaw and may be a useful research tool. Further studies of larger groups of rats will be necessary to obtain consistent quantitative data in this new model and to test tissue-engineering strategies for mandibular regeneration after irradiation.
Footnotes
Acknowledgment
The authors thank Sophie Chiavassa from the Institut de Cancérologie de l'Ouest (Saint Herblain, France) for her assistance with the irradiation procedures.
Ethical Approval
All applicable international, national, and/or institutional guidelines for the care and use of animals were followed. The protocols were approved by the Pays-de-Loire Animal Care and Use Committee (reference: CEEA.201610272139518/AFAPIS 7387), in accordance with the European directive 2010/63/EU.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by grants from the Côtes d'Armor and Loire-Atlantique branches of the La Ligue Contre Le Cancer foundation, from the Les Gueules Cassées foundation, and from IXBONE (ANR-18-CE18-0014).