
Abstract
Three-dimensional (3D) cardiac tissue reconstruction using tissue engineering technology is a rapidly growing area of regenerative medicine and drug screening development. However, there remains an urgent need for the development of a method capable of accurately measuring the contractile force of physiologically relevant 3D myocardial tissues to facilitate the prediction of human heart tissue drug sensitivity. To this end, our laboratory has developed a novel drug screening model that measures the contractile force of cardiac cell sheets prepared using temperature-responsive culture dishes. To circumvent the difficulties that commonly arise during the stacking of cardiomyocyte sheets, we established a stacking method using centrifugal force, making it possible to measure 3D myocardial tissue. Human induced pluripotent stem cell-derived cardiomyocytes were seeded in a temperature-responsive culture dish and processed into a sheet. The cardiac cell sheets were multilayered to construct 3D cardiac tissue. Measurement of the contractile force and cross-sectional area of the multilayered 3D cardiac tissue were then obtained and used to determine the relationship between the cross-sectional area of the cardiac tissue and its contractile force. The contractile force of the 1-, 3-, and 5-layer tissues increased linearly in proportion to the cross-sectional area. A result of 6.4 mN/mm2, accounting for one-seventh of the contractile force found in adult tissue, was obtained. However, with 7-layer tissues, there was a sudden drop in the contractile force, possibly because of limited oxygen and nutrient supply. In conclusion, we established a method wherein the thickness of the cell sheets was controlled through layering, thus enabling accurate evaluation of the cardiac contractile function. This method may enable comparisons with living heart tissue while providing information applicable to regenerative medicine and drug screening models.
Impact statement
Cell sheet technology was used to construct myocardial tissues to visually confirm pulsation. By stacking these cell sheets, a three-dimensional (3D) myocardial tissue was created and a method for measuring the contractile force was constructed. Our results revealed that the contraction force of 1- to 5-layer sheets increased linearly in tandem with the cross-sectional area, giving rise to the synchronized beats in the 3D myocardial tissue. This method allows for a more accurate evaluation of myocardial contractile force.
Introduction
I
In this study, we developed and tested a new method for evaluating the function of the contractile force of 3D cardiac tissue. This was accomplished by varying the thickness of the tissue by layering cardiac cell sheets. The physical properties of laminated cell sheet heart tissue may contribute to developing an optimal treatment strategy for future studies involving in vivo transplantation therapy.
Materials and Methods
Multilayered cardiac sheets were attached to fibrin gel as a culture base (Fig. 1a, b), and the fibrin gel base was attached to a force sensor (Fig. 1c). The contractile force measuring device consisted of a load cell (LVS-10GA; Kyowa Electronic Instruments, Tokyo, Japan) and a cultivation tank. A clip was fixed to the bottom of the cultivation tank capable of holding a fibrin gel-based grip. The fibrin gel base was attached to the load cell while holding the grip on the underside of the fibrin gel sheet with a clip. M199 Hanks' balanced salts (12350039; Thermo Fisher Scientific, Waltham, MA), 10% fetal bovine serum (FBS), 500 KIU/mL aprotinin, and 1% penicillin–streptomycin was poured into the cultivation tank and cultured. The load cell was connected to a strain amplifier (DPM-712B; Kyowa Electronic Instruments), and the contractile force was recorded with a personal computer using an A/D converter (Power Lab 8/30; AD Instruments, Bella Vista, Australia). At the time of contractile force measurement, an electric stimulator (UPS-801; Unique Medical, Tokyo, Japan) was used, and the measurement was performed at 1 Hz. At the time of the experiment in which the contraction force was continuously measured for 1 week, the construct remained in the culture tank. For other contraction force measurement experiments and morphological observation experiments, the constructs were placed in a φ60 mm culture dish and cultured for 1 week in an incubator in an environment of 37°C and 5% CO2.

The measuring device and fibrin gel base for measuring contractile force.
Experiment
Experimental design
Human iPSC culture
This study used iPS cardiomyocytes, as reported in previous studies.16,17 As human iPSCs (line 201B7; Riken, Tsukuba, Japan) transfer puromycin resistance gene through the α-myosin heavy chain, 17 the cells were purified with puromycin following their differentiation into cardiomyocytes.
Cardiomyocyte differentiation from human iPSCs in a suspension culture system
Human cardiomyocytes were obtained by differentiation from iPSCs using a method similar to a previously reported suspension culture system. On day 15 of the suspension culture, differentiated iPSCs containing cardiomyocytes were collected from the bioreactor. The detailed protocol of the culture medium is outlined in a previous culture method. 18
Cardiomyocyte purification
Differentiated iPSCs containing cardiomyocytes were collected from the bioreactor suspension culture and singled with Hanks' balanced salt solution (17460-15; Nacalai Tesque, Kyoto, Japan) containing 0.05% trypsin/EDTA (32777-44; Nacalai Tesque). The cells were separated and seeded at 1.7 × 105 cells/cm2 in a φ100 mm culture dish with Dulbecco's modified Eagle's medium (DMEM) (D6429; Sigma-Aldrich, St. Louis, MO), 10% FBS (10437028; Thermo Fisher Scientific), and 1% penicillin–streptomycin (15140122; Thermo Fisher Scientific). On the fourth day after seeding, 1.5 μg/mL puromycin (A11138-03; Thermo Fisher Scientific) was added, and cells were cultured for 24 h to eliminate noncardiomyocytes. The next day, cells were passaged with 0.05% trypsin/EDTA and seeded in culture dishes at 1.0–1.7 × 105 cells/cm2. This process was then repeated. Purified cardiomyocytes were treated twice with puromycin and passed through a cell strainer with a 70 μm mesh (352350; Corning, NY) to remove cell aggregates. From this purification process, cardiomyocytes with a purity of 97% or more can be obtained. 15 After purification, a cell sheet was prepared by seeding on an UpCell dish. The detailed method for evaluating the purity of cardiomyocytes was described previously. 18
Creation of a fibrin gel base
As the cell sheet alone is very fragile, it is difficult to measure the contractile force while holding the cell sheet. Therefore, a cardiac sheet was attached to fibrin gel as a culture base (Fig. 1a, b), and the fibrin gel base was attached to a force sensor (Fig. 1c). To produce the base, a resin grip was installed in a mold constructed with a silicone sheet, and fibrin solution was poured into the mold. The fibrin solution contained fibrinogen (F8630; Sigma-Aldrich), thrombin (T4648; Sigma-Aldrich), CaCl2 (038-24985; Fujifilm Wako Pure Chemical, Osaka, Japan), and human blood coagulation factor XIII (Fibrogammin P IVInjection; CSL Behring, Tokyo, Japan). These were dissolved in physiological saline with 0.025% Polyoxyethylene(20) Sorbitan Monooleate (Fujifilm Wako Pure Chemical) and mixed to final concentrations of 9 mg/mL, 0.5 units/mL, 2 mM, and 20 units/mL. The mixture was then allowed to stand at 25°C ± 1°C for 30 min.
After curing, the fibrin gel base with grips was removed from the silicone mold and placed in a culture dish containing culture medium (Fig. 1b and Supplementary Fig. S1). The fibrin gel base was immersed in DMEM containing 50 μm/mL fibronectin (354008; Corning) at 37°C for 2 h or more to enhance adhesion to the cardiac sheet. A 12 mm square-ring silicone mold was attached to a φ35 mm UpCell dish (CS3017; CellSeed, Tokyo, Japan) to control cardiac cell adhesion sites (Supplementary Fig. S2a). Purified iPSC-derived cardiomyocytes were seeded at 3 × 105 cells/cm2 on the culture surface, which was coated with FBS overnight.
Incubation was carried out in culture medium containing DMEM, 10% FBS, 1% penicillin–streptomycin, and 500 KIU/mL aprotinin (014-21021; Fujifilm Wako Pure Chemical) to prevent fibrin from melting. The medium was changed every other day from the day after incubation, and 1 week later, the cardiac cell sheet was transferred onto the fibrin gel base. The detailed cell sheet transfer methods were outlined previously. 15
Layering cardiac cell sheets
To layer cell sheets, cardiomyocyte pulsation was stopped during the procedure. Thirty millimolar KCl (163-03545; Fujifilm Wako Pure Chemical) was added to a normal culture solution of DMEM, and a further 50 mg/mL fibronectin (354008; Corning) was added to promote adhesion. Supplementary Figure S2a shows an illustration of the layering method involving centrifugation and fibrin gel. First, the prepared fibrin gel base was immersed in a transcription medium containing KCl and fibronectin and incubated for 2 h or more. The medium in the UpCell dish containing the cultured cardiomyocytes was removed, and the square-ring silicone mold was also removed from the dish (Supplementary Fig. S2b). The fibrin gel base was carefully placed on the cardiomyocytes in the UpCell dish (Supplementary Fig. S2c).
Next, to firmly attach the fibrin gel base to the cardiomyocytes, the construct was centrifuged at 130 g for 15 min (Rorze Lifescience, Hiroshima, Japan) (Supplementary Fig. S2d, e). 19 The construct was incubated at 20°C for 1 h to transfer the cardiomyocytes from the culture dish to the fibrin gel base. To facilitate adhesion of the cardiac cell sheets from the second layer, a small amount of fibrin gel was applied to strengthen adhesion. Fibrinogen (1.44 μL of 80 mg/mL) was added to the cardiac cell sheet on the fibrin gel base, and 1.44 μL of 4 units/mL thrombin was added to the cardiac cell sheet on the UpCell dish for layering. The fibrin gel base was placed on the cardiac cell sheet for layering, and centrifugation was performed again at 130 g for 15 min. The fibrin gel was then carefully peeled from the UpCell dish. This procedure was repeated to create 3-, 5-, and 7-layer cardiac tissues.
After the multilayered cardiac cell sheet was prepared, 10 mL of culture medium was placed in a φ60 mm culture dish. The cell sheet-side surface was left facing upward to ensure that only the fibrin gel was immersed in the culture medium. The construct was then incubated at 37°C overnight. The prepared construct was then fixed to a shrinking-prevention tool, followed by immersion in a medium containing 500 KIU/mL aprotinin in M199 (12340; Thermo Fisher Scientific). The construct was then incubated at 37°C for 7 days, after which the contractile force was measured.
Histological analysis
After measuring the contractile force, the fibrin gel base and layered cardiac cell sheets were fixed with 4% paraformaldehyde solution (33114; Muto Pure Chemicals, Osaka, Japan). The construct was periodically processed into paraffin-embedded sections at a thickness of 5 μm. Hematoxylin and eosin (H&E) staining was then carried out. For the first immunoreactive stain, cell sheet specimens were immunolabeled with anti-troponin T and cardiac isoform antibody (13-11; Lab Vision, Waltham, MA) at a dilution of 1:100 to detect cardiomyocytes.
For secondary antibody staining, the specimens were immunolabeled with the Alexa Fluor 568 F(ab′)2 fragment of goat anti-mouse IgG (H+L) (A11019; Thermo Fisher Scientific) at a dilution of 1:200 for 2 h at 25°C ± 1°C. Nuclei were stained with a 500 × dilution of Hoechst 33342 (H1399; Thermo Fisher Scientific). TUNEL staining, which labels the fragmented DNA generated by cell death, was used to morphologically analyze cell death. After labeling fragmented DNA, DAB color development and hematoxylin counterstaining were performed to distinguish between live and dead cells. These were observed using an optical microscope. DAB color development by TUNEL staining was outsourced to Kyodo Pathology using an apoptosis detection kit (MK500; Takara Bio, Shiga, Japan).
Live/dead staining was also performed as an additional form of analyzing cell death. After measuring the contractile force, the cardiac cell sheet was directly stained before paraformaldehyde fixation. The sample was placed on a 60 cm dish in 10 mL of phosphate-buffered saline (PBS), to which 20 μL of EthD and 5 μL of Calcein AM (L3224; Thermo Fisher Scientific) were added. This was allowed to stand for 30 min in a light-shielded environment at 25°C ± 1°C. After washing with PBS, the cardiac sheet was placed toward the bottom of the dish and observed with a confocal microscope.
Image analysis
To analyze the cross-sectional area of the layered cell sheets, the area was calculated from the H&E-stained image. The number of pixels in the extracted cardiac cell sheet portion of the H&E-stained image was calculated using image processing software (ImageJ; National Institutes of Health, Bethesda, MD). Using the calculated number of pixels, the ratio R% of the cardiac cell sheet portion in one visual field (1310720 pixels) was calculated. Using the size of one visual field of a 20 × optical microscope image (410 × 330 μm) and the calculated ratio R%, the partial cross-sectional area (μm2) of the cardiac cell sheet was calculated according to Equation (1):
where A represents the partial cross-sectional area of cardiac cell sheet (μm2) and R denotes the cardiac cell sheet area ratio (%).
To analyze the cross-sectional area of the entire tissue, it was assumed that the cross-sectional area of one field of the microscope image (horizontal length 410 μm) was continuous over the entire specimen (horizontal length 12 mm), and the total cross-sectional area was calculated.
To investigate the rate of cell death in the tissue, we analyzed the image by TUNEL staining using optical microscopy at 20 × magnification, and three specimens were photographed at the end, in each quadrant, and at the center. Using image processing software (VW-9000 Album; Keyence, Osaka, Japan), TUNEL-positive cells and viable cells were counted in the edges, quadrants, and center of the tissue.
Statistical analysis
Statistical analyses were performed with one-way analysis of variance followed by Tukey's post hoc test for multiple group comparisons. Data are presented as mean ± standard deviation. Statistical analyses were carried out with StatPlus:mac software.
Experimental results
Contractile force of human iPSC-derived cardiac cell sheets
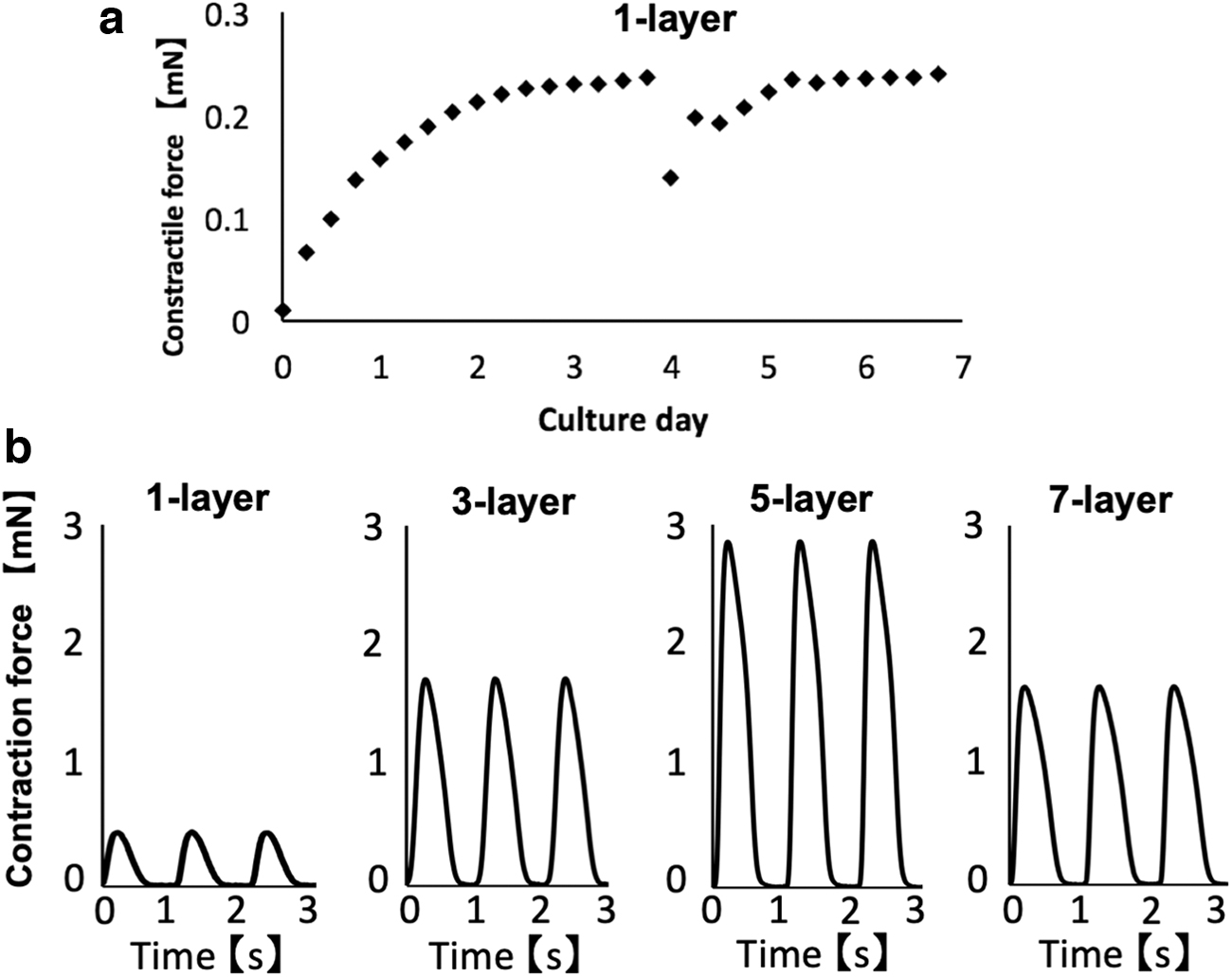
A fibrin gel base was created by the previously described method, and the contractile force was measured using our original system (Fig. 1). First, after placing the monolayer cardiac cell sheet, the fibrin gel base was immediately placed on the contractile force measuring device. The continuous contractile force was measured every 6 h until day 7. Although the contractile force after installation was very weak, it gradually increased with the duration of culture. The contractile force was stable on day 3 of the culture with a period of sufficient contractile force stabilization observed on day 7, except for when the culture solution was exchanged (Fig. 2a). The contractile force decreased when the culture solution was exchanged on day 4; however, it returned to the original levels 1 day later. The remaining experimental results, such as histological observations, were obtained on day 7 after layering the cell sheets, as a stable period sufficient for measuring contractile force was observed at this point.
Measurement of contractile force of the layered human cardiac cell sheets.
Next, 1, 3, 5, and 7 layers of cardiac cell sheets were layered on the fibrin gel base, and then incubated in a normal culture dish for 7 days. After culturing, the pulsation was adjusted to 1 Hz using a pacing device, and the contractile force was measured and analyzed. Average values of 0.4, 1.6, 2.8, and 1.6 mN were detected from the 1-, 3-, 5-, and 7-layer cell sheets, respectively. The waveforms of the contractile force of the cell sheets with differing numbers of layers are given in Figure 2b. The contractile force waveform was obtained with good reproducibility. The waveform increased sharply during contraction, became slightly slower immediately after relaxation, and then rapidly relaxed. The waveform then became asymmetrical.
Relationship between cardiac cell sheet thickness and contractile force
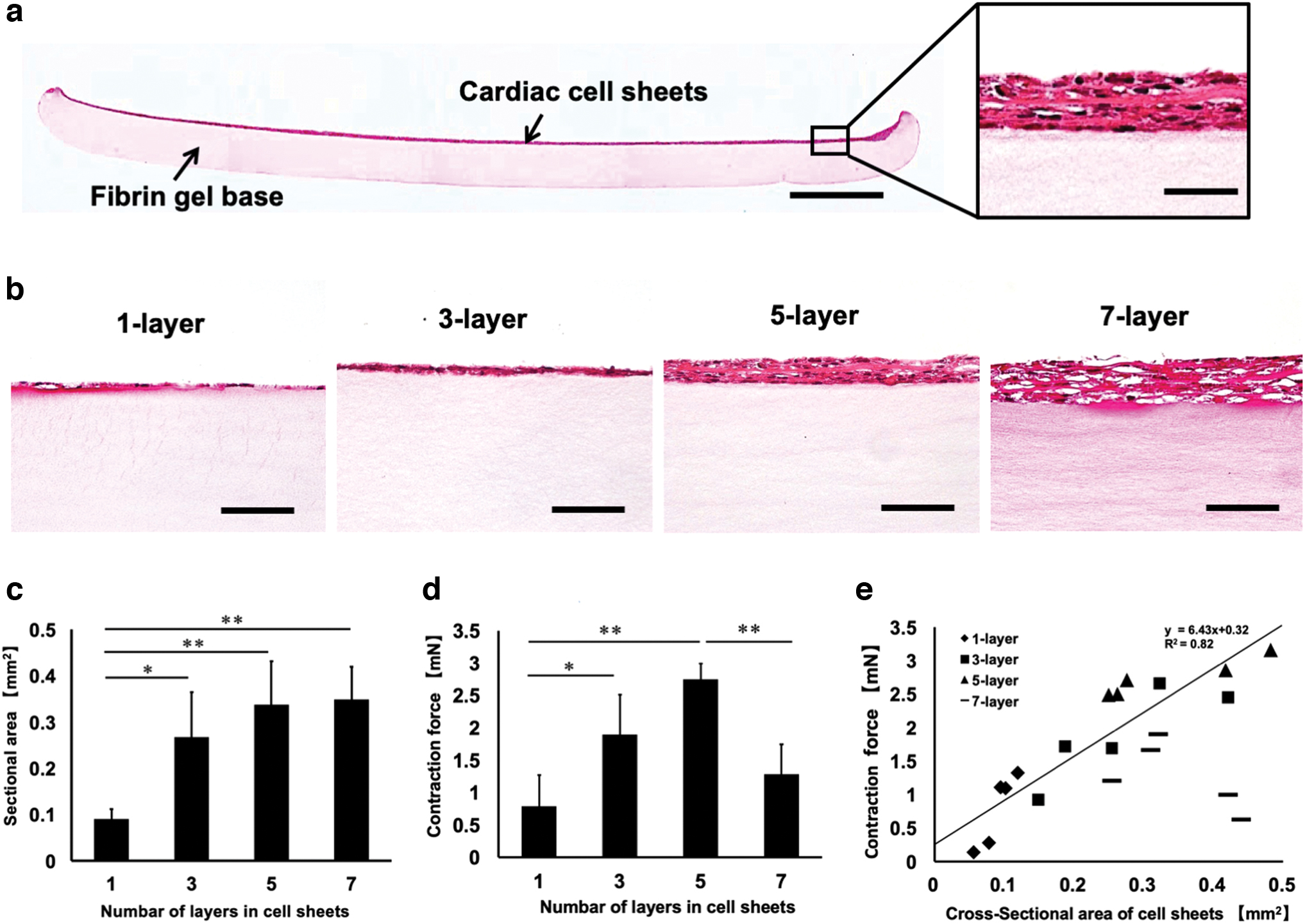
As the cardiac cell sheet has a very high cell density allowing for effective cell–cell communication, contractile force can be visually observed (Supplementary Movie S1). Using this cardiac cell sheet, we elucidated the relationship between the cross-sectional area and contractile force. Human cardiac cell sheets were constructed with 1, 3, 5, and 7 layers. After measuring the contractile force, tissue sections were prepared. H&E staining was performed to visualize the tissue thickness. The cardiac cell sheet was dyed dark red by the muscle fiber filaments, and this section was extracted with image software to calculate the cross-sectional area.
Figure 3a shows H&E staining of the entire tissue section of the fibrin gel base and 5-layer cardiac sheet. These results demonstrate that the thickness of the cell sheet increased with the number of layers. However, the 7-layer structure had many gaps, and the shape of the nucleus was distorted. The thickness of the cross-sectional area increased similarly for the 1- to 5-layer cell sheets; meanwhile for the 7-layer sheet, the same thickness was observed as that of the 5-layer sheet. Furthermore, the layered tissue was partially necrotized and could not be maintained in culture. The H&E staining images are given in Figure 3b, and a graph of the calculated cross-sectional area of each layer is given in Figure 3c. The average contractile force results obtained for the different number of layers in each of the five samples are graphically presented in Figure 3d. Similar to the cross-sectional area, the contractile force also increased in the 1- to 5-layer cell sheets as the number of layers increased. However, the contractile force of the 7-layer sheet was predominantly reduced compared with that of the 5-layer sheet. From these data, we constructed a graph showing the relationship between tissue thickness and contractile force (Fig. 3d). The contractile force of the 3D cardiac tissues with 1 to 5 layers showed a linear relationship, which was in proportion to the cross-sectional area. This relationship yielded a value of 6.4 mN/mm2.
Relationship between the contractile force and the cross-sectional area of the human cardiac cell sheets.
Limitation of multilayered cardiac cell sheets
Since the contractile force of the 7-layer cardiac cell sheet was found to be limited, various morphological observations were made to determine if the decrease in contractile force was caused by cell death owing to thickness increase. First, to confirm the presence of cardiac cells, cardiac troponin T and nuclear staining were performed, which demonstrated that cardiomyocytes were not significantly lost in the 7-layer myocardial tissue (Fig. 4a). However, delamination was observed in many places between the layers. Next, DNA fragmentation caused by cell death was detected using TUNEL staining, and DAB staining was performed to clearly distinguish between cells with and without DNA fragmentation (Fig. 4b). Approximately 12% of the total cell number, in a single field (live: 29.1 cells, dead: 1.7 cells), was positive for apoptosis in the monolayer cell sheet (Fig. 4c). For cell sheets with 3, 5 and 7 layers, 28% (live: 12.6 cells, dead: 11.3 cells), 20% (live: 38.6 cells, dead: 9.7 cells), and 31% (live: 43.2 cells, dead: 19.9) cell death was observed, respectively (Fig. 4c–e). The number of living cells in the 5- and 7-layer sheets was similar to that in the cross-sectional area given in Figure 3 (Fig. 4c). In comparison, many dead cells were observed in the 7-layer cell sheet (Fig. 4d); meanwhile the total number of cells increased with the number of layers (Fig. 4e). Finally, live/dead staining was performed to confirm cell death in the 1- and 7-layer sheets. Living cells (green) were densely organized in the monolayer. However, there were few live cells (green) in the 7-layer sheet, and many dead cells were observed (Supplementary Fig. S3). These results are highly associated with decreased contractile force.

Limitations of the numbers of human cardiac cell sheet layers.
Discussion
Herein, we successfully measured the contractile force of 3D myocardial tissue by layering cardiac cell sheets derived from human iPSC.
A typical contraction–relaxation waveform is confirmed as the myocardial electric potential. Herein, waveforms were observed in the first phase corresponding to increased contraction force because of the increase in intracellular sodium ion concentration, the second phase where the contraction force gradually decreases owing to extracellular calcium ion release, and the third phase where potassium ions are released (Fig. 2b).
Based on the design of this novel measurement system, it is important to address the potential inhibition of contractile force exerted by the fibrin gel. The unit of fibrin gel base and cell sheet was fixed with a clip on one side and with a load cell on the other. As for the sensitivity of the load cell used, the deflection stroke to detect 1 mN was 1.48 μm. From the Supplementary Movie S1 and a previous report, fibrin gel was observed to shrink by more than 1 mm under a load of 1 mN. 15 Therefore, when fibrin gel is deflected by 1.48 μm, the resistance is ∼1.48 × 10−3 mN, thereby causing insignificant interference of myocardial contraction.
When creating 3D myocardial tissue by layering cardiac cell sheets, a linear relationship was observed between the cross-sectional area and the contractile force of the multilayer cardiac cell sheets (up to five layers). This was accurately determined using thickness control technology to construct the cell sheet. The contractile force per cross-sectional area of the cardiac cell sheet was 6.4 mN/mm2, which is approximately one-seventh of the contractile force of adult left ventricular cardiomyocytes (44 mN/mm2). 20 The difference in contractile force from this adult myocardial tissue is generally observed in the cell orientation, maturity, and connection. In fact, transplantation of these human iPSC-derived cardiomyocytes into a living body reportedly causes maturation and an increase in myocardial contraction. 21 Moreover, the contraction force of myocardial tissue can be improved by aligning the orientation. 22 By these methods, it is possible to construct a 3D tissue that more closely resembles physiological tissue, and expand its role as a drug screening model.
Cell death, including apoptosis and necrosis, was confirmed in the 7-layer cell sheet during the layering of cell sheets. The rate of diffusion of the culture solution from the surface of the constructed tissue could not meet the demand for oxygen and nutrient supply or for waste product removal, resulting in cell death. Previous studies have reported that for cardiac tissue survival, the upper thickness limit is ∼80 μm 9 in vivo, and ∼20 μm in vitro.23,24 Although the 5-layer (t = 28.1) and 7-layer (t = 29.1) cell sheets were similar in thickness to the previously reported in vitro limit, the contraction force of the 7-layer cardiac cell sheet was significantly lower than the tension of the 3-layer or 5-layer cardiac cell sheet. This was considered as cell death in the 7-layer cell sheet, as a large number of spaces were observed between cell sheets; thus, coordinated contraction/relaxation could not be performed.
In future, a novel cultivation system with a microluminal structure similar to capillaries, through which culture fluid can flow, is required. This will allow for a thicker 3D myocardial tissue to be constructed. We have also developed a new system for constructing cardiac cell sheets with a tubular shape, allowing for the observation of internal pressure function.25,26 At present, we are planning to develop a bioreactor that combines a blood vessel construction system and a contraction force measurement system.
Conclusions
In our study, the contractile force of the multilayered tissues increased linearly in proportion to the cross-sectional area. We also demonstrated that the cell sheet technology and contractile force measurement system can accurately measure the contractile force per cross-sectional area. This measurement method may provide a new index for developing more effective applications for cardiac tissue engineering in the future.
Footnotes
Authors' Contributions
K.S. designed and performed the experiments, analyzed the data, and wrote the article. H.T. designed and performed the experiments and analyzed the data. Y.T. performed the experiments and analyzed the data. D.S. designed and performed the experiments. K.M. designed and performed the experiments and supervised the project. K.I. designed the experiments and supervised the project. T.S. designed the experiments, analyzed the data, wrote the article, and supervised the project. M.U. designed the experiments and supervised the project.
Disclosure Statement
T.S. was a member of the scientific advisory board and a shareholder of CellSeed, Inc. (Tokyo, Japan). Tokyo Women's Medical University receives research funds from CellSeed, Inc.
T.S. and K.M. are inventors of the bioreactor systems for iPSC proliferation and cardiomyocyte differentiation. Tokyo Women's Medical University, T.S., and K.M. received a license fee from ABLE Corporation, Tokyo, Japan.
T.S., D.S., and K.M. are inventors of the contractile force measurement system of Nihon Kohden Corporation, Tokyo, Japan. Tokyo Women's Medical University receives research funds from Nihon Kohden Corporation.
Funding Information
This research was supported by Japan Agency for Medical Research and Development under grant number JP18he0702249.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.