
Abstract
Osteoarthritis (OA) is a painful and disabling disease that affects millions of people worldwide. Symptom-alleviating treatments exist, although none with long-term efficacy. Furthermore, there are currently no disease-modifying OA drugs (DMOADs) with demonstrated efficacy in OA patients, which is, in part, attributed to a lack of full understanding of the pathogenesis of OA. The inability to translate findings from basic research to clinical applications also highlights the deficiencies in the available OA models at simulating the clinically relevant pathologies and responses to treatments in humans. In this review, the current status in the development of DMOADs will be first presented, with special attention to those in Phase II–IV clinical trials. Next, current in vitro, ex vivo, and in vivo OA models are summarized and the respective advantages and disadvantages of each are highlighted. Of note, the development and application of microphysiological or tissue-on-a-chip systems for modeling OA in humans are presented and the issues that need to be addressed in the future are discussed. Microphysiological systems should be given serious consideration for their inclusion in the DMOAD development pipeline, both for their ability to predict drug safety and efficacy in human clinical trials at present, as well as for their potential to serve as a test platform for personalized medicine.
Impact statement
At present, no disease-modifying osteoarthritis (OA) drugs (DMOADs) have been approved for widespread clinical use by regulatory bodies. The failure of developing effective DMOADs is likely owing to multiple factors, not the least of which are the intrinsic differences between the intact human knee joint and the preclinical models. This work summarizes the current OA models for the development of DMOADs, discusses the advantages/disadvantages of each, and then proposes future model development to aid in the discovery of effective and personalized DMOADs. The review also highlights the microphysiological systems, which are emerging as a new platform for drug development.
Burden of Osteoarthritis
Osteoarthritis (OA) is a progressive and debilitating disease that is a major cause of disability and reduced quality of life for patients worldwide. 1 According to the Centers for Disease Control (2015), there are currently 32.5 million adults in the United States who suffer from OA. The majority of these cases occur in adults over the age of 45, with women at higher risk 2 ; these numbers are expected to increase because of the aging population and prevalence of obesity. 3 Around 85% of reported cases occur in the knee, but the hip, hands, feet, and ankle exhibit OA as well.2,4 OA not only limits physical activity, but can increase social isolation, adding to psychological stress and resulting in depression.5,6 Furthermore, memory loss can occur in conjunction with pain related to OA.7,8 As OA progresses, so does the economic impact associated with health care costs and decreases in productivity.2,9
Symptom management strategies primarily target pain and include topical and oral nonsteroidal anti-inflammatory drugs, intra-articular corticosteroid and hyaluronate injections, and ultimately oral opioid analgesics. However, these drugs do not slow the progression of OA, and all are associated with potential side effects.
10
This leaves surgery, in the form of total joint arthroplasty (TJA), as the only long-term solution for most patients. The challenge with TJA is that it involves a significant surgical procedure associated with a relatively long recovery trajectory. The artificial joints have a finite lifespan, and revision joint replacement is often more complicated than the initial TJA. In addition, up to 20% of patients undergoing knee TJA are still in pain 1 year after surgery.
11
Thus, there is an urgent need for disease-modifying osteoarthritis drugs (DMOADs). In Table 1, agents in Phase II–IV OA trials listed in
Potential Disease-Modifying Osteoarthritis Drugs That Are Recently in Phase II–IV Clinical Trials (Data from clinicaltrials.gov, Up To September 30, 2020)
The studies that were completed in recent 10 years are also included.
ADAMTS5, a disintegrin and metalloproteinase with thrombospondin motifs 5; CatK, cathepsin K; CGRP, calcitonin gene-related peptide; CNS, central nervous system; FAAH, fatty acid amide hydrolase; FGF, fibroblast growth factor; IL, interleukin; IL-1(6)R, interleukin-1 (6) receptor; iNOS, inducible nitric oxide synthase; MMP, matrix metallopeptidase; P2X3R, purinergic P2X3 receptors; TNF-α, tumor necrosis factor-alpha; TRPV1, transient receptor potential cation channel, subfamily V, member 1.
Pathology of OA in Knee Joints
The knee joint is a complex organ system composed of multiple tissue elements that together contribute to its overall functionality. The dynamic interactions between the tissue elements support the concept that OA is a “whole joint disease.”24,25 There are at least six main tissue components within the knee joint: articular cartilage, subchondral bone, synovium, ligaments, menisci, and the infrapatellar fat pad (IPFP).26,27 Of these, pathological changes in cartilage, bone, and synovium have received the most intensive study. These joint components are also the primary targets for current DMOAD delivery (Fig. 1).
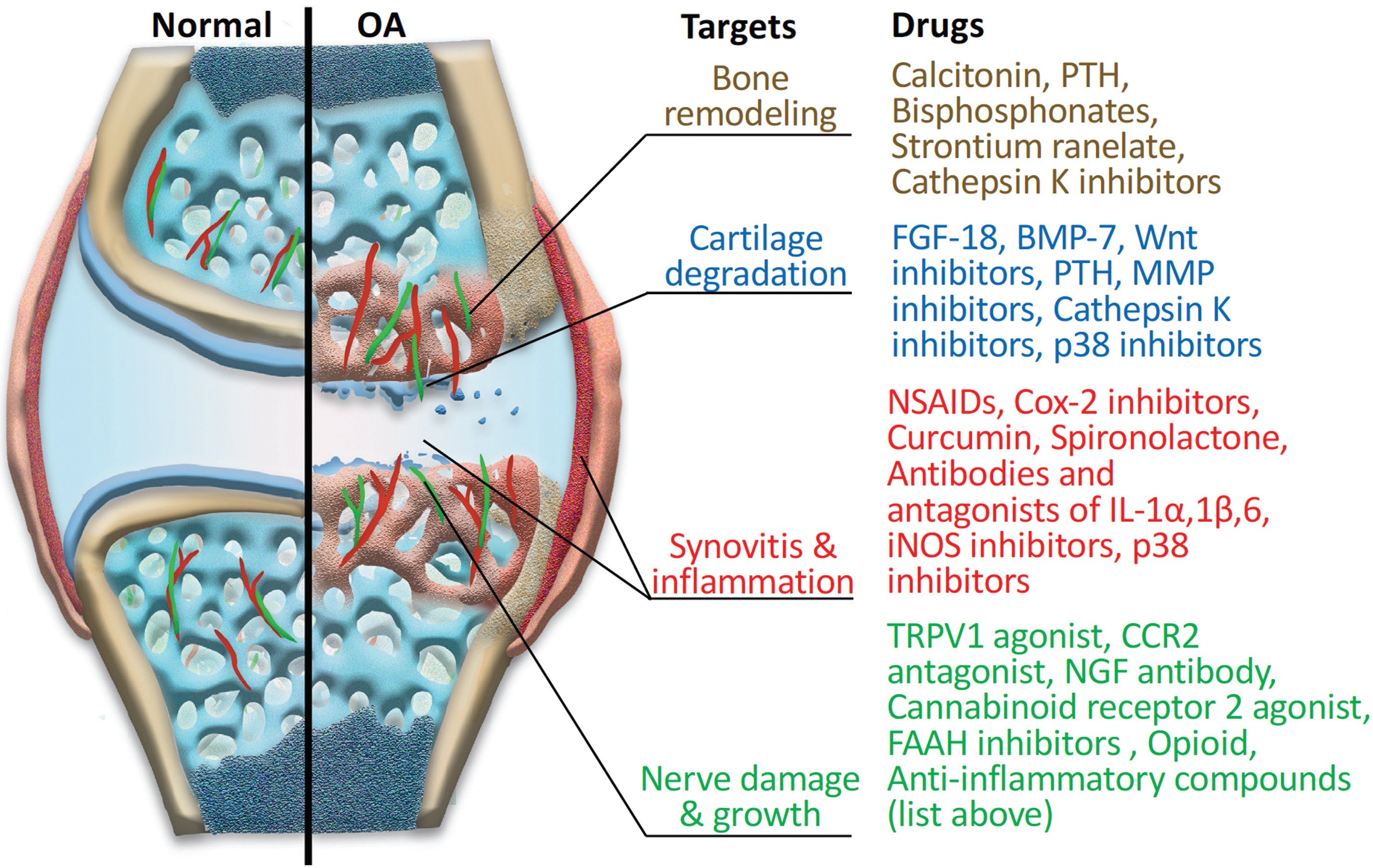
OA-associated histopathological changes in joint elements, and representative agents that target different pathological issues. OA, osteoarthritis. Color images are available online.
Cartilage is a hyaline, aneural, and avascular tissue with chondrocytes embedded in abundant extracellular matrix (ECM) consisting of type II collagen and sulfated proteoglycans. 28 The cartilage ECM functions to maintain frictionless contact of the synovial joint and supports mechanical loads and forces to which the knee is subjected. 28 Chondrocytes are the primary cell type of the cartilage that regulate its architecture and biochemical composition.24,29 In a healthy joint, chondrocytes are in a quiescent state and maintain the homeostasis of cartilage.25,30 However, under OA-like conditions, chondrocytes are “activated,” leading to the secretion of cytokines including interleukin (IL)-1, IL-4, IL-9, IL-13, and tumor necrosis factor-alpha (TNF-α), 10 which are accompanied by degradative enzymes including disintegrin and metalloproteinase with thrombospondin motifs (ADAMTS), and collagenases/matrix metalloproteinases (MMPs).25,31 The degradation of cartilage represents the most critical sign of OA.
Another essential component of the knee is the synovium. This fluid-secreting capsular tissue functions to lubricate and nourish the cartilage it encases. 32 The intra-articular side of the synovium surface is primarily composed of two types of synoviocytes: fibroblast- and macrophage-like cells.26,32 The fibroblast-like synoviocytes produce proteoglycans of the synovial ECM, such as hyaluronan (HA), which help to maintain synovial health.32,33 The macrophage-like synoviocytes remove tissue debris and are involved in the innate immune activation of the synovium during inflammation.32,33 In particular, cartilage degradation products can stimulate the synovium and induce the activation and migration of inflammatory cells, which produce and release cytokines and other substances mentioned previously.32,34 As inflammation within the synovium (synovitis) progresses, vascular endothelial growth factor is secreted by synovial macrophages and stimulates increased vascularization within the synovium and potentially vascular invasion of the cartilage.33,34 This increased vascularization also occurs in the subchondral bone as well and will be discussed later.
The synovium also plays a role in the structure and function of the IPFP, by forming the lining of the IPFP. 32 There is increasing evidence that the IPFP might also play a role in the progression of OA through the release of adipokines and cytokines from adipocytes that drive inflammation, a process presumably exacerbated in obese OA patients. 35 The level of inflammation observed in the IPFP and in the synovium are indicators of disease progression and are often used as a predictor of pain. 26
The subchondral bone is a distinct and essential component of the knee that is integrated with cartilage to form the osteochondral unit. With a mineralized ECM composed primarily of type I collagen, the subchondral bone has a distinct separation point with the cartilage called the tidemark, which delineates the calcified cartilage from the noncalcified cartilage.33,36 During OA, the tidemark moves into the noncalcified zone. 33 In addition, subchondral bone remodeling occurs between the calcified cartilage and the subchondral bone resulting in the formation of bone spurs, also known as osteophytes.24,31 These osteophytes play a role in the increase of pain caused by OA owing to the innervation of the bone. 37 In addition, the development of cysts and bone marrow lesions/edema, a clinical finding on magnetic resonance imaging (MRI), occurs in the subchondral bone. These sources of fluid buildup are thought to be a significant source of pain and are a central feature of OA. 37
The meniscus has an integral role in mechanical loading and shock absorption of the knee. Like cartilage, the meniscal ECM contains water, multiple collagen types, specifically type I collagen, and proteoglycans. 38 Prior trauma to the meniscus can lead to the onset of OA and is considered a significant risk factor for OA. 39 However, in OA patients, damage to the meniscus can result in degradation because of the release of inflammatory cytokines produced by the synovium and cartilage. 40 If mechanical trauma causes meniscal ECM degradation, such as loss of collagen, the resulting forces are then allocated to the cartilage owing to the loss of meniscal integrity; this in turn causes chondrocytes to produce inflammatory factors that result in further destruction of the meniscus, thus leading to the potential onset of OA.27,40
In addition to the tissues already discussed, other joint components, including muscle, intra-articular ligaments, and tendons also contribute to normal joint function, physiology, and OA pathogenesis. For example, trauma to the ligaments can cause bleeding, tissue degradation, and structural instability resulting in inflammation; these injuries are predisposing factors for OA. 41 Furthermore, these tissues have major biomechanical functions and their injuries, caused by abnormal mechanical loading, can eventually impact cartilage and bone, leading to joint diseases. 42
Current OA Models
There are a variety of models currently used to develop drugs for the treatment of OA. 43 In this section, we briefly describe the most common models and focus on how they are used for OA pharmaceutical development. It should be noted that treatment with IL-1β, commonly 10 ng/mL, is the most widely used method to generate OA-like phenotypes in various cell and explant cultures. However, it has been shown that in the OA knee joint, the average level of IL-1β is ∼20–30 pg/mL, 44 which is markedly lower than that used in many in vitro studies. Furthermore, most of the conventional OA in vitro and ex vivo models focus solely on cartilage, which fails to recapitulate the whole-joint nature of this disease. Therefore, any data generated with these models usually need to be re-evaluated in more physiologically relevant models, such as in vivo animal models or in vitro microphysiological systems (MPSs), which will be elaborated hereunder.
In addition, different in vitro culture methods result in different cell morphology, which has been shown to directly regulate chondrocyte phenotype. Typically, cells in monolayer culture and in the peripheral area of micromass cultures display a flat and well-extended shape, whereas in the center area of micromass culture, pellet culture and in-scaffold culture, cells adopted a sphere morphology. At present, it has been demonstrated that forcing chondrocytes to become round shape, such as in-agarose culture, can promote the expression of chondrogenic genes, which may function through modulating RhoA pathway and changing cytoskeletal structure.45–48
Monolayer cultures
Monolayer or two-dimensional (2D) culture cultures allow for the most convenient testing of therapeutics. The advantages of 2D culture include easy handling, need of a relatively low number of cells, and convenient experimental endpoints and analysis. Regarding the culture of chondrocytes, 2D culture was the first method used to study this cell type >50 years ago. 49 Overall, monolayer cultures of chondrocytes have greatly facilitated the understanding of chondrocyte phenotype, differentiation, the effects of cytokines and inflammation, and the alterations caused by exposure to growth factors. 50 For example, the 2D culture of chondrocytes permits the top surface of the cells to be exposed to inflammatory cytokines, such as IL-1β, in an effort to understand the consequences of their associated downstream inflammatory pathways on cartilage. 51 Koshy et al. used monolayer culture to pinpoint degradative mediators of cartilage degradation, 52 whereas Pearson et al. used this method to observe and clarify the differences in IL-6-mediated inflammation in obese versus nonobese OA patients. 53 Other research groups have used monolayer culture methods to study the role of synovium in OA.54,55
Two-dimensional cultures have been used to investigate plant extract-derived polyphenols to assess their anti-inflammatory potential in treating OA.56,57 For example, curcumin displayed anti-inflammatory activity in liposaccharide treated chondrocyte cultures. 58 Zheng et al. found that the administration of plumbagin, a compound that can be extracted from the roots of herbal therapeutics, to human chondrocytes in vitro successfully inhibited IL-1β inflammatory effects through the suppression of nuclear factor kappa beta (NF-κβ), 56 an inflammatory transcription factor responsive to the cytokines IL-1β and TNF-α. 59 More recently, curcumin, resveratrol, and epigallocatechin-3-gallate were shown to inhibit the production of reactive oxygen species and nitric oxide in the 2D culture of bovine and human chondrocytes, which implied their potential therapeutic values for OA clinical application. 60 A small-molecule inhibitor of the Wnt pathway was examined in 2D chondrocyte culture and it was shown to enhance chondrocyte differentiation and suppress degradation. 61 These results suggested that this compound might function as a novel DMOAD. Numerous miRNAs have also been studied using monolayer cultures to test their ability to inhibit inflammation. 62
Although monolayer culture protocols have aided with the testing of new DMOADs and the analysis of mechanistic pathways, there are significant disadvantages with their application for the study of OA. The knee is constantly subjected to loads and mechanical forces, which are nearly impossible to simulate in most monolayer cultures. 63 Cyclic tensile strain (CTS), a process that stretches the cell body through deforming the culture substate, has been explored to overcome this limitation. For example, Du et al. applied CTS on chondrocyte monolayer cultures and found that TRPV4-mediated Ca2+ signaling played a central role in the response of chondrocytes to physiologic levels of strain (3% and 8% of strain), whereas Piezo2-mediated Ca2+ signaling was central to injurious levels of strain (18% of strain). 64 In addition, CTS has been used to investigate diacerein, a potential DMOAD, on monolayered cultured OA chondrocytes, as well as explore its interaction with mechanotransduction pathways. 65
Chondrocytes in monolayer cultures also undergo dedifferentiation, resulting in the loss of type II collagen and aggrecan, and an increase of type I collagen and versican, thus altering the composition and natural structure of the ECM.63,66 Proteoglycans are also decreased with the dedifferentiation.67,68 The degradation of the natural ECM in the synovial joint is a primary factor in the progression of OA, and an accurate model of ECM degradation is imperative for the proper formulation of anti-inflammatory therapeutics. 69 Another issue with monolayer culture is the technical challenge of replicating the interaction of different cell types. Therefore, modeling OA in 2D cultures alone is inadequate to elucidate the interactions of different tissues of the joint.
Micromass culture
Micromass is a three-dimensional (3D), high-density culture system consisting of cell aggregates formed by seeding cells in droplets.70,71 Chondrocytes cultured as micromasses maintain higher levels of chondrogenesis 72 and produce an ECM that is rich in cartilage-associated proteoglycans and collagen, compared with 2D cultures of the same cell types. 73 Researchers have determined that the micromass-derived cartilage constructs were more extensive, more homogenous, and had less hypertrophic and fibrous features compared with pellet cultures formed by centrifugation of a cell suspension (see Pellet culture section). 74 Thus, micromass culture has been widely applied for studying chondrocyte cell physiology, pathophysiological mechanisms, and cartilage degradation.75,76 For example, Sun et al. recently used micromass culture to detect the effects of phosphocitrate, a potential DMOAD, on ECM production by OA chondrocytes. 77 A reliable assay system using micromass cultures of human chondrocyte line C-28/I2 was established by Greco et al. to demonstrate the modulatory functions of various pharmacological agents. 78
Although micromass is a classic in vitro culture model to generate cartilage tissue, it also has limitations. For example, chondrocyte micromass cultures maintained a differentiated phenotype up to 3 weeks, but culture durations longer than 6 weeks led to progressive dedifferentiation that should be considered during long-term evaluation. 79 In addition, the inability to study cell–cell and tissue–tissue interactions limits the application of the micromass culture system for understanding the pathogenesis of OA. These limitations call for more complex in vitro models.
Pellet culture
Another common method to create cartilage in vitro is the formation of chondrospheres or 3D cell pellets. Typically, these spheroids are generated by pelleting cells with centrifugation.49,80 In contrast to monolayer or micromass culture, 3D pellets allow cells to proliferate in all directions to better mimic the native environment of cartilage. Pellet cultures result in more robust chondrocyte formation, as indicated by higher glycosaminoglycan (GAG)/DNA ratios compared with the monolayer cultures. 81 The pellet culture model also allows the study of the cell–cell and cell–matrix interactions.66,82
Cartilage tissue generated from pellet cultures has been widely used in assessing potential DMOADs. Ziadlou et al. used the pellet model to test plant-based anti-inflammatory and NF-κβ pathway inhibiting drugs. 83 Specifically, they introduced 34 traditional Chinese medicine compounds to pellet cultures of human OA chondrocytes and investigated their influence on the ECM production and the expression of MMPs. Several of these compounds were shown to elevate ECM production. In particular, epimedin C enhanced the expression of type II collagen and aggrecan, potentially restoring the matrix loss in OA cartilage. 83 Another study tested the effects of a traditional Persian material known as Mummy, recognized for its ability to reduce joint inflammation. Polymerase chain reaction analysis determined that upon treatment with Mummy, OA pellets exposed to IL-1β had increased gene expression of type II collagen and downregulated expression of proinflammatory factors. 84
Although many studies have shown that the application of 3D pellet cultures can generate data that 2D models cannot, such as the study of ECM abundance and composition, this method also has its limitations. For example, pellets cannot be subjected to physiologically relevant mechanical forces precluding the ability of using this natural stimulus to study the progression of OA.82,85 Further engineering is thus needed to overcome some of these limitations of pellet cultures.
Three-dimensional scaffold cultures
Natural and synthetic materials have been used to construct 3D scaffolds for the engineering of different tissues. Hydrogels are commonly used to create cartilage tissue because of their inherent ability to retain the water, support cell proliferation and differentiation, and mimic native soft tissue. 86 Scaffold-based cultures may not only promote chondrogenesis, but also facilitate higher quality cartilage formation. For example, alginate beads were shown to yield more robust chondrogenesis compared with monolayer and pellet culture. 80 Chondrocytes derived from human mesenchymal stem cells (MSCs) displayed lower expression of hypertrophic and osteogenic genes in a hyaluronic acid hydrogel than in pellet culture. 87 Aside from maintaining chondrocyte phenotype, this culture method was also utilized to investigate the paracrine interactions between cells. For example, chondrocytes and macrophages were encapsulated in poly(ethylene glycol) diacrylate hydrogels, to better understand how macrophages alter the phenotypes of chondrocytes. In this study, the hydrogel network was tethered with the integrin-binding peptide, arginine–glycine–aspartic acid, to allow for cell–ECM crosstalk. 88 The use of scaffolds can also be used to simulate the physical properties of cartilage and thereby allow the assessment of the effects of DMOADs on the mechanobiological characteristics of cartilage.
Studies have used 3D culture of chondrocytes followed by the induction of OA for drug screening. Sun et al. successfully created a silk-based 3D engineered cartilage system and introduced inflammatory factors such as TNF-α and IL-1β to simulate an OA environment. 89 They have subsequently used this model for screening potential therapeutics. A collagen matrix laden with chondrocytes was used in another study that enabled the authors to assess the impact of incorporating platelet-rich plasma (PRP) on the inhibition of ECM loss. 90 The authors then used the same neo-cartilage to test the effects of hyaluronic acid and PRP on chondrocytes challenged with IL-1β. 91 Other researchers have used this model to monitor changes in OA-related gene expression after drug treatment, 92 to understand the effects of small molecule inhibitors on common cartilage degrading proteases (MMPs and ADAMTS),93,94 and to determine how growth factors aid in the proliferation of chondrocytes in vitro. 95 3D models have also been routinely used to assess the basis for the therapeutic efficacy of drugs such as FK506, originally thought to be a T cell suppressor, in the treatment of OA.96,97
Scaffolds can also be used to deliver candidate drugs, thereby avoiding complications associated with repeated intra-articular injections. For example, a poly(lactic-co-glycolic acid) scaffold was used to encapsulate rapamycin, which allowed for a controlled release of rapamycin for several days. 98 This study also reported the first successful administration of rapamycin in microparticle form for the prevention of senescence and OA changes in chondrocytes exposed to an induced oxidative stress microenvironment. 98
A major disadvantage of the most widely used scaffold cultures is that they fail to fully simulate the biological cues of the native cartilage ECM to support chondrogenesis. In addition, cell–cell interaction is often lacking. These limitations require the further development of chondrosupportive biomaterials, as well as the optimization of cell encapsulation methods. For example, HA hydrogels, which were functionalized with N-cadherin mimetic peptides, promoted a more robust chondrogenesis of MSCs and cartilage matrix production, compared with HA hydrogels in which a scrambled peptide was included. 99 Attempts to increase the cell–cell interaction in scaffolds have also been reported. For example, Rogan et al. generated an MSC-based μPellet (∼100 cells/pellet) before encapsulating them into a scaffold. However, this approach resulted in less chondrogenesis than when single cells were encapsulated into a scaffold. 100
Explant cultures
Also known as ex vivo cultures, tissue explants are considered the most natural DMOAD model compared with other in vitro cultures. Tissue explants are composed of tissue-specific cells that reside within the native ECM. They have therefore been used to study the cell–cell and cell–matrix interactions that occur within the native cartilage tissue.66,101 More importantly, explant cultures largely retain the native mechanical properties of tissues, and therefore are particularly useful in studying the role of mechanical loads in OA onset and progression. However, tissue explants tend to have a short life span, exhibiting tissue death along the outer edge of the explant, likely owing to the injury from the harvesting process.82,85 Therefore, they are not ideal for long-term studies. Potentially more problematic is that once removed from the donor, cell phenotypes start to change. 85 Furthermore, although this model might be inexpensive, access to tissue donors can be difficult and there may be considerable variability among different donor sites and donors.82,85
Knee joint components are known to respond to mechanical cues, and therefore explant cultures are commonly subjected to different loading protocols to determine how mechanical load affects the physiology of the knee. 85 Both static and dynamic compression methods are used. 102 For example, the drop-tower protocol, in which a free weight is released at a specific height and dropped onto the tissue to simulate a single impact load, has been used, and other methods such as hydraulic loading chambers have also been used to apply load in a cyclic manner. 85 Alexander et al. developed a spring-loaded system with spherical impact geometry to assess the effects of mechanical injury on the cell–cell interactions, ECM formation, and overall cell viability. 103 Dolzani et al. used a compression-inducing bioreactor to simulate physiological mechanical forces encountered by joint tissues. In this study, cartilage explants were loaded between two compression plates. A pressurized air system was used to reduce the distance between the plates, thus applying an unconfined compression to the explants. 104 Finally, Cutcliffe and DeFrate used explants to determine whether or not unloading/recovery response of cartilage after mechanical load could be used to replace the load response when used in in vivo models using MRI. 105 Thus, the use of explants for mechanical loading provides valuable information on how native cartilage responds to physical damage.
Explants of other knee joint elements have also been used to study their interaction with cartilage. Osteochondral explants from OA donors might be valuable for testing DMOADs. Geurts et al. observed that human explant specimens were capable of maintaining viability and undergoing an inflammatory response after TLR4 agonist exposure. 106 Nishimuta et al. showed that healthy IPFP explants promoted GAG production in cartilage explants. 107 In another study, He et al. demonstrated that conditioned medium from IPFP (FP-CM) aggravated GAG release in mechanically traumatized cartilage but did not significantly affect healthy cartilage. 108 FP-CM also enhanced the gene expression of cyclooxygenase-2, inducible nitric oxide synthase, and IL-6 in traumatized cartilage explants, compared with the nonconditioned medium. Of importance, they found that IL-6 was a crucial tissue degeneration mediator.
Synovium explants have also been used to research the pathophysiology of OA and test potential therapies. Synovial explants collected from OA patients have been used to test the anti-inflammatory and anti-catabolic, paracrine effects of MSCs. 109 When mechanically injured bovine cartilage was cocultured with bovine synovium/joint capsule (SJC) explants, the presence of SJC resulted in earlier aggrecan proteolysis and the release of additional types of aggrecan fragments, indicating the involvement of synovium-secreted molecules in the cleavage of cartilage aggrecan. 110 Beekhuizen et al. cocultured synovium and cartilage from OA donors and evaluated several outcome parameters, such as GAG release and content, MMP activity, and cytokine production. 111 This model was proposed to assess the effect of potential OA therapies. In fact, a bovine synovium–cartilage coculture model has been used to study the possible protective effects of IL-1 receptor antagonist (IL-1Ra) against catabolic activities in the cartilage explants induced by the proinflammatory cytokine IL-1α. 112 Of interest, cartilage catabolism could be more effectively suppressed by IL-1Ra addition in the presence of synovial explants. 112 In human articular cartilage–synovium cocultures, IL-1β-induced degradation of cartilage proteoglycans could be blocked by the selective cyclooxygenase 2 inhibitor, SC-236, suggesting the potential of this small molecule to inhibit cartilage degeneration. 113
The meniscus has a key biomechanical role of load distribution and shock absorption, and meniscal damage is frequently observed in osteoarthritic knee joints. 114 To understand the involvement of traumatic meniscus injury in OA pathogenesis, Nishimuta and Levenston 115 applied confined compressive overload on bovine meniscus explants and observed biological damage of the tissue even without obvious macroscopic injury. The authors also established a meniscus–IPFP coculture model, where the IPFP displayed a modulatory role in the metabolism of GAGs in the meniscus explants. 107 Gupta et al.116,117 stimulated porcine menisci with pathological overloading, which was found to upregulate the expression of major inflammatory and degenerative genes and increase the release of nitric oxide and GAGs. Models involving meniscus explants have been used to test several potential therapies for joint diseases, such as PRP, 118 insulin-like growth factor-I, 119 transforming tissue growth factor β3 (TGF-β3),120,121 TGF-β1, 119 basic fibroblast growth factor, 119 connective tissue growth factor, 120 and platelet-derived growth factor-AB. 119 What is clear from these studies is that the clinical relevance of meniscus explant-based in vitro models used to study joint pathophysiology is highly dependent on the recapitulation of tissue crosstalk between the meniscus and other joint components such as the articular cartilage, IPFP, and synovium. Future in vitro studies using meniscus explants would benefit from including multiple joint tissues. 122
Animal models
Given that the complex physiology of the knee joint has not been fully recapitulated in vitro, researchers often use in vivo animal models of OA. The stifle is the primary joint targeted for OA studies in animal models.40,123 A number of models are widely used and have yielded valuable information regarding the onset, signs, and progression of OA. 124 These models are also widely used to investigate the safety and efficacy of therapeutic interventions of OA. 125 There are a variety of small and large animal models of OA. Small animals such as rodents (mice and rats), rabbits, and guinea pigs are used because of their ready procurement, rapid OA progression, and ease of handling.43,126 However, these models may not accurately recapitulate the anatomy or physiology of the human knee joint. Although large animals such as dogs, horses, and sheep are used to address this issue, they are more expensive, difficult to work with, and tend to develop OA more slowly than the small animal models. 43
As summarized in Table 2, several methods are commonly used to create OA in animals. Surgical methods are commonly used to create mechanical instability and induce OA development and progression.123,124,127 Vincent suggested that research in surgical preclinical OA models aligns well with findings in clinical trials. 128 Destabilization of medial meniscus is one of the most studied methods to create OA in rodents. 129 In these models, the meniscus is surgically injured, although the surrounding ligaments can also be damaged. 123 Another model that is commonly used is anterior cruciate ligament (ACL) transection, in which the ACL is transected and causes instability of the joint. 130 Injury to the joint stimulates OA onset by the effect of inflammatory factors.
Current Osteoarthritis Animal Models
ACL, anterior cruciate ligament; DMM, destabilization of medial meniscus; MIA, monosodium iodoacetate; OA, osteoarthritis.
Chemical induction of OA is also widely used, where chemicals are introduced to the intra-articular surface that impact the homeostasis of the joint, leading to the release of inflammatory cytokines. 127 Common chemicals used include monosodium iodoacetate (MIA), papain, and collagenases.123,126 MIA inhibits chondrocyte function by halting the process of glycolysis, leading to chondrocyte apoptosis, inflammation, and the onset of OA.123,127 In addition, there are spontaneous cases of OA, owing to the genetics of the animal; this is common in dogs and guinea pigs. Recently, inspired by the link between obesity and OA, 131 high-fat diet-induced OA models have also been developed. The contribution of adipose tissue to OA has been shown in animal models.132–134 Serum levels of adipose-derived cytokines are elevated in OA patients, suggesting that metabolic disruption of adipose tissue may play a role in the severity and progression of OA. 135 Finally, to avoid the confounding effects because of the surgical/invasive injury procedure itself, noninvasive injury methods through mechanically inducing a joint injury externally have also been used in creating OA models. 136 This type of model facilitates the study of early adaptive processes at the time of injury, thus may be more representative of post-traumatic OA in humans.
The choice of an animal model and method of creating OA is based on the specific etiology and the purpose of the study. 43 Although there are numerous animal models to choose to study therapeutic efficacy and OA progression, it is still difficult to ascertain whether these models accurately simulate OA in human joints.
MPSs to simulate knee joint in vitro
MPSs, also called tissue/organ-on-a-chip, are emerging as a new platform for drug development.143,144 The primary endpoint for tissue-on-a-chip technology is to offer a system that simulates the in vivo microenvironment characterized by diverse cellular composition, tissue-specific ECM, and interactive physiological biochemical and physical signals. 145 By using human cells and integrating multiple tissues, it may be possible to partially overcome the limitations of current animal models and in vitro culture assays.49,146 Therefore, researchers are attempting to develop MPS that replicates the knee joint using human cells.
Although the “joint-on-a-chip” concept has been coined,1,49,146 the successful generation of such systems has not yet been reported. As mentioned previously, OA is considered a whole joint disease. 1 The multiple tissue types involved in the synovial joint require the creation of a microenvironment that is able to mimic the joint as a whole. Given the unique anatomical structure of the knee joint and its complex mechanical motion, in vitro knee joint simulation poses a technical challenge. Many MPS models are in the early stages of development, focusing on a single cell type. However, a few MPS that incorporate multiple cell lines have been developed. 1 In 2014, our team constructed, for the first time, an osteochondral tissue chip derived from human MSCs, 147 which has recently been expanded by using induced pluripotent stem cells as the constituent cell source. 148 Recently, the development of a polydimethylsiloxane-based cartilage-one-a-chip by Occhetta et al. focused on the mechanical compression of chondrocytes for simulating the effects of mechanical loading. 149
Although joint-on-a-chip technology holds tremendous promise, there are still several conceptual and technical barriers. For example, it is unclear how best to model the local and systemic influences on tissue properties, including physical and chemical signals (Fig. 2). Nevertheless, similar to the development of other tissue/organ chips,149–152 engineering a knee joint to fully recapitulate the native counterpart may not be necessary. That is, it may only be necessary to recapitulate select essential aspects of the organ physiology and diseases, and then use this model to generate new information on the screening of new drugs for safety and efficacy in humans. 151
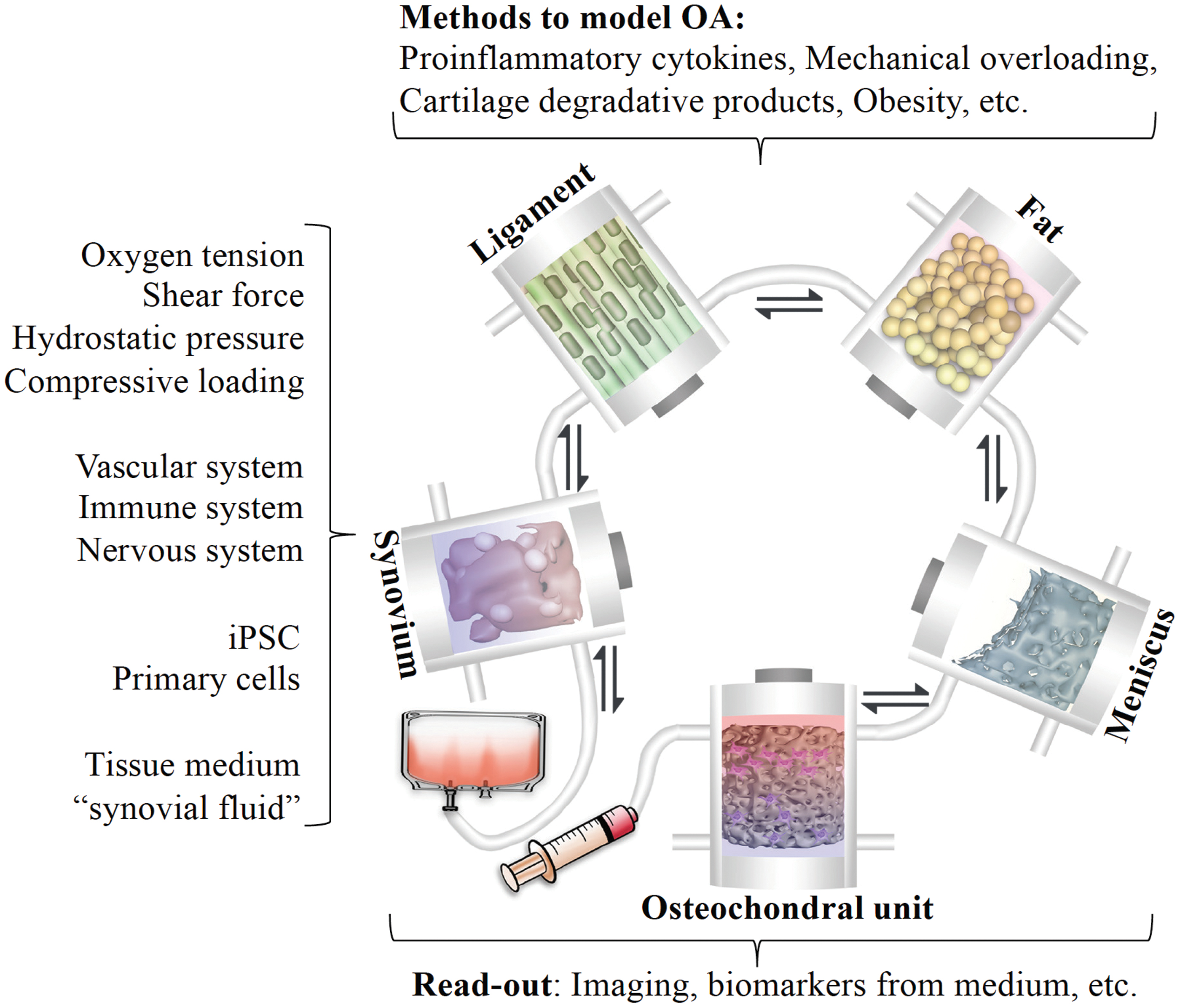
Generation of knee joint MPS through integrating individual tissue modules. Each tissue is perfused with the tissue-specific medium on one side and the “synovial fluid” on the other side, which is shared by all tissues except bone. The flow of the “synovial fluid” is bi-directional so that it can be conditioned and sensed by all tissues, simulating their crosstalk in the native knee joint. The inclusion of patient-specific cells allows the generation of personalized chip and the development of personalized DMOADs. The biomarkers in the “synovial fluid” are used to assess the types and severity of OA, as well as inform the treatment efficacy. DMOAD, disease-modifying osteoarthritis drug; MPS, microphysiological system. Color images are available online.
In summary, despite the multiple clinical trials that have been reported to date, many of the drugs that showed promising results in preclinical models have failed to demonstrate efficacy in OA patients. This failure rate is likely because of multiple factors, not the least of which are the intrinsic differences between the intact human knee joint and the preclinical models used to identify putative therapeutic targets and screen for efficacy. 153 The significance of these deficiencies was succinctly stated by Malfait and Little, who concluded that current preclinical OA models were poor predictors of the outcomes of clinical trials. 138 Therefore, identification of a relevant preclinical model would facilitate a clearer understanding of the drug mechanisms, safety and efficacy in OA before human studies and could potentially minimize the loss of valuable time and costly resources.
Conclusion and Future Perspectives
The current lack of robust, scalable, and physiologically relevant models of the human knee joint represents a significant impediment for the elucidation of the pathogenesis of OA and the discovery and development of DMOADs. OA can be caused by numerous factors including heredity, obesity, trauma, congenital or developmental anomalies, and other factors. 154 It is, thus, not surprising that there is extensive heterogeneity in disease presentation and progression in different OA patients, suggesting that patients should benefit from personalized medicine. Therefore, a more realistic goal may be to classify OA patients based on some validated common features, and then use models that most closely recapitulate OA to develop the DMOADs for this subgroup of OA patients (Fig. 3). In addition, comprehensive patient-specific efficacy/toxicity prediction models must be developed.

The DMOAD development pipeline that enables precision medicine. In traditional drug development, the potential agents are created (Step 1) and then tested in 2D or 3D disease models (Step 2). The candidates that show efficacy without cytotoxicity are further screened in animal models (Step 3) before one to two drugs finally enter human clinical trial (Step 4). In general, the conventional models for drug testing lack the personalized features of participants in the clinical trials. In the future, as the first step toward “personalized OA medicine,” validated biomarkers will be used to first classify patients into different groups (endotypes or phenotypes). By studying the specific etiologies and pathologies, drug candidates and testing models will be developed for the different patient groups. Next, by using patient-derived cells and simulating the specific disease features of the patient, the personalized models will be applied to develop candidate therapeutics for the specific patient. With the capability of using human cells, including differentiated cells, MSCs, and/or induced pluripotent stem cells, and recapitulating relevant human physiological parameters, MPS represent a potentially high-utility system in the development of personalized DMOADs. In particular, the observations derived from the two physiological models, that is, MPS and animals, can be cross-checked and validated to further enhance the prediction of drug efficacy and toxicity in humans. 2D, two-dimensional; 3D, three-dimensional; MSC, mesenchymal stem cell. Color images are available online.
In that regard, OA-specific and sensitive biomarkers will be critical for the accurate classification of the phenotype of each patient to aid in the prediction of appropriate interventions. This approach will encompass the key principles of personalized medicine for OA treatment. Although several molecules, such as urinary excreted CTX-II (C-terminal cross-linked telopeptide of type II collagen) and serum COMP (cartilage oligomeric protein) have been proposed as predictive OA biomarkers, biomarker(s) that can precisely distinguish the etiologies/pathologies of different subgroups of OA patients or determine treatment efficacy have not been established. This represents a major obstacle to the development of personalized OA models and the future development of DMOADs. Recently, mass spectrometry, a technology that can examine candidate proteins without being limited by the availability of antibodies, has been used to profile metabolomics in human OA synovial fluid.155,156 In these studies, different metabolomic phenotypes were found within healthy, early, and late OA cohorts, and several pathways, such as those related to keratan sulfate and N-glycan degradation, may provide new information in developing biomarkers of OA. It should be noted that while obtaining a blood or urine sample is less invasive than synovial fluid, molecules from the diseased joint must gain entrance to the synovium before entering the systemic circulation. The efficiency of such penetration is unknown. In addition, the molecules are diluted significantly and subjected to potential degradation in the blood. Therefore, synovial fluid remains the most relevant sample for the isolation of biomarkers.
Extensive evidence has demonstrated that cell–cell crosstalk is a primary contributor to OA pathogenesis. It is expected that such communication will also play a key role in the prevention or reversal of OA after treatment. For example, the physiological models with multiple tissues, such as MPSs and animal models, should provide more power in terms of predicting the toxicity and efficacy of drugs in clinical trials. As demonstrated in Figure 3, these two types of models can be complementary. For example, MPSs can be used to exclude the drugs that may be toxic to human cells, thus reducing animal use. In addition, the drugs that are screened in animal studies can be further validated in the MPSs and inform the patient subpopulations that may benefit from the drugs. Also, to enable personalized medicine, the new OA models need to be versatile with the capacity to readily generate different types of pathological changes.
Moreover, more comprehensive tools are needed to further assess the OA models, as well as the effect of treatments. Currently, most studies use limited parameters, such as MMP-13 expression, GAG loss, and the presence of proinflammatory cytokines, to indicate the disease state. However, at least 1500 genes are found to be differentially expressed in chondrocytes isolated from the intact and damaged areas.157,158 Therefore, “omic”-based methods, such as mass spectrometry mentioned previously, will facilitate future studies. The comprehensive characterization of models not only improves the classification of patients and indicates the fidelity of modeling, but also may reveal potential adverse or beneficial effects of treatments that cannot be identified through analysis of the “known” targets alone. At present, such “omic” studies are rarely seen in the testing of DMOADs.
Finally, to further validate the models to enable the prediction of the efficacy of novel therapeutic interventions in humans, it is important to first assess the impact of agents with known clinical efficacy. This validation step will justify moving forward to screen for new drugs. Ideally, one should start with the “gold standard,” that is, a drug with well-recognized treatment efficacy. However, to date, there are no FDA-approved DMOADs, and numerous late-stage clinical trials have failed to demonstrate effectiveness. 154 We may examine the effect of these failed drugs in the OA models and compare the results with clinical observations. Ideally, the efficacious models should be capable of reproducing the deficiencies of the failed drug.
In conclusion, clinically relevant and personalized models of OA are urgently needed to enhance our understanding of the pathogenesis of joint diseases in humans and facilitate the discovery and development of novel drug treatments. 1 In Figure 3, we summarize the current models and demonstrate their utilities in the DMOAD development pipeline. With the development of efficacious biomarkers and “true” MPS, we will finally be able to apply precision medicine in the treatment of OA. In particular, the inclusion of MPSs will increase the predictive power in the discovery phase, reduce animal numbers in the preclinical stage, and predict the efficacy and toxicity of compounds before human clinical trials.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work is supported by the NIH (UH3TR002136, UG3TR003090).