
Abstract
A chondral injury is a limiting disease that can affect the quality of life and be an economic burden due to the cost of immediate treatment and loss in work productivity. If left untreated, such an injury may progress to osteoarthritis, a degenerative and debilitating joint disease characterized by pain and functional impairment. Mesenchymal stromal cells (MSCs), which have immune-modulatory properties and the ability to differentiate into chondroblasts and osteoblasts, are a predictable source for the treatment of cartilage injuries. This article presents tools to evaluate cartilage restoration by tissue engineering and cell therapy treatment in a translational and preclinical large animal model. In this controlled experimental study with 14 miniature pigs, a scaffold-free tissue engineering construct (TEC) derived from dental pulp and synovial MSCs for cartilage therapy was tested. Total thickness cartilage defects were performed in both posterior knees. The defect was left empty in one of the knees, and the other received the TEC. The tissue repair was morphologically assessed by magnetic resonance imaging (MRI) using the three-dimensional double echo steady-state (3D-DESS) sequence, and compositional assessment was carried out based on the T2 mapping technique. The osteochondral specimens were fixed for histopathology, decalcified, subjected to standard histological processing, sectioned, and stained with hematoxylin and eosin. The sections stained for immunohistochemical detection of collagen types were digested with pepsin and chondroitinase and incubated with antibodies against them. The mechanical evaluation involved analysis of Young's modulus of the cartilage samples based on the indentation and maximum compression test. In addition, a finite element model was used to simulate and characterize properties of the osteochondral block. At 6 months after surgery, there were no complications with the animals and the MRI, histological, immunohistochemical, and biomechanical evaluations proved to be effective and qualified to differentiate good quality chondral repair from inadequate repair tissue. The proposed methods were feasible and capable to properly evaluate the defect filled with TEC containing stromal cells after 6 months of follow-up in a large animal model for articular cartilage restoration.
Impact Statement
Articular chondral injuries are prevalent and represent an economic burden due to the cost of treatment. The engineering of cartilage tissue can promote the repair of chondral injuries and is dependent on selecting appropriate cells and biocompatible frameworks. In this article, methods for evaluation of a scaffold-free cell delivery system made from mesenchymal stromal cells were present in a translational study that allows further clinical safety and efficacy trials.
Introduction
The chondral lesion is a prevalent pathology, reaching as much as 63% of the population, causing clinical repercussions in quality of life and economic burden due to the cost of treatment and loss in work productivity.1–3 Untreated cartilage defects may enlarge and result in lesions in the subchondral bone, leading to biomechanics and homeostasis disturbances in the knee. Indeed, a cartilage lesion can predispose an individual to osteoarthritis (OA). 4 Pain and loss of mobility characterize the progress of this disease, which is highly disabling and without cure.5,6 For this reason, the study of new therapies for cartilage lesions is clinically relevant and deserves to be highlighted.
Attention to research involving tissue engineering principles for cartilage therapy has risen in the past decades. 7 Langer and Vacanti, in 1993, described tissue engineering as a multidisciplinary field that applies theories of different disciplines in the development of biological substitutes that seek to restore, maintain, or improve the function of organs and tissues affected by pathologies. 8 The engineering of cartilage tissue is critically dependent on selecting appropriate cells, such as mesenchymal stromal cells (MSCs), 9 biocompatible frameworks, and inductor factors. 10
MSCs may be isolated from bone marrow, adipose tissue, dental pulp, synovial membrane, and other different tissues. 7 The dental pulp contains a stromal cell niche where the dental pulp stromal cells (DPSCs) preserve their self-renewal capacity due to the active environment in the dental pulp of deciduous teeth.11–13 DPSCs can differentiate into chondroblasts and osteoblasts suggesting that this type of stem cell is helpful for tissue engineering to treat cartilage injuries. 14
Patients with cartilage injuries often undergo knee arthroscopic surgery for another reason, such as the regularization of meniscal injuries. During this procedure, synovia and fat pad can be easily harvested, which are another source of MSCs and cause minimal or no complications in the donation area. 15 In addition, synovial MSCs (SMSCs) have a greater proliferation and chondrogenic potential than bone marrow MSCs.15,16
Furthermore, local delivery of cells has been another concern for cell-based therapy. In this research, we used a scaffold-free cell delivery system called tissue engineering construct (TEC). It is a structure formed by cells (MSC) and extracellular matrix (ECM) cultured in a three-dimensional (3D) environment, which is vital to optimizing cell proliferation and differentiation. 7
The clinical relevance of this article is to present methods for a translational study and to allow further clinical trial phase I/II studies of safety and efficacy using good manufacturing practices (GMP) for human usage.17,18 This methodological study describes some evaluation tools for cartilage restoration by cell therapy treatments in a preclinical large animal model.
Methods
This study was conducted in collaboration with the Sírio-Libanês Hospital in Sao Paulo and Hospital das Clínicas, University of Sao Paulo (USP), Brazil.
The methods for assessing cartilage repair involved (1) magnetic resonance imaging (MRI) for morphological and quantitative evaluation, (2) macroscopic, histological, and immune histochemistry tests for collagen types, and (3) mechanical characterization, which are presented in detail hereunder. Outcomes were measured after 6 months of surgery follow-up.
Harvesting, isolation, and expansion of MSCs
The ethics committee approved this research at the Hospital das Clínicas, USP (protocol: CAPPesq n° 15428, IOT n° 1216). All patients signed informed consent forms for synovial and fat-pad discarded tissue usage in research.
In this study, the MSCs were harvested from two different sites, the synovial tissue from human knees and deciduous teeth. The harvesting process of synovial tissue included seven patients between 22 and 34 years of age (five men and two women), who underwent arthroscopic surgery for anterior cruciate ligament or meniscus injury. Patients with a history of surgery, infection, inflammatory arthritis, and pregnant women were excluded.
Knee synovia was harvested at the beginning of arthroscopy through the anterolateral portal. A sample up to 1 g of tissue with synovia was stored in a 50 mL sterile falcon flask containing phosphate-buffered saline (PBS) (Gibco Invitrogen) and was sent immediately to the Advanced Cellular Technology Laboratory (ACTL) at Sírio-Libanês Hospital and processed up to 6 h after harvesting. The presence of aerobic and anaerobic bacteria and fungi in harvested tissue was analyzed with the automated microbial detection system BacT/Alert 3D (BioMérieux, France), and a mycoplasma detection kit (MycoAlert; Lonza) was used for mycoplasma detection.
Each sample was washed twice with PBS plus 4% penicillin–streptomycin. Its digestion was performed using 0.2% Collagenase NB 4G Proved Grade (Serva Electrophoresis, Germany) for 90 min at 37°C. This process ended by adding 4 mL of Dulbecco's modified Eagle's medium/Nutrient Mixture F-12 (DMEM/F-12; Gibco Invitrogen) supplemented with HyClone 15% fetal bovine serum (FBS) U.S. Origin (Cytiva), and centrifuged at 300 g for 5 min. Next, the cell pellet was diluted in DMEM/F-12 and FBS before plating the cells in a 25 cm2 cell culture flask.
The other harvesting sites were the deciduous teeth of seven healthy children (five boys and two girls, 7 to 9 years old), which were lost spontaneously. The dental pulps were obtained from dental offices in our affiliate institutions and immediately added to a sterile collector with 2 mL DMEM–F12 solution supplemented with 100 IU/mL penicillin–streptomycin. Deciduous dental pulp was processed on average at 15 h after initial collection to avoid cell loss and possible cross-contamination.
In the laboratory, the deciduous dental pulp specimens were washed twice with PBS, and digested with a solution containing 1 mg/mL of trypsin in PBS for 30 min at 37°C. After tissue digestion, the samples were centrifuged at 300 g for 5 min. After these procedures, the cells were cultured in a 25 cm2 culture flask.
The 14 MSC samples used in this research (7 from synovial tissue and 7 from deciduous teeth) were processed, cultured, and plated separately. The cell culture was performed in 25 cm2 flasks maintained with DMEM–F12 solution supplemented with 15% FBS, 4% NEAA (nonessential amino acid solution, Gibco Invitrogen), and 4% penicillin–streptomycin and incubated at 37°C in an atmosphere of 10% CO2. Every 3 days, the culture medium was replaced.15,19
All cells were isolated and cultivated in a GMP laboratory for human usage, following the directives elaborated by the national regulatory authority (ANVISA, RDC N° 214) to guarantee the standards of efficacy and safety in the manufacturing processes. According to these directives, our laboratory facilities have regular inspections, provision of regular reports, conduct staff training, execute routine equipment maintenance and risk and adverse event assessments, and usefully traceable reagents and processes. We have the recommended infrastructure for cleanrooms, including airflow and air particulate control (high-efficiency particulate air filter) and antechambers for personal protection attiring. Only human cells can be processed at our ACTL. Furthermore, all reagents from cell isolation to cryopreservation are certified, prion-free, and nonpyrogenic. 20
Characterization and differentiation of MSCs
The SMSCs and DPSCs were characterized by flow cytometry between passages four and five. In total, 1 × 106 cells of each population, individually, were evaluated. The cells were labeled with monoclonal antibodies, including CD29-PE, CD44-PE, CD73-FITC, CD90-FITC, CD105-PE, CD166- PE, CD31-FICT, CD34-FITC, and CD45-PE (BD Biosciences). An appropriate isotype-matched control antibody was used for all analyses. Flow cytometry was performed with a FACSCalibur flow cytometer (BD Biosciences), and the data were analyzed using Cell Quest Software (BD Biosciences).
The MSC strains (fourth or fifth passage) were induced in vitro into osteogenic, chondrogenic, and adipogenic differentiation with respective specific StemPro Differentiation Kit (Gibco Invitrogen) for osteogenesis, chondrogenesis, and adipogenesis. According to manufacturer data sheets, the three media types were prepared. 15
To confirm osteogenic differentiation after 21 days, cells were fixed with 70% ethanol and incubated in 0.2% Alizarin Red S (Sigma-Aldrich, Germany) for 30 min. For chondrogenic differentiation verification after 21 days, cells were fixed with 4% paraformaldehyde (PFA) for 10 min, and Alcian Blue 8GX (Sigma-Aldrich) was used to stain the ECM mucopolysaccharides. Moreover, for adipogenic differentiation, after 18 days, the cells were fixed with 4% PFA for 30 min and stained with a working solution of 0.5% oil red O (Sigma-Aldrich) for 20 min. Finally, we analyzed the staining by optical microscopy (Microscope Olympus CK40). 15
Development of the TEC
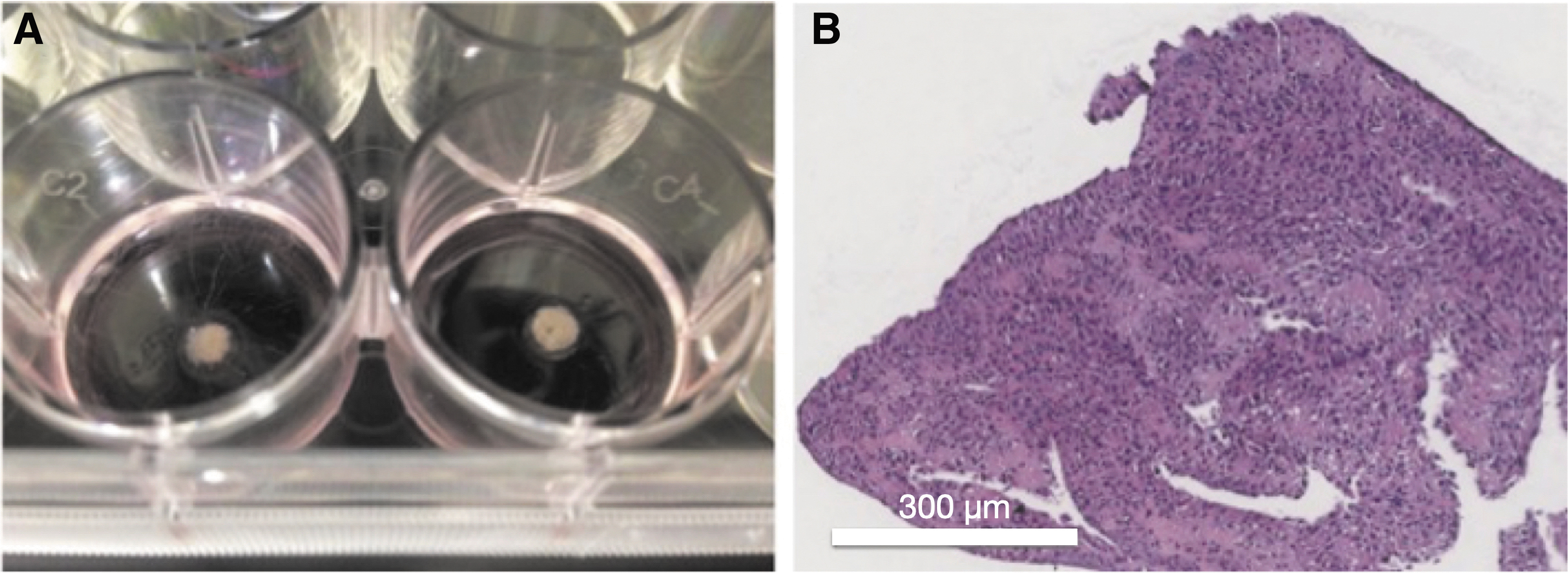
After cell culture, the MSCs from each sample were plated in a 12-well culture dish. Each well contained cells at a density of 4.0 × 105 cells/cm2 in culture medium to which 0.2 mM ascorbic acid 2-phosphate (Asc-2P; Sigma-Aldrich) was added. After ∼15 days, the cultured cells and ECM synthesized by these cells became a layered structure and could be detached from the substratum by applying a gentle shear stress using a pipette. The detached complex formed a 3D structure by active tissue contraction that began after the detachment. It led to the development of a several millimeters thick spherical body in each well. This 3D tissue formed by cells and ECM has termed TEC (Fig. 1). The TECs from the same dish were gathered, forming a grouped TEC ∼1 cm in diameter.
Experiment
Experimental design
Animal model
The ethics and research committee at Sírio-Libanês Hospital approved this study (protocol: CEUA-P 2015-07). Fourteen female adult miniature pigs BR1 21 (mini-pigs) were used in this research. Information on the characteristics, care, and procedures related to animals was collected following the ARRIVE Guidelines Checklist 22 and kept in the REDCAP digital repository. 23
Surgical technique
First, the animals were induced for general anesthesia with propofol, and anesthesia was maintained throughout surgery with isoflurane. Morphine was used for analgesia. Mini-pigs were placed in supine position on the operating table. Both limbs were scrubbed and sterile covered.
At the time of surgery, the surgeon was told which side would receive the TEC, while the defect in the other knee was left empty. Randomization was performed by a researcher not involved in the surgical procedure.
Medial arthrotomies of the knee in posterior limbs (∼6 cm) were performed to expose the medial condyle articular cartilage. 24
A full-thickness cartilage defect measuring 6 mm in diameter was made in the loading area of the medial femoral condyle of the two hind limbs of each animal, using a biopsy punch, and then the calcified basal layer of the cartilage was removed with a scalpel blade. Subsequently, the TEC was placed into one of the defects (Fig. 2). After implantation, the TEC firmly adhered to the injured joint surface without suturing.

Six millimeters defect in the cartilage of the femoral condyle of the miniature pig's hind limb
Postoperative care and euthanasia
The pigs were able to bear weight within 12 h and usually walked in 10 days. The animals were kept in individual boxes and were fed twice a day with food and water ad libitum.
At 6 months postsurgery, each animal was euthanized with an overdose of propofol and potassium chloride. The hind limbs were disarticulated at the hip.
Evaluation Methods
Magnetic resonance imaging
Before histological tests, the disarticulated limbs were prepared for MRI examination of the femoral condyles. A 7-tesla high-field MRI scanner (Magnetom 7 Tesla, Siemens Healthcare, Germany) with a head coil with 1 transmission channel and 32 receiving channels (Nova Medical, Inc.) was used for imaging at PISA Project (Faculdade de Medicina USP).
Images were collected from both knees of the 14 animals using two sequences. The first was based on 3D double echo steady state (3D-DESS), [repetition time (TR) = 12.2 ms, echo time (TE) = 4.1 ms, FA = 25°, voxel = 0.4 × 0.4 × 0.4 mm3, field of view (FoV) = 192 × 256 mm, slice thickness 0.4 mm, acquisition time 10:52 min] for morphological evaluation. The images from the 3D-DESS sequence were evaluated by two readers blinded to the treatment received (Fig. 3A, B).

A second image acquisition used a spin-echo sequence with multiecho to evaluate the cartilage composition based on the creation of a T2 map (TR = 10,000 ms, 18 echoes, TE = 9/18/27/336/45/54/63/72/81/90/99/108/117/126/135/144/153/162; voxel = 0.6 × 0.6 × 2.0 mm3, FoV = 93 × 229 mm, slice thickness 2.0 mm, acquisition time 18:44 min). The images were subjected to T2 mapping using the ImageJ software (National Institutes of Health).
Three consecutive cuts were selected from each knee covering the cartilage defect. Thereafter, two regions of interest (ROIs) were demarcated by two observers blinded to the treatment received. One ROI is the healthy tissue or native cartilage, and the other ROI is the region where the cartilage defect was made. After area selection, they verified whether there was a similarity between the T2 value of the native cartilage and the cartilage defect (Fig. 3C, D).
Gross and histopathological evaluation, and immunohistochemistry
After MRI, both knees were dissected and subjected to gross evaluation of the cartilage defects by visual inspection. Then, a 2.0 × 2.0 × 2.0 cm block around the defect was cut to allow evaluation of bone and subchondral zone.
The tissue block was fixed in 4% PFA, decalcified with ethylenediamine tetra-acetic acid (EDTA), processed for histological and immunohistochemical evaluation. Histological sections with a thickness of 4 μm were prepared and stained with hematoxylin and eosin. Two observers who were blinded to treatment assessed the quality of the repair.
For immunohistochemical staining, sections were deparaffined and rehydrated through graded ethanol and rinsed in distilled water. Next, antigenic sites recovery was performed by enzymatic digestion with pepsin for 30 min for collagens I and X and 1 h for collagen II. All enzymes were pipetted onto the sections and incubated at 37°C in a humid chamber.
Hydrogen peroxide, PBS, and methanol were applied for 10 min to block endogenous peroxidase present in red blood cells. Next, the primary specific antibodies for collagen types I (USBiological), II (Invitrogen), and X (eBioscience) with 1:50 dilution were applied to the sections, followed by overnight incubation at 4°C.
Subsequently, the sections were incubated with secondary antibodies for 30 min at 37°C in a humid chamber (IgG-PK6105 Vector Lab, collagen I and IgG-PK6102 Vector Lab, for collagens II and X). Diaminobenzidine (Sigma-Aldrich) as chromogen originated brown staining in immunoreactive structures.
Mechanical evaluation
To analyze the properties of the solid matrix, the mechanical characterization experiments used in this study were indentation test, maximum compressive test, and finite element (FE) analysis. 25
A height of 5 mm of bone was taken, and primary measurements of the osteochondral block were made, that is, thickness, weight, width, and height of the total sample set. 26
A minimum load was applied to ensure alignment and complete contact between the cartilage surface and the spherical tip indenter (2 mm diameter). The indentation test consisted of three cycles of strain–stress relaxation performed at a constant loading rate with a fixed displacement of 5% of the cartilage thickness (Fig. 4A). Subsequently, the maximum compression test was performed with a fixed displacement of 50% of the total height (Fig. 4B). 26

We created a FE model for the indentation test using the ANSYS R17.2 software. To simulate the osteochondral block, Young's modulus as determined in the mechanical analysis was inserted in the program, and the cartilage, characterized as a viscoelastic material, was modeled as a thin layer over the bone structure. The spherical indenter was created as a rigid material with a 2 mm diameter (Fig. 4C). 27
The sample size was defined based on similar preclinical studies with large animals and phases I and II studies in humans, as published in high impact factor journals.24,28 The demographic animal results as mean. The results of the different assessments of chondral repair are presented descriptively. It was described how each assessment can differentiate a typical chondral tissue from fibrocartilage.
Experimental Results
Demographic animal aspects
All 14 pigs survived during the study. The age of the animals at surgery averaged 11.2 months. The time between surgery and euthanasia averaged 6.4 months. The final animal weight at euthanasia had an average of 66.5 kg. There were no operative and postoperative complications. Regarding the age of the animals at surgery, the final weight, and the time of euthanasia, there was no significant difference between the experimental and control groups.
Characterization of MSC strains
The MSCs were characterized by flow cytometry, showing positive reactions for mesenchymal markers (CD29, CD44, CD73, CD105, CD90, and CD166) and negative reactions to hematopoietic (CD34 and CD45) and endothelial markers (CD31). Moreover, MSCs from both sources differentiated into osteogenic, chondrogenic, and adipogenic strains (Fig. 5).

Example of MSCs differentiation:
Magnetic resonance imaging
The morphological evaluation of cartilage repair showed that cartilage repair in those subjected to treatment with SMSCs and DPSCs improved compared with control groups.
The evaluation of cartilage composition by T2 mapping showed similarity between the T2 average value of cartilage defect ROI and native cartilage ROI in almost all samples of the group treated with MSCs. In the control group, the T2 average values in the cartilage defect region were different from the T2 average value in the native cartilage ROI for the majority of evaluated samples (Fig. 3C, D). The outcomes from MRI were similar between SMSCs and DPSCs experimental groups.
Gross and histopathological evaluation and immunohistochemistry
Untreated lesions showed only partial tissue coverage (Fig. 6A) or no evidence for repair (Fig. 6C). The cartilage lesion seeded with TEC loaded with MSCs from both sources exhibited totally or primarily coverage of the defect (Fig. 6B, D).
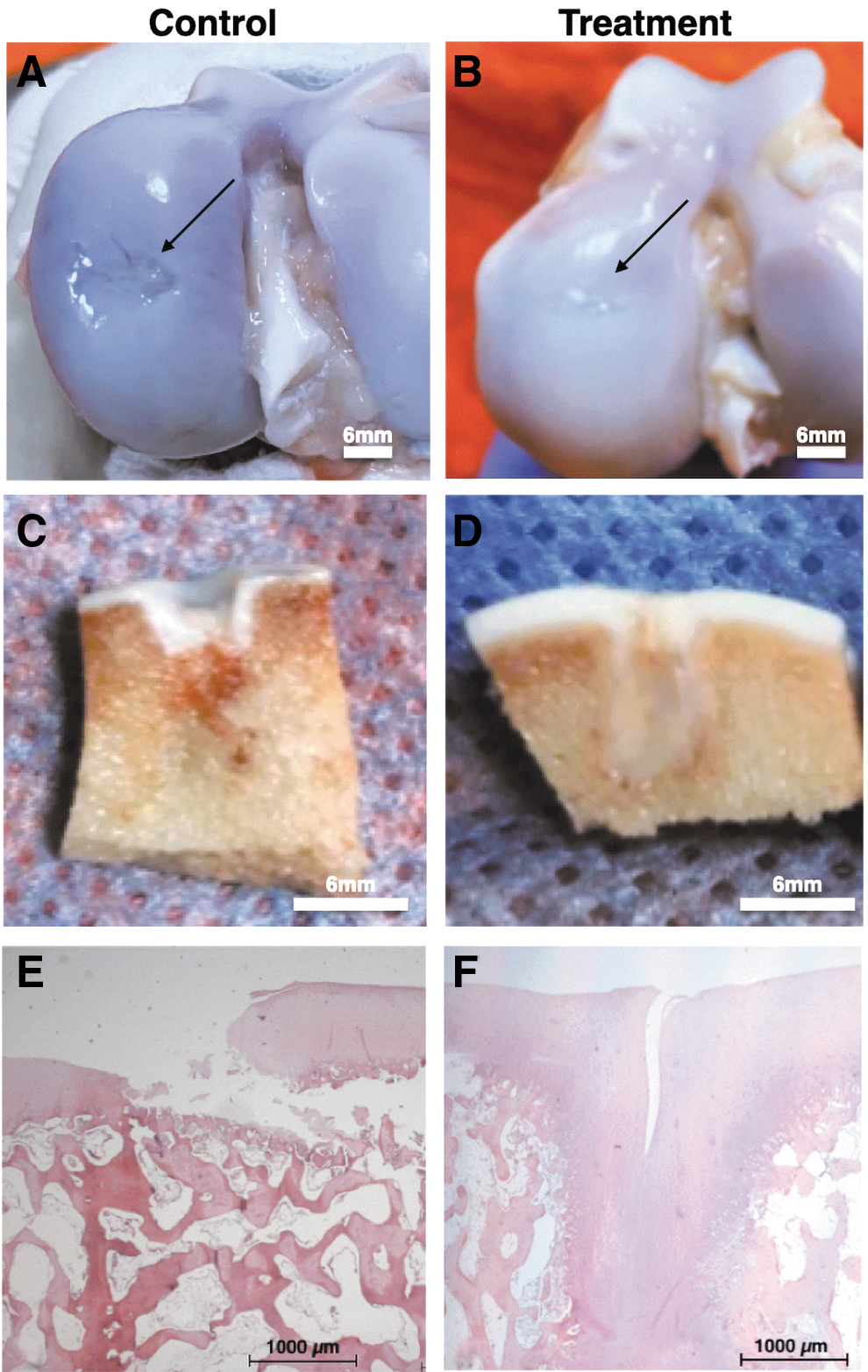
Macroscopic examination of standard samples with cartilage defect in the control group
Histologically, the chondral defects of nontreatment group showed loss of cartilage and destruction of subchondral bone (Fig. 6E). In contrast, when treated with a TEC, the defects were filled with repair tissue exhibiting a restored surface (with fissures in some samples) and good integration to the adjacent cartilage and subchondral bone. In addition, in some regions, the subchondral bone was undergoing a remodeling process, forming a tissue with hyaline-like cartilage (Fig. 6F).
The immunohistochemical staining for collagen II in experimental groups was evident in the implant and the adjacent native cartilage tissue, indicating successful integration. Even specimens that showed partial filling or fissure in the treated chondral defect exhibited collagen II expression comparable with adjacent native cartilage (Fig. 7A). The collagen II staining was irregular in most control samples (Fig. 7B). The expression of type X (Fig. 7C) and type I collagen was observed in experimental groups. In some control group samples, irregular tissue formed on the chondral defect showed expression of collagen I (Fig. 7D).

Mechanical evaluation
Young's modulus was determined based on the second ramp of the stress-relaxation indentation test, as this step presents a more linear behavior and the lowest amount of error. The elasticity module depends on the straight slope value, which is associated with the cartilage elasticity (N/mm) (Fig. 8A).

Biomechanical analysis of one sample.
In a preliminary analysis, the samples presented different cartilage thickness, directly affecting the indentation response and Young's modulus. However, it is possible to observe in all results the hysteresis phenomenon when applying the three cycles of strain–stress relaxation, evidencing the viscoelastic property of the articular cartilage.
Discussion
This article presents different evaluation methods for an innovative technology for cartilage therapy, using a preclinical large animal model. In 2015, Shimomura et al. reported about the development of scaffold-free approaches for cartilage treatment with SMSCs. 29 The current research is the first to use DPSCs to create a 3D structure that does not need a scaffold.
The effectiveness of the TEC with MSCs for cartilage treatment was shown by Ando et al.7,30 Furthermore, because it does not need an artificial framework, it increases safety and reduces the costs of treating chondral lesions by cell therapy.
The TEC is created from MSCs cultured in an appropriate cell concentration with a specific amount of ascorbic acid, which has the ability to enhance ECM production, improve the expression of cellular markers, and increase collagen synthesis significantly. 29 Also, Asc-2P can enhance the expression of genes related to positive telomerase activity, which is associated with cellular longevity. 31
Regarding the animal model, the Brazilian miniature pig BR1 presented itself as a preclinical large animal model suitable for the use of human MSCs. 32 Previous studies have shown that the mini-pig has no immunological reaction due to incompatibility when receiving human MSCs to treat chondral lesions in the knee and other joints.33,34 It shows that this porcine model is safe and adequate. 32
This study evaluated the repair of articular cartilage using a noninvasive imaging method, of which the results can be translated to humans. MRI is the primary noninvasive tool to assess the structure of cartilage repair tissue. Similar to our results, Goebel et al. 35 indicated that the MRI assessment of osteochondral repair in animal models correlates with histological findings. MRI is a technology that allows the necessary resolution standards for a good assessment of chondral tissue.36,37 Also, it allows a morphological and compositional evaluation of chondral repair.
For the evaluation of knee cartilage morphology with MRI, a 3D-DESS sequence was used, which is described as more effective in the diagnosis of cartilage injury compared with the Spin Eco sequence. 38 Our study observed that it is possible to adequately assess the morphology of cartilage repair using the DESS sequence, which enabled a more precise and accurate assessment of cartilage volume and thickness at a reasonable acquisition times. 39
MRI can also be used to evaluate the composition of cartilage repair through T2 mapping. This technique can evaluate the composition or quality of the cartilage tissue present, because it is sensitive to specific changes in the chemical composition and structure of the cartilage even before profound morphological changes occur.36,40–43 The T2 relaxation time variations in the articular cartilage reflect changes in the orientation of collagen fibers and, consequently, in the water concentration, which interacts with these macromolecules in the ECM, and its values can be represented by a color or gray-scale coded map.36,43
Similar mean T2 values between cartilage defect and native cartilage ROIs in experimental groups suggested a compositional similarity between the native cartilage and the tissue formed by TEC after 6 months. Chen et al. 44 evaluated a tissue-engineered mosaicoplasty using T2 mapping and found similar results. Furthermore, the authors observed clear histological correlation with MRI findings. 44
The histological evaluation made it possible to estimate the intrinsic characteristics of the new tissue formed. A correlation analysis allows studying the specimen histological properties and the imaging correspondence. In the same manner, mechanical properties can be correlated with histological findings.
As in our study, Ando et al. 30 showed from histological and macroscopic evaluation a significant improvement in the coverage of a cartilage defect in animals treated with TEC compared with animals in which only a cartilage defect was made. 30
Recently, Shimomura et al. 45 took a step forward and carried out the first pilot study in humans using bioengineered cells from SMSCs. Thorough evaluation by arthroscopy, histology, and resonance imaging concluded that the TEC could be used to repair articular cartilage using a simple implantation procedure without sutures.
Our histological descriptive evaluation of the cases suggests that the complex of MSCs and ECM is responsible for more significant and better coverage of the cartilage defect after 6 months of implantation.
We also investigated the biomechanical behavior of the newly formed tissue. Despite having several parameters that can affect the mechanical test response, such as cartilage stiffness and indenter diameter, it is possible to observe the viscoelastic property of the cartilage by determining its Young's modulus. Biomechanical characteristics are related to the integrity of articular cartilage, and any difference in these parameters might indicate alterations in the cartilage structure. 46
This study poses some limitations. First, all the results of the different evaluations were not grouped and statistically compared. The focus of this article was to present the detailed methodology of the different assessment techniques for cartilage repair in a preclinical study. Second, the sample size was too small to compare the findings of all performed assessments. Furthermore, the descriptive results showed that the evaluations are viable and qualified for differentiating good quality chondral repair from inadequate repair tissue. Further studies should focus on the outcomes of each evaluation and present potential correlations between them.
Conclusion
The applied assessment methods were feasible and capable to properly evaluate articular cartilage restoration in chondral defects filled with TEC containing stromal cells after 6 months of follow-up in a large animal model.
Footnotes
Authors' Contributions
J.P.C.S. and T.L.F. took responsibility for the integrity of the study from conception and design to completion. The article was drafted and critically revised by J.P.C.S., R.R.F., I.P.A., C.C.G.P., D.F.B., C.A.-N., R.B., M.J.S.M., I.A.C., A.J.H., and T.L.F.
Acknowledgments
The authors thank Isabella Zaia, Bruno Gregnanin Pedron and Khalil Taverna Chaim for their support.
Disclosure Statement
The authors declare that they researched in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This study was supported by Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP–Process 2017/05774-5), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES–Process 88881.171651/2018- 01), grant from the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine and the Orthopaedic Research and Education Foundation (ISAKOS Osteoarthritis Grant −2018), Sírio-Libanês Hospital and IOT HC-FMUSP (Hospital das Clínicas, Faculdade de Medicina da USP).