
Abstract
Regenerative medicine approaches to restore the mandibular condyle of the temporomandibular joint (TMJ) may fill an unmet patient need. In this study, a method to implant an acellular regenerative TMJ prosthesis was developed for orthotopic implantation in a pilot goat study. The scaffold incorporated a porous, polycaprolactone-hydroxyapatite (PCL-HAp, 20wt% HAp) 3D printed condyle with a cartilage-matrix-containing hydrogel. A series of material characterizations was used to determine the structure, fluid transport, and mechanical properties of 3D printed PCL-HAp. To promote marrow uptake for cell seeding, a scaffold pore size of 152 ± 68 μm resulted in a whole blood transport initial velocity of 3.7 ± 1.2 mm·s−1 transported to the full 1 cm height. The Young's modulus of PCL was increased by 67% with the addition of HAp, resulting in a stiffness of 269 ± 20 MPa for etched PCL-HAp. In addition, the bending modulus increased by 2.06-fold with the addition of HAp to 470 MPa for PCL-HAp. The prosthesis design with an integrated hydrogel was compared with unoperated contralateral control and no-hydrogel group in a goat model for 6 months. A guide was used to make the condylectomy cut, and the TMJ disc was preserved. MicroCT assessment of bone suggested variable tissue responses with some regions of bone growth and loss, although more loss may have been exhibited by the hydrogel group than the no-hydrogel group. A benchtop load transmission test suggested that the prosthesis was not shielding load to the underlying bone. Although variable, signs of neocartilage formation were exhibited by Alcian blue and collagen II staining on the anterior, functional surface of the condyle. Overall, this study demonstrated signs of functional TMJ restoration with an acellular prosthesis. There were apparent limitations to continuous, reproducible bone formation, and stratified zonal cartilage regeneration. Future work may refine the prosthesis design for a regenerative TMJ prosthesis amenable to clinical translation.
Impact statement
The impact of this study is its translational approach to temporomandibular joint (TMJ) tissue engineering. Specifically, inspiration from the only FDA-approved custom TMJ prosthesis (TMJ Concepts/Stryker) was uniquely infused into an acellular design for a biphasic device to be an “off-the-shelf” approach to regenerate the mandibular condyle. Such a prosthesis would offer an alternative for TMJ patients with condylar fractures or with pediatric reconstruction needs, where current alloplastic devices may be limited. The current study was a pilot study, and helped to identify limitations in the design and to thus inform future work.
Introduction
The temporomandibular joint (TMJ) is essential to many daily life functions such as speaking, laughing, mastication, and upper-airway support. Although TMJ disease prevalence is high, affecting up to 12% of the overall population,1,2 treatment with a TMJ total joint prosthesis is indicated only for a select patient population of the ∼1 in 800 who have open surgery.3,4 Inflammatory TMJ arthritis, recurrent fibrous and/or bony ankylosis, failed autogenous or alloplastic reconstruction, resorption, and trauma are among indications for a TMJ prosthesis.5–7 Current TMJ prosthesis biomaterials cannot accommodate pediatric patient growth, and may not be appropriate for patients with metal hypersensitivities.8,9 Therefore, regenerative medicine approaches are actively being investigated to develop a prosthesis capable of mandibular condylar tissue regeneration.10,11
TMJ animal models range from small, such as mouse or rabbit, to large, such as goat or Yucatan minipig.12–16 Goat TMJ disc attachments to the condyle are similar to human disc attachments with medial and lateral collateral ligaments. 17 Zhu et al. 18 examined coronoid process donor tissue to reconstruct the mandibular condyle of goats. The Almarza group has performed a range of studies to establish baseline knowledge of the goat's TMJ tissue structures and behaviors.15,19
Both prevascularized and dual perfusion bioreactor-incubation regenerative medicine approaches have recently been pursued for TMJ tissue engineering. Hollister and colleagues 20 implanted a 3D printed mandibular condyle scaffold coated with bone morphogenetic protein (BMP)-2 into the temporalis muscle of Yucatan mini-pigs. After cellular infiltration and vascularization were established, a horizontal condylectomy was performed and the scaffold was fixed in place. After 6 months, computed tomography (CT) scans and histology suggested vascularization, bone infiltration, and signs of neocartilage formation in the porous condyle scaffold. Chen et al. 14 pre-cultured autologous stem cells on subject-specific decellularized bone matrix geometries for 6 weeks before implantation.
The bioreactor-derived cartilage-bone construct regenerated tissues that more closely resembled control cartilage and subchondral bone tissues than either bone-only or acellular grafts. Previously, our group employed an acellular approach with a gradient of growth factors in a cylindrical, microsphere-based scaffold to regenerate focal mandibular condyle defects in rabbits. 21 Research to date has reported signs of mandibular condyle bone and cartilage regeneration with a seeded scaffold approach, 22 yet a practical approach that can be rapidly produced for off-the-shelf immediate implantation for successful regeneration of continuous bone and cartilage tissues remains elusive.
A resorbable scaffold that can support loads and regenerate mature, stratified cartilage on the articulating surface of regenerated bone leaving no trace of the implanted material remains a common limitation for TMJ tissue engineering.14,18,23 Significant bone regeneration has been documented with porous polycaprolactone (PCL) and hydroxyapatite (HAp) scaffolds. 24 In this study, a biphasic scaffold prosthesis was assembled from two parts: (1) an anatomically correct 3D printed bone regeneration structure comprising porous polycaprolactone and 20% w/w hydroxyapatite (PCL-HAp) and (2) a potentially chondrogenic hydrogel comprising photocrosslinkable, 4% w/v pentenoate-modified hyaluronic acid (PHA), 20% w/v polyethylene glycol (PEGDA), and 15% w/v devitalized cartilage (DVC).25–27
Chondrogenesis and mechanical properties of the PHA-PEGDA-DVC hydrogel were previously reported by our group. 28 The 3D printed PCL-HAp was characterized for structure, mechanical properties, and biofluid transport. A Spanish cross goat model with an approximately human-sized TMJ was used to evaluate tissue regeneration in a pilot study over 6 months of orthotopic implantation. 15 PCL-HAp only, and a biphasic PCL-HAp + PHA-PEGDA-DVC hydrogel-integrated condylar prosthesis were evaluated against native tissues from the contralateral condyle. The purpose of the study was to characterize an acellular scaffold and regenerate bone throughout the condylar head with cartilage regeneration on the condyle's articulating surface.
Methods
Three-dimensional printing biphasic prosthesis and cartilage-matrix hydrogel synthesis
Polycaprolactone (PCL, 50 kDa; Polysciences, Inc., Warrington, PA) filament with 20% w/w hydroxyapatite powder (HAp; Sigma-Aldrich, St. Louis, MO) was made using a filament extruder (Noztek Touch, Shoreham, West Sussex, or Filabot Ex6, Barre, VT). PCL and HAp were mixed with the desired ratio and planetary ball-milled for 6 h (PQ,N2 Across International, Livingston, NJ), and extruded at 135°C at a rate of 30 rpm. Filament was fed into a Flashforge Creator Pro printer (Zhejiang, P.R. China) for 3D printing at 135°C.
For 3-point bend testing, parts were printed on a Cura Lulzbot Taz 6 3D printer (Lulzbot, Fargo, ND) with the same parameter settings as the Flashforge. A patient-fitted prosthesis was digitally designed using CT scans of each goat (16-slice Philips CT, Amsterdam, Netherlands) with a microporous architecture inside the condylar head (Fig. 1A). Three-dimensional printed PCL-HAp was then submersed in 5 M NaOH for 30 min, washed 3 × in DI water, and sterilized overnight using ethylene oxide. Two different prosthesis groups were made either without a hydrogel (i.e., PCL-HAp only), or with PHA-PEGDA-DVC hydrogel syringed onto the surface and into mechanical integration features.
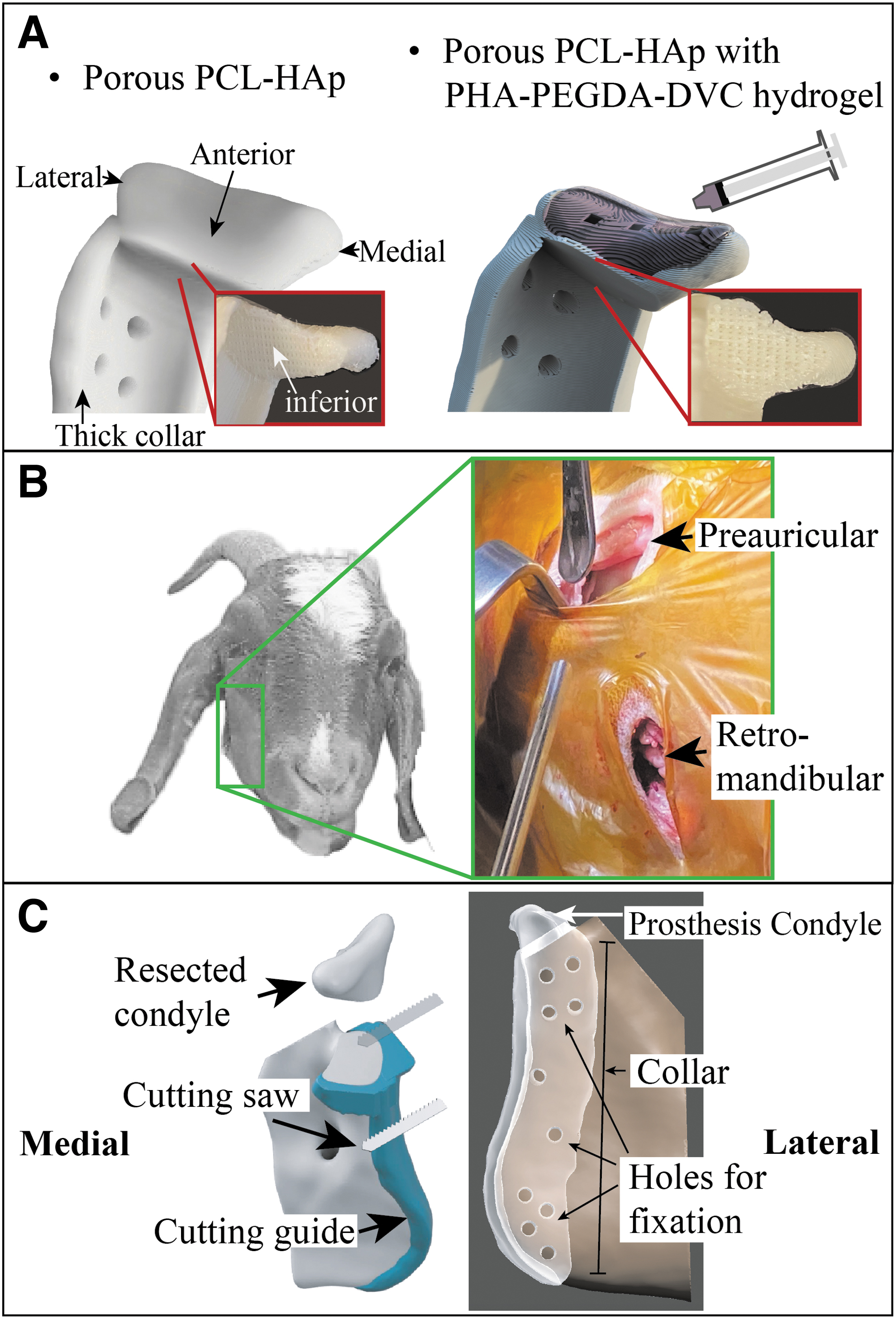
Schematic diagram of the prosthesis and surgical implantation.
The hydrogel was synthesized as previously described. 28 Briefly, 1.5 MDa hyaluronic acid (HA; Lifecore Biomedical, Chaska, MN) was dissolved and functionalized with 4-dimethylamino pyridine and 4-pentenoic anhydride added at 0.25 g per g HA and 10-fold molar excess, respectively (Sigma-Aldrich). Functionalized PHA solution was precipitated using acetone, purified, and frozen, before lyophilization on a FreeZone 6 Plus lyophilizer (Labconco, Kansas City, MO) and stored at −20°C.
NMR characterization of PHA was performed as previously described 29 with a 64% functionalization of the disaccharide repeat units.
Porcine knees (Hampshire and Berkshire, female, 1-year old, 180–220 kg) were obtained from a local abattoir to prepare DVC powder from cartilage as previously described. 26 The DVC was lyophilized and stored at −20°C.
Hydrogels were prepared with 4% PHA, 20% PEGDA, and 15% w/v DVC as previously described. 28 The photoinitiator, 2.2 mM lithium phenyl-2,4,6-trimethylbenzoylphosphinate (LAP; 98%; TCL0290-1G) (TCI America, Portland, OR), was prepared in phosphate-buffered saline (PBS; Sigma-Aldrich). Once dissolved, the crosslinker dithiothreitol (Sigma-Aldrich) was added to ensure a 1:1 thiol:ene molar ratio for all composites. Precursor mixtures were spatulated for at least 15 min and then syringed onto the 3D printed scaffold bedside before photocrosslinking for 10 min (365 nm light at 1280 μW · cm−2, EA-160; Spectroline, Westbury, NY).
CT scans from each goat were registered and implants designed following consultation with TMJ concepts. Each scan was segmented for the condyle and ramus using Seg3D (University of Utah SCI Institute). The part was enlarged such that a 0.165 mm offset resulted between prosthesis and bone. A condyle cutting plane was derived from points in the superior external auditory meatus and inferior orbit. The implant collar was extruded from the ramus surface and combined with the resected condyle in Meshmixer (San Rafael, CA). All screw holes were 0.094.”
Surgical implantation
All experiments were performed with the approval of the Institutional Animal Care and Use Committee. After a surgical plane of anesthesia was achieved (Supplementary Data S1), two incisions were performed to gain access to the bone, and permit both the guided condylectomy and the condylar implants insertion (Fig. 1B). Initially, a preauricular incision was performed 1 cm below the zygomatic arch, parallel to the posterior border of the mandible with ∼2.5 cm of extension. After that, another 2.5 cm long retromandibular incision was performed in a curvilinear manner, following the mandibular angle contour at the level of the mandibular inferior border. The two incisions were separated by a length of ∼2 cm.
After reaching the bone, subperiosteal dissection was accomplished to expose the medial and the lateral aspects of the ramus and condyle, with attention to preserve the disc. After adequate level of dissection was obtained, a custom-made cutting guide was inserted through the retromandibular incision and fixed to the ramus with four titanium screws (KLS Martin, Jacksonville, FL), thus providing a planar guide for condyle resection, performed using a Bien-air reciprocating saw (Bien-air Dental, Bienne, Switzerland). The condyle was then disinserted and removed, taking care to preserve the disc, and the cutting guide was replaced by the implant, which was fixed in place with eight screws (Fig. 1C).
Load transmission to underlying jaw
To estimate physical forces transmitted to the underlying bone, a uniaxial mechanical testing setup was used to evaluate loads in two locations: (1) applied to the surface of the condyle, FApplied, and (2) FTransmitted measured between the prosthesis condyle and underlying jaw structure with a FlexiForce pressure sensor (Barneveld, Netherlands) (Fig. 2). The % load transmitted was calculated using the following equation.

Illustration of the testing setup for load transmission. The upper half of the prosthesis was fixed to a 3D printed ramus-shaped base. A 5 lbf load was applied to the condyle and the transmitted load was measured with a force-sensitive resistor positioned between the condyle and the base. Following each sample, the force sensitive resistor was calibrated by repeating the test with an unconstrained condyle.
Experiment
Animals
Six Spanish cross female goats (initial weight: 33 ± 5 kg, final weight: 52 ± 13 kg, and age: 3–5 years) were used in this study. All goats were purchased and boarded at the University of Oklahoma Health Sciences Center Division of Comparative Medicine. Goats were assigned to two pilot groups for 6-month implantation periods with either no-hydrogel or a hydrogel-integrated prosthesis.
Structural characterization of 3D printed prosthesis
Three dimensional printed PCL-HAp specimens were sputter coated with gold on a Hummer VI (Anatech Ltd., Battlecreek, MI), and examined under a field emission scanning electron microscope (SEM; Zeiss NEON 40 EsB, Stuttgart, Germany) with 5 kV acceleration voltage. Furthermore, energy-dispersive X-ray spectroscopy (EDS) was used to identify elemental structure.
Uniaxial tensile testing
Uniaxial testing followed American Society for Testing and Materials (ASTM) standard #D1708. Briefly, dog bone shapes with a 5 × 3 mm cross-section, and 22 mm gauge length were extended uniaxially at a rate of 1 mm·min−1 in a TestResources uniaxial tester (Shakopee, MN). Three groups were evaluated for tensile properties: (1) PCL, (2) PCL-HAp, and (3) etched PCL (ePCL-HAp). For ePCL-HAp, the composite was submersed in 5 M sodium hydroxide (30 min) to improve hydrophilicity and washed thrice in DI water before testing. Linear regression from 5% to 30% of the ultimate strain was used to obtain the Young's modulus. The ultimate stress and strain were determined from the global maximum stress, and the yield stress and strain were determined using the 0.2% strain offset. n = 5–6.
Three-point bend testing
PCL, PCL-HAp, and PCL-HAp beams were 3D printed (70 × 15 × 3 mm) and tested for flexural stiffness following ASTM standard #D790. A span length of 48 mm was set on a 3-point bending fitting for the TestResources machine. Beams were deflected at a flexural strain rate of 1%·min−1 to 5% flexural strain. The flexural modulus was determined from the slope of the 1–2.5% flexural strain range. Beams were printed on the Cura TAZ 6 Lulzbot 3D printer. n = 6.
Load transmission test
PCL-HAp prostheses with either a thick, 5 mm collar used in the current animal study, or a thin, 3 mm collar prosthesis were tested for load transmission. Prosthesis fixation was achieved using the top four screw points where only the top half of the prosthesis with the condyle was printed and tested. A load was applied at a rate of 10 lb·min−1 to 5 lbs. and held for 1 min. Transmitted load was measured on a FlexiForce load sensor (Tekscan, Norwood, MA), preconditioned with a 70 lbf load for 5 min. After each data-collection run, a calibration run was performed with an unconstrained condyle. A power law equation was fit to the calibration data to convert signal to transmitted load from the FlexiForce sensor. n = 4.
Biofluid transport through capillary rise
Scaffolds from either PCL-HAp or ePCL-HAp were printed to assess whole blood capillary rise through the porous architecture. A 10 × 10 × 3 mm scaffold was printed with a zig-zag pattern and 0.60, 0.85, and 1.10 mm line distances such that the actual cross-sectional pore sizes were 152 ± 68, 360 ± 140, and 570 ± 240 μm for the 150, 350, and 550 μm groups, respectively. A bath with whole goat blood (Innovative research, Novi, MI) was raised to contact the scaffold. Imaging was captured at 60 fps and a custom MATLAB script was used to process each image and calculate an ensemble average of the blood height. The initial velocity for each sample was calculated from a linear fit to the initial 2s of data. n = 6–7.
Bone assessment with Micro-CT
At the 6-month completion of the study, each implant was resected en bloc along with the TMJ disc and fossa. The specimens were then scanned with a micro-CT system set to 70 kV, and 200 μA (Quantum FX, Perkin Elmer Co, Waltham, MA) with a 30 mm field of view. Each scan was segmented using Seg3D (University of Utah SCI Institute) for implant, screw, and bone materials. A custom MATLAB script was used to register each object in space for consistent viewing perspectives. Renderings of the segmented and registered objects were performed using Autodesk Fusion 360 (San Francisco, CA).
Soft tissue assessment with histology and immunohistochemistry
Resected tissue specimens were fixed in 10% neutral buffered formalin (VWR, Radnor, PA), dissected, and imaged for gross morphology. Boney tissues were decalcified in newcomer supply (Newcomer Supply, Fisher, Hampton, NH) for at least 4 months before sectioning with a blade. All tissues were dehydrated in 70% ethanol (VWR) overnight and paraffin embedded for slide mounting. Slices 4-μm thick were mounted and stained with hematoxylin and eosin (H&E), or Alcian blue on a ST5020 workstation (Leica, Wetzlar, Germany).
Immunostaining was performed with a Leica BOND III BOND RX automatic system with a 12-h antigen-retrieval step at 60°C at pH 9.0 to prevent bone delamination. Soft tissue specimen antigen retrieval was performed at 100°C for 20 min at pH 6.0. For collagen II and CD4 immunostaining, rabbit primary antibodies were purchased from Abcam (#ab34712, Cambridge, United Kingdom) and Novus (#NBP1-19371SS, St Louis, MO), respectively. For secondary antibody, post-primary IgG-linker reagent was used with 3,3′-diaminobenzidine tetrahydrochloride (DAB) as chromogen and counterstained with hematoxylin. Antibody-specific positive and negative control (omission of primary antibody) were parallel stained. Additional positive control tissue for CD4 was obtained from goat submandibular lymph node.
TMJ disc gross morphology scoring
TMJ discs were randomly sorted and scored by four oral surgery clinicians. A scoring system was modified from van den Borne et al. 30 with a range from 0 (poor) to 4 (excellent).
Statistical analyses
Statistical analyses were performed with one-way ANOVA with Tukey's post hoc test, or a one-way t-test for two groups. Significance was defined when α = 0.05. All data were mean ± standard deviation.
Experimental Results
Animals
Five goats were euthanized after 6 months and one euthanized early (4 months) due to conditions unrelated to the study, that is, a caseous lymphadenitis caused by a Corynebacterium pseudotuberculosis infection likely contracted before boarding (Supplementary Data S1). Results were thus reported for three no-hydrogel and two hydrogel group specimens. All animals exhibited weight gain averaging 18 ± 10 lbs. over the study duration and resumed normal jaw function within 2 h of surgery.
Structural and mechanical properties of 3D printed prosthesis
EDS exhibited a homogeneous distribution of calcium and phosphorous throughout 3D printed PCL-HAp (Fig. 3).
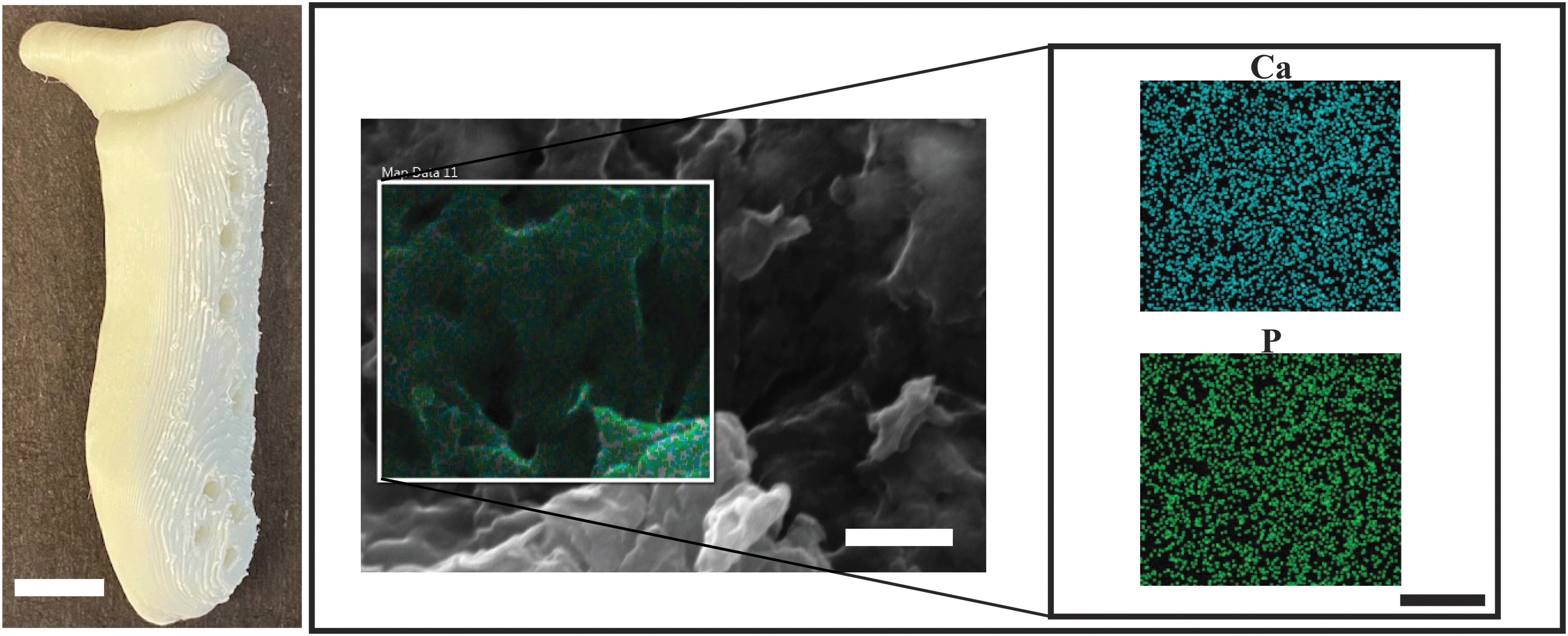
Calcium and phosphorous were distributed throughout the 3D printed PCL-HAp. Scanning electron microscopy (SEM) of 3D printed PCL-HAp using energy-dispersive x-ray spectroscopy exhibited homogeneously distributed calcium and phosphorous. Scale bar for left-hand image of prosthesis was 10 mm. Scale bars for SEM and EDS were 1 μm. EDS, energy-dispersive X-ray spectroscopy; Ca, calcium; P, phosphorus.
Young's moduli increased by 67% with the addition of HAp relative to PCL PCL-Hap, with no difference after etching (Fig. 4C). Strain energies were 1.8-fold higher in PCL than PCL-HAp, and not different between PCL-HAp and ePCL-HAp (Fig. 4D). Ultimate tensile stresses and yield stresses did not exhibit differences among groups (Fig. 4E, G). Ultimate strains reduced by 0.6-fold from PCL to PCL-HAp, and ePCL-HAp (Fig. 4F). Furthermore, yield strains were 1.5-fold higher in PCL than in PCL-HAp and ePCL-HAp (Fig. 4H).
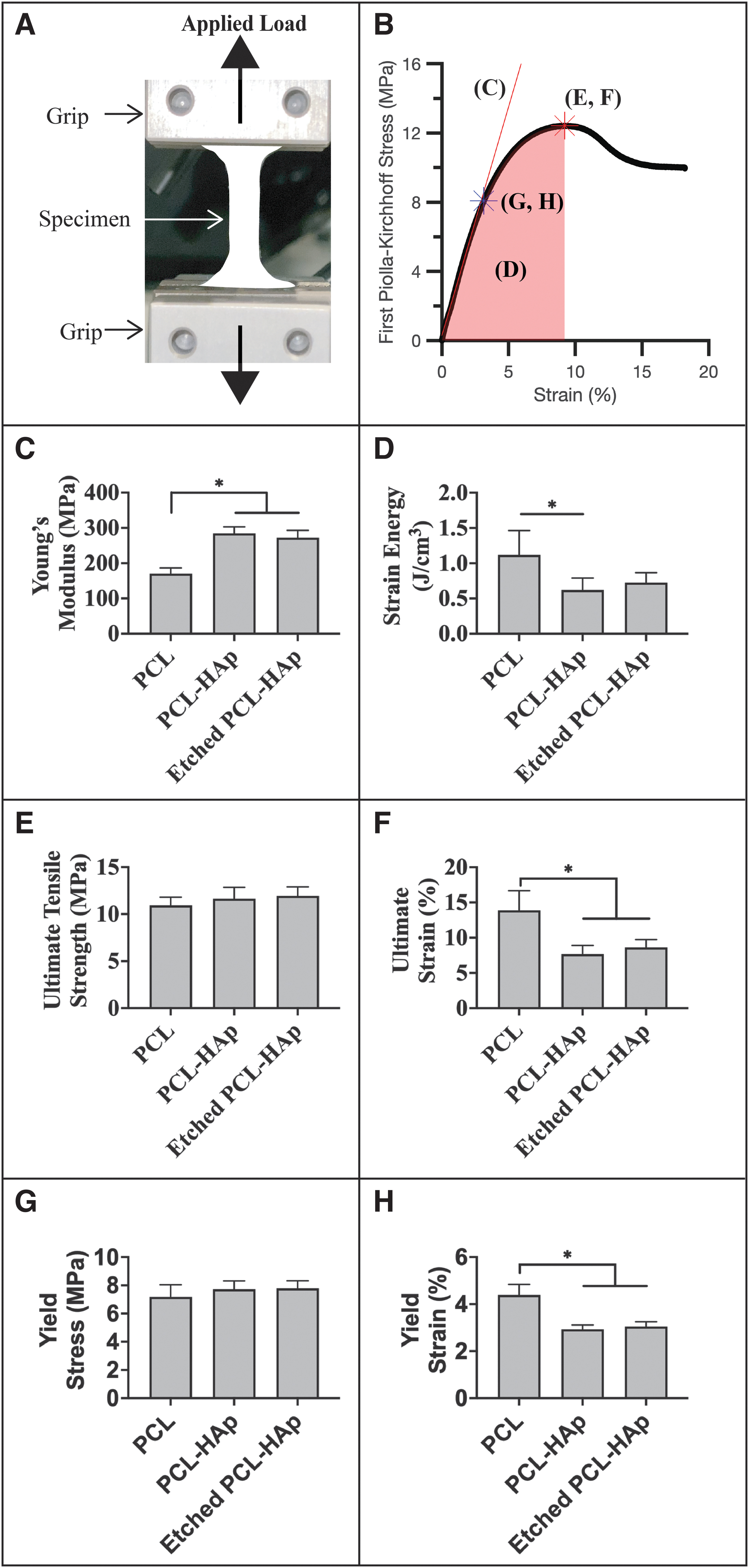
Uniaxial tension of 3D printed PCL-HAp. Adding HAp significantly enhanced PCL's mechanical performance.
Flexural stiffness was 2.06-fold higher in PCL-HAp than the PCL group, but did not change after etching (Fig. 5).
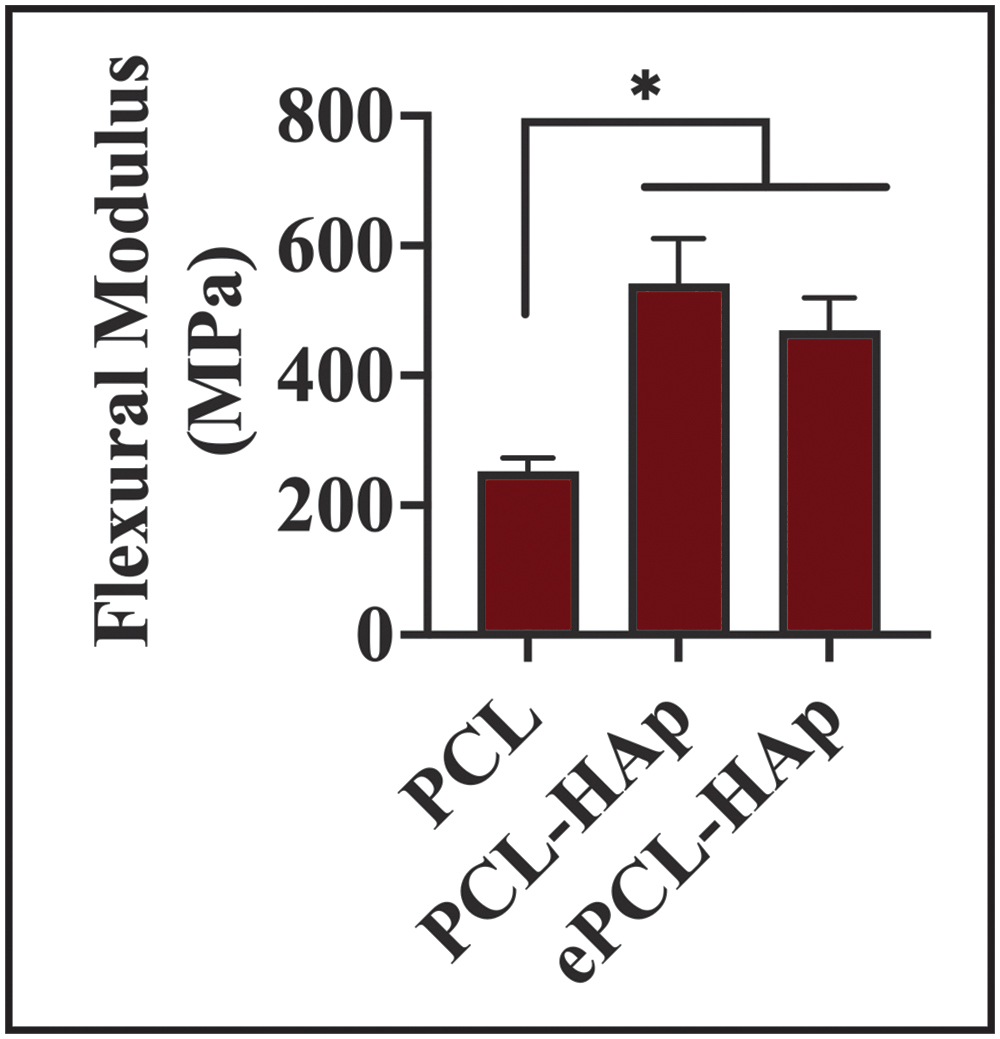
Three-point bend test of 3D printed composites following ASTM D790. The addition of HAp increased PCL flexural stiffness, but the reduction in stiffness after NaOH etching (ePCL-HAp) was not different from nonetched PCL-HAp. n = 6–7. *p < 0.05. All data are mean ± standard deviation. HAp was 20 wt%.
Load transmission to underlying bone grip was ∼12% higher for thin-collared implants than for thick-collared implants, which were used in this study's pilot animal study (Fig. 6).
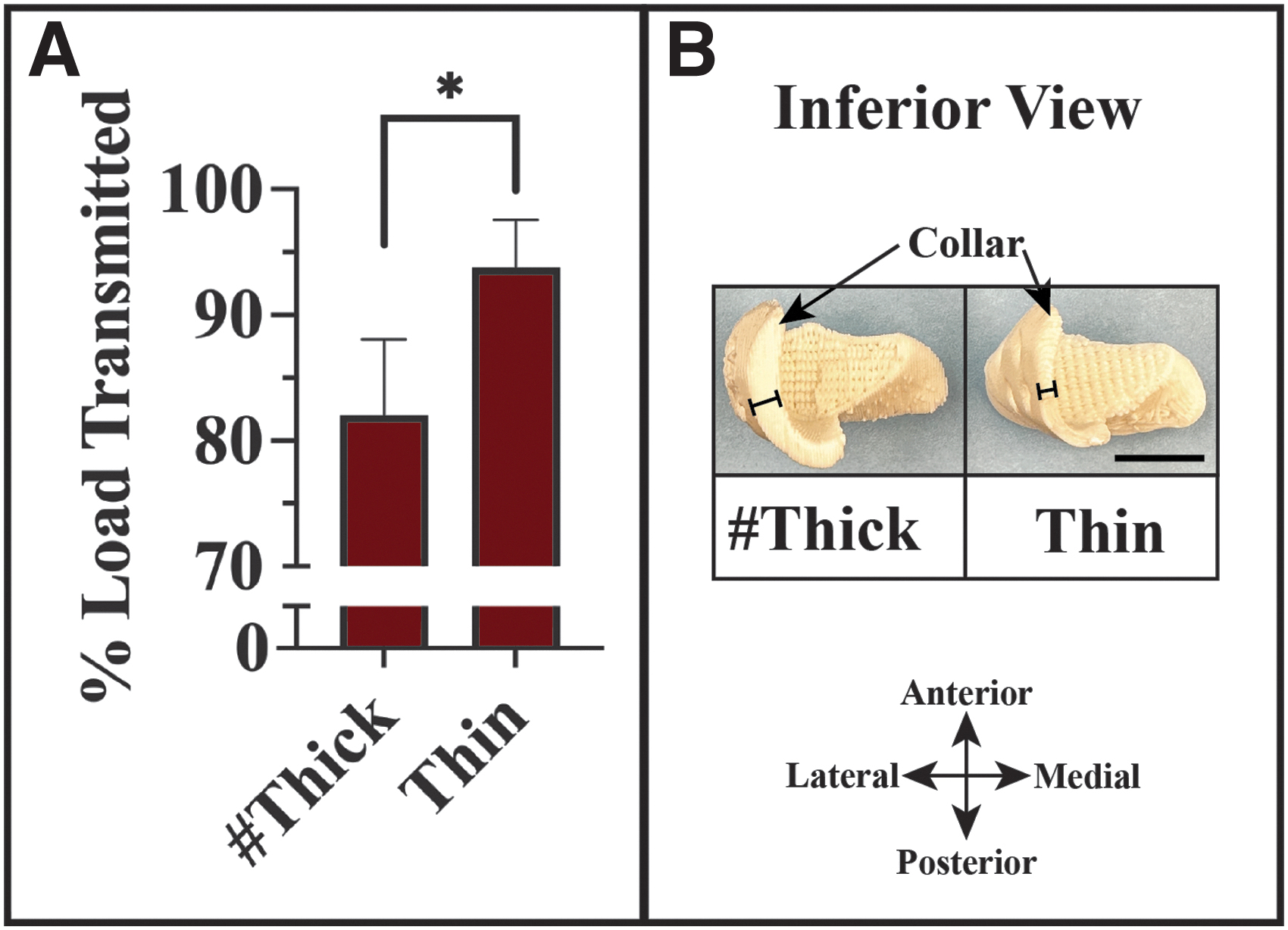
Evaluation of the load transmitted through the condyle to the underlying bone geometry.
Porous architecture supports whole blood infiltration
For all the NaOH-etched scaffolds, capillary rise of whole blood reached the full 1-cm height within 1 min (Fig. 7A). Small, 152 ± 68 μm pore length scaffolds exhibited an initial velocity of 3.7 ± 1.2 mm·s−1, and increasing pore sizes reduced the initial velocities by 31% and 77% for 360 ± 140 and 570 ± 240 μm, respectively (Fig. 7B). Differences in initial velocity were not exhibited by the etched 150 and 350 μm groups. Nonetched scaffolds exhibited negligible capillary rise (Fig. 7B).
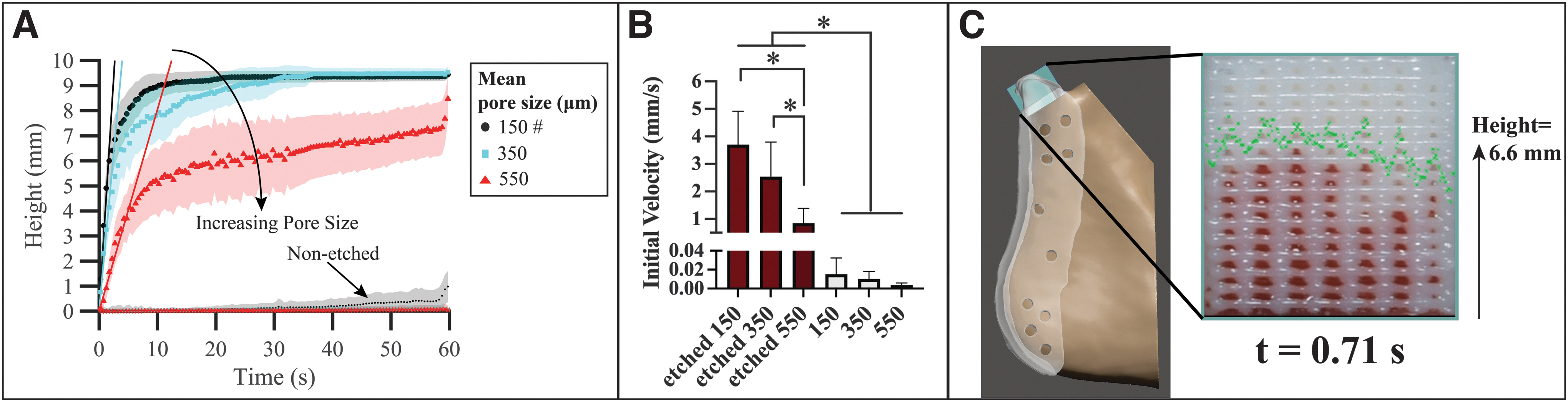
Three-dimensional printed PCL-HAp composite scaffold exhibited capillary rise of whole blood.
Bone growth and resorption surrounding condyle
Bone growth and resorption exhibited by micro-CT-derived renderings were highly variable from specimen to specimen. Resorption was focused to regions directly under the prosthesis condyle and a gap was left between the prosthesis collar and bone (Fig. 8). An approximate measurement made on MicroCT images suggested the depth of resorption was lower in the no-hydrogel group (A: 6.0, B: 5.6, and C: 2.6 mm) than the hydrogel group with lengths of D: 7.2 and E: 9.2 mm. Bone growth surrounding the implanted condyle was localized to both the medial and posterior regions of the condyle. In all cases, except B, soft tissues enveloped the condyle.

Assessment of bone with MicroCT data prepared from each subject 6 months after implantation. Gross images were captured from the tissue's superior viewpoint with the camera pointed from the superior perspective. Renderings for each case were displayed with the view direction listed across the top row (superior, anterior, posterior, medial, and lateral). In each case, bone growth was exhibited around the prosthesis condyle, but not inside the condyle's porous region. Bone resorption was observed in all cases with more pronounced bone loss in groups with the hydrogel (D, and E). The control group is shown as the mirror image of the left condyle from subject C to facilitate visual comparison with the experimental group right condyles. In the CT images, the prosthesis, ramus bone, and fossa bone were labeled as #, @, and ^, respectively. The prosthesis was displayed as white, and bone as brown in the renderings. Dashed line in ‘superior’ column represents plane of CT image in right-most column. The approximate distance between the prosthesis collar and bone was shown with a red line superimposed on the CT sections. The approximate lengths were 6.0, 5.6, and 2.6 mm for nonhydrogel groups A, B, and C, and 7.2, 9.2 mm for groups D and E, respectively. MicroCT imaging volume was focused on the condylar region, although the prostheses extended down to the angle of the mandible. Scale bar: 10 mm.
Possible neocartilage in regenerated soft tissue
Sagittal sections of soft tissue enclosing the implanted condyle exhibited signs of neocartilage formation. Positive Alcian blue and collagen II staining were localized to the functional anterior side in nonhydrogel C and hydrogel-integrated D implant (Fig. 9). CD4 staining for helper T cells was variable with faint to no stain in the control, B, C, and D to moderate staining in A and E.
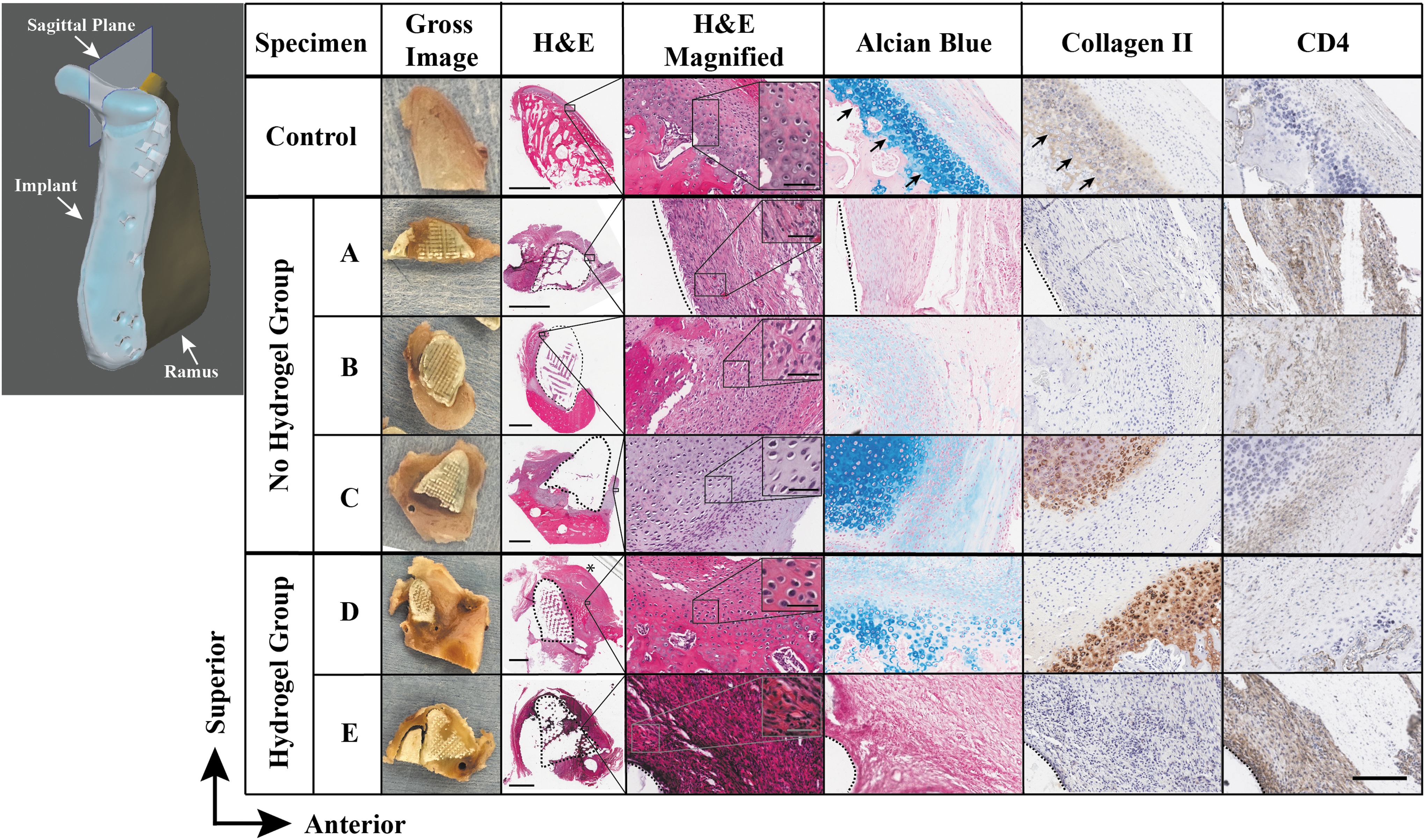
Assessment of neocartilage and bone formation with histology and immunohistochemistry from selected regions of sagittal condyle sections. Note in the healthy control tissue the deeper hyaline-like cartilage layer (black arrows) below the overlying proliferative and superior fibrous zones. Cases C (without hydrogel) and D (with hydrogel) exhibited evidence of cartilage-like soft tissue regeneration. Alcian blue staining was exhibited by the control mandibular condylar cartilage's deep layer, and in subjects A, B, C, and D with the richest experimental tissue staining in C and D. Collagen II staining was exhibited by the control specimen's deep layer, in addition to subjects C and D on the anterior, articulating surfaces. Subject B exhibited faint collagen II staining in the pericellular matrix. Generally, high collagen II staining was localized to the pericellular matrix. Specimens A and E exhibited darker CD4 staining for helper T cells than the other cases, suggesting a variable innate immune response. Little to no CD4 staining was exhibited by the contralateral control condyle. The disc fused to the surface of condyle D shown with *. Gross images presented the tissue sections before slide mounting. Illustration of ramus and condylar prosthesis (left panel) with sagittal plane was provided for orientation purposes. Dashed lines represent prosthesis border. Scale bars: 3 mm for H&E, 50 μm for insets, and 200 μm (lower right) for all other images. H&E, hematoxylin and eosin.
TMJ disc histology
Histology of the TMJ discs exhibited highly variable results from perforated, granulation tissue, to nearly pristine (Fig. 10). No observable granulation tissue was exhibited by the discs for control, B, C, and E. For B, a central disc perforation was observed. Discs for A and E presented with granulation tissue. For C, the disc histology closely matched that of the unoperated control disc.

Assessment of TMJ disc structure with histology. Disc outcomes were variable from nearly pristine to perforated. MicroCT after tissue resection illustrates approximate disc location relative to condyle and fossa. Gross images exhibit changing sizes among disc tissues. Subjects A and E exhibited granulation tissue, with some remaining discernable disc tissue in subject E (arrow). Subject C disc tissues matched the histological structure of the control, although the aspect ratio appears to have changed to a shorter medial-lateral and longer anterior-posterior than control disc. In subject D, the disc fused to the condyle; hence, there were no data. Alcian blue staining was positive in a distinct band in the control disc (*). Alcian blue staining persisted in B and C, although was largely absent in A and E. The overall gross morphology score was highest in subject C. Details regarding scoring information can be found in Supplementary Table. Orientations were medial (M), lateral (L), anterior (A), and posterior (P) for the gross images; and superior (S), and inferior (I) for histology images. Control displayed as mirror image for comparison with experimental data contralateral side of jaw. Dashed lines denote sectioning. H&E staining. Scale bars are 10 mm for gross images, 50 μm for H&E magnified column, and 3 mm for remaining images (lower right). TMJ, temporomandibular joint.
TMJ disc gross morphological scoring
Disc scores suggested degeneration, hypertrophy, and irregular macroscopic appearances for discs A, B, and E (Table 1). Although goat B scored 0 for degeneration due to perforation, the macroscopic appearance scored 1.8, higher than discs A (1.3) and E (1.0). Discs A and B scored 30% higher overall than goat E. The disc from goat C scored slightly higher than the average control disc score (4.0 vs. 3.9). It is noteworthy that the disc from goat C appeared longer anteroposteriorly and shorter mediolaterally than the contralateral control disc. No score could be collected for goat D because the disc fused to the condyle, making it difficult to discern disc tissue from other soft tissues.
Gross Morphology Grading Scale for Temporomandibular Joint Disc Evaluation
Discussion
This study demonstrated the feasibility of an acellular, biphasic TMJ prosthesis for immediate loading. The integrated hydrogel prosthesis exhibited variations in gross appearance and staining of key neocartilage markers. Specifically, one specimen from each group (hydrogel and no-hydrogel) exhibited collagen II and Alcian blue staining. CD4 staining was pronounced in one specimen from each group, and the remaining specimens exhibited little CD4 staining. It is possible that higher inflammation was associated with CD4 staining, although Vapniarsky et al. 31 demonstrated animals with chronic inflammation did not exhibit higher levels of CD4 compared to a negative control. All specimens featured fibrous soft tissues throughout the condylar head's porous architecture. Furthermore, the TMJ disc exhibited variable gross appearances and Alcian blue staining, with a nearly pristine disc coming from a hydrogel-free prosthesis.
Further studies may examine strategies for TMJ disc management and attachment during implantation. In addition, a more sophisticated, zonal material approach may be warranted to integrate stratified subchondral bone, and layered cartilage structures into a regenerated mandibular condyle. Adjustments to both biochemical (e.g., BMP-2) and physical (e.g., adjusting pore size, loading to bone, and degradation) signaling could be incorporated into the prosthesis design to improve tissue regeneration and reproducibility.
In both hydrogel and no-hydrogel groups, the prosthesis restored chewing function in a human-sized TMJ model. All subjects resumed eating a normal diet and gained weight throughout the study period. Bone responses to the scaffolds, however, were variable with regions of resorption immediately under the prosthesis. The condyles in some cases appeared to have plastically deformed toward the underlying ramus. Tensile testing revealed that the Young's modulus of PCL was enhanced to 269 MPa by the addition of HAp. For comparison, the compressive modulus of PCL-HAp has been reported in the range of 20 kPa to 150 MPa.32–34 Additional bending support in the collar of the prosthesis was enhanced by the HAp with a flexural modulus of 470 MPa.35–37 For plastic deformation or failure, strains beyond 3% in the prosthesis collar were likely allowed by resorption of supporting bone.
There are many different sources of signaling for bone maintenance and growth, including mechanical forces to the underlying bone. The mechanical loading regimen most suitable to restore bone remains unclear for the TMJ. Loads of ∼20 lbf have been measured in Macau condyles, and loads of 5 lbf were estimated from a study with humans during normal chewing function.38,39 Analysis of joint implants has suggested higher load transmission can prevent stress-shielding and thus improve bone density.40,41 In contrast, dental implants may fail to osseointegrate when immediately loaded without a 4–6-month period of load-free conditions.42,43 In this study, we introduced a method with a load sensor to measure transmitted loads.
The prosthesis design in this study transmitted a significant proportion of a 5 lbf applied load (>80%) to the supporting structure, and yet all subjects exhibited bone loss. In contrast, high stiffness metal TMJ implants rarely exhibited significant bone loss with reports of functional success for over 20 years.44,45 A more refined understanding of the types and magnitudes of stresses that encourage bone formation may be important to successful bone regeneration strategies in immediate TMJ loading applications.38,46–48 The load transmission test introduced in this study may be useful in future work for TMJ prosthesis designs that take bone mechanotransduction into consideration. Clinical joint immobilization following surgical implantation may be a further consideration for bone integration. 49
Neocartilage formation suggested evidence of a functional environment for cartilage tissue stimulus. Staining for Alcian blue and collagen II was localized to the anterior, functioning surface of a prosthesis that had no hydrogel to provide any chondroinductive cue. The posterior, nonfunctioning surface of the condyle exhibited no Alcian blue or collagen II staining. Furthermore, for the integrated hydrogel case, there were signs of bone formation on the anterior surface, although positive Alcian blue and collagen II were exhibited in a region adjacent to new bone on the anterior surface. These observations were in agreement with the concept of using functional loading to regenerate cartilage tissues.50,51
Although it may not be possible to determine cell source for regenerated neocartilage based on staining and morphology from histology, potential tissue sources that could contain progenitor cells were considered based on anatomic proximity. Given the higher numbers of stem cells in bone marrow than blood, adipose, or TMJ, the cell source for regenerated condylar tissues could likely have been bone marrow from the ramus or through systemic circulation. 52 The TMJ disc is a dense collagenous structure, but evidence of vasculature through the TMJ disc could provide transport for some Chad+ chondrogenic fibroblasts.53,54 Future work may be able to develop cell lineage tracking methods to provide compelling evidence for the origins of regenerated tissue.14,55–57
Within the condyle porous architecture, highly aligned fibrous tissues formed, although more time in vivo could potentially allow for mineralized tissue formation. This study emphasized a capillary rise scaffold design with ∼150 μm pore sizes to gain regenerative utility from the native cells located in the adjacent ramus bone marrow. Future work may explore larger, transport-sustaining pore sizes, or other pore geometries to better stimulate osteogenesis throughout the scaffold.58,59
The health of the TMJ disc offered signs of functional joint regeneration. Pristine disc structures scored higher than the average control disc throughout the 6-month implantation period. The presence of Alcian blue staining in the disc, although only on the anterior region, suggested a healthy disc structure. However, other cases here exhibited disc perforation, or granulation tissue, and potential signs of fibrous ankylosis with disc fusion to the condyle. Tissue-scale pathogenesis of ankylosis in TMJ and other joints warrants further investigation.60–64
This study had certain limitations. Additional time points with CT scans would be helpful for characterizing prosthesis deformation, or identifying locations where bone changes initiated. The structural integrity of the condyle was only examined after resection and may not provide an accurate reflection of in vivo relationships between TMJ structures. Although a biphasic scaffold was developed, only a bulk hydrogel was used here. Regenerating zonal cartilage architectures remains a goal for TMJ tissue engineering, although progress has been made with a bioreactor approach. 14 Hypothesis testing was not available due to the limited number of animals in this pilot study. A larger number of animals (n = 6+) may allow for hypothesis testing and statistical analysis for future investigations beyond this pilot study.
Conclusions
The results of this pilot study suggested improving bone continuity with the scaffold is a major goal for acellular TMJ condylar tissue engineering, which may require future efforts to consider cell seeding in the operating room and/or addition of biologic signals. An additional goal remains, improving cartilage regeneration with an integrated and layered structure like that of native condylar cartilage. Design features for resorbable scaffolds that could improve bone regeneration include adjustments to the porous architecture, load transmission profile, degradation rate, and use of biochemical signaling from growth factors (e.g., BMP-2) or peptides.
Footnotes
Acknowledgments
We would like to acknowledge generous contributions from the following, without whom this study would not have been possible: Dr. Emi Kiyotake, Chris Billings, Dr. Yingtao Liu, Dr. Shawn Lane, Courtney Rasbach, Dr. Hong Liu, Yuhua Li, Sheeja Aravindan, Dr. Reem Hossameldin, Dr. Adam Biedrzycki, Dave Samson, Mike Puccio, Ashley Potter, Dr. Jeremiah Easley, Jeannie Salash, Dr. Louis Mercuri, Dr. Jonathan Fillmore, Dr. David Hinkl, Dr. Shivakumar Raman, and Dr. Aaron Kotecki.
Authors' Contributions
D.S.N.: Methodology; conceptualization; formal analysis; software; and writing. A.R.: Methodology; formal analysis; and collect and analyze data. B.A.: Methodology. C.P.J.: Methodology and collect and analyze data. P.H.: Methodology and conceptualization. F.G.R.: Surgery; methodology; and writing-review and editing. W.R.W.: Methodology. K.-M.F.: Methodology. B.W.G.: Methodology. J.M.T.: Conceptualization and writing-review and editing. M.S.D.: Conceptualization and writing-review and editing.
Disclosure Statement
The authors have no conflicts of interest.
Funding Information
We thank the Osteo Science Foundation #10556980 for their generous support. Research reported in this publication was supported, in part, by the National Cancer Institute Cancer Center Support Grant P30CA225520 and COBRE P20GM103639 awarded to the University of Oklahoma Stephenson Cancer Center and used the Tissue Pathology Shared Resource. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.