
Abstract
Platelet-rich plasma (PRP) was prepared from goat blood using a modified Landesberg method. A PRP/calcium phosphate bone cement (CPC) composite paste was then prepared by combining PRP with injectable CPC, whereby the platelet counts in PRP increased by about 5.9-fold compared to that in the whole blood. Additionally, the levels of PDGF-AB, TGF-β, and VEGF in PRP were significantly higher than those in the whole blood. The new PRP/CPC composite exhibited significantly better injectability, initial setting time, final setting time, and washout resistance compared with CPC alone. A lumbar vertebral defect model was established in 18 Hainan indigenous male black goats via a retroperitoneal approach. Six lumbar vertebrae from each goat were randomized to three groups: a control group receiving normal saline, a CPC group using CPC paste alone, and a PRP/CPC group treated with the autologous PRP/CPC composite paste. The goats were maintained under standard feeding conditions postoperatively. Six goats were euthanized at 1, 3, and 6 months after operation to obtain vertebral specimens for assessment of vertebral strength and stiffness. Digital radiographical imaging at 6 months after operation showed that the vertebrae had normal growth and morphology in all groups. At 1, 3, and 6 months after operation, the vertebral strength and stiffness in PRP/CPC group were significantly greater than those in CPC-alone group. In addition, both vertebral strength and stiffness showed further improvement with the extension of postoperative recovery time. The PRP/CPC composite exhibited commendable rheological properties, and its application in repair of vertebral bone defects yielded favorable biomechanical properties. Furthermore, the new autologous PRP/CPC composite showed excellent biocompatibility and tissue repair capability and may prove to be a suitable candidate for repair of load-bearing bone defects, particularly those present in vertebrae.
Impact Statement
This study demonstrates that the platelet-rich plasma (PRP)/calcium phosphate bone cement (CPC) composite prepared via CPC-PRP combination has a significantly prolonged setting time, enhanced injectability and washout resistance, and remarkable rheological properties. It exhibits superior biomechanical properties in repair of vertebral bone injuries by increasing vertebral strength and stiffness. This innovation provides a robust scientific foundation for the clinical application of the PRP/CPC composite in addressing load-bearing bone defects in critical anatomical regions such as the vertebrae.
Introduction
Calcium phosphate bone cement (CPC) is a synthetic biomaterial characterized by excellent biocompatibility and porosity, which promote the ingrowth of new bone tissues and subsequent remodeling. Its effectiveness in filling bone defects can be assessed through imaging techniques during surgical procedures, making it an optimal choice for this application.1,2 The development of injectable CPC formulations has significantly expanded the clinical utility of CPC as a bone substitute graft material.3,4 These injectable formulations can be precisely tailored to match the specific characteristics of bone defects or delivered into voids and cavities via fluid flow, thus enhancing uniform and secure integration with the surrounding bone tissue. For over two decades, CPC has been utilized in orthopedic surgeries for both filling and reinforcing purposes. However, CPC has inherent limitations, including brittleness, a low degradation rate, and limited osteoconductivity, which compromise its capacity to provide sufficient vertebral stability and mechanical strength prior to fracture healing, thereby necessitating chemical modifications. Platelet-rich plasma (PRP) is an autologous blood derivative enriched with a concentrated population of platelets, which are rich in various growth factors essential for bone repair and restoration, offering excellent biocompatibility. PRP has been shown to enhance the healing process of various traumatic tissues, including those involved in sports injuries, joint pain, fractures, and osteoarthritis.
The combination of CPC (which possesses osteoconductive properties) with PRP (which provides osteoinductive capabilities) at a defined ratio can form a PRP/CPC composite. Synergistical integration of the growth factor-mediated effects of PRP with the defect-filling and hardening properties of CPC provides this PRP/CPC composite with remarkable injectability and biological activity, thus effectively facilitating new bone formation, improvement of mechanical properties, effective repair of bone defects, and reinforcement of the vertebrae. Our study aims to verify the rheological properties of the PRP/CPC composite and confirm the characteristics of the repaired vertebrae, with the objective of assessing its potential for the repair of vertebral bone defects and providing empirical evidence to support its clinical application.
Materials and Methods
Experimental animals
Eighteen Hainan indigenous male black goats weighing 19–27 kg with a mean weight of 21.56 ± 2.59 kg were sourced from the Animal Breeding Center of the Department of Animal Sciences in Hainan University [Haikou, China; License No. SYXK (Qiong) 2014-0017]. All experimental procedures were conducted in this facility. Prior to inclusion of the animals in this study, routine digital radiography (DR) and CT scan were performed to exclude vertebral anomalies and lesions. Animals diagnosed with infectious diseases were excluded. In addition, no animal had undergone anesthesia or received other medical or surgical interventions due to illness. The goats were housed indoors for 15 days prior to surgery to allow for acclimatization, ensuring stable body weight and normal physiological functions, including feeding, drinking, and daily activities. A routine fasting protocol was instituted for 36 h before surgery, along with a 6 h period of water deprivation. This study received approval from the Hospital Animal Research Ethics Committee (Approval No. 2016003).
Preparation of PRP
PRP was prepared using a modified Landesberg method, 5 with strict adherence to aseptic techniques throughout the procedure. Whole blood (5 mL) was drawn from the jugular vein of each goat using a syringe containing 1 mL anticoagulant sodium citrate, ensuring thorough mixing to prevent stratification. The blood was allowed to stand at room temperature for 2 h before being transferred to a centrifuge tube for the initial centrifugation at 2400 r/min for 10 min, with a centrifuge radius of 15 cm. After centrifugation, the supernatant was discarded, and 1–2 mm liquid interface between the upper layer and the sedimented red blood cells was carefully transferred to a new centrifuge tube for a second centrifugation at 3600 r/min for 15 min, again with a centrifuge radius of 15 cm. This process yielded a stratified supernatant and concentrated platelets. One-fourth of the supernatant obtained from the second centrifugation was combined with the concentrated platelets to yield 0.8 mL PRP. Following this, 0.2 mL coagulant, prepared by mixing 1 mL 10% calcium chloride injection with 1000 U thrombin, was added. The container was then kept open to facilitate air introduction while thoroughly mixing until a 1 g PRP gel was formed. The preparation process of PRP using the modified Landesberg method is illustrated in Supplementary Figure S1.
Preparation of PRP/CPC composite paste
Self-solidified CPC powder (10 g) was placed into two small drug cups, to which the solidifying liquid was added while stirring counterclockwise. Subsequently, 1 g prepared PRP gel and 1 g normal saline (NS) were incorporated at a mass ratio of 10:1, and stirring was continued to produce both the PRP/CPC composite paste and the CPC paste.
Detection of platelet counts and growth factors in PRP
One day prior to surgery, three 5 mL tubes of whole blood were collected from the jugular vein of each goat, ensuring thorough mixing to prevent stratification. The first tube was sent for platelet counting directly. The supernatant discarded after the initial centrifugation of the second tube was subsequently analyzed for three growth factors: platelet derived growth factor-AB (PDGF-AB), transforming growth factor-β (TGF-β), and vascular endothelial growth factor (VEGF) by using enzyme-linked immunosorbent assay in accordance with the subsection “Preparation of PRP.” The third tube underwent identical procedures for both the first and second centrifugations to prepare PRP, which was then submitted for platelet count evaluation; three-quarters of the supernatant obtained from the second centrifugation was employed to quantify the levels of PDGF-AB, TGF-β and VEGF in PRP.
Determination of injectability of the PRP/CPC composite
The PRP gel derived from the second tube in the subsection “Detection of platelet counts and growth factors in PRP” was utilized to formulate CPC paste and PRP/CPC composite paste, following the subsection “Preparation of PRP/CPC composite paste.” Each 5 mL paste was extracted using a 5 mL syringe (inner diameter 12 mm, tip diameter 2 mm). After a 2 min interval, pressure was applied to the syringe plunger to extrude the bone cement at a consistent rate of 10 mm/min, with the process ceasing after 3 min. The total mass of the bone cement in the syringe prior to applying pressure (M0) and the mass of the residual bone cement in the syringe postinjection (M1) were recorded. The injectability of the bone cement was determined using the formula: Injectability (%) = (M0-M1)/M0 × 100%.
Measurement of the setting time of the PRP/CPC composite
1 mL CPC paste and 1 mL PRP/CPC composite paste, as referenced in the subsection “Determination of injectability of the PRP/CPC composite” were aspirated using a 5 mL syringe and subsequently injected into a prefabricated cylindrical mold with dimensions of 6 × 10 mm. The mold was positioned horizontally on a cement consistency setting time tester at room temperature, with the total mass of the tester’s sliding rod calibrated to 300 ± 0.5 g and the needle diameter set at 1 ± 0.05 mm. The Vicat testing needle was then inserted perpendicularly into the surface of the bone cement and held in place for 5 s before removal. Following extraction, the needle was cleaned with a designated tissue, and this procedure was repeated at 60-second intervals until the bone cement had fully hardened. The initial setting time was defined as the moment when the needle penetrated less than 2 mm into the bone cement, and the final setting time was recorded when the needle could no longer penetrate the material and no discernible indentation remained on its surface.
Determination of the antiwashout properties of the PRP/CPC composite
Employing the methodology outlined in the subsection “Determination of injectability of the PRP/CPC composite,” 1 mL CPC paste and 1 mL PRP/CPC composite paste were drawn using a 5 mL syringe and injected into a prefabricated cylindrical mold measuring 6 × 10 mm. Following the attainment of the initial setting time, the mold was promptly removed, and the specimen was completely submerged in a petri dish filled with NS. The morphology of the specimen was evaluated at intervals of 5, 30, 60, and 120 min postsubmersion to ascertain its antiwashout properties.
Establishment of a lumbar vertebral defect model
One day prior to surgical intervention, the skin in the designated surgical area of the goat was meticulously prepared. Thirty minutes before the procedure, atropine sulfate (0.05 mg/kg) was administered intramuscularly in the gluteal region, followed by an intravenous administration of 1.6 million units of penicillin. After anesthesia induction, the goat was positioned laterally and secured on the surgical table. A jugular venipuncture was performed to establish an intravenous infusion line, and endotracheal intubation was conducted to facilitate anesthesia maintenance through intravenous infusion. The surgical field was thoroughly disinfected and draped. Utilizing a refined animal model methodology from our prior investigations, 6 a lumbar vertebral defect model was established in the goat via a retroperitoneal approach. Upon complete exposure of the lumbar vertebrae, an orthopedic high-speed drill fitted with a 6 mm diameter bit was employed to create a 6 × 10 mm cylindrical cavity on the lateral aspect of the 6 lumbar vertebrae. The drilling was performed perpendicular to the sagittal plane and parallel to the posterior margin of the vertebrae, with a controlled penetration depth of 10 mm. Following creation of the cavity, bone debris was meticulously removed from both the cavity and the surgical site. The surgical area was subsequently irrigated with NS, and hemostatic packing was applied to achieve hemostasis, thereby establishing the lumbar vertebral defect model in the goat. The anesthetic dosage was gradually tapered in accordance with the surgical progress to facilitate the goat’s awakening postprocedure. Upon regaining consciousness, the endotracheal tube was extubated, and suction was applied as necessary to ensure unobstructed airway patency. The preparation process for the goat lumbar vertebral bone defect model is shown in Supplementary Figure S2A-C.
Filling of the cavity with bone cement and vertebral repair
The CPC paste and PRP/CPC composite paste, prepared as described in section “Preparation Method of PRP/CPC Composite Paste,” were allowed to gradually solidify into a viscous state. Subsequently, 2 mL of each paste was drawn into two separate 5 mL syringes, while an additional 2 mL NS was drawn into a third 5 mL syringe. Following the preoperatively established filling protocol utilizing a random number table, these three solutions were randomly injected into the 6 lumbar vertebral cavities of the autologous PRP donor goat, with each solution administered into two cavities at a volume of 1 mL per cavity. The filling status of the 6 lumbar vertebrae was meticulously documented. Once it was confirmed that the bone cement was completely filled and had set, a curette was employed to excise any excess bone cement protruding above the surface of the bone defect. The wound area was subsequently irrigated profusely with NS, and electrocautery was applied to ensure hemostasis. Direct electrocautery was performed in regions devoid of bone cement to guarantee comprehensive hemostatic control. Throughout the procedure, careful observation was maintained for potential damage to the peritoneum and other vital organs, and a drain was inserted as warranted by the intraoperative bleeding conditions. The fascia layer, subcutaneous tissue, and skin were meticulously sutured using No. 4 silk thread. The wound was then dressed with alcohol-soaked gauze and fat-free gauze, followed by secure application of a sterile iodine adhesive film over the skin. The wound meticulously sutured closed is shown in Supplementary Figure S2D.
Postoperative management of animals and specimen collection
Following complete recovery from anesthesia, the goats were transported to the animal housing facility, where they underwent management utilizing a combination of free-range and confined rearing methods. Water and food were positioned approximately 1 m above the ground, supplemented with a ramp to mimic human upright posture and facilitate vertical loading on the spine. Water was administered 2 h postsurgery, and feeding commenced 6 h postsurgery, with unrestricted access to food and activity initiated on the second postoperative day. Surgical wounds were dressed every other day, with no antibiotics or additional medications employed. During the initial dressing change on the second postoperative day, the drainage tubes were removed, and sutures were extracted between 10 and 12 days postsurgery. The overall condition of the experimental animals was closely monitored. Utilizing a random number table, six goats were randomly euthanized at 1, 3, and 6 months postsurgery. Euthanasia was conducted using a substantial dose of pentobarbital sodium administered intraperitoneally, resulting in rapid deep anesthesia and subsequent painless death. Prior to euthanasia, all animals underwent DR examination. At T12/L1 and L6/S1 intervertebral levels, the supraspinous ligament, interspinous ligament, intervertebral disc, and joint capsule were transected, and the vertebral bones of six lumbar vertebrae from each goat were meticulously harvested. Based on the filling conditions specified during the surgical procedure, the vertebral specimens were classified into three distinct groups: the saline-filled specimens served as the control group, while the other groups consisted of the CPC group and the PRP/CPC group. All soft tissues, including tendons, muscles, ligaments, and intervertebral discs, were thoroughly excised from the surface of the vertebral specimens, preserving only the intact vertebral bone and adjacent endplates. Bone healing and growth were assessed in each group, and the specimens were subsequently sealed and stored at −20°C for future analysis.
Measurement of vertebral morphological parameters
Prior to euthanasia, the lumbar vertebrae of goats were analyzed using a medical imaging system to obtain anteroposterior and lateral radiographs. The morphological parameters of each lumbar vertebral bone, specifically length, width and height, were measured. Length was defined as the shortest distance between the bilateral cortical edges observed on the anteroposterior view, and width was determined as the shortest distance from the anterior to the posterior cortical edges on the lateral view. Height was defined as the shortest distance between the superior and inferior endplates, as seen on either the anteroposterior or lateral view. The methodologies for measuring vertebral morphological parameters are detailed in Supplementary Figure S3. Each morphological parameter was measured three times by a designated radiologist with expertise in imaging, and the mean value was recorded for analysis.
Determination of the vertebral biomechanical properties
Vertebral specimens from each group were subjected to cryopreservation and then transported to the biomechanics laboratory for biomechanical testing, where they were thawed at room temperature. Portions of the transverse processes were excised, and the roots of the spinous processes were trimmed to facilitate their insertion into a prefabricated mold. The superior and inferior endplates were embedded using a self-curing dental resin mixture (polymethyl methacrylate, PMMA), which consists of self-curing denture base liquid and powder to ensure a flat surface on both extremities. The process of vertebral bone treatment for evaluating biomechanical properties is shown in Supplementary Figure S4. Following treatment, the vertebrae from each group were sequentially placed into a high-precision biomaterial testing system for axial compression testing. To enhance the accuracy of the measurement data, the testing protocol commenced with the application of a preload of 200 N axially via a specially designed loading head for 30 s to eliminate the time-dependent effect, relaxation, creep and other rheological factors intrinsic to the vertebrae. Subsequently, the parameters were adjusted to a load of ±7.5 kN and dynamic strain of ±25 mm, with the load being gradually increased until a compressive fracture of the vertebrae occurred. A graphic recorder automatically captured the load-displacement curve at a frequency of 100 Hz; the peak value of this pressure curve was designated as the strength value, and the slope of the linear segment was identified as the stiffness value (Supplementary Fig. S5). The load-displacement curves of partial vertebrae at various postoperative time points for the three groups are represented in Supplementary Figure S6.
Statistical analysis
Statistical analyses were conducted using SPSS 21.0 software, with data expressed as the mean ± standard deviation (
Results
Platelet count and growth factor levels
Platelet count in PRP group increased by 5.9-fold (588.8% ±62.8%) compared to that in whole blood group (p < 0.0001). Additionally, the levels of PDGF-AB, TGF-β and VEGF in e PRP group were significantly higher than those in the whole blood group (p < 0.0001, p < 0.001, p < 0.0001, respectively). These findings, illustrated in Figure 1, indicate that the PRP preparation effectively enriched both platelets and essential growth factors crucial for bone repair.

Comparison of platelet count and levels of three growth factors between whole blood group and PRP group (
Injectability of the PRP/CPC composite
Both CPC and the PRP/CPC composite displayed favorable rheological characteristics and excellent injectability during the infusion process. The extruded bone cement retained a rod-like morphology, remaining intact without signs of dispersion or hardening (Fig. 2). The injectability rate in PRP/CPC group was significantly higher than that in CPC group (63.10 ± 3.08% vs. 50.97 ± 2.48%, p < 0.0001) (Fig. 3). These results demonstrated that CPC and PRP combination substantially enhanced the injectability of the PRP/CPC composite.

Injection characteristics of CPC and the PRP/CPC composite.
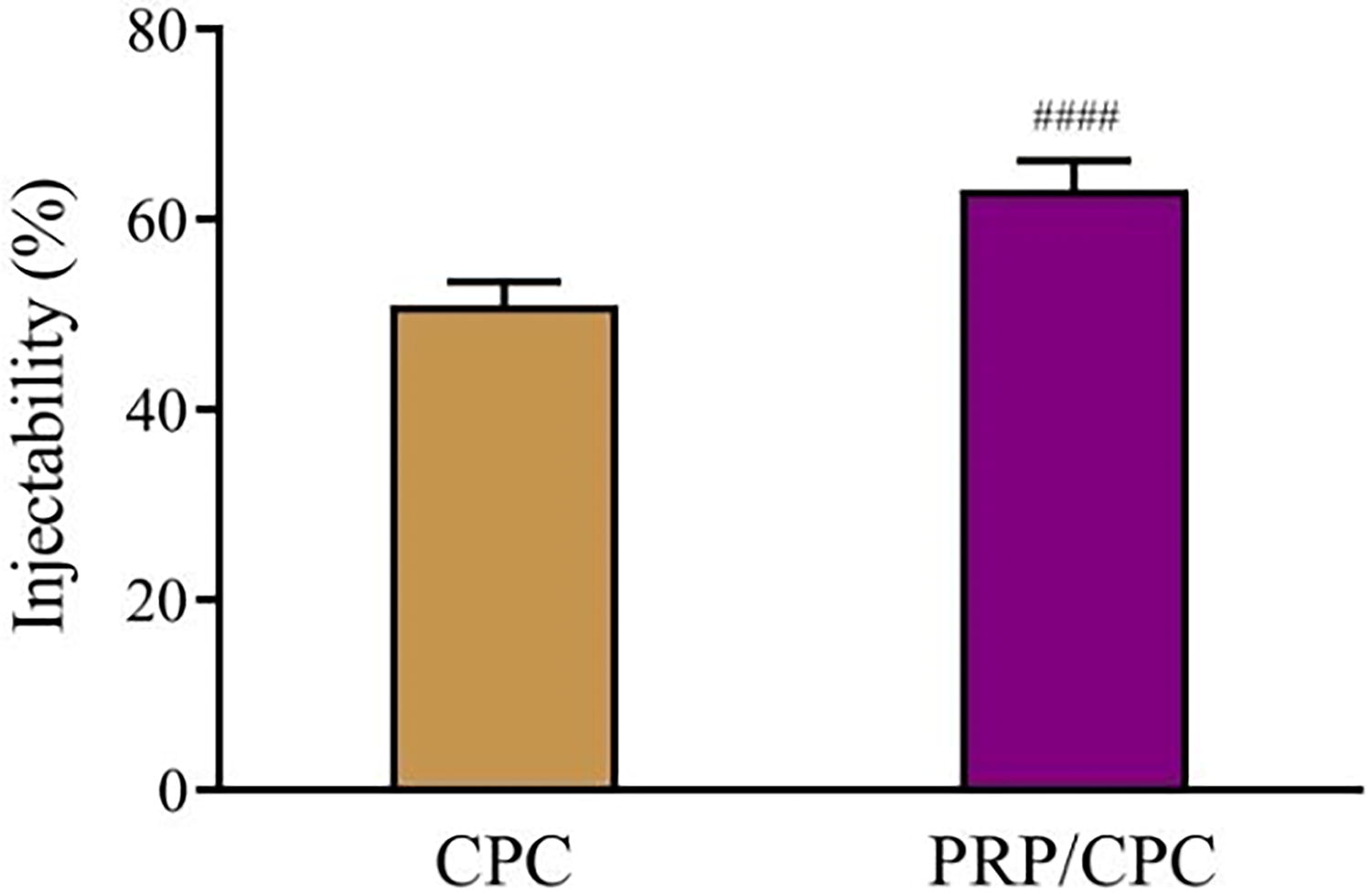
Comparison of injectability between CPC and PRP/CPC groups (
Coagulation time of the PRP/CPC composite
The initial coagulation time in PRP/CPC group was significantly longer than that in CPC group (13.37 ± 1.03 vs. 11.33 ± 1.03 min, p < 0,001). The final coagulation time in PRP/CPC group was also significantly longer than that in CPC group (19.22 ± 0.90 vs. 16.52 ± 0.83 min, p < 0.001) (Fig. 4). These results demonstrate that PRP/CPC combination significantly prolonged the coagulation time.

Comparison of initial and final setting time between CPC and PRP/CPC groups (
Antidisaggregation properties of the PRP/CPC composite
Immersion of the initial coagulation model of CPC in NS for 5 min resulted in a noticeable loss of powder due to material washout, which presented as a cloudy suspension. After 30 min, this dispersion became increasingly obvious, with the presence of particles of varying dimensions. The quantity of fine particles continued to escalate at the 60 min mark, while no significant change was observed at 120 min (Fig. 5a). In stark contrast, the initial coagulation model of the PRP/CPC composite maintained its integrity after 120 min immersion in NS, with no observable loss of powder or particles at any time point (Fig. 5b). These findings indicate that the integration of CPC and PRP markedly enhanced the antidisaggregation properties of the PRP/CPC composite.
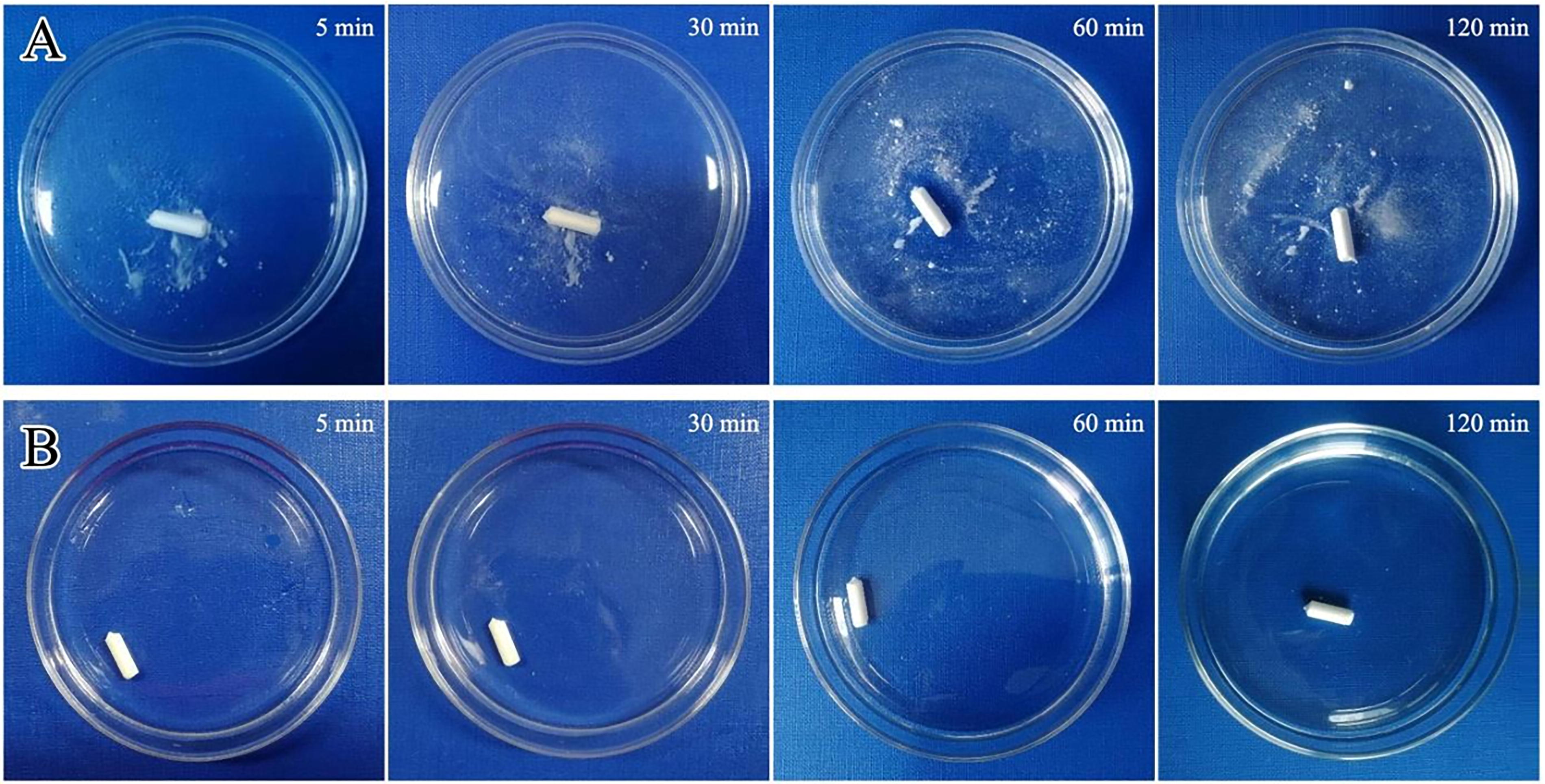
Comparison of the appearance of CPC and the PRP/CPC composite after immersion in saline.
The general condition of experimental animals
All experimental animals successfully underwent the surgical modeling procedures and were subjected to final observations at the predetermined time points. The duration of surgery varied between 64 and 92 min, with a mean of 75 ± 6.95 min. Intraoperative blood loss ranged from 50 to 110 mL, averaging 81.94 ± 15.64 mL. No adverse events, including intraoperative or postoperative mortality, were recorded throughout the experimental timeline. During the postoperative observation period, there was no occurrence of wound infection, cement leakage, cauda equina or nerve root damage, pathological vertebral fractures, or ectopic bone formation.
Morphological parameters of vertebral repair with the PRP/CPC composite
Comparative analysis indicated no statistically significant differences in the length, width, and height of the vertebrae between control, CPC, and PRP/CPC groups at 6 months after operation (p >0.05) (Fig. 6). This finding indicates that the vertebrae repaired with the PRP/CPC composite exhibited normal growth and morphological characteristics.
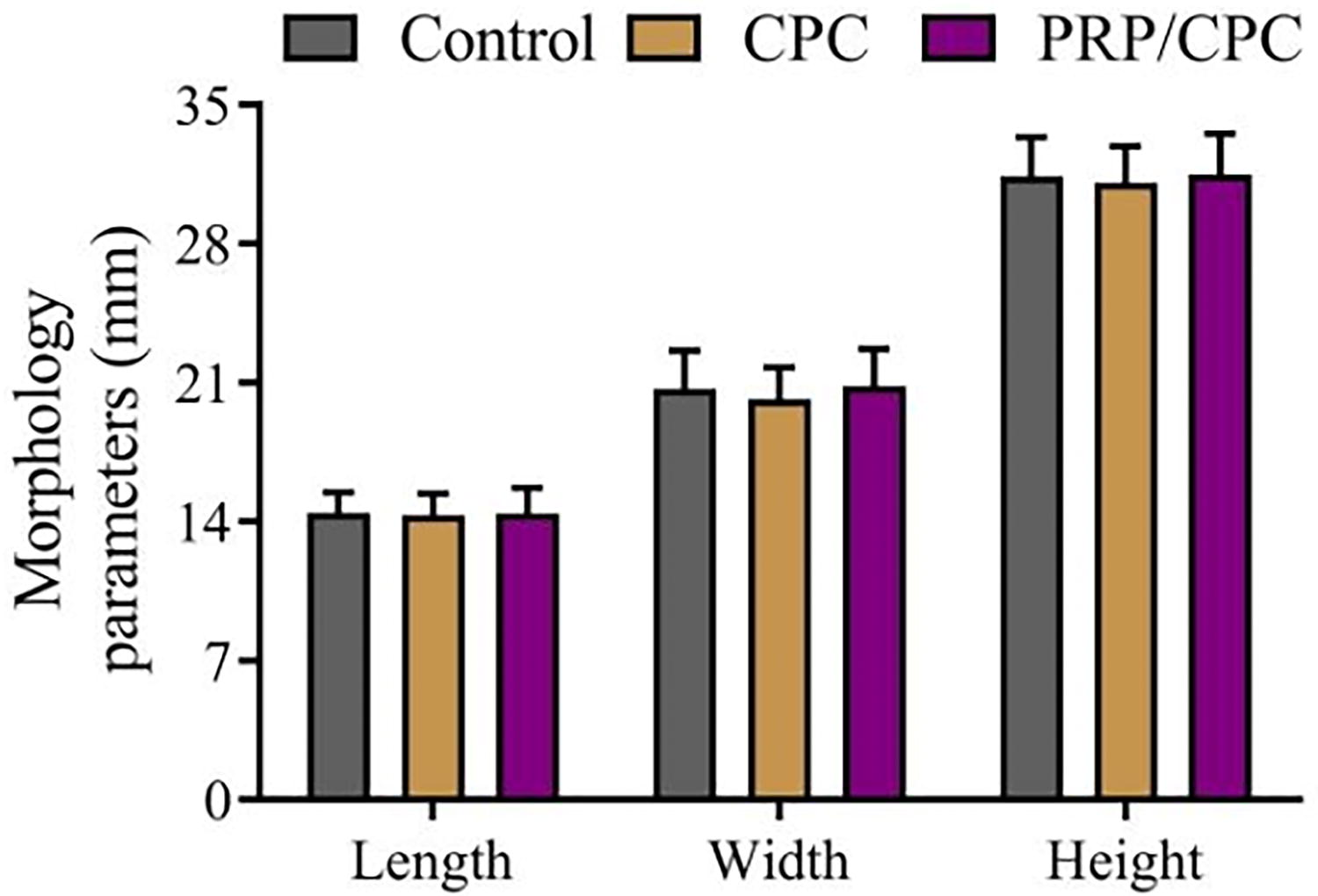
Comparison of morphological parameters of vertebrae between three groups at 6 months postsurgery (
Strength of vertebral bone repaired with the PRP/CPC composite
The vertebral strength measured one month after operation was 2929.77 ± 89.21 N/mm in PRP/CPC group versus 2622.60 ± 105.78 N/mm in CPC group and 2402.70 ± 78.80 N/m in control group, indicating that the vertebral strength in PRP/CPC group was significantly greater than that in both CPC and control groups (both p < 0.001). Additionally, the vertebral strength in CPC group was significantly higher than that in control group (p < 0.01). The vertebral strength measured at 3 and 6 months after operation was significantly higher than that measured at one month after operation in both PRP/CPC and CPC groups as compared to that in control group. The vertebral strength in control group remained relatively stable. At 3 months after operation, the vertebral strength in PRP/CPC group was significantly superior to that of CPC and control groups (both p < 0.0001). Similarly, at 6 months after operation, the vertebral strength in PRP/CPC group continued to show significant superiority over that of CPC and control groups (both p < 0.0001). The results are detailed in Figure 7.
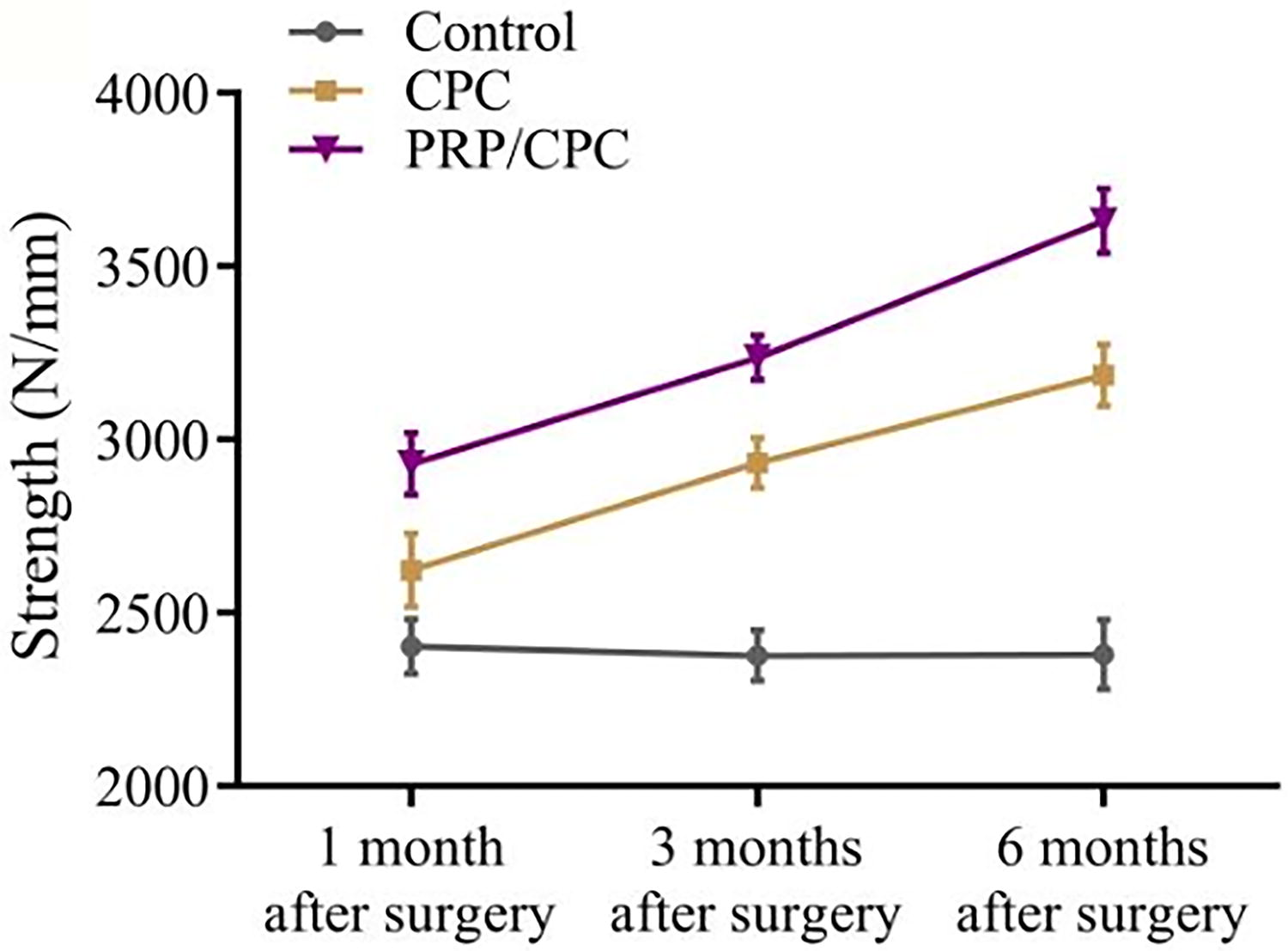
Variation curves and comparison of vertebral strength between three groups at 1, 3, and 6 months postsurgery (
Stiffness of vertebral bone repaired with the PRP/CPC composite
In PRP/CPC group, the vertebral stiffness measured at one month after operation was 1065.69 ± 87.74 N/mm versus 930.37 ± 46.87 N/mm in CPC group and 920.56 ± 37.48 N/mm in control group, showing that the vertebral stiffness in PRP/CPC group was significantly greater than that in both CPC and control groups (both p < 0.01), while no significant difference in vertebral stiffness was observed between CPC and control groups (p >0.05). At 3 and 6 months after operation, the vertebral stiffness gained a substantial increase in both PRP/CPC and CPC groups compared to that measured at one month after operation, while the vertebral stiffness remained relatively stable in control group. At 3 months after operation, the vertebral stiffness in PRP/CPC group was significantly higher than that in both CPC and control groups (both p < 0.0001). Similarly, at 6 months after operation, the vertebral stiffness in PRP/CPC group continued to increase compared with CPC (p < 0.01) and control group (p < 0.0001). The results are detailed in Figure 8.

Variation curves and comparison of vertebral stiffness between three groups at 1, 3, and 6 months postsurgery (
The composite resulting from the combination of CPC and PRP, referred to as the PRP/CPC composite, exhibited a remarkable improvement in the strength and stiffness of the repaired vertebrae. Moreover, as the duration of postoperative recovery increased, both vertebral strength and stiffness continued to enhance, indicating that the PRP/CPC composite possessed excellent biocompatibility and reparative capabilities.
Discussion
PRP is a readily accessible and cost-effective blood derivative which provides a diverse array of autologous growth factors and cytokines, including PDGF, TGF-β, VEGF, platelet-derived endothelial cell growth factor, platelet-derived angiogenesis factor, and platelet factor 4. These growth factors are predominantly secreted by the α-granules of platelets, and upon activation they not only facilitate tissue repair but also enhance tissue recovery by self-regulating the equilibrium between the synthesis and degradation of bioactive components. 7 The constituents of PRP are naturally occurring bioactive substances that do not elicit immune rejection when administered to humans. 8 Extensive research has demonstrated that PRP can significantly promote new bone formation, particularly during the early phases of bone healing. The diverse growth factors present in PRP influence the chemotaxis, differentiation, and proliferation of bone cells, thereby promoting the aggregation and mitosis of osteoblast precursors and osteoclasts, which in turn regulates bone growth and remodeling. 9 Currently, commercially available growth factor products are prohibitively expensive and may induce adverse effects, such as immune rejection, due to their nonautologous origins. In the present study, we employed a modified Landesberg method at the first centrifugation rate of 2400 r/min and the second centrifugation rate of 3600 r/min. This modification resulted in a higher concentration of platelets in the isolated PRP, achieving a platelet concentration that was 5.9 times that of whole blood. The subsequent experiments verified that this PRP was enriched with critical growth factors, including PDGF, TGF-β, and VEGF, thus enhancing the release of growth factors through CPC scaffolds, inducing the proliferation and differentiation of osteoblasts, and facilitating new bone formation within bone defects. This approach effectively addresses the challenge of inadequate blood volume in small animals for the preparation of autologous PRP by utilizing peripheral venous whole blood. 10
Polymethyl methacrylate is the most commonly utilized autologous bone substitute material for the repair of bone defects. Once injected into the body, PMMA can diffuse through the interstices of the loose trabecular bone and solidify rapidly, thereby providing adequate mechanical strength. But as PMMA lacks the abilities to integrate with the bone tissue, promote new bone formation, or facilitate remodeling of the trabecular structure, it may ultimately fail to restore the internal anatomical integrity. For this reason, PMMA is unsuitable for young patients with robust bone quality and pronounced bone growth and remodeling capabilities, particularly those with vertebral fractures or lesions. 11 In addition, the polymerization reaction of PMMA during its solidification generates substantial heat, potentially reaching temperatures of up to 60°C, which can adversely affect normal bone tissue and adjacent soft tissues. In contrast, CPC has emerged as a widely employed biological filling material intended to substitute autologous bone grafts within orthopedic applications. Upon hardening, CPC forms hydroxyapatite, which closely resembles the primary component of the bone extracellular matrix, thereby demonstrating excellent biocompatibility with surrounding tissues. Notably, the in vivo hardening process of CPC does not generate excessive heat, thereby preventing necrosis of adjacent bone tissues. Additionally, CPC exhibits strong osteoconductive properties, facilitating new bone formation and ingrowth through its inherent degradation and absorption mechanisms. Particularly, injectable CPC can be percutaneously administered to the bone defect site for diffuse filling, ensuring intimate adhesion to the normal bone tissue, which promotes optimal osteogenesis and efficient bone remodeling. This innovative approach enables the performance of numerous open surgical procedures through minimally invasive techniques, thus significantly broadening the application scope of CPC in orthopedic surgery.
Experimental studies on repair of nonload-bearing bone defects in the cranial bone, sacrum, and radius of small animals have shown that the combination of CPC with PRP can significantly accelerate new bone formation, producing results comparable to those achieved with autologous bone grafts. However, most of these studies employed granular or block solid materials. 12 In vitro experiments have demonstrated that when PRP is combined with CPC powder at a mass ratio of 1:9 [Mass PRP/(Mass PRP + Mass CPC) = 10%], there is a positive impact on the release of active substances from PRP, as well as on the elastic modulus and growth factor release of the composite. 13 In our study, the mass ratio of CPC to PRP in the prepared PRP/CPC composite is 10:1, resulting in a significant improvement in the injectability of the composite. Our study showed that CPC and PRP combination could effectively reduce the osmotic pressure of the raw materials, and that lowering or eliminating osmotic pressure is a critical factor in enhancing the injectability of the CPC slurry. It has been reported that a higher liquid-to-powder volume ratio (L/P ratio) can markedly enhance the injectability of the material. 14 Our study showed that mixing CPC with PRP generated a fluid state, thus increasing the L/P ratio and consequently extending the setting time of the bone cement, which is consistent with the previous findings of our research group. 15 PRP is enriched with proteins and other active components that contribute to viscosity; thus, despite the increased L/P ratio, the viscosity of the PRP/CPC composite did not significantly decrease. In addition, the incorporation of PRP into CPC improved the rheological properties of the composite material, thereby enhancing its injectability, primarily through the modulation of CPC viscosity by citrates and other small molecules present in PRP. Citrate, a weak organic acid with three carboxyl groups, can form composites with calcium ions, reducing the adsorption of metal ions on the solid particles within CPC, which weakens the interactions between particles and lowers the viscosity of CPC. Some studies reported that addition of citrates to CPC could enhance its injectability by 50–100%. 16 Furthermore, the initial and final setting time of the PRP/CPC composite was significantly extended, potentially due to the interactions between proteins and growth factors in PRP, a phenomenon that has been documented in calcium phosphate-based systems.17,18 The prolongation of the setting time is advantageous for clinical applications.
Brittleness is the primary limitation of CPC, which adversely affects its mechanical properties and hampers cell infiltration. 19 The intrinsic brittleness and limited compressive strength of CPC restrict its utilization in load-bearing applications, particularly within vertebral bones. Due to the degradation of CPC materials and the protracted duration required for new bone ingrowth, it fails to provide adequate mechanical strength during the initial phases of filling and solidification. Consequently, the exclusive use of CPC for the treatment of high-energy, unstable spinal injuries is not advisable. 20 The repair of bone defects transcends mere filling; it necessitates the promotion of bone growth and healing to restore mechanical properties that align with physiological requirements. 21 Injectable CPC features a microscopically uneven surface, which enhances the adhesion of various growth factors and facilitates new bone formation. Research indicates that the rate of postoperative new bone formation using a composite of PRP and CPC is 8–10% higher than that observed with pure CPC alone. 22
Our study has demonstrated that the PRP/CPC composite can markedly enhance the mechanical properties of the CPC material. In terms of vertebral biomechanical properties, both stiffness and strength of the vertebrae in PRP/CPC and CPC groups exhibit an increase over time postoperatively. Nevertheless, the mechanical properties of the vertebrae in PRP/CPC group consistently surpassed those in CPC group at all postoperative time points. Given that the compressive strength of cortical bone significantly exceeds that of trabecular bone, these findings may correlate with the successful healing of the cortical surface in certain vertebrae within PRP/CPC group and the complete encasement of the bone cement within the bone defect. Although some growth of the outer cortical bone occurred in control group, the internal bone defect remained inadequately repaired and lacked support from bone cement; thus, even with cortical bone development, the capacity to resist fractures induced by external forces is limited. As a result, during the experiment, no significant change in the stiffness and strength of the vertebrae in the control group was observed as the postoperative recovery time increased. In contrast, the vertebral stiffness and strength in PRP/CPC composite group were markedly superior to those in both CPC and control groups, underscoring the critical role of the diverse growth factors abundant in PRP in the repair of bone defects and in enhancing the load-bearing capacity of the materials. This beneficial effect is likely attributable to growth factors such as PDGF and TGF-β present in PRP, which can directly stimulate osteoblasts and augment their activity, thereby promoting the differentiation and maturation of osteoprogenitor cells. 23 The findings of this study align with the existing literature, 24 highlighting the enhancement of bone cement properties and facilitation of bone repair by PRP. The underlying mechanism may involve the particles of bone cement achieving optimal solubility in PRP, thereby maximizing the load-bearing capacity of the bone cement and its efficacy in promoting bone repair.
Conclusions
This study has demonstrated that the PRP/CPC composite by combining CPC with PRP can significantly extend the setting time and improve injectability and washout resistance, with favorable rheological properties. When applied to the repair of vertebral bone injuries, it markedly increases the vertebral strength and stiffness, demonstrating superior biomechanical performance. This research provides a solid scientific basis for the clinical application of the PRP/CPC composite in addressing load-bearing bone defects in critical anatomical regions, such as the vertebrae. Furthermore, it enriches our understanding of the biological functions of PRP composites and opens new avenues for the design and application of biomaterials. It is essential to acknowledge that, despite the dual advantages of biomechanical stability and biological activity inherent in the PRP/CPC composite, comprehensive cost-benefit analyses are required prior to its clinical implementation, and the protocols for PRP preparation and application require optimization. Future investigations should focus on the preparation of human PRP, the standardization of human PRP/CPC composite production, and assessment of their therapeutic efficacy and safety across a broader range of clinical contexts.
Footnotes
Authors’ Contributions
Y.G.: Conceptualization, experimental research, funding acquisition, writing—original draft. Y.Y.: Conceptualization, data curation, supervision, writing—review and editing. B.P. and G.X.: Experimental research and methodology validation.
Ethics Statement
This study was approved from the Hospital Animal Research Ethics Committee of the 928th Hospital of the Chinese PLA Joint Logistic Support Force. We affirm that this study was carried out in accordance with the relevant guidelines and regulations.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Health and Wellness Industry Research Project of Hainan Province, China (22A200177), the Natural Science Foundation Project of Hainan Province, China (20168345), and the Discipline Innovation Project of the 928th Hospital of the Chinese PLA Joint Logistic Support Force (2025YJKT002).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.