
Abstract
Background:
Implantation of thyroid cells (ITC) into extrathyroidal locations is a rare complication of thyroid fine-needle biopsy (FNB) and thyroid surgery. Here we review the prevalence, likely pathogenesis, treatment, and likely ways to minimize this complication of invasive thyroid procedures and present an illustrative patient.
Summary:
Tumor aggressiveness more likely leads to ITC after FNB. Large needle size may be associated with increased risk of ITC. Number of passages during biopsy, excessive suction, needle withdrawal without releasing suction, and injection of tumor cells during biopsy may be associated with ITC after FNB. This statement is based on rational hypotheses. Cutting or rupture of a thyroid nodule during surgery leads to ITC into extrathyroidal soft tissue.
Conclusions:
ITC occurs rarely with needles smaller than 23 gauge. Some authorities suggest the use of gentle suction and release suction during extraction and a reduced number of passes based on entirely theoretical grounds. In conventional surgery, lobectomy for all thyroid nodules rather than nodulectomy or partial lobectomy should be performed. If endoscopic surgery is performed on larger nodules, the surgeon should take great care to avoid rupturing the tumor.
Introduction
Prevalence
ITC after FNB
ITC has been reported when FNB has been performed for papillary (3 –6,9), follicular (8,11), and anaplastic thyroid carcinomas (2) (Table 1). ITC after FNB for benign thyroid lesions has not been reported. The prevalence of ITC after FNB in papillary thyroid carcinoma (PTC) was 0.14% in a study of 4912 patients (5). In the Ito et al.'s study (5), FNB was performed with a 22-gauge needle and the median interval from the FNB to the finding of ITC was 77.5 months (range, 2–131 months). ITC after FNB has been reported less often in follicular thyroid carcinoma with only two reported cases (8,11) and in anaplastic thyroid carcinoma (2) with only one reported case. There may be reasons for the lower prevalence of ITC in patients with follicular and anaplastic carcinomas than in patients with PTC. First, the incidence of follicular and anaplastic thyroid carcinomas is lower than that of PTC (5). Second, patients with PTC survive longer than those with anaplastic carcinomas (5).
Age at first procedure.
Size of thyroid lesion at the time of the initial procedure.
Interval between initial needle biopsy and implantation.
The patient underwent needle biopsy three times: 5, 7, and 9 years after implantation. Implantation of the thyroid lesion was detected 3 weeks after the third needle biopsy. It was suggested that implantation may have developed after the first or second needle biopsy.
SC, subcutaneous; SCM, sternocleidomastoid muscle; PD, poorly differentiated; WD, well differentiated.
ITC after surgery
ITC is probably less likely to occur after thyroid surgery than after FNB (5). In contrast to ITC after FNB, most ITC after surgery have been reported in benign thyroid tumors (7,13,14) such as colloid nodules, adenomatous hyperplasia, follicular adenoma, and Hurthle cell adenoma except one case of follicular carcinoma (13) (Table 2).
Age at first procedure.
Size of the thyroid lesion at the time of the initial procedure.
Interval between surgery and implantation.
Pathogenesis
ITC after FNB
FNB of human tissues may cause a release of tumor cells due to damage at the puncture site and adherence of tumor cells around or in the needle, which become implanted as the needle is withdrawn (5,15 –17).
The study of Ito et al. (5) found that most cases of needle tract implantation occurred in patients aged 50 years or above and in thyroid carcinoma with an extrathyroidal extension. ITC after FNB usually occurred with large thyroid nodules (5). The smallest thyroid nodule with ITC after FNB was 1.9 cm in the study of Ito et al. (5). The interval between an FNB and the diagnosis of needle tract implantation for PTC was related to the growth activity of the tumor (5).
ITC occurs after needle biopsy of a variety of human cancers (18,19). Weiss reported that the number of tumor cells released by an FNB of renal cancers was quite variable in the excised surgical specimen (20). The prevalence of ITC in thyroid carcinoma (0.14%) is lower than in hepatocellular carcinoma (1.22–2.7%) or in pancreatic carcinoma (1.4%) (19). We believe that it is likely that thyroid cancers are less aggressive than hepatocellular or pancreatic carcinoma. In addition, smaller caliber of the biopsy needles usually used (22–27 gauge) for thyroid carcinoma than for hepatocellular or pancreatic carcinoma (19), the shorter needle tract, and the use of radioactive 131I ablative therapy, and thyroxine therapy after surgery are likely factors in the difference in these prevalences. There have been no evidence-based randomized studies, however (2,5,8,11).
We are not aware of studies of ITC after FNB of the thyroid gland in animals. Implantation of malignant cells as a result of FNB has been noted in animal models of cancers other than the thyroid (15,21). Engzell et al. reported implantation of rabbit V2 carcinoma cells along the needle tract after FNB of a popliteal lymph node (15). Ryd et al. noted tumor growth along the needle tract in 65% to 83% of mice (21). FNB of sarcoma or fibrosarcoma (MCG101-AS, MCB21-AS, and MCB21-SS) was performed through the leg muscle of a healthy mouse into the tumor of a donor mouse (21). They estimated that about 103–105 tumor cells were implanted into the leg muscles of mice after this procedure (21).
Tumor cells from spontaneously occurring human cancers seem to require larger inocula for growth than those noted in animal studies (21). Experimental animal tumors are highly malignant. These tumors typically have little stroma and no intercellular junctions. Therefore, large numbers of cells are easily released from the biopsy needle (21). Some released human tumor cells are damaged, others are nonviable outside the main tumor mass, and the host immune system can destroy most implanted cells (20).
ITC after surgery
Harach et al. (13) reported eight cases of thyroid implantation after surgery. Three were colloid nodules, three were follicular adenoma, one was a Hurthle cell adenoma, and one was follicular carcinoma. In all or a majority of the cases, cutting nodular thyroid tissue at initial thyroid surgery led to implantation of cells released from thyroid nodules into the surrounding tissue of the neck, resulting in multiple subcutaneous nodules (13). During endoscopic thyroid surgery for adenomatous hyperplasia, rupture of the thyroid nodule has led to ITC into soft tissue (7).
Characteristics and Differential Diagnosis of Thyroid Tissue in Extrathyroidal Locations
When thyroid tissues are found in the extrathyroidal location, the differential diagnosis includes implantation during FNB, surgical implantation, metastatic lymph node from thyroid carcinoma, benign metastatic thyroidosis, true ectopic thyroid tissue, and a detached thyroid nodule (Table 3) (13). ITC after FNB has been noted in the skin, the subcutaneous layer, and the muscular layer (2 –4,6,8,9,11). If nodules are located in the skin and correspond to the needle entry site, or if multiple nodules are lined vertically from the dermis to the muscle and are immediately above the thyroid nodules, ITC should be considered in the differential diagnosis (Fig. 1) (6,8,9,11). Surgery does not disrupt the internal layer of the sternocleidomastoid muscle. Therefore, metastatic nodules within the muscle layer suggest ITC after FNB (6). Multiple subcutaneous nodules located in the previous operating field and resembling previous intrathyroid tumors on histology are consistent with intra- or postprocedure ITC (13,14,22). Benign metastatic thyroidosis or benign thyroid inclusions are defined as small groups of well-differentiated thyroid follicles in the lymph nodes without a primary carcinoma (23,24). Rosai et al. reported on the histologic criteria for differentiating malignant metastasis from benign metastatic thyroidosis or benign thyroid inclusions (25). When more than one-third of the lymph node is altered, or several lymph nodes are affected, metastases from malignancy are more likely. The presence of psammoma bodies within the lymph nodes is suggestive of malignant metastasis. Benign metastatic thyroidosis or benign thyroid inclusions are defined as a few small follicles that are located within the lymph node or immediately beneath the capsule. These follicles have no cytologic features of papillary carcinoma. Ectopic thyroid usually occurs adjacent to the normal thyroid gland in the midline from the foramen cecum to the isthmus (26). Embryologically, the thyroid gland is derived from three anlages, a large median endodermal anlage and two lateral anlages (27). The median anlage is the more important in the development of the thyroid gland. Failure of the median anlage to descend commonly results in ectopic thyroid tissue located in the midline, for example, lingual thyroid (27,28). Ectopic thyroid, which is located lateral to the midline, is extremely rare (29 –31). Failure of a lateral anlage to fuse with the median anlage results in a laterally located ectopic thyroid (28). They are usually found in the submandibular area (32 –39). In patients with a nodular goiter, some nodules can detach from the main thyroid gland. Many remain connected to the main thyroid gland by a vascular pedicle. The detached nodule is usually located on the same facial plane, and is supplied by the same blood vessel. It is not associated with lymph nodes and has an identical histology to the nodule in thyroid gland (14). The detached nodules are usually singular and located deeper when compared to ITC after surgery (40,41).
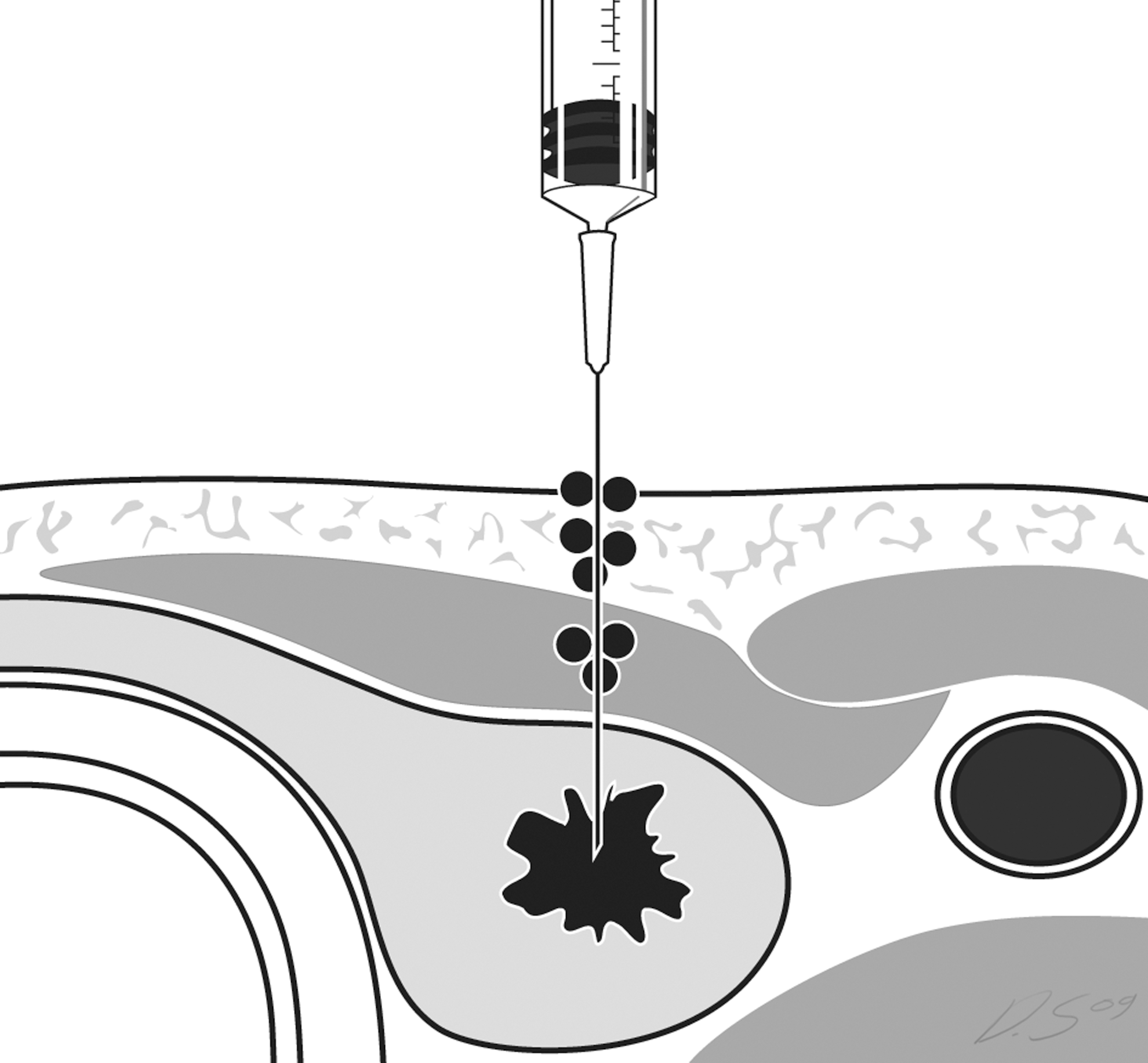
Diagram of implantation of thyroid cells after fine-needle biopsy.
Treatment
ITC from thyroid cancer can be removed by surgery without risk of recurrence, therefore not affecting the application of FNB at thyroid cancer (5). ITC after surgery of a benign thyroid lesion is generally not a serious medical condition. As it is usually located in subcutaneous layer and so is easily palpable, it is a source of anxiety for patients and their physicians. In most reports, the implanted nodules were excised (7). Treatment of ITC is difficult, however, because the surgery is performed at a site of previous malignancy, and therefore there is alteration of tissue planes (13). Radioiodine therapy may be effective if the implanted nodules have radioactive iodine avidity (13).
Prevention
ITC after FNB
ITC usually occurs after using 23-gauge or larger needles. There was one patient in whom it occurred using a 25-gauge needle (Table 3). Twenty-five- to 27-gauge needles are best used for FNB (42) and may avoid ITC, especially for larger thyroid nodules. An effort to decrease the number of needle punctures should also be made. Needles should be pulled back evenly and without creating positive pressure, which is likely to inject cells (2,11). Piston-like motions of the biopsy needle should also be avoided to protect extrathyroidal areas such as the trachea and esophagus (5). These recommendations are logical but controlled studies have not been performed.
ITC after surgery
To prevent ITC after conventional surgery, a lobectomy for all thyroid nodules rather than nodulectomy or partial lobectomy should be performed (13). For procedures on benign thyroid nodules that are larger than 4 cm, conventional surgery rather than endoscopic surgery should be considered. If endoscopic surgery is performed on these larger nodules, the surgeon should take great care to avoid rupturing the tumor (7). Although extraction of the thyroid lobe through a small skin incision could result in spillage of thyroid cells during endoscopic thyroid lobectomy, there is no additional risk of cell seeding in patients who undergo video-assisted thyroidectomy if the procedure is performed correctly (43).
Illustrative Patient
A 73-year-old woman presented with a palpable anterior neck mass. She had been found to have follicular neoplasm in March 1999 and with adenomatous hyperplasia in April 2002 and August 2004 based on ultrasound-guided FNB (US-FNB) at our institution. Neck US detected mixed echoic masses in the thyroid without interval changes since March 1999 and newly developed several subcutaneous nodules in the midline at May 2006 (Fig. 2; arrows). The intervals from the first, second, and third FNB to detection of subcutaneous nodules were 86, 49, and 21 months, respectively. Computed tomography revealed multiple masses in both thyroid glands and subcutaneous nodules in the midline (Fig. 3; arrows). US-FNB was performed from a right thyroid mass and a subcutaneous nodule and diagnosed as adenomatous hyperplasia of the thyroid mass and benign from a subcutaneous nodule. Chest X-ray revealed multiple well-defined nodules in both mid and lower lung fields. Whole-body fluorodeoxyglucose positron emission tomography showed marked uptake in the thyroid gland and both lungs. Lung aspiration biopsy showed metastasis from follicular thyroid carcinoma. Subsequent total thyroidectomy confirmed widely invasive follicular carcinoma. The subcutaneous nodules were diagnosed ITC on histopathology after being diagnosed as benign on FNB (Fig. 4; 15×, black arrows). This was based on the fact that the removed subcutaneous nodules did not include any components of lymph node metastasis on pathological examination and were located the biopsy line between skin and thyroid nodule (Fig. 1).
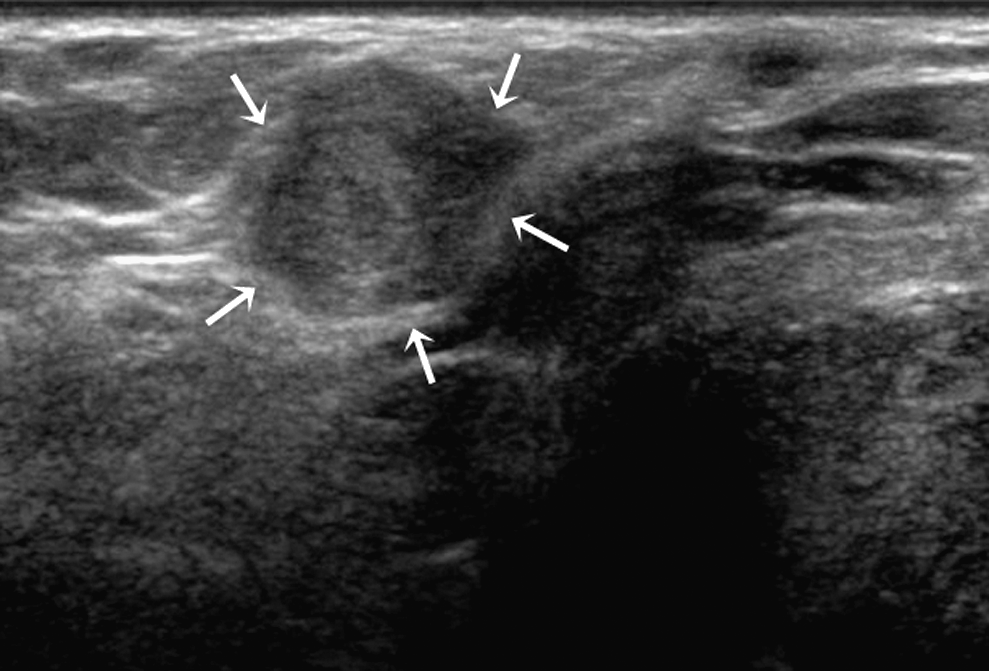
Neck ultrasound showed several subcutaneous nodules (arrows) in the midline.
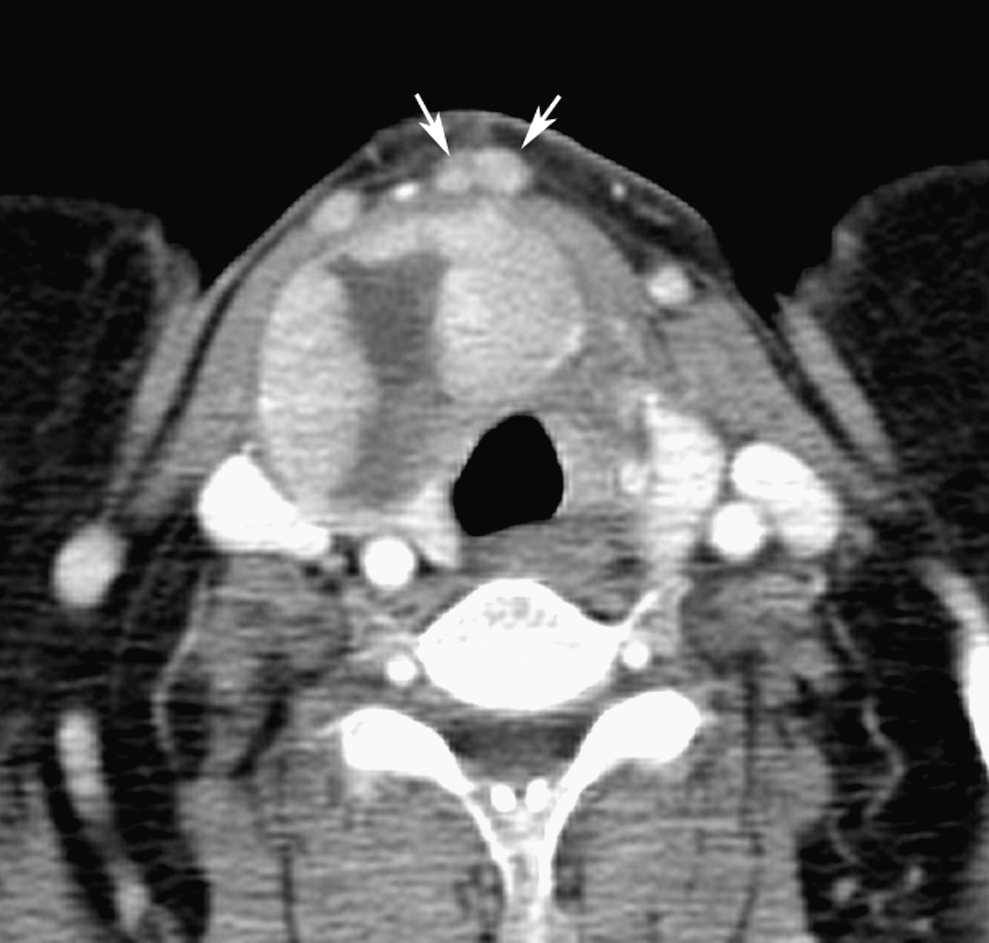
Computed tomography scan revealed multiple masses in the thyroid gland and subcutaneous nodules (arrows) in the midline.

The subcutaneous nodules were removed with the skin and diagnosed as implantation of thyroid cells after fine-needle biopsy (15×, Papanicolaou staining, black arrows).
Conclusions
ITC after FNB or thyroid surgery for benign or malignant thyroid nodules is extremely uncommon. Aggressive characteristics of malignant tumors increase the risk for ITC. Despite the relatively low risk, precautions should always be considered. ITC is very rare with needles smaller than 23 gauge. Some authorities suggest the use of gentle suction and release suction during extraction and a reduced number of passes based on entirely theoretical grounds. In conventional surgery, a lobectomy for all thyroid nodules rather than nodulectomy or partial lobectomy should be performed. If endoscopic surgery is performed on larger nodules, the surgeon should take great care to avoid rupturing the tumor.
Footnotes
Acknowledgment
The authors are grateful to Dong-Su Jang (Medical Illustrator, Medical Research Support Section, Yonsei University College of Medicine, Seoul, Korea) for his help with the illustrations.
Disclosure Statement
The authors declare that no competing financial interests exist.