
Abstract
Background:
Treatment of multinodular goiters (MNGs) is highly controversial. Radioiodine (RAI) therapy is a nonsurgical alternative for the elderly who decline surgery. Recently, recombinant human thyrotropin (rhTSH) has been used to augment RAI uptake and distribution. In this study, we determined the outcome of 30 mCi RAI preceded by rhTSH (0.1 mg) in euthyroid (EU) and hyperthyroid (subclinical/clinical) patients with large MNGs.
Methods:
This was a prospective cohort study. Forty-two patients (age, 43–80 years) with MNGs were treated with 30 mCi RAI after stimulation with 0.1 mg of rhTSH. Patients were divided into three groups, according to thyroid function: EU (n = 18), subclinically hyperthyroid (SC-H, n = 18), and clinically hyperthyroid (C-H, n = 6). All patients underwent a 90-day low-iodine diet before treatment, and those with clinical hyperthyroidism received methimazole 10 mg daily for 30 days. Serum TSH, free thyroxine (FT4), total triiodothyronine (TT3), and thyroglobulin were measured at baseline and at 24, 48, 72, 168 hours, and 1, 3, 6, 9, 12, 18, 24, and 36 months after therapy. Thyroid volume was assessed by computed tomography at baseline and every 6 months.
Results:
Patients had high iodine urinary excretion (308 ± 108 μg I/L) at baseline. TSH levels at baseline were within the normal range (1.5 ± 0.7 μU/mL) in the EU group and suppressed (<0.3 μU/mL) in the SC-H and C-H groups. After rhTSH, serum TSH peaked at 24 hours reaching 12.4 ± 5.85 μU/mL. After RAI administration, patients in both hyperthyroid groups had a higher increase in FT4 and TT3 compared with those in the EU group (p < 0.001). Thyroglobulin levels increased equally in all three groups until day 7. Thyroid volume decreased significantly in all patients. Side effects were more common in the SC-H and C-H groups (31.4% and 60.4%, respectively) compared with EU patients (17.8%). Permanent hypothyroidism was more prevalent in the EU group (50%) compared with the SC-H (11%) and C-H (16.6%) groups.
Conclusions:
Patients with MNG may have subclinical and clinical nonautoimmune iodine-induced hyperthyroidism. Despite a low-iodine diet and therapy with methimazole, hyperthyroid patients have a significantly higher increase in FT4 and TT3 levels after RAI ablation. This can lead to important side effects related mostly to the cardiac system. We strongly advise that patients with SC-H and C-H be adequately treated with methimazole and low-iodine diet aiming to normalize their hyperthyroid condition before rhTSH-stimulated treatment with RAI.
Introduction
Treatment of patients with MNG is highly controversial. Surgical removal of large goiters carries surgical and anesthetic risks especially in the elderly. Cardiovascular disorders, such as arrhythmias, are also frequent in these patients, and can represent additional surgical risks (1,2). As a noninvasive treatment alternative, radioiodine (RAI) therapy leads to significant thyroid volume reduction as well as correction of the hyperthyroid state (8 –12). However, iodine 131 (131I) uptake by the MNG has been shown to be relatively low and not uniformly distributed among the various nodules (12). Therefore, high amounts of RAI are necessary to achieve effective results. The use of recombinant human thyrotropin (rhTSH) has been shown to increase the amount and homogeneity of RAI uptake within MNGs (13). Trials evaluating the use of rhTSH before RAI therapy in patients with MNG have shown promising results. Some groups have used relatively high doses of rhTSH in single and double injections (14 –21), which may transiently exacerbate posttherapeutic hyperthyroidism. Others (15–16) have utilized 131I activity calculation, a method that could prove impractical in many settings. One study has evaluated the administration of RAI on an outpatient basis using a fixed activity of 30 mCi of 131I (22). However, comparison between these studies is difficult because of different methods in assessing goiter volume (ultrasonography vs. computed tomography [CT]) and different follow-up periods (6‱12 months) (23). Moreover, the impact of hyperthyroidism compared with euthyroidism in MNG patients receiving rhTSH-stimulated RAI therapy has not been addressed. In this study, low-iodine diet and methimazole treatment were instituted to minimize the adverse effects of the predictable thyroid hormone elevation after RAI therapy.
We aimed at evaluating the long-term outcome of rhTSH as an adjuvant to RAI therapy administered on an outpatient basis for euthyroid (EU) and hyperthyroid elderly patients with large MNGs.
Patients and Methods
The analysis included 42 patients (41 women) with a mean age 61.4 ± 11.2 years. MNG was diagnosed by palpation, and confirmed by ultrasonography and noncontrast CT scan. A random urine sample was collected for evaluation of iodine concentration, and blood was drawn for assessment of TSH, free thyroxine (FT4), and total triiodothyronine (TT3) levels as well as thyroglobulin (TG), and thyroid autoantibodies. According to thyroid laboratory tests, patients were subdivided into three groups: (i) EU (euthyroid patients with normal serum TSH and FT4 levels, n = 18; (ii) SC-H (patients with subclinical hyperthyroidism, with suppressed serum TSH and normal serum FT4 levels, n = 18); and (iii) C-H (patients with clinical hyperthyroidism, with suppressed serum TSH and elevated serum FT4 levels, n = 6). A detailed cardiologic evaluation was conducted by clinical examination, electrocardiogram, Doppler echocardiography, and 24-hour Holter monitoring as previously described (22). Baseline RAI uptake was determined 24 hours after oral administration of 0.5 MBq (14.0 μCi) of 131I. All patients were instructed to follow a low-iodine diet for 90 days before treatment. Patients with overt hyperthyroidism were treated with methimazole 10 mg a day for 1 month. A second tracer activity of 0.5 MBq (14.0 μCi) of 131I was administered 15 days before a therapeutic activity of RAI and after stimulation with 0.1 mg of rhTSH RAI, 24-hour RAI uptake was carried out. Fine-needle aspiration biopsy was performed in dominant and/or suspicious nodules on ultrasonography to exclude malignancy. Patients were recommended for treatment if presenting symptoms of cervical compression, airway compromise, cosmetic discomfort, and presence of subclinical or overt hyperthyroidism.
The study was approved by the Standing Committee for Ethics in Research Projects of Hospital das Clínicas, University of São Paulo Medical School. All patients signed an informed consent form and were instructed about the 36-month follow-up period of the study.
Treatment protocol
Flasks containing 0.9 mg of rhTSH (Thyrogen®; Genzyme Transgenics, Cambridge, MA) were diluted in 9 mL of isotonic sodium chloride solution; 1 mL of this solution (0.1 mg of rhTSH) was injected intramuscularly 24 hours before the RAI activity.
Twenty-four hours after intramuscular injection of 0.1 mg rhTSH, a fixed single oral activity of 30 mCi of 131I (1.1 GBq) was administered on an outpatient basis. This activity is the maximum radioactivity allowed on an outpatient basis in Brazil. Subsequently, the three groups of patients were followed for 36 months as detailed below.
Thyroid function tests
After RAI therapy, blood samples were collected during short-term (24, 48, 72, 168 hours, and 1 month) and long-term (3, 6, 9, 12, 18, 24, and 36 months) follow-up for evaluation of thyroid status (TSH, FT4, TT3, and TG), as well as to detect the presence of thyroid autoantibodies (anti-thyroid peroxidase [TPO], anti-TG, and TSH-receptor antibody [TRAb]). Serum TSH (normal range, 0.4‱4.0 μU/mL), FT4 (0.9‱1.7 ng/dL), TT3 (90‱180 ng/dL), TG (0.1‱15 ng/mL), anti-TPO (<60 U/mL), and anti-TG antibodies (<60 U/mL) were assayed by chemiluminescence (ECLIA; Roche Diagnostics, São Paulo, Brazil). TRAb (<15%) was assayed by Kronus TRAb–coated tube kit (Kronus, Boise, ID). Urinary iodine excretion was estimated using a modified Sandell–Kolthoff method (normal values between 100 and 299 μg/L of urine).
Thyroid volume
Thyroid volume was assessed at each time point with noncontrast CT scan (GE Medical Systems, Milwaukee, WI) using 130 mA, 120 Kvp, and 5 mm collimation with a pitch of 1 from the mandible to the end of the enlarged thyroid gland. Axial images were reconstructed with a standard algorithm, and postprocessing was performed on a commercially available workstation, as previously described (17).
Cardiovascular evaluation
Cardiovascular evaluation was conducted by an independent cardiologist in all patients. Electrocardiogram, two-dimensional Doppler echocardiography with analysis of systolic function (shortening percentage and ejection fraction), diastolic function (isovolumetric relaxation time and ratio), and left ventricular mass were performed. Cardiovascular assessment was repeated by the same examiner and with the same tests between 7 and 15 days after RAI therapy.
Statistical analysis
Values are presented in the text as mean ± standard deviation and in figures as mean ± standard error of mean. The Student paired test was used to analyze variables with normal distribution. Measurements in relation to time were analyzed by analysis of variance with repeated values, using a matrix of regressive correlations of order one for these comparisons. The Mann–Whitney test was conducted to verify the hypothesis of whether clinical and laboratory values at baseline could indicate a higher probability of a given patient developing hypothyroidism after rhTSH and RAI. After the analysis, time points were compared by the multiple comparisons technique of Bonferroni and Dunnett. The Spearman correlation test was also employed for some variables (thyroid volume, TG), where a p-value < 0.05 was considered significant.
Results
Results are shown in Tables 1 –3 and Figures 1 –3.

Note the increase in serum TSH after rhTSH administration. Subsequently, after 3 months, elevated serum TSH indicates the presence of permanent hypothyroidism in a variable proportion of patients.
(
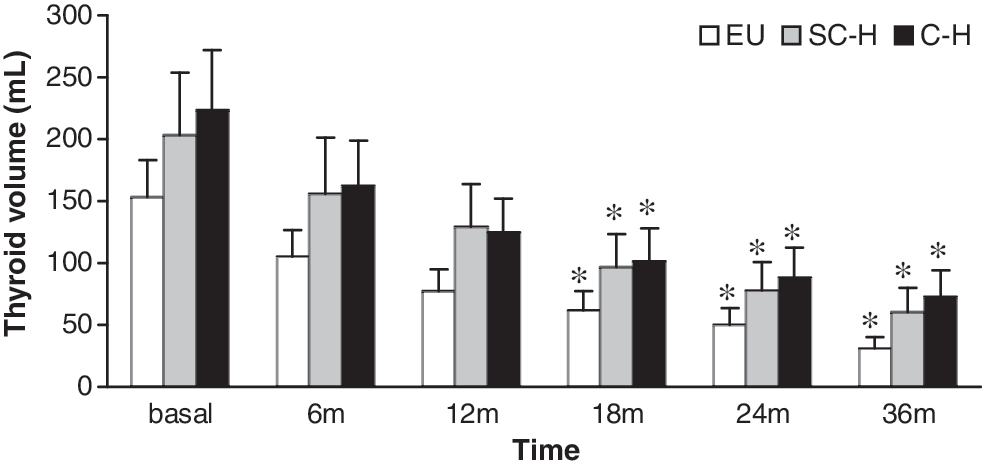
A progressive decrease in thyroid volume (assessed by computed tomography) was noted in the three groups. EU patients had a significantly higher reduction in goiter size compared with those of hyperthyroid patients (*p < 0.01).
After stimulation with 0.1 mg rhTSH.
RAI, radioiodine; TSH, thyrotropin; rhTSH, recombinant human TSH; FT4, free thyroxine; TT3, total triiodothyronine; TG, thyroglobulin; SD, standard deviation.
After stimulation with 0.1 mg rhTSH.
Atrial fibrillation was detected 2–4 weeks after rhTSH + RAI.
Permanent hypothyroidism was confirmed and treated with levothyroxine.
SC-H, subclinically hyperthyroid; C-H, clinically hyperthyroid.
Baseline
Twenty-four-hour 131I uptake and distribution
Administration of 0.1 mg of rhTSH increased 24-hour 131I uptake from 26.8 ± 14.4% to 44.8 ± 14.0% (p < 0.0001) without significant differences among groups of patients. A comparison between pre-rhTSH and post-rhTSH scintigraphic patterns showed greater increase of RAI concentration in stimulated nodules, resulting in a more homogeneous scan, as previously demonstrated (13).
Urinary excretion of iodine
At baseline, most patients (73%) had elevated urinary iodine concentration (308 ± 108 μg I/L, range 168‱642 μg/L). After 90 days of low-iodine diet, mean urinay iodine concentrations decreased to 165 ± 98 μg/L (p < 0.01). There were no significant differences in urinary iodine excretion before and after low-iodine diet between the three groups of patients.
Thyroid volume
Mean thyroid volume by ultrasonographic evaluation was 128.8 ± 109.2 mL, and by CT, 184.0 ±168.2 mL (p = 0.001). Since ultrasonography had limited ability to estimate the volume of retrosternal portions of the goiters, we decided to assess goiter volume only by CT scan over the subsequent 36-month period.
Thyroid function tests
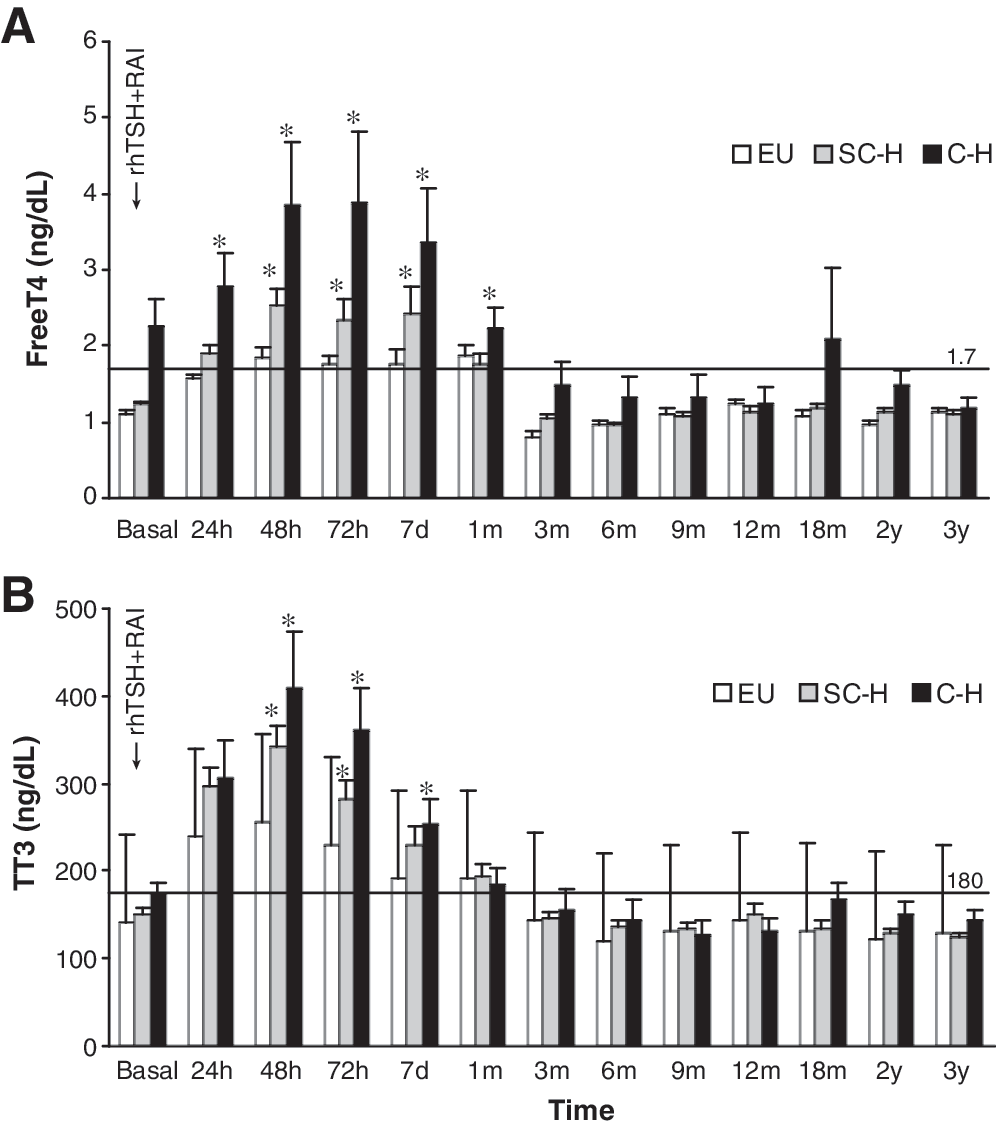
At baseline, mean serum TSH levels were 1.34 ± 0.74 μU/mL in the EU group, 0.27 ±0.23 μU/mL in the SC-H group, and 0.04 ± 0.02 μU/mL in the C-H group. Hyperthyroid patients had significantly lower serum TSH concentrations compared with those with euthyroidism (p < 0.001). After rhTSH administration, there was an elevation in TSH levels for 24–48 hours that was similar in all three groups (Fig. 1). Mean FT4 level at baseline was 2.27 ± 0.83 ng/dL and was significantly higher in the C-H group (p = 0.001) when compared with that of the other two groups (Fig. 2A). TT3 concentrations at baseline (Fig. 2B) were similar in all three groups: 140 ± 48 ng/dL in the EU group, 150 ± 29 ng/dL in the SC-H group, and 174 ± 32 ng/dL in the C-H group. TG was equally elevated in all three groups, as expected for patients with large goiters (EU = 342 ng/mL, SC-H = 447 ng/mL, and C-H = 429 ng/mL). A positive and significant correlation was seen between TG levels and goiter volume (r = 0.569, p < 0.01). TRAb was negative in all patients, and two patients had low positive values for both anti-TPO and anti-TG autoantibodies.
Cardiovascular evaluation
Systemic hypertension was present in 21 patients, and 9 had concomitant type 2 diabetes mellitus. One patient in the EU group underwent coronary bypass surgery 3 years before enrollment. None of the patients presented abnormal cardiac signs or symptoms on clinical examination or electrocardiogram. Doppler echocardiography evaluation was performed in 39 patients at baseline (EU = 16, SC-H = 17, and C-H = 6). Mild aortic, mitral, and tricuspid regurgitation were observed in eight patients (SC-H = 4 and C-H = 4). Holter monitoring was performed in 27 patients (EU = 14, SC-H = 10, and C-H = 4). Sinus rhythm was present in 25, and atrial fibrillation was detected in 2 patients (SC-H = 1 and C-H = 1).
Posttreatment
As mentioned previously, serum TSH increased similarly in all the three groups 24 to 48 hours after rhTSH administration and returned to normal values at 72 hours and 30 days after RAI ablation (Fig. 1). In the following months, there was a marked increase in TSH levels (more evident in the EU group), suggesting the onset of RAI-induced hypothyroidism (Fig. 1). All three groups presented elevation in both FT4 (Fig. 2A) and TT3 (Fig. 2B) after RAI. Until day 7, levels of FT4 and TT3 were significantly higher in both groups of hyperthyroid patients when compared with the EU group (Fig. 2A, B). Peak levels of FT4 were reached at 72 hours (2.53 ±0.91 ng/dL in the SC-H group and 3.88 ± 2.27 ng/dL in the C-H group). Of note, patients in the C-H group presented persistently elevated levels of FT4 up to 1 month after RAI treatment (2.22 ± 0.67 ng/dL).
Goiter volume after RAI
A progressive reduction in the volume of the thyroid was observed in all the three groups, as shown in Figure 3. However, after only 18 months the difference from the baseline volume was significant in all the three groups (p < 0.001). At 36 months, the mean goiter volume was 31.5 ± 34 mL in the EU group, 60.3 ± 73 mL in the SC-H group, and 72.8 ± 48 mL in the C-H group. Patients in the EU group had a significantly higher reduction in thyroid volume when compared with the two hyperthyroid groups (p < 0.01).
Adverse effects
Side effects of RAI ablation were more common in the two groups of hyperthyroid patients (Table 3). Remarkably, 31.4% of the patients in the SC-H group and 60.4% in the C-H group had at least one important side effect that required medical intervention compared with 17.8% of the patients in the EU group. Enlargement of the goiter and local tenderness were the most frequent and early side effects observed. Tachycardia was present in 13 patients with SC-H and C-H. Atrial fibrillation was observed 2–4 weeks after rhTSH and RAI in four patients in the SC-H and C-H groups, and was controlled with propranolol. Two of these patients had cardiac arrythmia in the past. Permanent hypothyroidism, however, was significantly more prevalent in the EU group (50%) when compared with the SC-H (11%) and C-H (16.6%) groups. Hypothyroid patients were subsequently treated with levothyroxine.
Discussion
Programs of table salt iodination instituted in iodine-deficient regions of Brazil before 1995 were unsuccessful in most rural areas because of irregular purchase of potassium iodate by salt mills, lack of cooperation among salt producers, and absence of an efficient general surveillance (4,5). After universal table salt iodination was implemented in 1995 and potassium iodate was delivered free of charge to all salt mills by the Brazilian Health Authorities, a tighter control of table salt iodination was introduced, enforcing a legal range of 40–100 mg of iodine per kg of salt (40‱100 ppm). Until 2004, when this relatively high iodine content in the salt was lowered to 20–60 ppm, the Brazilian population was exposed to excessive nutritional iodine (6,7,24). A large segment of the elderly population who lived in rural areas with chronic iodine deficiency developed large MNGs over the years and became at risk for subclinical and overt hyperthyroidism as well as cardiac arrhythmias secondary to iodine-induced hyperthyroidism.
Hyperthyroidism secondary to iodine, either in its subclinical (suppressed TSH, normal FT4 levels) or clinical (overt) form may be transient and self-limited in a number of patients (25). Patients with large MNGs, however, have a more prolonged and possibly more clinically important form of hyperthyroidism, frequently with repercussions to the cardiovascular system (25). This segment of elderly patients is considered poor surgical candidates. RAI therapy is a reasonable alternative for this population and results in a mean thyroid volume reduction of approximately 40% of the original MNG size 1 year after treatment (23).
Most patients with large goiters attending our clinics have relatively low RAI uptake by the thyroid and need a large amount of 131I to effectively reduce the volume of the goiter. rhTSH approximately doubles thyroid 131I uptake in patients with MNG as well as helps distribute the tracer homogeneously throughout the various nodular compartments. Several reports have evaluated the efficacy of rhTSH-stimulated 131I therapy on goiter size reduction as recently reviewed (23,26). In our previous report (17), we analyzed the effects of a relatively high dose of rhTSH (0.45 mg) along with high, nonfixed therapeutic activities of 131I (50‱150 mCi, 2.75‱5.50 GBq) in a selected group of patients. Because of the elevated radiation activity, these patients were hospitalized and presented a high prevalence of side effects within the first few weeks after treatment, including hyperthyroidism, radiation thyroiditis, esophagitis, and enlargement of the goiter. Long-term hypothyroidism was a common adverse effect seen in 64% of these patients (17).
In the present study, which aimed at observing the short-term and long-term side effects of combined treatment with RAI and rhTSH, a lower dose of rhTSH (0.1 mg) was used 24 hours before a fixed RAI activity of 30 mCi (1.11 GBq) that was administered on an outpatient basis, as legally permitted in Brazil. This approach has reduced considerably the therapeutic costs of patients with large MNGs.
We took special care in reducing the risk of iodine-induced hyperthyroidism by instituting a low-iodine diet for at least 90 days before RAI therapy. In fact, the relatively high urinary iodine excretion (which reflects a high dietary iodine intake) was significantly reduced by the end of the low-iodine diet period. In spite of a relatively low nutritional iodine intake, approximately 57% of our patients had suppressed serum TSH at baseline with subclinical and overt hyperthyroidism (group SC-H and C-H). Six patients with overt hyperthyroidism were treated with methimazole before rhTSH and RAI therapy. Cardiological examination before RAI was mostly normal, although Holter monitoring identified two patients with cardiac arrhythmia. Moreover, recent studies have observed no serious cardiovascular side effects in EU patients with MNG who receive rhTSH (21,22). As recently stated by Fast et al. (26), “the rise in thyroid hormones seems to be of little clinical relevance when limiting rhTSH to 0.1 mg or less.”
We decided to compare the early follow-up period (days 1‱30) and the prolonged follow-up (3‱36 months) in patients categorized at baseline as EU, and compare clinical and laboratory data with two other groups of patients, one with subclinical and the other with clinical hyperthyroidism. The two latter groups had a significantly higher increase in FT4 and TT3 when compared with the EU group in the first 7 days post-RAI. Also, the group with clinical hyperthyroidism maintained the excessive output of thyroid hormone for up to 30 days after RAI treatment. Consequently, patients in both hyperthyroid groups had higher prevalence of cardiac abnormalities (tachycardia and arrhythmia) compared with the EU group. Both hyperthyroid groups also had a higher prevalence of local side effects (goiter enlargement, tenderness, tracheitis, and difficulty in swallowing) compared with EU patients. Obviously, the use of low-iodine diet for 90 days and the short course of Methimazole (10 mg q.d.) were not enough to render the hyperthyroid patients a safe clinical condition preceding the RAI therapy preceded by rhTSH. Therefore, we strongly advise that in similar future studies a new protocol providing a prolonged low-iodine diet should be instituted. Moreover, for overt hyperthyroid patients, methimazole therapy is suggested to be 15 mg q.d. for 2–3 months to render the overt hyperthyroid patients to euthyroidism as well as to deplete the thyroid gland of stored hormone. On a later follow-up, however, the EU group had a higher prevalence of permanent hypothyroidism. This may be the reflection of normal serum TSH at baseline that would favor a better uptake of the radionuclide by the MNG.
The hyperthyroid state that follows RAI administration is potentially dangerous in the elderly. Recently, Magner (27) described a fatal outcome of a hyperthyroid woman who was treated with RAI preceded by rhTSH. In our patients with SC-H and C-H, the 90 days of low-iodine diet did not seem to prevent the elevation in FT4 and TT3 levels after RAI administration. Moreover, the use of methimazole in the C-H group had no apparent effect in the severity of the hyperthyroid period after RAI administration. Thyroid volume decreased in all three groups of patients, and the prolonged follow-up period was uneventful, except for a progressive number of patients who developed permanent hypothyroidism, mostly in the EU group.
In conclusion, the protocol for treating SC-H and overt hyperthyroid patients with MNG should be adequately modified. A more prolonged methimazole (MMI) treatment with 15 mg q.d. for at least 2 months in parallel to low-iodine diet would be required. All patients should be in EU condition before rhTSH-stimulated treatment with RAI.
Footnotes
Acknowledgments
This work was supported by a grant from FAPESP 02/06892-6 (State of São Paulo Research Foundation) and by a partial grant from Instituto da Tiroide, São Paulo, Brazil. We are grateful to Carlos Buchpiguel, M.D. (Nuclear Medicine), for the RAI treatment and Eloisa Gebrin, M.D. (Department of Radiology), for the CT scan analyses. Urinary iodine excretion was assayed by Ana Luiza Galrão.
Disclosure Statement
The authors declare that no competing financial interests exist.