
Abstract
Background:
Papillary thyroid cancer (PTC), the most prevalent type of differentiated thyroid carcinoma, displays a strikingly high frequency of lymph node metastasis (LNM). Recent data suggest that chemokines can play an important role in promoting tumor progression and metastatic migration of tumor cells. Here we have evaluated whether PTC tissues express a different pattern of chemokine receptors and if the expression of these receptors correlates with LNM.
Methods:
We assessed by immunohistochemistry and flow cytometry the expression of the chemokine receptors CCR3, CCR7, and CXCR4 in tumor and nonmalignant thyroid tissues from patients suffering from PTC. Expression of these receptors in PTC was correlated with the clinical pathological condition of PTC.
Results:
Our data show a significant enhancement of CCR3 (2.5 times higher, p = 0.038) and CXCR4 (1.7 times higher, p = 0.02) expression in PTC tissues as determined by immunohistochemical staining, and of CCR3 (3.5 times higher, p < 0.002) in the plasma membrane as determined by flow cytometric analyses, compared to controls. In addition, while CCR3 (100%) and CXCR4 (90%) were present in both tumor and control thyroid tissues, expression of CCR7 was scarcely detected in PTC cells (5–10%) and not found in control cells. CXCR4 expression correlated with the classical variant of PTC (p < 0.035) and extranodal extension (p < 0.010) in patients with LNM.
Conclusions:
Our data support the notion that CCR3, CCR7, and CXCR4 are increasingly expressed in tumor cells from PTC and that CXCR4 expression in PTC could be a potential marker for enhanced tumor aggressiveness.
Introduction
The high frequency of LNM in PTC contrasts with the low frequency of hematogenous dissemination, suggesting preferential metastatic spread via the lymphatic pathway. Nevertheless, until now, the factors regulating the metastatic process in PTC remain poorly understood. Recently, it has been shown that chemoattractant molecules secreted from target organs and the specific pattern of chemoattractant receptors expressed on tumors cells can define the destination of tumor metastases (12). Therefore, the selective trafficking of PTC metastases to lymph nodes could be a result of a particular expression of chemoattractant receptors by PTC cells. Hence, expression of those chemoattractant receptors could promote the migration of tumor cells in response to a gradient of chemoattractant molecules derived from lymph nodes. The identification of these molecules and their receptors could be considered as markers for those PTC that are more likely to undergo LNM. Candidates for chemoattractant receptors are chemokine receptors. Chemokines contribute to the development and progression of cancer (13,14) and tumor metastasis (12,15,16). Chemokines are a family of about 50 chemotactic proteins (8‱10 kDa) classified into four highly conserved groups—CXC, CC, C, and CX3C—based on the position of their first two cysteines adjacent to the amino-terminus (17 –19). These molecules stimulate cell movement during inflammation, as well as the homeostatic transport of hematopoietic stem cells, lymphocytes, and dendritic cells (20 –22). The activity of chemokines is mediated by their binding to a large family of seven-transmembrane G protein–coupled receptors (18 in humans) (23), which promote receptor internalization (24,25) and the signaling leading to the transcription of genes required for cell motility, invasion, interaction with the extracellular matrix, and cell survival (17,24 –26).
Altered expression of chemokine receptors has been reported in several tumors, including breast cancer (12), malignant melanoma (27,28), lung cancer (29), and squamous cell carcinoma of the head and neck (30). For thyroid cancer, expression of chemokine receptors CXCR4 and CCR7 has been evaluated (31 –33). CXCR4 has been particularly studied due to its previous involvement in tumor growth, survival, and spread to other tissues (32–33). CCR7 is also expressed in thyroid carcinoma cell lines (TPC-1) and thyroid cancer tissues (31,33), which is thought to contribute to tissue invasion and cellular proliferation (31). CCR3 is another receptor associated with development, progression, and aggressiveness of several types of cancer (34,35).
The objective of this study was to evaluate the expression and cellular localization of CCR3, CCR7, and CXCR4 in thyroids of patients suffering from PTC and to determine its correlation with LNM and clinical pathological features. We observed that thyroid cells from PTC patients show an altered expression of chemokine receptors. CCR3, CCR7, and CXCR4 were overexpressed in PTC tissues and always found mainly in the intracellular region of PTC cells. The expression of these three receptors was independent of whether the patient developed LNM or not. However, the expression of CXCR4 correlated with the classical variant of PTC and extranodal extension.
Materials and Methods
Patients and tissue samples
Thirty patients with suspicious thyroid nodules had a confirmed diagnosis of PTC by fine needle aspiration in the Hospital Clínico de la Pontificia Universidad Católica de Chile. All those patients, included in this study, signed a written informed consent approved by the ethical committee of the hospital before they underwent surgery. Preoperative ultrasound staging of the neck determined if the patients had macroscopic LNM. Total thyroidectomy was performed in all patients and lymph node dissection (central compartment or comprehensive) only in those with ultrasonographic evidence of macroscopic adenopathy. Presence of metastasis was defined as patients with macroscopic pathologically confirmed metastasis. Tumor samples and matched nonmalignant tissue (control) were obtained immediately after total thyroidectomy. The control tissue was obtained from the tumor-free contralateral lobe of the same patient from whom the tumor sample was obtained. After surgery, a pathology report was obtained for each patient. Tumor characteristics and staging for each patient are shown in Table 1.
All patients had histologically confirmed papillary thyroid cancer (PTC). F, female; and M, male. The cancer stage classification was according to AJCC TNM staging system, 6th edition. T, primary tumor; N, regional lymph nodes; M, distant metastasis. T1 is a tumor 2 cm or less in greatest dimension limited to the thyroid. T2 is a tumor more than 2 cm but not more than 4 cm in greatest dimension limited to the thyroid. N0, absence of regional lymph node metastasis; N1a, presence of metastasis to level VI (pretracheal, paratracheal, and prelaryngeal lymph nodes); N1b, presence of metastasis to unilateral, bilateral, or contralateral cervical or superior mediastinal lymph nodes. M0, absence of distant metastasis. The histopathology characteristics were classified with + or − according to the presence or absence of the condition, respectively. Multifocal refers to the presence of more than one foci of tumor in the thyroid gland. Invasion of thyroid capsule is the invasion for the tumor cells. Extrathyroidal extension refers to the presence of tumor cells beyond the thyroid capsule with invasion of subcutaneous soft tissue or other local structures. Surgical margin denotes the presence of tumor in the surgical resection margin of the thyroid gland. Vascular invasion is the presence of tumor cells in the blood vessels of the thyroid gland. Extranodal extension implies the presence of proliferating malignant cells outside the capsule of an involved lymph node.
Immunohistochemistry
For immunohistochemistry analyses, fresh thyroid tissues obtained from patients were fixed in 4% paraformaldehyde in 140 mM sodium chloride (NaCl), 3 mM potassium chloride (KCl), 0.01 M sodium phosphate, and 1.8 mM potassium phosphate at pH 7.4 (phosphate buffered saline [PBS]) overnight at 4°C. The tissues were dehydrated using an ethanol and xylol battery. Briefly, tissues were kept in 70% ethanol three times for 20 minutes, 95% ethanol three times for 20 minutes, 100% ethanol three times for 30 minutes, 34% xylol/66% ethanol for 30 minutes, 50% xylol/50% ethanol for 30 minutes, 66% xylol/34% ethanol for 30 minutes, and finally in 100% xylol three times for 30 minutes. The dehydrated tissues were embedded first in 50% xylol/50% paraffin for 1 hour at 56°C, then in 100% paraffin overnight at 56°C, and finally in 100% paraffin for 1 hour at 56°C. The tissues were sliced into 5 μm sections using a microtome (Leica, RM2235; Wetzlar, Hesse, Germany). These thyroid sections were deparaffinized using a battery of alcohols (100% xylol three times for 10 minutes, 100% ethanol three times for 10 minutes, 95% ethanol three times for 2 minutes, and 70% ethanol three times for 2 minutes). The sections were then mounted on silanized microscope slides and rehydrated in 140 mM NaCl, 3 mM KCl, and 20 mM tris at pH 7.4 (tris-buffered saline). The endogenous peroxidase activity in the thyroid sections was blocked using 6% hydrogen peroxide in tris-buffered saline for 15 minutes at room temperature. Nonspecific binding was blocked using a blocking solution (5 mM EDTA, 1% fish gelatin, 1% bovine serum albumin [BSA] IgG free, 2% horse serum) in a wet chamber for 1 hour at room temperature. The thyroid tissue sections were incubated overnight at 4°C with primary specific antibodies prepared in blocking solution diluted 10 times. The primary antibodies used were monoclonal anti-human CCR3 antibody (MAB155, 1:1000 dilution; R&D Systems, Minneapolis, MN), monoclonal anti-human CCR7 (1:250 dilution; R&D Systems), and monoclonal anti-human CXCR4 (MAB173, 1:250 dilution; R&D Systems). The sections were rinsed six times for 5 minutes with blocking solution diluted 10 times and incubated with a secondary biotinylated antibody provided in the LSAB + System-HRP kit (cat. no. K0679) (DakoCytomation, Glostrup, Hovedstaden, Denmark) for 1 hour at 4°C. The sections were washed six times for 5 minutes with blocking solution diluted 10 times.
Immunohistochemistry was revealed by substrate-chromogen solution provided by the DakoCytomation kit. To identify cells and nuclei, tissues were stained with hematoxylin (Merck, Darmstadt, Hesse, Germany). The immunohistochemistry for each antibody was quantified using the Image-Pro Plus program version 6.0 (Media Cybernetic Inc., Bethesda, MD). Briefly, at least three representative pictures of each thyroid tissue section were taken and analyzed with Image-Pro Plus program. The value obtained from each quantification analysis was normalized by the number of nuclei in this picture and was referred as mean intensity value (MIV). To normalize the expression of chemokine receptors in the tumor relative to the matched nonmalignant tissue, the ratio of MIV of tumor tissue to MIV of the match nonmalignant tissue for each patient was calculated. To determine the differences in chemokine receptor expression, an average of the ratio was calculated, referred to as relative expression.
Flow cytometry analysis of CCR3, CCR7, and CXCR4
For flow cytometry analysis, tumor and control thyroid tissue were processed immediately after surgery. Briefly, thyroid tissues were kept in RPMI medium without supplements (cat. no. 31800-89) (Gibco®, Carlsbad, CA) and dissociated manually with a scalpel at room temperature. During this procedure, the adipose and connective tissues were removed from the sample tissue and the latter passed through a syringe (tip G 5/8). The cell suspension obtained was incubated with primary antibodies. For CCR3 detection, a monoclonal anti-human CCR3 antibody (MAB155, 500 μg/mL; R&D Systems) diluted 1:200 and unlabelled streptavidin (S-888, 10 mg/mL; Invitrogen, Carlsbad, CA) diluted 1:500 were used. Cells were centrifuged at 250 g (IEC Centra CL3R, Thermo, Waltham, MA) for 6 minutes and rinsed two times with 3% BSA in PBS (PBS/BSA). Then the cells were incubated with 1.5 mg/mL of an anti-rat biotinylated secondary antibody (BA-4000; Vector, Burlingame, CA) diluted 1:200 for 30 minutes at 4°C. After incubation cells were rinsed with PBS/BSA and incubated with 0.2 mg/mL streptavidin-PerCP (cat. no. 554064; BD Pharmingen, San Diego, CA) diluted 1:300 in PBS/BSA. For CCR7 detection, a monoclonal anti-human CCR7 antibody (MAB197, 500 μg/mL; R&D Systems) diluted 1:100 was used, and an anti-mouse IgG made in goat labeled with R-phycoerythrin (cat. no. 31861; Pierce, Rockford, IL) diluted 1:200 was used as a secondary antibody. For CXCR4 detection, a monoclonal anti-human CXCR4 antibody (MAB172, 500 μg/mL; R&D Systems) diluted 1:100 was used, and an anti-mouse IgG made in goat labeled with R-phycoerythrin (cat. no. 31861; Pierce) diluted 1:200 was used as a secondary antibody. The incubations of cells with antibodies were performed in PBS/BSA for 45 minutes at 4°C. The expression of CCR3, CCR7, and CXCR4 at the cell surface was analyzed on a FACSCalibur (Becton Dickinson Instrument Systems, Sparks, MD). Flow cytometry analysis was performed using the program CellQuest Pro (BD Biosciences, San Jose, CA) and Winmdi 2.8 (Developed by Joe Trotter, available at
Statistical analyses
All statistical analyses were performed using GraphPad Prism version 4.0 (GraphPad Software, San Diego, CA) and SPSS Statistic 17.0 for Windows. The statistical analyses for both immunohistochemistry and flow cytometry were done by Wilcoxon test. Differences between patients with and without LNM was analyzed by the Mann-Whitney test. Correlation of positive staining of CCR3, CCR7, and CXCR4 with clinicopathologic features (Table 2) was done by t-test or Mann-Whitney test depending on whether the samples had normal distribution or not. The Kruskal-Wallis test was used to statistically analyze the stage of disease.
p denotes p-value obtained after t-test or Mann-Whitney test. # denotes the number of patients who have the clinical pathological condition. LNM, lymph node metastasis. * denotes significant differences (p < 0.05). Negative expression was considered when there was no staining for the receptor in the PTC tissue. Positive expression was considered when there was staining in the PTC tissue. **denotes p-value obtained after Kruskal-Wallis test for statistic analysis of all three PTC stages and chemokine receptor immunohistochemical staining.
Results
CCR3 and CXCR4 are overexpressed in PTC
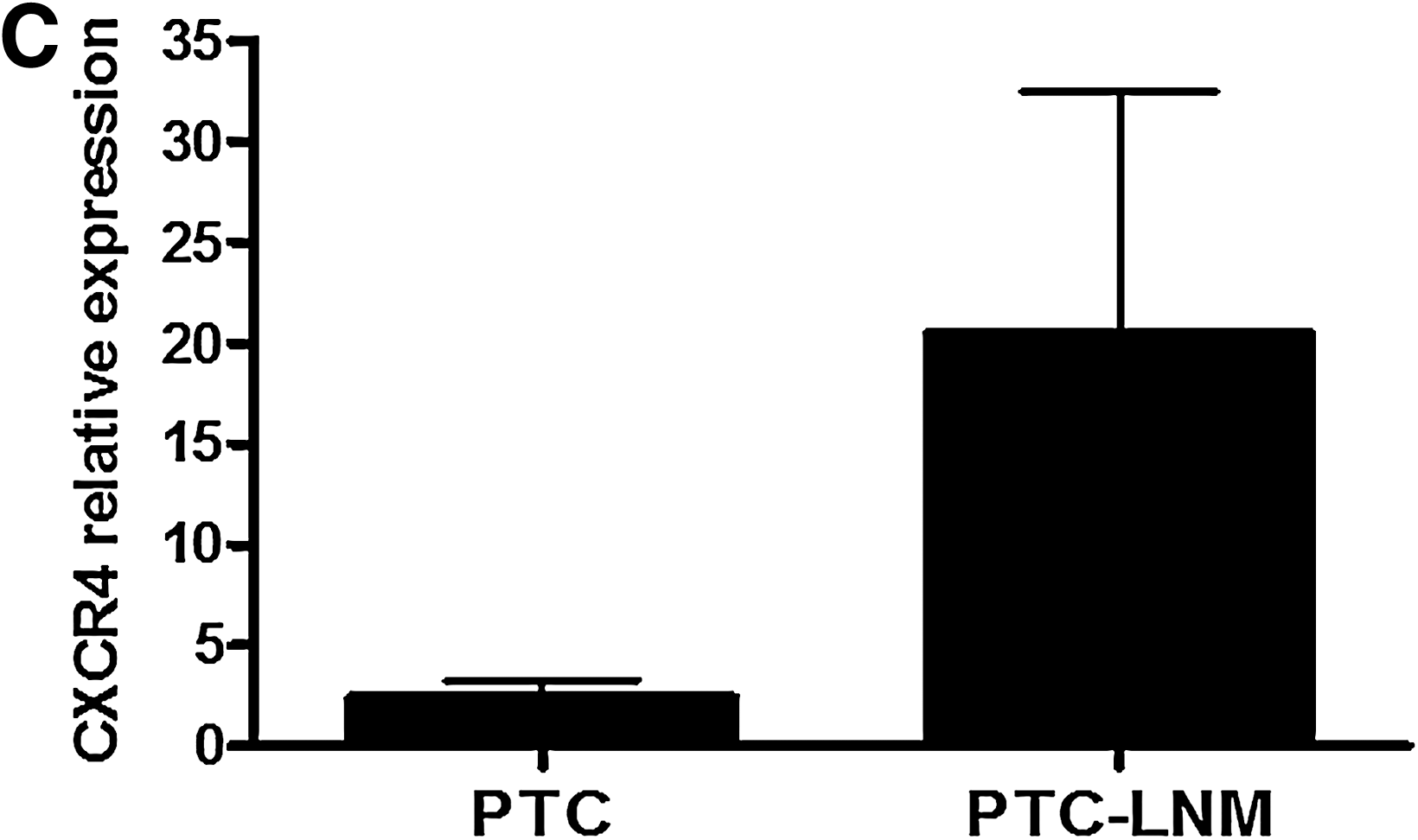
Expression of CCR3, CCR7, and CXCR4 was analyzed in PTC and control tissue by immunohistochemical staining using specific antibodies for these receptors (Fig. 1). CCR3 staining was observed in all tissues, both control and PTC samples (Fig. 1a‱d). Near to 100% of tumor cells in PTC samples stained for CCR3 (Fig. 1c). The intensity of CCR3 staining in all tissues was quantified (see Materials and Methods) and referred to as MIV. The quantitative analysis of CCR3 indicated that its expression was approximately 2.5 times higher in PTC than in control tissues (for control, MIV ± SEM =445.08 ± 124.47; for PTC, MIV ± SEM = 1070.636 ±259.316; p = 0.038, n = 19). Representative slides for CCR7 staining are shown in Figure 1f–i. Staining was detected in one normal thyroid tissue and in seven PTC samples. Even though CCR7 expression was significantly different between PTC and normal tissue (control, MIV ±SEM = 0.378 ± 0.378; PTC, 7.106 ±3.007; p = 0.017, n = 16) (Fig. 1f‱j), it was scarcely detected in thyroid cells from PTC (5‱10% of tumor cells stained for CCR7). Representative slides for CXCR4 staining are shown in Figure 1k–n. Staining was observed in all samples, both control and PTC. CXCR4-derived signal was present in approximately 90% of tumor cells in PTC tissues. CXCR4 staining was significantly higher in PTC than in control tissues (control, MIV ± SEM = 313.68 ± 79.11; PTC, 525.17 ± 84.205; p = 0.02, n = 16) (Fig. 1k‱o). The relative expression of chemokine receptors was compared among patients with and without LNM (Fig. 2 and Table 2). None of CCR3, CCR7, and CXCR4 expression correlated with LNM (Fig. 2). Potential associations between the relative expression of CCR3, CCR7, and CXCR4 seen by immunohistochemical staining and the patients' clinicopathologic features were evaluated (Table 2). While CCR3 and CCR7 expressions were independent of all these clinical features, a positive correlation was found between CXCR4 expression and the extranodal extension in patients with LNM and the classical variant of PTC type.
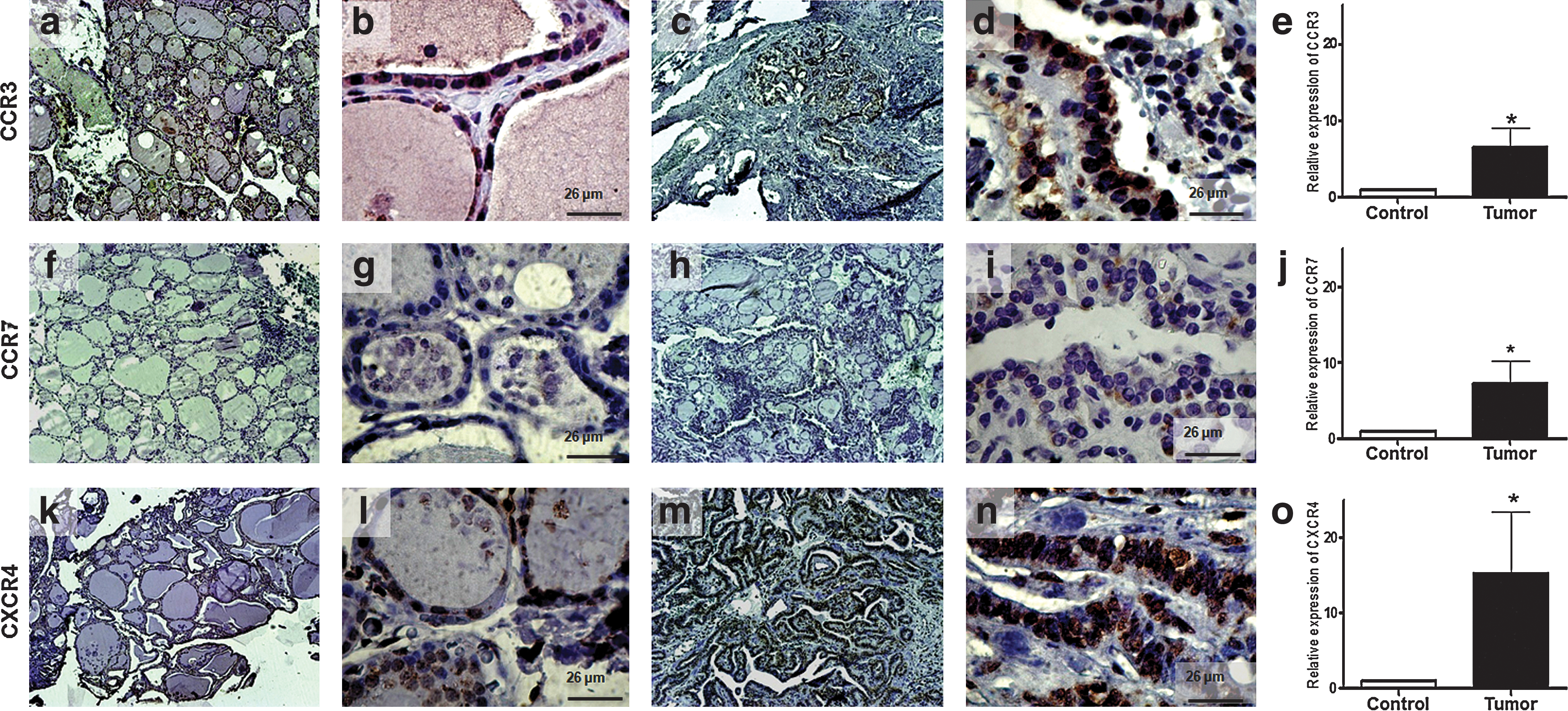
CCR3, CCR7, and CXCR4 show a significantly increased expression in papillary thyroid cancer (PTC). Representative pictures of immunohistochemistry slides show chemokine receptor expression at low (× 10) (
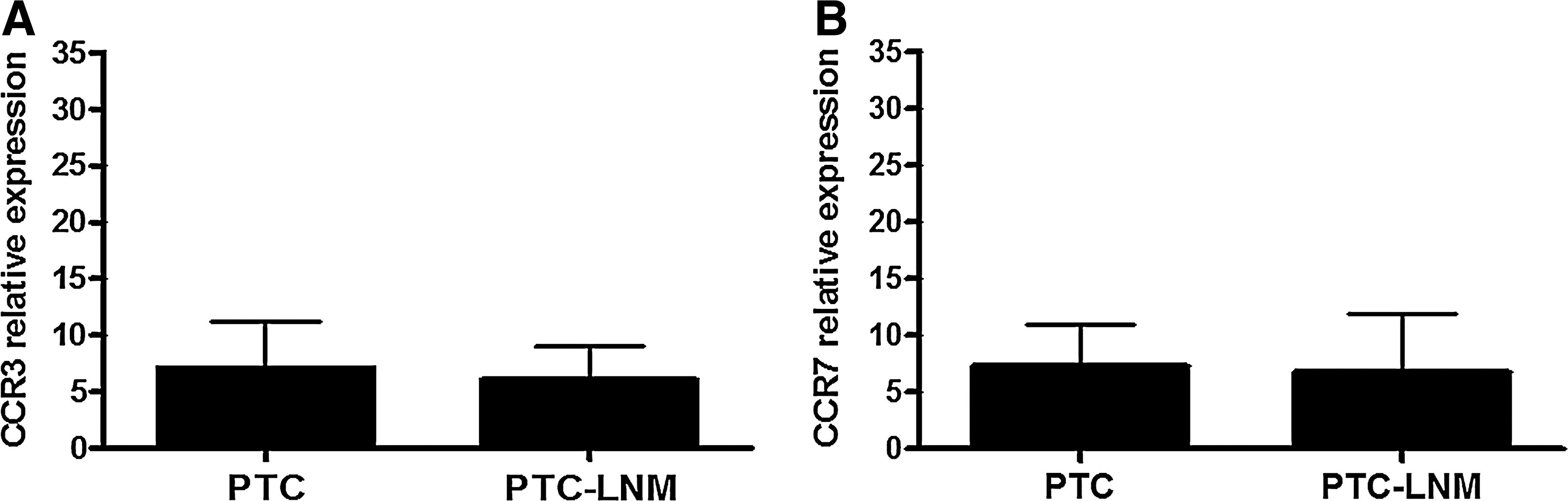
Metastatic PTC shows equivalent CCR3, CCR7, and CXCR4 expression than nonmetastatic PTC. Quantitative analysis for the relative expression of CCR3 (
The qualitative analysis of the immunohistochemical staining for each chemokine receptor showed that all receptors were present mainly in the cytoplasm, in both control and PTC tissues (Fig. 1). We measured by flow cytometry the expression of CCR3, CCR7, and CXCR4 at the plasma membrane of PTC and control cells. Cells from PTC and normal thyroid tissues were prepared as described in Materials and Methods. CCR3 expression at the plasma membrane showed a 3.5-fold increase in PTC cells compared to control cells (Fig. 3A). However, no significant correlation could be demonstrated between CCR3 expression at the cell surface and the patients' clinicopathologic characteristics (data not shown). On the other hand, CCR7 expression at the plasma membrane was similar for PTC and control cells (Fig. 3D). Similarly, surface expression of CXCR4 was equivalent between PTC and control cells (Fig. 3G). Representative histograms for the three receptors in normal cells and PTC are shown (Fig. 3B, C, E, F, H, and I).
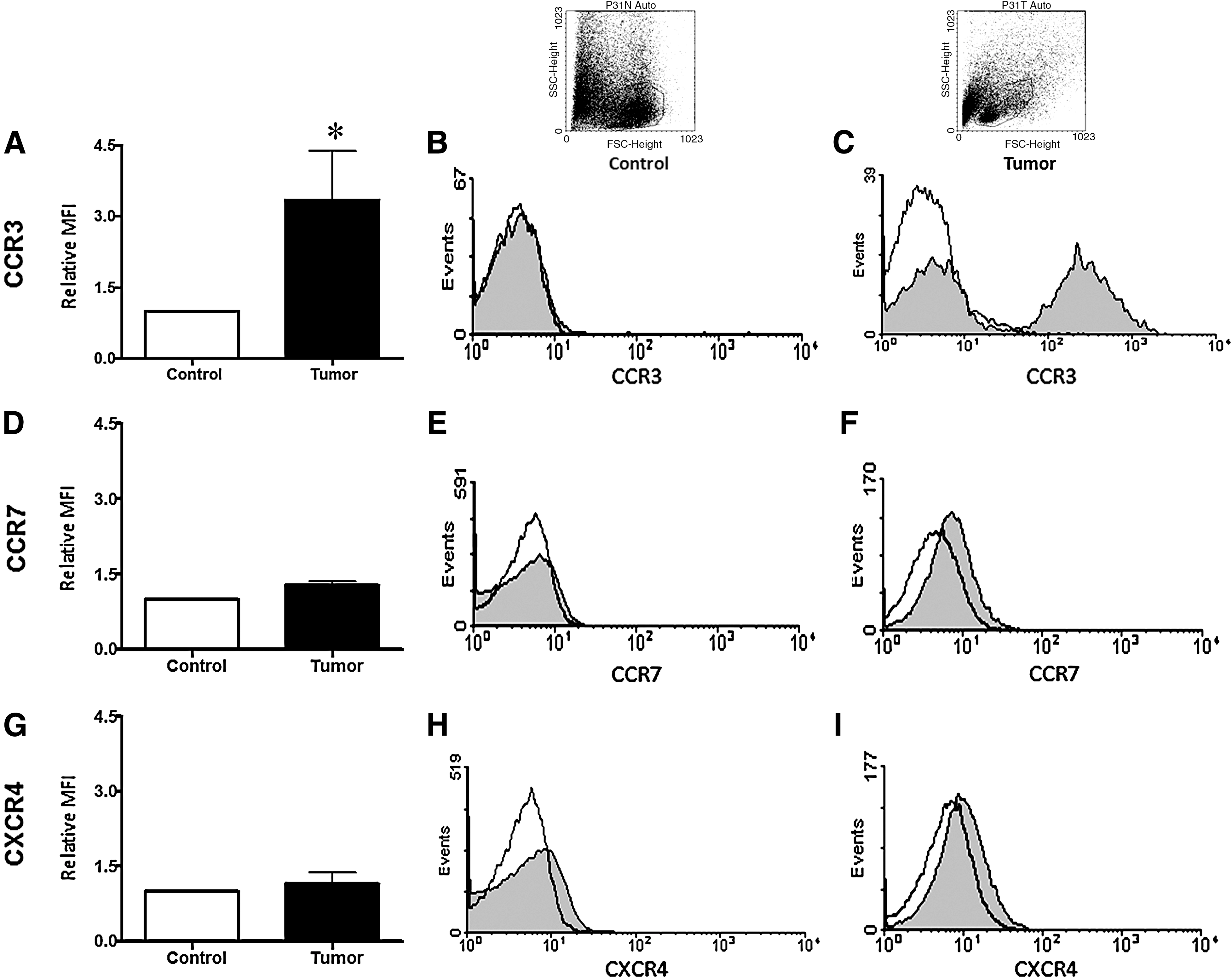
Flow cytometry analysis for CCR3, CCR7, and CXCR4 in PTC. Cell surface expression for CCR3, CCR7, and CXCR4 in control and PTC samples was determined by flow cytometry. The mean fluorescence intensity (MFI) for the three receptors in tumor cells was normalized to the MFI shown by each receptor on the respective control sample, for each patient. The average of these normalized values was calculated, plotted, and referred to as relative MFI. (
Discussion
Chemokines and their receptors contribute to migration and proliferation of malignant cells during metastatic processes (14). Here we have analyzed the expression of three chemokine receptors (CCR3, CCR7, and CXCR4) in thyroid samples obtained from PTC patients. Our results showed a significant increase in the expression of these receptors in PTC samples compared to normal thyroid tissue from the same patient. To our knowledge, this is the first report of a significant increase in CCR3 expression in PTC compared to matched nonmalignant tissue samples (control), both by immunohistochemistry (Fig. 1e) and flow cytometry analyses (Fig. 3A). Consistent with previous reports (31,32), PTC tissues significantly expressed CXCR4 and CCR7, supporting the notion that these two receptors can be potential markers for PTC. We found that near 100% and 90% of tumor cells overexpressed CCR3 (Fig. 1c) and CXCR4 (Fig. 1m), respectively, while CCR7 was scarcely expressed (less than 5% of tumor cells in PTC stained for CCR7) (Fig. 1h). While CCR3 (Fig. 1a) and CXCR4 (Fig. 1k) were found in 25% of normal thyroid cells, CCR7 was absent in these cells (Fig. 1f). We observed in some PTC tissues and in matched nonmalignant tissue the presence of infiltrated cells that also stained for these three receptors.
Chemokine receptors potentially promote tumor progression and LNM. A recent study reported that the expression of CXCR4 in PTC correlated with larger tumor size (33). In the same article the authors reported that CCR7 correlated with extrathyroidal extension, angiolymphatic invasion, and LNM (33). In our study, no statistically significant correlations could be demonstrated between the expression of CCR3, CCR7, or CXCR4 by PTC and LNM (Fig. 2). However, we observed a tendency for an increased CXCR4 expression by PTC samples derived from patients with LNMs. It is possible that this tendency would become statistically significant if the number of patients analyzed is increased.
Further, we found that CXCR4 expression correlated with extranodal extension and classic variant PTC (Table 2), suggesting that CXCR4 expression could be related to more aggressive tumors and negative prognosis (36,37). The expression of CCR3 and CCR7 showed no significant correlation with any of the pathological parameters analyzed (Table 2). However, the expression of chemokine receptors might be possibly linked to other clinical features not assessed in this study, such as the risk of recurrent disease. To approach this issue, appropriate prospective follow-up of patients is required, which is currently taking place in our hospital. In other types of cancer CCR3 expression is shown to correlate with LNM (34,38), and CCR7 (33,39) and CXCR4 (32) with thyroid carcinoma. It is also possible that the increased expression of CCR3, CCR7, or CXCR4 in PTC is a consequence of tumor-associated inflammatory environment, as has been shown for other types of tumors (34). Regardless of the cause, altered expression of CCR3, CCR7, or CXCR4 could likely associate with the acquisition of a malignant potential, as seen for other tumors such as T-cell lymphoma (40), kidney cancer (34), and glioblastoma (35).
Flow cytometry analyses showed an increased expression of CCR3 on the surface of PTC-derived cells (Fig. 3A). In contrast, no significant changes were observed for CCR7 and CXCR4 expression on PTC compared to control cells (Fig. 3D and G). On the other hand, immunohistochemistry analyses showed that CCR3, CCR7, and CXCR4 were strongly expressed intracellularly both in PTC and in control samples. These observations are consistent with the notion that active chemokine receptors are normally located intracellularly (24,25). Receptor internalization seems to be necessary to trigger the signal transduction pathways induced by the chemokine binding to the receptor (25,41,42). A similar intracellular pattern for CCR3 location has been previously described for dendritic cells (43), lymphocytes (44), and for CXCR4 and CCR7 in thyroid cancer (31,33). Further functional studies for CCR3, CCR7, and CXCR4 in PTC are required to evaluate whether their intracellular location is related to their activity.
In summary, this report shows for the first time a significant increase of CCR3 expression in PTC, as compared to control thyroid tissues. Our data indicate that at least three chemokine receptors, CCR3, CCR7, and CXCR4, are likely involved in the tumorogenic process of PTC and support the notion that a particular pattern of chemokine receptor expression could be related to PTC.
Footnotes
Acknowledgments
We thank Dr. Oslando Gutierrez for helping us with the statistical analyses. This work was supported by the Millennium Nucleus on Immunology and Immunotherapy (P04/030-F) and the Biomedical Research Consortium CTU06, Chile.
Disclosure Statement
The authors declare that no competing financial interests exist.