
Abstract
Background:
Cutaneous metastases from well-differentiated thyroid carcinomas are rare and usually identified in patients with widely disseminated disease. Fine-needle aspiration biopsy (FNAB) has become an acceptable method for the assessment of thyroid nodules. Very rarely needle track dissemination of tumor cells in the thyroid nodule occurs, but, when this occurs, it is evident many years after the FNAB. We report a patient who appears to have tumor dissemination from an FNAB needle track only 4 months after the procedure.
Summary:
An 85-year-old female presented with a mass on her neck, skin ulceration, and hemorrhage 4 months after FNAB was performed for a thyroid nodule by another physician. A second FNAB with ultrasound guidance yielded cytology diagnostic of papillary thyroid carcinoma. Papillary thyroid carcinoma was confirmed by surgical dissection of the mass, and a linear array of tumor was noted in skin and muscle was performed again, and the cytological diagnosis revealed papillary carcinoma. After surgical resection, the histopathological diagnosis determined the nodules to be papillary carcinoma. Metastatic deposits appeared in the skin and the muscle. The linear array and the site of metastases implied that seeding most probably resulted from the needle biopsy.
Conclusion:
Although FNAB is a useful tool for the diagnosis of thyroid nodules, it is important to consider the risk of tumor cell dissemination.
Papillary thyroid carcinoma (PTC) is the most common thyroid malignancy and is usually associated with an excellent prognosis even with regional lymph node metastases (1,2). Generally these carcinomas have an indolent character, but the older the patient, the more aggressive is the tumor. Fine-needle aspiration biopsy (FNAB) is one the most useful method for the preoperative evaluation of patients with thyroid nodules. Implantation metastasis along the needle track following FNAB is a potential risk for any type of cancer but is very rare in PTC and usually does not occur until many years after the procedure (3 –5).
Here, we report a patient who developed muscle and cutaneous lesions that appeared to be due to needle track seeding of a PTC in the setting of a FNAB 4 months back. The patient was an 85-year-old woman who presented with a mass in the thyroid area, skin ulceration, and hemorrhage on her anterior neck (Fig. 1) after a FNAB for a thyroid nodule. She first visited a physician for a nodule in the left lobe of the thyroid 4 months back, and a FNAB was performed with two passes using a 23-gauge needle without ultrasound guidance. A definitive cytological diagnosis was not made and the patient refused further investigation or surgery at this center. When we saw her she gave a history of a gradually enlarging mass on her neck, skin ulceration, and hemorrhage since her first FNAB. Physical examination revealed a 7 cm cervical mass with skin ulceration and hemorrhage. Her thyroid-stimulating hormone level was normal. As the lesion had grown rapidly we thought that it was most likely anaplastic thyroid carcinoma. A FNAB with ultrasound guidance was performed with one pass using a 23-gauge needle. The cytological diagnosis was PTC. Ultrasound examination confirmed a large lobulated mass within the left thyroid lobe and isthmus and pathologic lymphadenopathy in the cervical region VI. A neck computed tomography (CT) scan revealed that the nodule adhered to the dermis and the strap muscle, but there was no invasion in the internal jugular vein, carotid artery, or trachea (Fig. 2). CT of the thorax, abdominopelvic ultrasonography, and CT of the head and whole body I-131 scan did not show findings suggestive of distant metastasis. The patient underwent total thyroidectomy and central neck lymph node dissection. The skin around the tumor and a segment of the strap muscle was completely resected because the tumor was adhered to these structures. There was no infiltration to the internal jugular vein or carotid artery. Histopathology revealed a 6 × 5 × 4 cm of PTC (Fig. 3) with extracapsular and vascular invasion of the tumor cells, and metastases of skin and muscle, and all of the eight lymph nodes were metastatic. The linear array of the tumors in the skin and muscle was highly suggestive of needle track dissemination. After surgery she was treated with radioactive iodine.

An anterior neck mass with skin ulceration and hemorrhage.
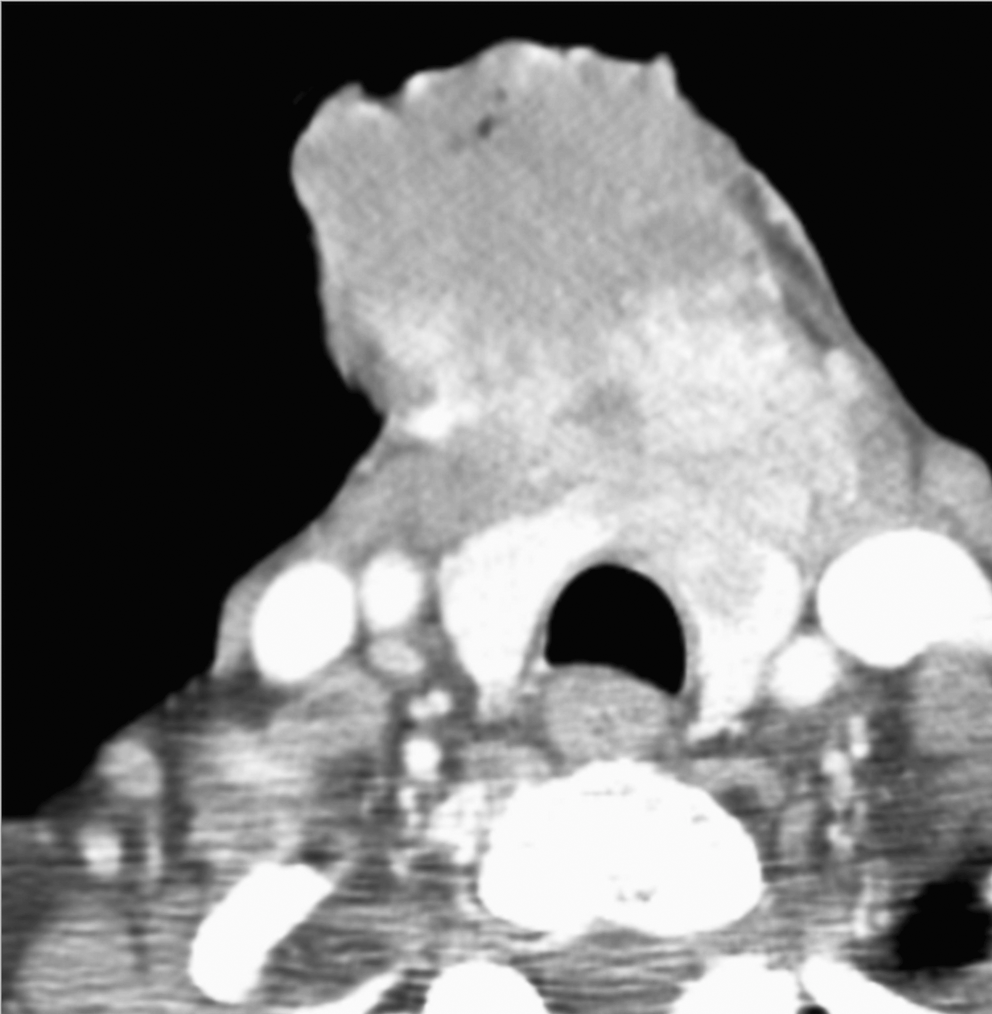
Neck computed tomography showing 7 × 5 cm mass anterior to the thyroid cartilage with an invasion of skin and strap muscles.
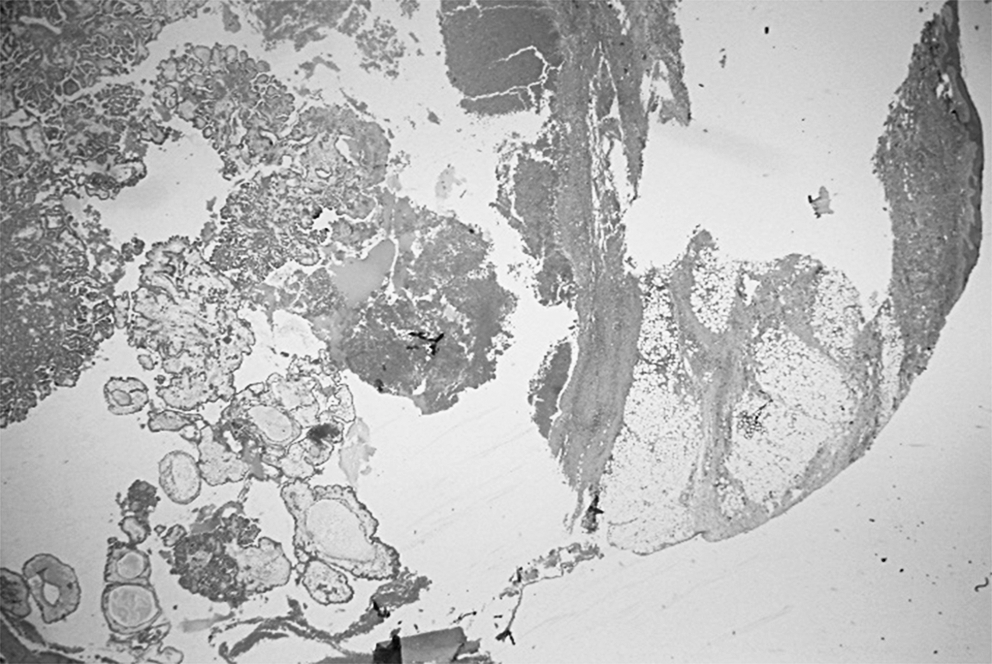
Thyroid papillary carcinoma showing randomly oriented, branching papillae with fibrovascular cores and necrosis, infiltrating the subcutaneous adipose tissue of the skin (hematoxylin and eosin, × 40).
Cutaneous metastases from well-differentiated thyroid carcinomas are rare. We concluded that the metastases in this patient were probably caused by needle track implantation from her FNAB for several reasons. First, the cutaneous lesions occurred at the entry side of the previous biopsy, and second the linear relationship between the cutaneous metastases and the muscle implant strongly suggests needle track dissemination of tumor cells. In previous reports of probably seeding of tumor cells from a thyroid needle biopsy, the interval between the biopsy and the finding of clinically apparent tumors was from 2 to 131 months (1,3 –11).
It is noteworthy that our patient was of relatively advanced age when she first presented with PTC, and it is uncertain how advanced her tumor was at that time but her history indicated growth of cutaneous lesions following the initial FNAB. Patients with advanced age, in particular, should probably have imaging studies performed in conjunction with their initial FNAB when they present with a neck mass since’ if this is malignant, they will probably require aggressive management.