
Abstract
Background:
Anaplastic thyroid carcinoma (ATC) has a very dire prognosis and no effective therapeutic strategies have been established for ATC patients, especially those with stage IVB or IVC. Our objective was to investigate the effectiveness of weekly paclitaxel administered as induction chemotherapy and to establish novel therapeutic strategies for ATC.
Methods:
We performed induction chemotherapy by weekly paclitaxel administration for patients with stage IVB (nine patients) and IVC (four patients) disease. Clinical and histological responses were assessed. Overall survival was compared with that of ATC patients with stage IVB (n = 50) and IVC (n = 13) treated without paclitaxel.
Results:
One patient demonstrated complete response (CR) and two demonstrated partial response (PR) in the stage IVB group (response rate: 33%), and one patient showed PR in stage IVC (response rate: 25%). Curative surgery and adjuvant therapy were performed for four patients with stage IVB, and 32 months after treatment, all the four are alive and free of disease. One CR patient and one stable disease patient were assessed as grade IV (complete remission) and grade III (nearly CR) on histological response, respectively. All four patients with stage IVC died of carcinoma within 8 months. Overall survival of stage IVB patients with induction chemotherapy was better (p = 0.0213) than that without the chemotherapy and also better (p = 0.0467) than those with chemotherapy other than paclitaxel. However, induction chemotherapy did not improve the overall survival of stage IVC patients (p = 0.2002).
Conclusions:
Induction chemotherapy by weekly paclitaxel is a promising therapeutic strategy for stage IVB ATC patients. Responders can be expected to achieve long-term survival. We could not get significant difference of overall survival between stage IVC patients with or without weekly induction paclitaxel, although there were some cases that responded well.
Introduction
Because of the poor prognosis, all ATCs are classified as stage IV on International Union Against Cancer (UICC) staging (2) and stage IV is divided into three subcategories: stage IVA, tumor limited to the thyroid and is surgically resectable with or without regional lymph node metastasis; stage IVB, tumor extends beyond the thyroid capsule and is usually surgically unresectable; and stage IVC, tumor with distant metastasis. Although the prognosis of stage IVA patients who have undergone curative surgery remains dire (3 –5), there is a small chance for long-term survival. Patient prognoses are significantly different at each stage. Stage IVB patients undergoing curative surgery showed a prognosis similar to that of stage IVA patients, but the prognosis of those with noncurative surgery is as poor as that of stage IVC (6). For ATC patients, especially for those with stage IVB or IVC, various adjuvant therapies have been performed and some chemotherapeutic agents such as doxorubicin, cisplatin, uracil/tegafur (UFT; Bristol Myers Squibb, Wallingford, CT) and combination chemotherapy with cisplatin, etoposide, and/or doxorubicin (EP or EAP) have been reported to be effective but the findings are far from conclusive (7 –15).
Paclitaxel is the first member of the taxane family to exert a cytotoxic effect by arresting mitosis through microtubule stabilization, resulting in cellular apoptosis. The use of paclitaxel as a chemotherapeutic agent has become a broadly accepted option in the treatment of patients with ovarian, breast, and nonsmall cell lung cancers, malignant brain tumors, and a variety of other solid tumors (16). In 2000, Ain et al. reported that paclitaxel appeared to be the only agent with significant clinical systemic activity against ATC by phase 2 trial using 96-hour infusion (17). However, to our knowledge, this is the only report that documents the effect of paclitaxel for ATC and its influence on survival is uncertain.
Since 2005, we have performed induction chemotherapy with weekly paclitaxel for previously untreated ATC patients in stages IVB and IVC. Significant prolongation of overall survival was seen, especially in stage IVB patients.
Patients and Methods
Patients
Between 2005 and 2008, 13 patients who were diagnosed as having ATC by cytological and pathological examinations and treated at Kuma Hospital were enrolled in this study. All patients gave informed consent prior to participation. They were divided into two groups according to UICC staging, nine in stage IVB and four in stage IVC. Mean ages of patients were 61.5 and 54.8 years, respectively. Mean tumor sizes were 5.1 and 7.3 cm, respectively. The clinical features are summarized in Table 1. There were no patients in stage IVA in this series. When the patient presented to our hospital, fine-needle aspiration cytology was performed to diagnose ATC, and then core needle biopsy was performed to confirm the diagnosis. Extrathyroid extension was assessed by palpation and imaging studies such as ultrasonography and computed tomography (CT) scan. Distant metastasis was assessed by CT scans of the chest, abdomen, and brain. Induction chemotherapy was started within 1 week after the diagnosis of ATC.
CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease.
Chemotherapy regimen
Weekly paclitaxel was performed at 80 mg/m2 as a 1-hour intravenous infusion on days 1, 8, and 15 of each 21- or 28-day cycle, indicating that one cycle consisted of three courses. Patients received premedication with dexamethazone, ranitidine, chlorpheniramine, and granisetron as described elsewhere (18).
Treatment
Thirteen patients received the induction chemotherapy described above. All had measurable tumors and objective responses were assessed. The protocol for stage IVB was induction chemotherapy with two to three courses of weekly paclitaxel, and then surgery, if possible, followed by adjuvant weekly paclitaxel for a total of six courses, and radiotherapy after completion of chemotherapy. CT scans of the neck, chest, and abdomen were obtained at 2- to 4-week intervals to assess tumor response. The therapy was withheld if a treatment-related adverse event beyond grade III or progressive disease (PD) with no benefit of continuing the protocol occurred. Management for stage IVC was almost the same but patients did not undergo planned surgery or radiotherapy and tried to continue weekly paclitaxel for as long as possible. Other additional therapies including palliative surgery, intratracheal stent, tracheotomy, or radiotherapy were allowed to control the local lesion.
Controls
Fifty stage IVB and 13 stage IVC patients served as controls to assess overall survival. Between 1983 and 2005, these patients presented to our institute and were found to have ATC. They were treated by multimodal therapy other than paclitaxel. Thirty-eight patients underwent surgery; 10 stage IVB patients underwent complete resection, and 25 stage IVB and 3 stage IVC patients received palliative surgery. Chemotherapy with cisplatin, etoposide, vincristine, doxorubicin, or UFT was administered to 24 stage IVB and 4 stage IVC patients. External beam radiotherapy (XRT) was administerd to 24 stage IVB and 1 stage IVC patients. Mean ages of stage IVB and IVC patients were 69.8 and 70.1 years, respectively. Mean tumor size was 6.0 and 6.8 cm for stage IVB and IVC, respectively. The patients with anaplastic transformation of recurrent tumor after surgery for differentiated carcinoma, those with anaplastic carcinoma detectable only in the lymph nodes but not in the primary tumor, and those who were treated with paclitaxel as adjuvant chemotherapy by regimens other than that used in this study were excluded from the series.
Assessment of tumor response
Objective clinical response was assessed by CT images according to Response Evaluation Criteria in Solid Tumors (19). The primary endpoint was at 8 weeks after diagnosis (and initiation of chemotherapy). Patient responses were classified into four categories: complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). The clinical response of CR, PR, or SD was confirmed by repeat imaging studies at least 4 weeks later except when all measurable tumors were resected. Brain or bone was examined if symptoms were present.
The histological response to chemotherapy was assessed by the previously described method (20). Sections of each surgical specimen were examined, and the histological response to chemotherapy was graded semiquantitatively by tumor regression into grades I to IV based on the percentage of vital residual tumor cells (VRTCs): grade I, >50% VRTCs; grade II, 10% to 50% VRTCs (PR); grade III, nearly CR (NCR) with <10% VRTCs; and grade IV, complete remission.
Postoperative follow-up
Recurrence and distant metastasis of patients who underwent surgery were evaluated by ultrasonography and CT scans at 4-week intervals up to 24 months after the diagnosis. Blood tests were performed at each hospital visit to assess inflammatory reaction and adverse events associated with chemotherapy.
Statistical methods
The Kaplan–Meier method and log-rank test were adopted to analyze overall survival. These analyses were performed using StatView-J 5.0. A p-value of less than 0.05 was regarded as significant.
Results
Clinical response
Clinical courses of patients are summarized in Table 1. The follow-up period was counted from the point of diagnosis as ATC to the last day of follow-up. Figure 1 shows representative cases of CR and PR. Of nine stage IVB patients, one demonstrated CR (case 1) and two demonstrated PR (cases 2 and 3), indicating a response rate (CR + PR) of 33%. One of the four stage IVC patients showed shrinkage of lung metastasis and demonstrated PR (case 10) at the evaluation point and a response rate of 25%. Total response rate was 31% and mean time to achieve PR was 6 weeks. Two patients in stage IVB (cases 4 and 5) and two in stage IVC (cases 11 and 12) showed SD. Clinical benefit rates (CR + PR + SD) of stage IVB and stage IVC were 56% and 75%, respectively.

Computed tomography images of representative cases that responded to induction therapy with weekly paclitaxel. Case 1 showed a complete response (CR) in the anaplastic carcinoma lesion encasing the trachea. The calcified tumor in the right lobe was a preexisting papillary carcinoma. Case 3 showed partial response (PR). Note marked reduction in size in the anaplastic carcinoma lesion ventral to a round tumor of poorly differentiated follicular carcinoma from which anaplastic transformation occurred. In case 10, pulmonary metastases showed PR and dyspnea was relieved.
After chemotherapy, grossly curative surgery was performed for four patients with stage IVB (cases 1–3, and 5) who were judged as CR, PR, or SD, and these patients are alive without evidence of carcinoma recurrence from 11 to 32 months after the diagnosis. The size of their tumors ranged from 35 to 48 mm and was smaller than that of the other patients (51–72 mm). One patient (case 4) was judged as SD at the initial evaluation point, but died because of the progression of primary tumor thereafter. Four patients with stage IVB with PD also died of carcinoma within 4 months after diagnosis. Three patients demonstrated enlargement of primary lesions after 2–8 weeks (mean time: 5.3 weeks). One patient (case 7) demonstrated shrinkage of the tumor to 77% after 2 weeks, but during the next 4 weeks, it grew 1.5-fold. Palliative surgery was performed for this patient, but she demonstrated local recurrence at 1 week after surgery and died of carcinoma at 4 weeks after surgery.
Although three of four patients with stage IVC were judged as PR or SD at the initial evaluation point, all died of subsequent carcinoma progression within 8 months. None of these patients showed a response to the therapy in the primary lesions. Cases 10, 11, and 12 showed shrinkage of lung metastasis at the initial evaluation point, but subsequently case 10 died of multiple metastases to the lung, liver, and brain, case 11 died of primary tumor development, and case 12 died of unknown cause. One remaining patient (case 13) did not show any change in the primary tumor or liver metastases before or after chemotherapy, but bone metastasis newly appeared during chemotherapy. He was judged as having PD and died of carcinoma at 9 weeks after diagnosis.
Changes in the sum of the diameters of target lesions compared with baseline values are shown in Figure 2. Mean time to PR was 6 weeks and mean time to PD was also 6 weeks.
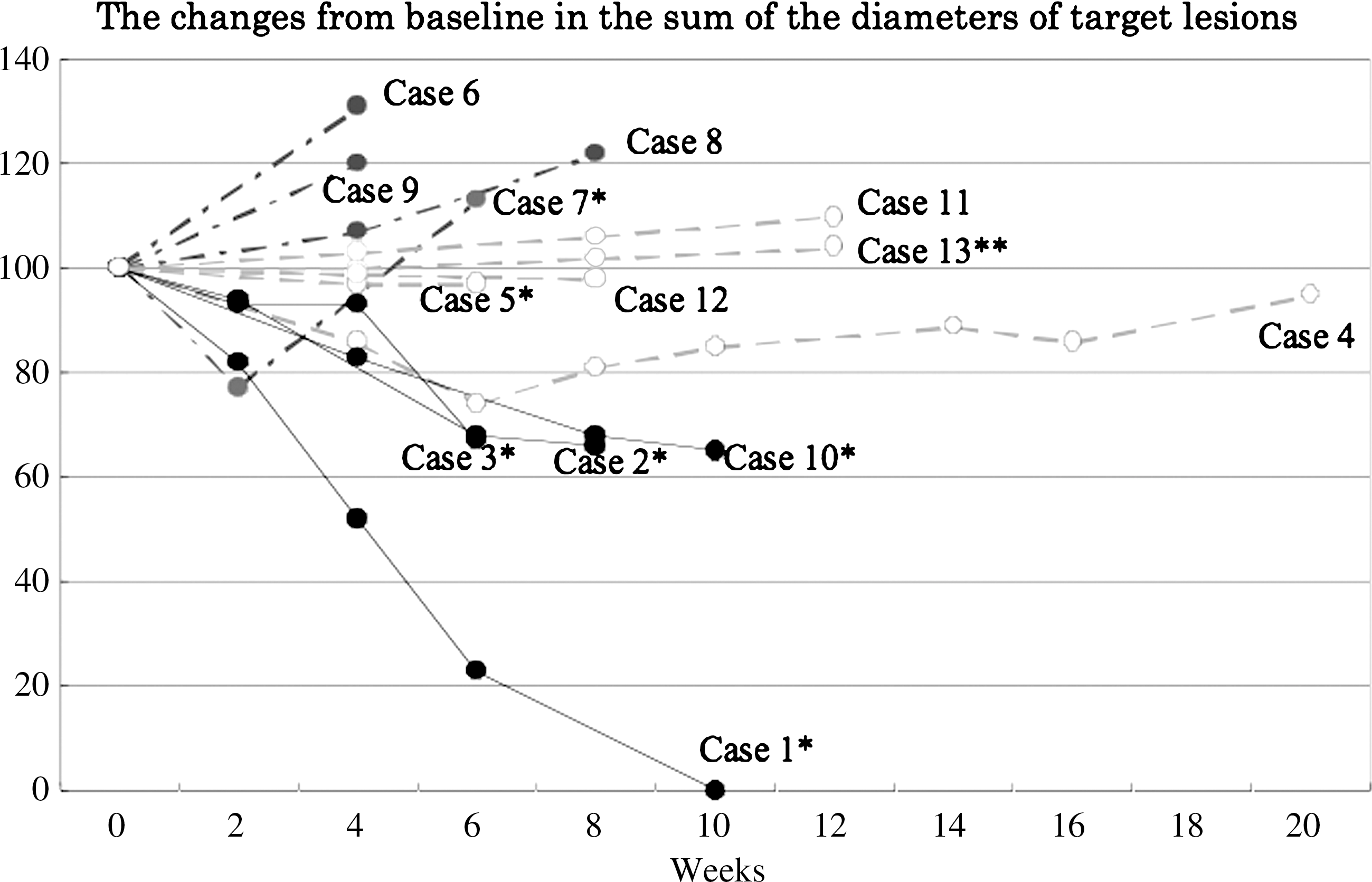
Changes in the sum of the diameters of target lesions compared with baseline values. Clinical response: CR and PR (solid line), stable disease (broken line), progressive disease (dashed line). *Indicates patients who underwent primary tumor resection. **Case 13 was assessed as progressive disease because of newly developed bone metastasis.
Histological response
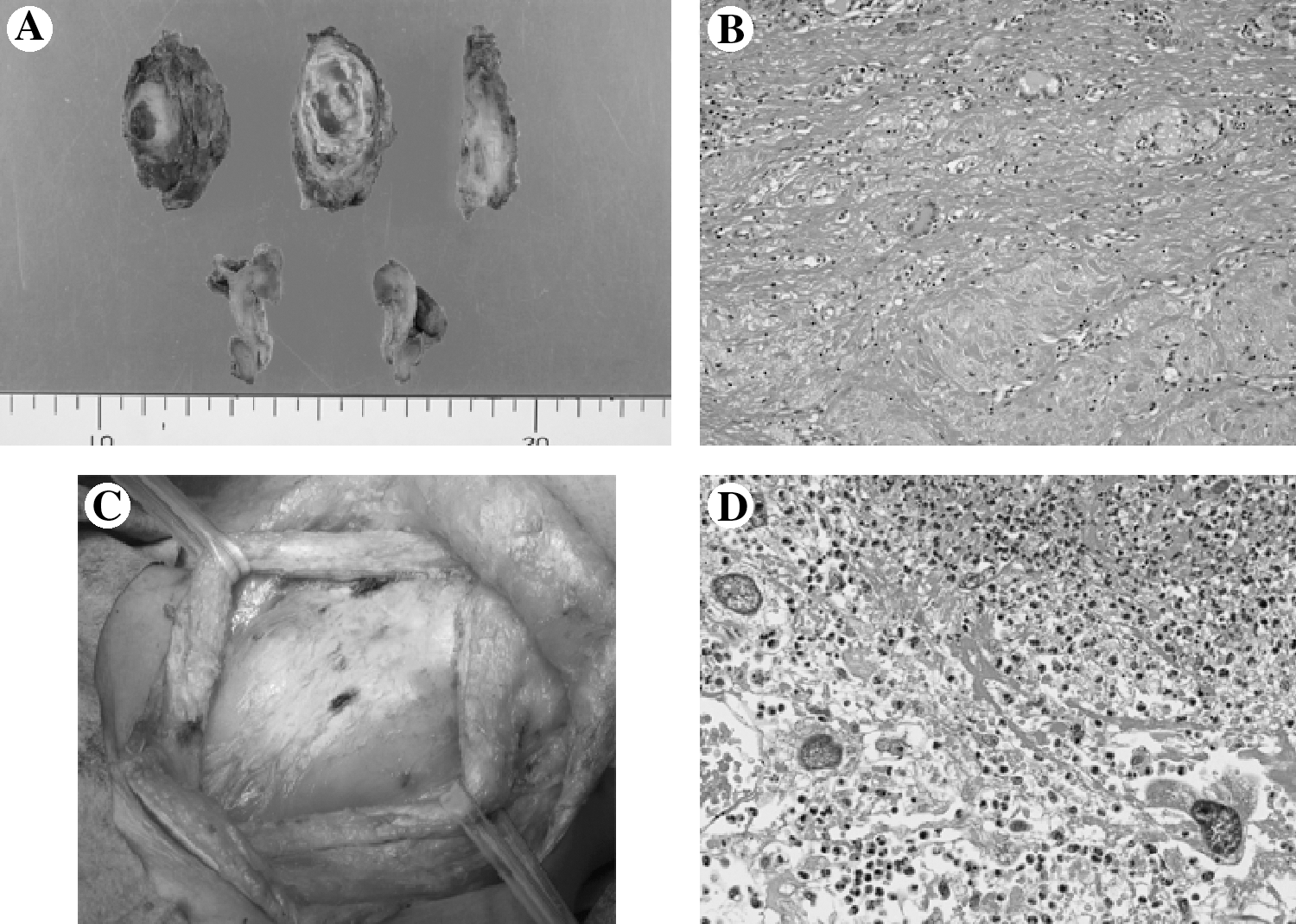
Histological response was evaluated for 7 of 13 patients who received surgical resection of the primary tumor (Table 2). The size of tumors graded as II or greater tended to be smaller (35–47 mm) than those graded as I (44–79 mm). Of four patients with stage IVB, one who was classified as having clinical CR also demonstrated histological CR (complete remission, grade IV) (case 1). In this case, calcified tumor from which ATC was presumed to have evolved demonstrated papillary thyroid carcinoma cells, but the tissue surrounding the tumor but exterior to the thyroid showed complete change to connective tissue (Fig. 3). One patient (case 5) was clinically judged as having SD, but was graded as III (NCR) on histological response (Fig. 3). This patient is alive 7 months after diagnosis. Other two PR patients demonstrated grade II and grade I (cases 2 and 3), respectively. Figures 1 and 4 indicate that antecedent tumor of follicular carcinoma transformed to ATC and extrathyroid invasion of ATC changed to fibrous tissue by chemotherapy (case 2). Three patients with stage IVC were classified into grade I regardless of their clinical response.
(

Pathological studies of the resected specimen from case 2 showing residual anaplastic carcinoma lesion (
pCR, complete remission; NCR, nearly CR.
Overall survival
Overall survival of stage IVB patients who underwent induction chemotherapy was significantly better than that of the control group (p = 0.0213; Fig. 5) and also better than that of the subset of patients who received chemotherapy other than paclitaxel (p = 0.0467; Fig. 6). However, the survival of stage IVC patients receiving induction chemotherapy did not differ from that of the control group (p = 0.2002; Fig. 7). The 6- and 12-month survival rates of stage IVB patients with induction chemotherapy were both 44%, and those of the control group were 25.5% and 5.9%, respectively. In stage IVB, three responders (CR + PR) to preoperative chemotherapy with weekly paclitaxel showed significantly better overall survival than the nine nonresponders. However, the p-value was not calculable because none of the three responders died of carcinoma to date (Fig. 8).
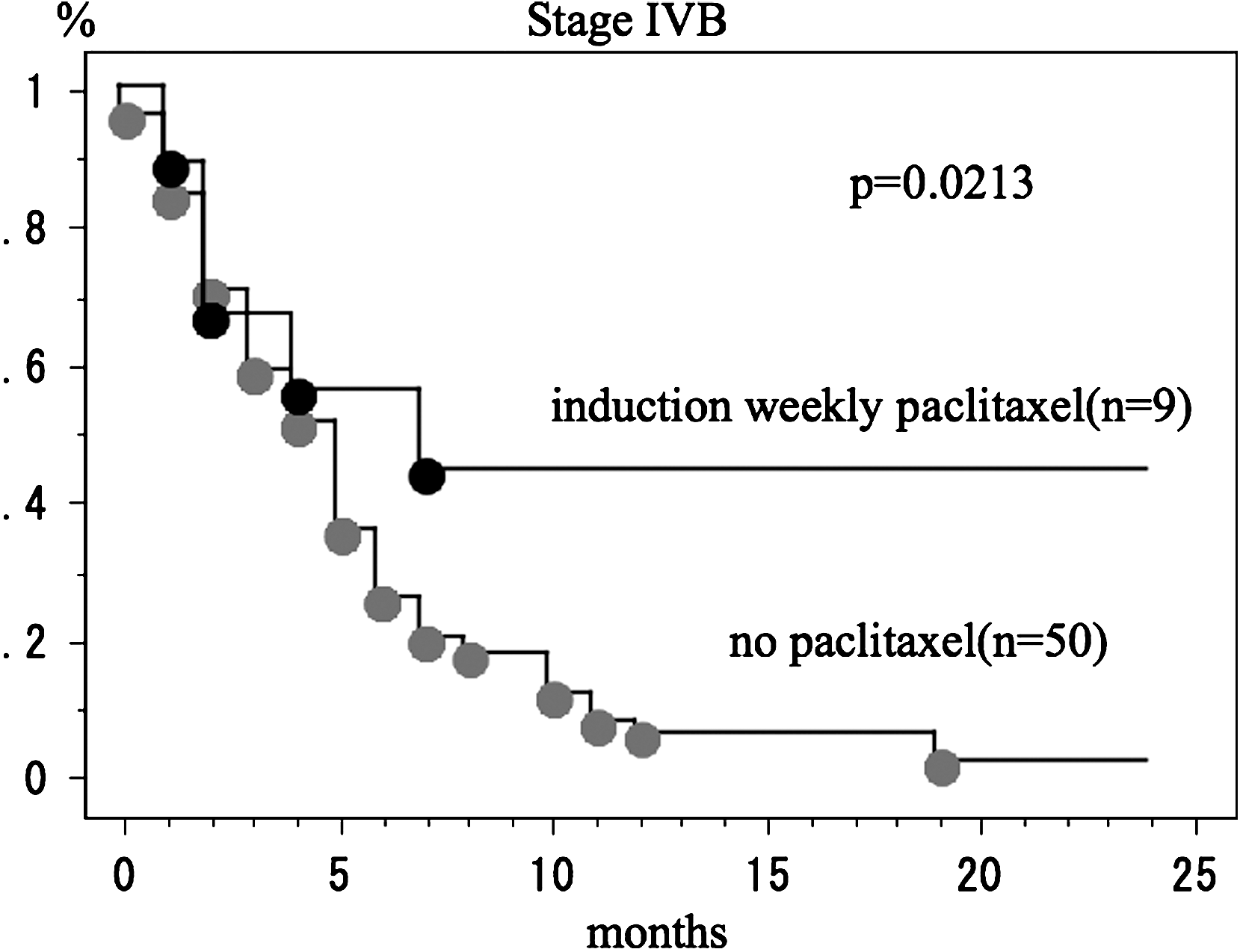
Comparison of overall survival between stage IVB ATC patients with induction weekly paclitaxel and without paclitaxel.
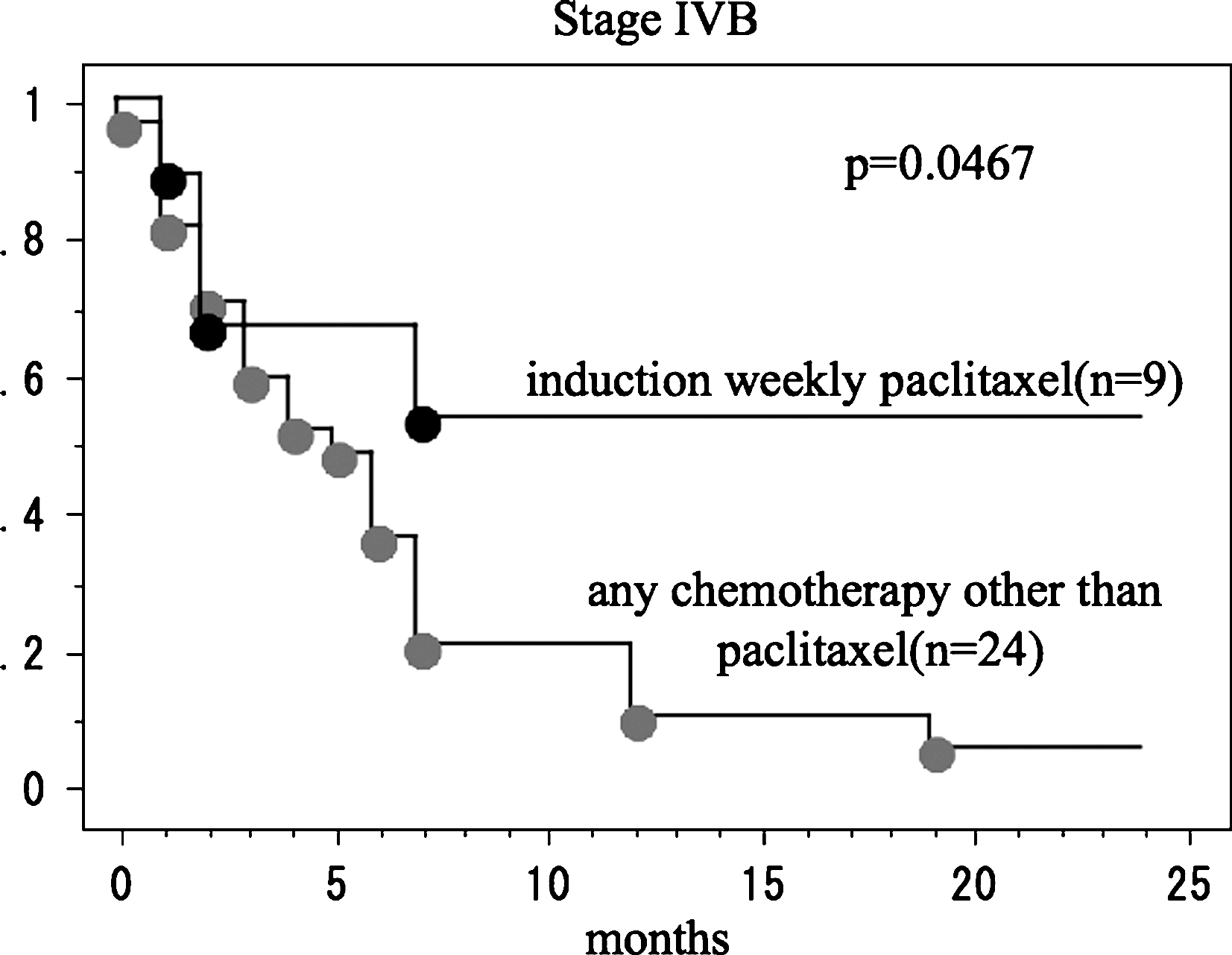
Comparison of overall survival between stage IVB ATC patients with induction weekly paclitaxel and with chemotherapy other than paclitaxel.

Comparison of overall survival between stage IVC ATC patients with induction weekly paclitaxel and without paclitaxel.

Comparison of overall survival of stage IVB ATC patients receiving induction weekly paclitaxel between responders to chemotherapy and nonresponders.
Adverse events of weekly paclitaxel
There were no severe treatment-related adverse events except for one case of grade III pulmonary fibrosis. In this case, treatment was withheld after a total of 17 courses and the symptom improved immediately (case 3). Most of the therapies were performed on an outpatient basis. Because of grade II leukocytopenia, the schedule was postponed for 1 week in one patient (case 11). Most of the patients demonstrated alopecia and grade I nausea. Peripheral neuropathy developed in five patients who had received more than five courses of chemotherapy (cases 1, 2, 3, 5, and 10; Table 1).
Discussion
Multimodal therapy including surgery, chemotherapy, and radiotherapy is a basic treatment for aggressive carcinoma. Aggressive multimodal therapy may be encouraged for ATC patients (21) or should be applied only for selected patients (22 –25). In this study, we showed that induction chemotherapy with weekly paclitaxel is very effective for patients in stage IVB. The response rate was 33% (three of nine patients) and all of the responders are alive without evidence of carcinoma recurrence 15–32 months after curative surgery. The remaining one patient who survived for 11 months showed clinical SD but also showed prominent histopathological response (NCR) (Fig. 3). In contrast, other patients, including three PD patients, died of carcinoma within 6 months after diagnosis. These findings suggest that the prognosis of stage IVB patients is polarized between responders and nonresponders to weekly paclitaxel.
All stage IVB patients who achieved long-term survival underwent grossly curative surgery, which is a requirement for patients to improve their survival (3,6). However, it is difficult to evaluate the timing of surgery, that is, whether these patients can undergo locally curative surgery at presentation. Indeed, one SD patient underwent curative surgery after chemotherapy and it is possible that tumors of other patients could be curatively resected at presentation. However, we previously demonstrated that more than half of patients with stage IVA who underwent curative surgery died of carcinoma, predominantly because of distant metastasis, within 1 year after surgery (6). In contrast, none of the four patients with stage IVB who underwent weekly paclitaxel as an induction therapy and subsequent curative surgery showed any recurrence to the distant organs at 11–32 months of follow-up. These findings allow us to speculate that weekly paclitaxel is effective not only for primary lesions but also for micrometastases in distant organs.
Although the clinical benefit rate (CR + PR + SD) was high at 75%, we failed to establish the improvement of survival of stage IVC patients and all patients died of carcinoma within 8 months after the diagnosis. According to Response Evaluation Criteria in Solid Tumors, clinical response is evaluated by the summation of multiple carcinoma lesions, indicating that the evaluation depends mostly on the size of lung metastasis in these four patients. This suggests that the responses of these patients are overestimated. However, three of four patients with stage IVC showed, at least temporarily, shrinkage of lung metastasis, indicating that this therapy can be effective for stage IVC patients to some extent. The reason for the lower effectiveness of this therapy for stage IVC patients remains to be elucidated, but a large volume of carcinoma metastases with polyclonality in distant organs may make the therapy less effective. Further studies using a large series of patients with stage IVC are needed to elucidate this issue.
The optimal sequence of paclitaxel and other therapies for stage IVB patients remains debatable. One alternative is preoperative XRT, which may shrink and downstage primary lesions and enhance surgical resectability. The possible sequence is that the patient undergoes a partial course of XRT, curative surgery after the shrinkage of tumor, completes the course of XRT, and then receives six courses of paclitaxel. The merit of this sequence is that paclitaxel does not need to be applied to a large mass of carcinoma. It is generally known that systemic chemotherapy is more effective in micrometastatic tumor than macrometastatic tumor (26,27). Indeed, as shown in Tables 1 and 2, small tumors showed more effective clinical and histological responses to paclitaxel. For this reason, administration of paclitaxel as adjuvant therapy may be more advantageous than as induction therapy. However, this sequence definitely results in a delay of systemic treatment, which may allow the growth of distant metastasis before the use of paclitaxel. Induction chemotherapy may be effective not only for primary lesions but also for micrometastases in distant organs. Further, another advantage of induction chemotherapy is that it provides measurable target lesions allowing us to evaluate its effectiveness. Adjuvant chemotherapy after surgery is often difficult to evaluate whether it is effective. Further studies are required to establish the most efficient sequence of therapy for stage IVB patients.
Optimal schedule of chemotherapy is important. Weekly regimens of paclitaxel were developed in an effort to increase the treatment efficacy and reduce toxicity. As the estimated doubling time of ATC is only 3–12 days,17 the interval between the administrations of the chemotherapeutic agent should be optimized. The intervals in most chemotherapeutic regimens are 3–4 weeks. However, we should consider how fast ATC cells grow. If the doubling time is 3 days, the tumor will grow 1000-fold during a 4-week interval. This means that even if the chemotherapeutic agent successfully kills 99% of the cancer cells, after 4 weeks the cancer would become 10 times larger than the initial volume. Ki67 immunohistological staining of our specimens of ATC showed only 60–95% of the proliferation rate of ATC cells. Because chemotherapeutic agents affect only proliferated (mitotic) cells, the best performance rate of any chemotherapeutic agent is at most 95%. From this perspective, strong medication at long intervals does not make sense, and the agent must be administered at relatively short intervals. Weekly administration of paclitaxel is rational for this reason.
Because weekly paclitaxel 80 mg/m2 is a well-established method of dose-dense chemotherapy for various cancers (18), we adopted the same dose in this study. A higher dose may improve the response, but it increases toxicity and reduces the frequency of administration. We aimed to achieve frequent and constant administration rather than high dose intensity for patients in our series. In addition, 1 week is an appropriate interval to evaluate tumor size and to enable patients to easily return to the hospital for the next treatment. We should investigate the optimal dose and frequency of paclitaxel administration for these patients in the future.
In summary, we demonstrated that induction chemotherapy with weekly paclitaxel is effective and that long-term survival can be expected for stage IVB patients who respond to the therapy. For stage IVC patients, this regimen may contribute to improving the quality of life, but other strategies such as multiagent chemotherapy should be investigated. Further studies are necessary to evaluate the effect on stage IVC patients.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.