
Abstract
Background:
Solitary fibrous tumor (SFT) is a rare spindle cell tumor most often found in the mediastinal pleura. Nineteen cases of SFT arising in the thyroid gland have been reported. We report a case of SFT of the thyroid gland with immunohistochemical and cytogenetic investigation.
Summary:
A 58-year-old man had pulmonary symptoms, thought to be asthma. Computed tomographic scan revealed a large goiter with a solid hyperechoic nodule. The results of thyroid function tests were normal. Microscopically, the lesion was composed of fibroblast-like spindle cells in a patternless growth. Cellular atypia or necrosis was not seen, and mitotic activity was low. Immunohistochemistry showed positive reaction for CD34, vimentin, bcl-2, and CD99. Fluorescence in situ hybridization analysis of more than 100 cells exhibited no trisomy 21. Complete surgical removal of tumor is the treatment of choice.
Conclusion:
The histological appearance and immunohistochemical reaction pattern of SFT is characteristic. The entity should be considered when dealing with a spindle cell lesion in the thyroid gland. All cases of this site of origin reported have had a benign clinical course. As only a small number of cases have been described, we recommend long-term follow-up.
Introduction
Patient
A 58-year-old man presented with increasing respiratory symptoms that were thought to be caused by his well-known asthma. A chest X-ray was suspicious for intrathoracic goiter. Computed tomographic scan showed a well-demarked inhomogeneous mediastinal lesion connected to the left thyroid lobe with compression and displacement of the trachea (Fig. 1). The results of thyroid function tests were normal. Ultrasonography showed that the cervical part of the left thyroid lobe was normal. The mediastinal part showed a hyperechoic nodule with hypoechoic areas that were thought to be cystic degenerations. Cervical lymph nodes were normal. An expanded hemi-thyroidectomy was carried out, including removal of the mediastinal lesion. Follow-up revealed no postoperative complications, and the patient's shortness of breath was resolved.

Computed tomographic scan showing tumor in relation to the left thyroid lobe marked with an arrow.
Grossly, the upper part of the left thyroid lobe appeared normal. The intrathoracic nodule was firm, measured 80 × 55 × 42 mm, and seemed to be encapsulated. The cut surface was solid with a pale yellow-grayish appearance and cystic areas (Fig. 2). Histology showed the intrathoracic nodule to be a tumor composed of a cellular proliferation of fibroblast-like spindle cells, mostly without any characteristic growth pattern. Characteristic features of the lesion were present consisting of bands of hyalinization (Fig. 3). There were thin-walled vessels that varied in number and shape. Cysts were present because of marked dilation of vascular spaces. Extravasations of erythrocytes as well as an inflammatory infiltrate with lymphocytes were also found. The tumor cells varied in shape and size. The nuclei were ovoid with finely dispersed chromatin and only discrete nucleoli. Mitoses were scarce.

Gross specimen of solitary fibrous tumor (SFT).
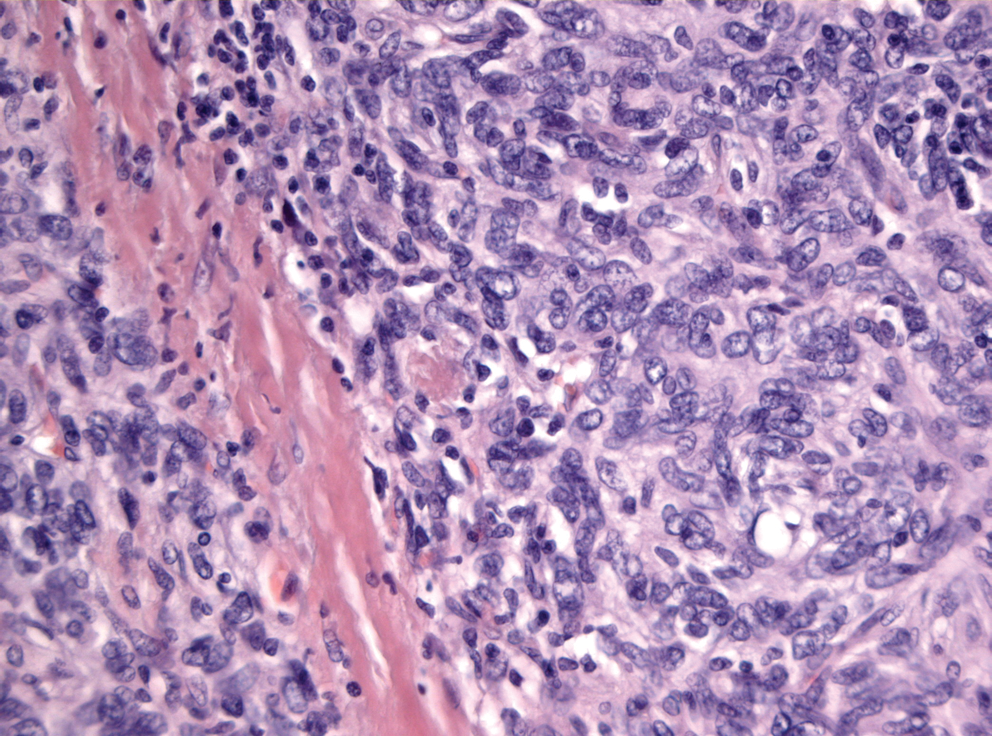
Collagen bundles lying between tightly packed spindle-shaped cells in SFT. Original magnification, × 200. Color images available online at www.liebertonline.com/thy.
The tumor showed a strong positive immunohistochemical reaction for CD34 (Fig. 4), vimentin, and bcl-2, as well as a weak but positive reaction for CD99. There were no reactions for cytokeratin, s-100, thyroglobulin, thyroid transcription factor-1 (TTF-1), or monoclonal carcio-embryonic antigen (CEA). More than 100 tumor cells were examined for trisomy 21 by fluorescence in situ hybridization, and results were negative.
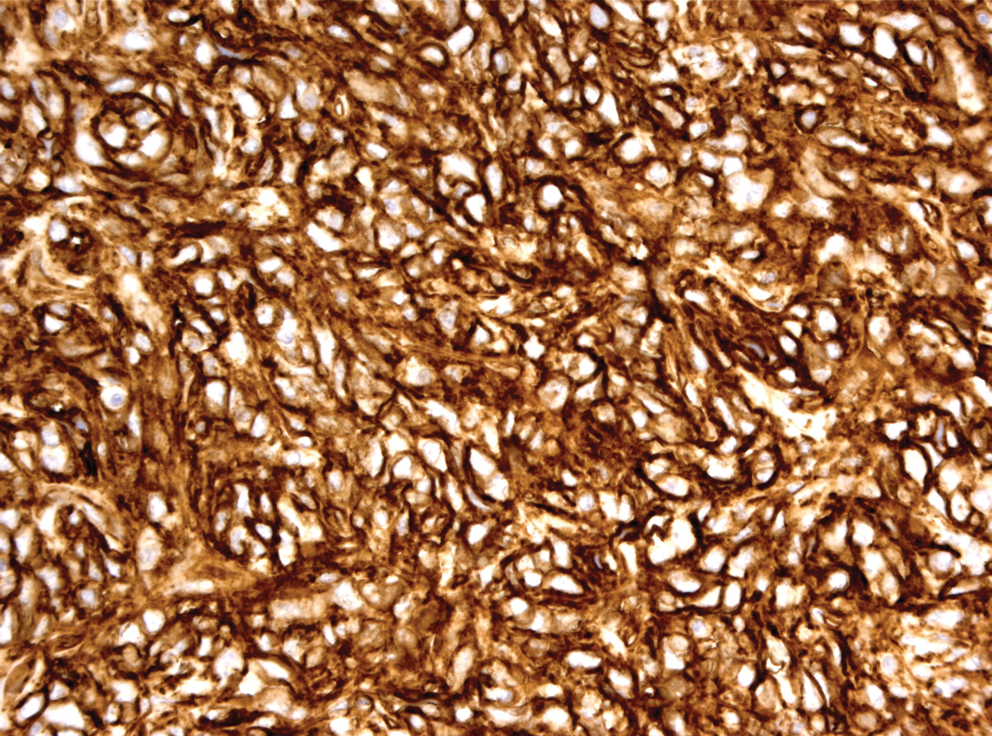
SFT strongly and diffusely immunoreactive for CD34. Original magnification, × 200. Color images available online at www.liebertonline.com/thy.
Discussion
SFT is very uncommon in the upper respiratory tract, comprising < 0.1% of all neoplasms (14). Its etiology is unknown. The epidemiology of SFT was described in the review by Papi et al. (15). Of the 19 cases of SFT in the thyroid gland reported, all have been adults with their median age being 48 (range: 28–70 years), and the number of men and women was similar (female/male ratio of 1.1/1).
These tumors typically present as cold nodules (15) in a long-standing goiter, slowly increasing in size. There are no clinical features that distinguish this tumor from other entities (15). In our patient, the intrathoracic location caused dyspnea because of tracheal compression discovered by X-ray examination of the chest.
Normally, fine-needle aspiration biopsy (FNAB) is used to separate benign and malignant nodules in the thyroid gland. In this case, surgery was not preceded by FNAB because of intrathoracic location. In one study of FNAB before surgery, there was adequate material for a definite diagnosis of a spindle cell tumor (11). However, the diagnosis of spindle cell tumor is not specific and there are a variety of lesions in the differential diagnosis.
When the tumor arises in a goiter, the possibilities of the lesion being a goiter nodule, an adenoma, or a carcinoma have to be considered. The lesion had a complete capsule, excluding a goiter nodule. Both benign and malignant spindle cell tumors can be found in the thyroid gland, including leiomyomas, schwannomas, neurofibromas, hemangiopericytomas, medullary carcinomas, and sarcomas. Our patient's tumor did not express any cytokeratin and was therefore diagnosed as a mesenchymal tumor. We found only a few mitoses, and necrosis or vascular invasion was not seen, indicating that the tumor was benign. The immunohistochemical profile showed strong expression of CD34, vimentin, and bcl-2, and a weaker but still positive reaction for CD99, which, in agreement with the morphological appearance, was diagnostic for an SFT. In the present case, the tumor showed the same immunohistochemical profile as described in several previous cases (5,6,8 –10,12,13). Strong expression of CD34 in SFT is useful for distinguishing this tumor from other spindle cell tumors. The primary differential diagnosis is between SFT and hemangiopericytomas, which also expresses CD34, but to a lesser degree than SFT. Further, in our case the vessels were prominent, but there was no obvious appearance of staghorn-shaped vessels as seen in hemangiopericytomas.
A variety of genetic changes are found in fibrous lesions, but as chromosomal aberrations differ in otherwise identical tumors, they are not of diagnostic use (16,17). Further, the abnormalities are size related, as they usually are undetectable in SFTs measuring less than 10 cm (18). No specific aberrations can differentiate pleural from extra-pleural SFT. So far, SFT arising in the thyroid gland has not been a target of cytogenetic analysis. Dal et al. (19) describe the occurrence of trisomy 21 as the only aberration in an extra-pleural STF measuring 10 cm. In the present case, a fluorescence in situ hybridization analysis for trisomy 21 could not confirm this chromosomal aberration, and because our tumor was only 8 cm, we did not search for other cytogenetic abnormalities.
Ninety-two cases of extrathoracic SFT were reported in a 1998 study (3). The histological features associated with malignancy in this study were increased cellularity, pleomorphism, necrosis, and > 4 mitoses/10 HPF. Ten of the reported patients showed atypical histological features or recurrent disease. In three of these cases there was no relationship between the histological features and the clinical course. Two patients had at least one of the criteria, but did not show recurrent or metastatic disease; one patient did not have atypical histologic features, but the disease still recurred. Therefore, the authors concluded that histological criteria of malignancy were not sufficient to predict clinically aggressive behavior. Our patient's SFT did not have any criteria for malignancy. In prior reports of SFT in the thyroid gland, all patients had a benign course, including one in which capsular invasion was observed (6). Nonetheless, since clinical experience with SFT is very limited, we recommend complete excision of the tumor and lobe of the thyroid gland containing the tumor as well as long-term follow-up.