
Abstract

Thyrotoxic periodic paralysis (TPP) can occur with any form of thyrotoxicosis. The most common cause of TPP in thyrotoxicosis is the Graves' disease (1). Only one patient with TPP due to a painless thyroiditis (PT) has been reported (2). Here we describe an additional patient with TTP due to PT who had polymorphic ventricular tachycardia. This is an extremely unusual presentation of TTP.
A 38-year-old Korean man was admitted to the emergency room for flaccid paralysis of the lower limbs for 6 hours duration. His past medical history was unremarkable. He had not taken any prescribed medications, and he did not have a history of drug abuse. There was no family history of Graves' disease. On arrival at the emergency room, his blood pressure was 150/100 mmHg, and the heart rate was 96 beats/minutes. He was alert with a respiratory rate of 20 breaths/minutes and a body temperature of 36°C. There was no proptosis. Palpation of the thyroid showed slight enlargement of the right lobe without tenderness or palpable nodule. Auscultation of the thyroid revealed no bruit. The lower limbs had flaccid paralysis with intact sensory function. Baseline laboratory data indicated normal serum sodium, magnesium, and calcium levels. The potassium level was 2.5 mEq/L (normal range 3.5–5.1 mEq/L), free thyroxine was 2.4 ng/dL (0.9–1.8 ng/dL), thyroid-stimulating hormone was 0.02 μIU/mL (0.17–4.65 μIU/mL), triiodothyronine was 179.41 ng/dL (78–200 ng/dL), thyroid-binding inhibitory immunoglobulins was 4% (normal rage <15%), and the antimicrosomal antibody was 1:6400. The initial electrocardiogram showed normal sinus rhythm (Fig. 1A). Twenty minutes after admission, he had polymorphic ventricular tachycardia with loss of consciousness (Fig. 1B). He was successfully resuscitated with 250 J cardioversion. He regained consciousness and his cardiac rhythm converted to atrial fibrillation (Fig. 1C). Cardiac enzyme measurements were as follows: creatine phosphokinase 626 U/L; creatine phosphokinase-MB 2.55 ng/mL; and troponin T < 0.010 mg/dL. A repeat electrocardiogram showed normal sinus rhythm (heart rate: 100 beats/minutes) and normal corrected QT interval. An echocardiogram performed 2 days later showed normal cardiac function without structural heart disease. Twenty-four hour holter monitoring did not show arrhythmias. A thyroid scan with Tc-99m revealed little or no uptake in the thyroid area compatible with thyroiditis (Fig. 2A). Therefore, no antithyroid drugs were administered. He was discharged from the hospital without further untoward events. The serum potassium and thyroid function was normal for 3 months (free thyroxine 1.07 ng/dL, thyroid-stimulating hormone 1.07 μIU/mL, potassium 4.1 mEq/L), and there were no symptoms of hypokalemia and muscle paralysis. A repeat thyroid scan with Tc-99m performed 3 months after the initial test revealed normal uptake in the thyroid area (Fig. 2B).
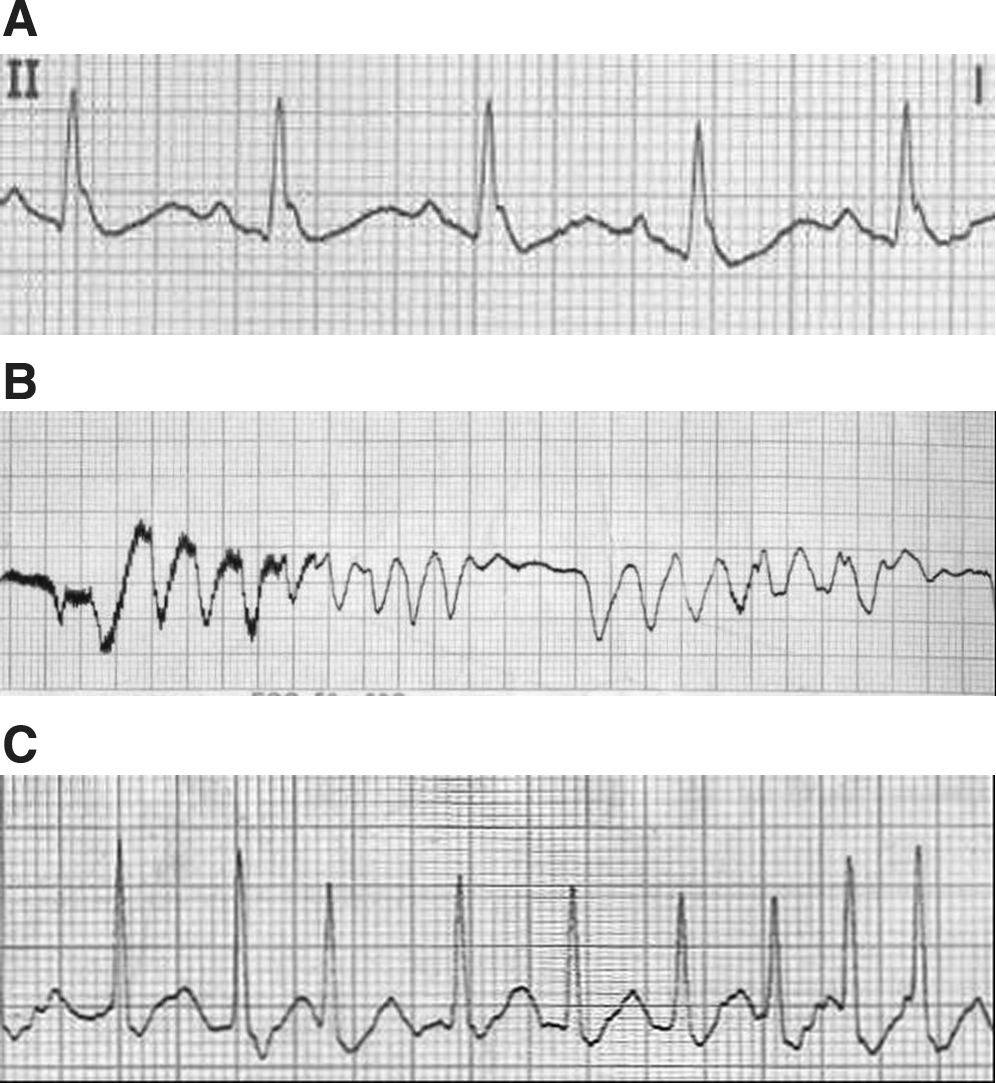
Electrocardiogram in emergency room on arrival (

Tc-99m thyroid scan on admission (
Although PT is a self-limited disease associated with transient mild thyrotoxicosis and hypothyroidism, our patient not only had TPP but also a near-fatal ventricular arrhythmia. This finding supports the concept that hypokalemia during transient thyrotoxic phase of PT can cause serious ventricular arrhythmias. Supraventricular arrhythmias (supraventricular tachycardia or atrial fibrillation) occur in 5–15% of patients with thyrotoxicosis, usually due to Graves' disease. There have been few reports of fatal ventricular arrhythmias (3). This patient's course indicates that the serum potassium level and electrocardiogram should be checked in all patients with PT who have muscular paralysis.