
Abstract
Background:
The purpose of this study was to investigate the efficiency of a radioguided occult lesion localization technique in reoperative thyroid and parathyroid procedures in patients who had undergone previous neck exploration for thyroid or parathyroid disease.
Methods:
Twenty-one consecutive patients who were scheduled for reoperative thyroid or parathyroid surgery were studied. The indication for reoperation was recurrent papillary thyroid cancer (PTC) in eight patients, completion thyroidectomy for PTC in eight patients who had previously undergone a bilateral subtotal thyroidectomy, recurrent goiter in two patients, primary hyperparathyroidism in two patients, and recurrent parathyroid cancer in one patient. Ninety minutes before surgery, 0.1 mL of Technetium-99m (0.2 mCi)-labeled macroaggregated albumin was injected directly into the lesion under ultrasonographic guidance. During surgery, a handheld gamma probe was used to localize and excise the lesions. The background and postexcisional site radioactivities were compared to confirm the completeness of each procedure. The radiation dose in the operating room environment, duration of surgery, and postoperative complication rates were evaluated in all patients. In patients with PTC, the change in serum thyroglobulin (Tg) following surgery was noted.
Results:
Thirty lesions were marked and excised. The postexcisional bed gamma counts (610 ± 141) were markedly decreased compared with the pre-excisional site counts (21,415.8 ± 4993.4; p = 0.0001). The ratio of the postexcisional and background counts (4.6 ± 4.3) was significantly lower than the ratio of the pre-excisional and background counts (173.7 ± 156.4; p = 0.0001). The mean operation duration was 53.3 ± 7.5 minutes. The dose absorbed by the hands of the surgeon was estimated as 0.07 ± 0.02 and 0.15 ± 0.05 millisievert/h when one or three lesions were marked, respectively. One patient developed postoperative transient hypoparathyroidism. After surgery, serum Tg levels dropped to <2 ng/mL in 86% (6/7) of the patients with PTC whose preoperative serum Tg was elevated.
Conclusions:
The radioguided occult lesion localization technique was efficient in the perioperative identification of thyroid and parathyroid tumors in patients who were undergoing reoperation for PTC and hyperparathyroidism.
Introduction
Radioguided occult lesion localization (ROLL) involves the preoperative intratumoral injection of a tracer, which is guided by an imaging method such as ultrasonography (US) or computed tomography (8). This method was first described for the preoperative localization of occult lesions of the breast (9). In the present study, we investigated the excision efficiency of ROLL in performing reoperative thyroid and parathyroid procedures in patients who had undergone previous neck explorations for thyroid or parathyroid disease.
Materials and Methods
This prospective study included 21 consecutive patients (15 women, 6 men; mean age: 41.5 ± 14.3 years) scheduled, between March and November 2009, for reoperative thyroid or parathyroid surgery. The median time between their prior surgery and reoperation was 24 months (range: 3–120 months).
The most common indications for reoperation were recurrent papillary thyroid cancer (PTC) in eight patients and CTx for PTC in eight patients (Table 1). Notably, the patients who had CTx had previously undergone a bilateral subtotal thyroidectomy. In the eight patients with recurrent PTC, their recurrence was detected by the finding of increased serum thyroglobulin (Tg), the presence of positive test for anti-Tg antibody at a time the patients were on thyroid hormone replacement, neck US, and fine-needle aspiration biopsy (FNAB) of suspicious lesions. Elevated levels of serum Tg were present in seven of eight patients with recurrent PTC. In one patient the serum Tg level was normal, but there was an elevation in serum anti-Tg antibodies. These patients had undergone previous operations for thyroid cancer and had received ablative doses of radioiodine (Table 1). The site(s) of recurrence were in both the central and lateral compartments (n = 2), or either the lateral (n = 2) or central (n = 4) compartment (Tables 1 and 2).
CCR, central compartment recurrence; CLND, central lymph node dissection; CTx, completion thyroidectomy; LCR, lateral compartment recurrence; PHPT, primary hyperparathyroidism; T, thyroidectomy; UMRND, unilateral modified lateral neck dissection.
The eight patients who were scheduled for CTx had previously undergone subtotal thyroidectomy elsewhere for presumed benign goiter. However, their final pathology revealed PTC. In the remaining five patients, the indications for reoperation were recurrent goiter (n = 2), primary hyperparathyroidism (PHPT) (n = 2), and recurrent parathyroid cancer (n = 1) (Table 1). The two patients with recurrent goiter had previously undergone thyroidectomy elsewhere for benign goiter, 10 and 4 years previously. A US-guided FNAB was performed for impalpable nodules that were suspicious on ultrasound in these patients. The cytology was read as PTC. Two patients who had undergone previous thyroidectomies were reoperated on for PHPT due to a single parathyroid adenoma. One patient with recurrent parathyroid cancer underwent parathyroidectomy for PHPT elsewhere at 18 months before his reoperation. This patient was referred to our clinic for treatment of recurrent HPT due to parathyroid cancer recurrence, which was presumed to result from possible seeding during the first operation. The final pathology in this patient was parathyroid cancer.
In all patients who were scheduled for CTx, neck US and Tc-99m (99mTc) thyroid scintigraphy were performed preoperatively to localize and estimate the residual thyroid tissue volume. Preoperative and postoperative vocal cord examination was performed by laryngoscopy in all patients to evaluate preoperative recurrent laryngeal nerve (RLN) palsy or the development of postoperative RLN palsy. All patients had serum calcium concentrations determined the morning after surgery. In patients with recurrent PTC, the serum levels of Tg were measured at 3 weeks after surgery, and serum thyroid-stimulating hormone (TSH) and anti-Tg antibodies were measured in patients taking thyroid hormone replacement. Successful excision of recurrent PTC was determined by histopathology showing PTC, by neck US that showed clearance of the preoperative lesion, and by a significant decrease in serum Tg after surgery. Incomplete excision of a recurrent PTC was considered to have occurred if there was no decrease in serum Tg or by persistence of the abnormal lesion on repeat neck US after surgery.
In patients who had reoperations for PTC or recurrent goiter with an FNAB that revealed a malignancy, pre- and postoperative TSH levels were obtained at a time when they were not on thyroid hormone replacement therapy. A postoperative TSH level of >30 mIU/L confirmed successful resection of the remnant thyroid tissue in such patients. In patients who had reoperations for PHPT or recurrent parathyroid cancer, the postoperative parathyroid hormone (PTH) and calcium levels were measured at 1 week, 3 months, and 6 months to confirm the cure of HPT.
The mean postoperative follow-up period was 5.5 months (range: 1–9 months).
Tracer injection technique
A 0.1 mL (0.2 mCi) of 99mTc-labeled macroaggregated albumin (MAA) was injected directly into each lesion under US guidance at 90 minutes before surgery (Fig. 1). Scintigraphy was performed at 30 minutes after injection to visualize the focally increased uptake of radiotracer, corresponding to the impalpable lesion.

Intratumoral injection of 99mTc-labeled macroaggregated albumin under ultrasonography guidance in a patient with central compartment recurrence.
Intraoperative technique
A standard Kocher incision, made through the previous incisions, was used in patients who underwent reoperations for CTx, recurrent goiter, or parathyroid adenoma. The sternocleidomastoid muscle was dissected away from the strap muscles, and both muscles were retracted away from each other. The residual thyroid tissue or parathyroid adenoma was approached through a lateral route. In patients with central compartment recurrence, a median approach was preferred. In patients with recurrent PTC in the lateral compartment, the previous incision was extended, if necessary, to improve exposure.
The background activities were counted from the left and right shoulders with an intraoperative handheld gamma probe (Navigator® surgical γ-probe; USSC). Intraoperative lesion detection was performed with the gamma probe by identifying areas of high radioactivity and recording the count rates for 10 seconds in these areas. Sites with high count rates when compared with background activity were explored, and lesions with high radioactivity counts were excised. After excision, the area was monitored for residual radioactivity. The background activity was compared with the postexcision bed radioactivity to confirm completeness of their procedure.
In patients with PTC who had recurrent metastatic cervical lymph nodes, the site with the highest gamma count was explored to identify the lesion. Next, the recurrent lymph node(s) were excised with the adjacent soft tissues, sparing the vital structures. In such patients, ROLL was used to guide the compartment-oriented lymph node dissection. Berry-picking procedures were not preferred.
The radiation dose to the operating room environment was measured by a Geiger-Müller counter (Biodex; Model 2 survey meter) at 0 and 30 cm from the injection site immediately before the operation (90 minutes after injection).
For statistical analyses, the Mann–Whitney U test was performed using the Statistical Package for Social Sciences software (SPSS 10.0 for Windows). Radioactivity measurements determined by the handheld gamma probe are given as the means ± standard error of the mean. A p-value of <0.05 was considered statistically significant. Informed consent was obtained from all patients participating in the clinical study, which was approved by the ethics committee of our institution.
Results
Preoperative results
Thirty lesions in 21 patients were marked under US guidance by intratumoral injection of 99mTc-labeled MAA. The characteristics of these lesions are summarized in Table 2. No complications were encountered during the injections. Postinjection scintigraphy showed increased focal uptake in the lesions in all patients (Fig. 2).
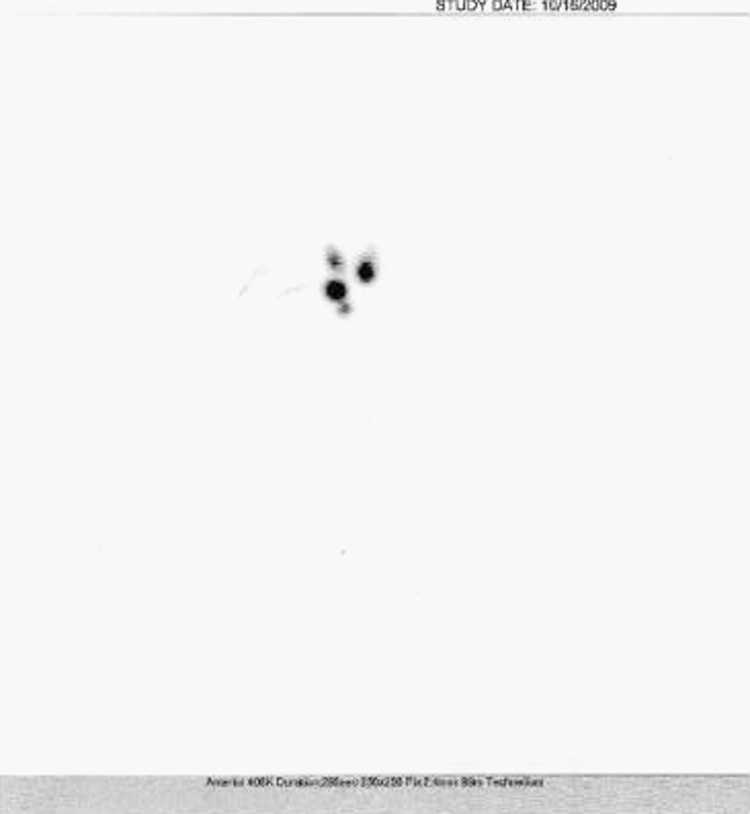
Postinjection scintigraphy of a patient who is scheduled for completion thyroidectomy. The scintigraphy shows increased focal uptake in bilateral residual thyroid tissue that was marked.
Intraoperative results
All of the marked lesions were successfully detected and excised under the guidance of a handheld gamma probe. The mean gamma counts of the excision sites pre- and postexcision were 21,415.8 ± 4993.4 and 610 ± 141, respectively (p = 0.0001) (Fig. 3). The mean ratio of the postexcision and background counts (4.6 ± 4.3) was markedly less than the ratio of the pre-excision and background counts (173.7 ± 156.4; p = 0.0001) (Fig. 4). The mean operation duration was 53.3 ± 7.5 minutes. Radiation doses at 0 and 30 cm from the injection site were 7 ± 2 and 0.4 ± 0.2 milliroentgen/h, respectively. The dose absorbed by the hands of the surgeon was estimated as 0.07 ± 0.02 or 0.15 ± 0.05 millisievert (mSv)/h when one or three lesions, respectively, were marked. Thus, if 100 patients were treated by a single surgeon in 1 year, the absorbed dose to his hands would range 7–15 mSv/year, which is lower than the recommended limit for the general population (50 mSv/year).

The pre- and postexcision mean gamma counts of the marked lesion sites.
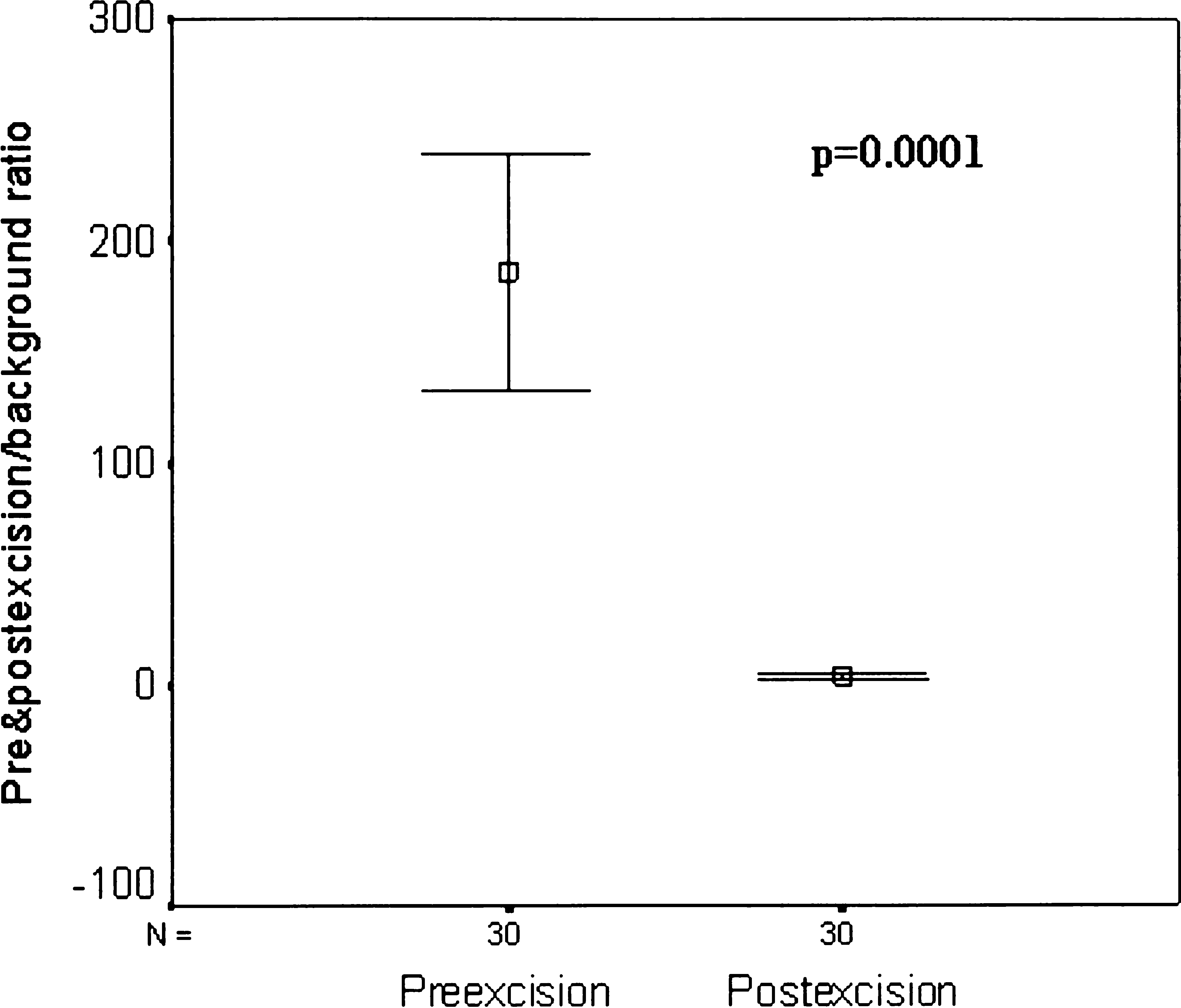
The mean ratio of pre- and postexcision and background gamma counts.
Postoperative results
Postoperative transient hypoparathyroidism developed in one patient who had undergone bilateral residual thyroid tissue resection due to recurrent goiter. The serum calcium levels of this patient returned to normal values within 7 days with oral calcium supplementation. None of the patients suffered loss of voice tone after the operation. The postoperative laryngoscopy results, which were obtained 1 week after surgery, were normal in all patients.
Histopathological examination revealed PTC in patients who were operated on for recurrent PTC (n = 8) or for recurrent goiter with a diagnosis of malignancy on FNAB (n = 2). The margins of the excised lesions were free of thyroid cancer in PTC patients. One of the eight patients who underwent CTX had thyroid carcinoma in the excised residual tissue. In the two patients who had reoperation for PHPT, the histopathological diagnosis was parathyroid adenoma.
Repeat neck US in the eight patients who underwent reoperation for recurrent PTC demonstrated clearance of the preoperatively identified abnormal lesions. Serum Tg levels of seven patients with preoperatively elevated serum Tg levels were significant decreased after surgery (Table 3). In one patient with recurrent PTC and increased serum anti-Tg antibody levels, the anti-Tg antibody levels dropped from 243 to 50 IU/mL after surgery.
Further studies revealed a bone metastasis in this patient.
Recurrence was detected by increased level of anti-Tg antibody in this papillary thyroid cancer patient. Anti-Tg antibody value dropped from 243 to 50 IU/mL after the operation.
Tg, thyroglobulin.
In one patient with recurrent PTC, the serum Tg level dropped from 5000 to 1265 ng/mL. Further examination revealed a bone metastasis in this patient. In the remaining patients, the serum Tg level was <2 ng/mL and none of these patients developed any increase in serum Tg level during the follow-up period. Postoperative TSH values were >30 mIU/L in all of the patients who underwent reoperation for PTC or excision of recurrent goiter with FNAB revealing a malignancy. Two patients who underwent parathyroidectomy for PHPT and one for recurrent parathyroid cancer were normocalcemic at the postoperative 6-month examination and the levels of serum parathyroid hormone were within the normal ranges in these patients.
Discussion
In this study, we investigated the efficiency of the ROLL technique in reoperative thyroid and parathyroid procedures in patients who had previously undergone neck surgery for thyroid or parathyroid disease. The intraoperative use of a handheld gamma probe facilitated the successful localization of nonpalpable lesions that were marked with 99mTc-labeled macro-MAA. In patients with PTC and recurrent metastatic lymph nodes, ROLL enabled compartment-oriented dissection while sparing vital structures. Postoperative transient hypoparathyroidism developed in one patient, and the mean duration of the operation was 53.3 ± 7.5 minutes. Postoperative Tg levels dropped to <2 ng/mL in 86% of patients with PTC and preoperatively elevated serum Tg concentrations.
The recurrence rate of DTC ranges from 10% to 45% and is influenced by the patient's risk factors (10). The most common sites of recurrences are the ipsilateral central and lateral neck nodes, and the contralateral neck nodes and thyroid bed (11). The combined use of sensitive Tg assays and high-frequency neck US, which has an excellent sensitivity for detecting locoregional DTC metastases, has led to the frequent detection of nonpalpable metastatic lesions (12,13). Nonpalpable metastatic lymph nodes that have survived radioactive iodine ablation should be considered for resection (14). During resection, a compartment-oriented approach that includes dissection of the involved compartment without harming the vital structures is preferred over berry-picking procedures (14). However, the identification of nonpalpable lesions embedded in scarred and fibrotic tissues is difficult. Radioguided surgical procedures, hook-needle guided excision, US-guided blue dye injection technique, or intraoperative ultrasonography (IOUS) are recommended, as they allow easier and safer reoperations with a decreased rate of negative explorations (1 –4,15 –19).
In recent years, radioguided techniques have become increasingly popular in thyroid and parathyroid surgery. RGS depends on the accumulation of a specific radioactive tracer in a target tissue. Targeting the tumors with a radioactive tracer facilitates its detection by an intraoperative handheld gamma probe. The most common indications for RGS techniques in thyroid surgery are patients with recurrent or persistent DTC and patients who have to undergo CTx (7). In contrast to the method described here, the most common way that RGS has been performed for reoperative thyroid and parathyroid procedures is to administer radioisotopes by the systemic route before surgery (7). The radioisotopes used for these in vivo diagnostic procedures include 131I, 123I, 99mTc, and 99mTc sestamibi (7,20). 131I is the most commonly used radioisotope in reoperative RGS for iodine-avid DTC.
RGS reportedly improves surgical completeness for lymph node dissection in patients with persistent or recurrent DTC (2,3,15). It also allows the dissection of nonpalpable metastatic lymph nodes or lymph nodes that are resistant to radioiodine treatment (2,3,15,21). Negele et al. showed that RGS led to complete clearance of persistent lymph node metastases by limited recurrent neck surgery in patients with DTC who developed recurrence following lymphadenectomy (15). Additionally, RGS improved the resection completeness in recurrent operations, particularly in anatomically difficult areas. In patients having primary lymphadenectomy, they found that RGS allowed the detection of recurrent disease in scarred and hidden areas.
RGS using 131I for recurrent DTC has some limitations. False-negative and -positive results can alter the efficiency of RGS. False-positive 131I imaging can arise when the radioisotope is taken up by the thymus or submandibular glands, and false-negative imaging can occur when tumor foci are undetectable by the gamma probe (1). The patient must receive a high dose of radiation for diagnostic (nontherapeutic) purposes when 131I is used for RGS (3). Further, 131I ablative treatment has been shown to interfere with subsequent radioiodine uptake in patients with recurrent DTC (22). A significant proportion of such patients have non–iodine-avid recurrences.
The most common radioisotope used for the radioguided resection of non–iodine-avid DTC recurrences, 99mTc sestamibi, is also used during radioguided parathyroidectomy in the reoperative neck (23,24). Minimally invasive radioguided parathyroidectomy is reported to be extremely effective in patients with HPT who had previously undergone neck operations for parathyroid and thyroid disease (5). Rubello et al. found that a low-dose 99mTc sestamibi protocol was effective for reoperative procedures in patients with non–iodine-avid DTC recurrences and in patients with HPT who had undergone unsuccessful parathyroid surgery (23,24). However, some patients with recurrent HPT may have nonavid adenomas (7). An absence of radioisotope avidity limits the use of RGS in reoperative neck procedures. The use of preoperative imaging such as a neck US, sestamibi studies, computerized tomography scan, magnetic resonance imaging and selective venous sampling, and intraoperative parathyroid hormone (IOPTH) monitoring was found to allow for a focused operative approach in reoperative parathyroidectomy (25). In >50% of such patients, the time required for the reoperation was comparable to the original operating time (25). IOPTH monitoring has been reported to provide an accurate prediction of curative operations in reoperative parathyroidectomy (26). Although these adjuncts may be sufficient to achieve the successful resection of an abnormal parathyroid gland from the neck of most reoperative patients, the use of IOUS or ROLL technique can help find abnormal parathyroid glands that are embedded in scar tissue from a previous resection. In our study, abnormal parathyroid lesions were located at previously dissected regions of neck in all patients who underwent reoperations for HPT. The number of patients in whom this was used for parathyroid disease, however, was very small.
The use of RGS in patients with recurrent medullary thyroid cancer (MTC) is more complicated than in patients with DTC, primarily because different radioisotopes are required. The combined use of 111Indium pentetreotide and 99mTc (V) dimercaptosuccinic acid reportedly has 97% sensitivity in detecting recurrent MTC (27). Antibodies specific to carcinoembryonic antigen can be labeled with 99mTc or 111Indium and used to target MTC (7). The use of RGS through a two-step radioimmunotargeting system with carcinoembryonic antigen–specific antibodies reportedly yields 86% accuracy in detecting recurrent MTC (28). Despite these encouraging results, the intraoperative localization of MTC may suffer from false-positives, because of the affinity of the radioisotopes to other tumoral and inflammatory lesions of the head and neck (7). Endogenous somatostatin production can also complicate detection (7).
Triponez et al. performed insertion of a hook needle to central or lateral lymph node metastases in seven patients with recurrent thyroid cancer to perform a focused node dissection (16). This method confirmed the tumor position, allowed a straightforward and successful operation, and decreased the rate of negative explorations. However, the proximity of the nodal metastasis to the carotid artery prevented the use of this technique in one patient, and bleeding after insertion of the hook needle into the anterior jugular vein occurred in one patient.
Preincision US-guided blue dye injection into abnormal lymph nodes is feasible and useful for identification and removal of lymph node recurrences in the reoperative neck (17). IOUS is a useful method to identify nonpalpable locoregional recurrences in thyroid cancer (18). Intraoperative surgeon-performed US influences the extent of resection by identifying and confirming removal of recurrent thyroid cancer or nonpalpable lymph nodes in 31% of patients (19). However, the technique can be challenging in small cervical lesions. IOUS may increase operative times, expertise can vary among institutions, and US image resolution may be superior when performed transcutaneously compared with IOUS used under open incision (29).
The ROLL technique was first used as an alternative to conventional wire-guided localization to localize and resect nonpalpable breast lesions (9) as it might allow faster, more accurate, and simple excision of impalpable breast lesions than wire-guided localization (30). Tukenmez et al. used ROLL to detect and excise metastatic impalpable cervical lymph nodes in two patients with thyroid cancer (31). Intratumoral injection of 20 MBq of 99mTc rhenium colloid was performed under US guidance, and the nonpalpable metastatic lymph nodes were detected and removed by an intraoperative handheld gamma probe. The authors concluded that this radioguided localization method could be safely used to resect cervical lymph node recurrences in thyroid cancer patients who had undergone previous total thyroidectomy and cervical lymph node dissection.
We previously performed RGS with systemic radioisotope administration in patients who were undergoing CTx (32). We found that in our center experienced in endocrine surgery, RGS offered no benefit over conventional surgical exploration, with respect to operation time, complication rates, or surgical completeness. In the previous study, the ratio of the pre-excision and background counts was 8.7 ± 6.1, which is significantly lower than the ratio (173.7 ± 156.4) found in the present study. This difference was probably due to the different radioisotope administration routes used. In the ROLL technique, radioisotope-labeled MAA concentrates in the lesion, and the radiation absorbed by the other tissues is negligible. Systemic radioisotope administration probably increases the tissue background signal activity compared with ROLL and this interferes with lesion localization using the intraoperative gamma probe.
Preoperative imaging studies and anatomical cues should be sufficient to locate the remnant thyroid tissue during a CTx, particularly if the patient had previously undergone a unilateral thyroid lobectomy. However, it is important to emphasize that in our study all of the patients who were scheduled for a CTx had previously undergone a bilateral subtotal thyroidectomy. Therefore, finding the remnant tissue was likely to be more difficult in these patients than if they had undergone a lobectomy and isthmusectomy as there would be bilateral scarring. Therefore, we prefer to use the ROLL technique in such patients.
To our knowledge, our study is the first to investigate the efficiency of ROLL in a large number of consecutive patients with different indications for reoperative thyroid and parathyroid surgery. We found that ROLL is a simple and effective technique to remove radioisotope-labeled recurrent metastatic cervical lymph nodes of PTC, residual thyroid tissue, parathyroid adenoma, or recurrent parathyroid carcinoma in patients who have undergone previous thyroid and parathyroid operations or cervical lymph node dissections. In patients with recurrent metastatic lymph nodes, we used ROLL to localize the lesions and perform a wider dissection, including the adjacent soft tissues. We sought to use ROLL to guide compartment-oriented dissections, rather than using berry-picking techniques, in patients with recurrent thyroid cancer. The high radioactivity counts facilitated tumor detection in scarred tissues, and the observed decreased radioactivity at the excision sites verified resection completeness.
Six of the studied patients had central compartment recurrence due to PTC. Reoperations at the central neck have high complication rates, particularly of RLN palsy. None of the patients who underwent reoperation for central compartment recurrence developed RLN palsy or hypoparathyroidism. The precise localization of lesions by ROLL decreases the need for unnecessary dissections that can lead to an increased complication rate.
There are some limitations of this study. The follow-up period was relatively short in terms of evaluating the long-term results, especially in patients with recurrent PTC. There was no control group in which the ROLL technique was not used to document whether this technique is superior to other imaging approaches with respect to successful excision of the lesion or postoperative complications. Also, as noted, the number of patients with parathyroid disease was quite small.
Preoperative imaging studies and surgeon-performed US help the surgeon to find abnormal lesions surgically in the reoperative neck. IOPTH monitoring is a good predictor of complete resection in reoperative parathyroidectomy (26). However, to use an intraoperative guide would be advantegous in the identification of lesions localized at previously dissected regions. In reoperative thyroid and parathyroid procedures, the use of the ROLL technique has the greatest potential advantage for removing abnormal lesions in previously dissected neck compartments. Future studies are needed to compare the impact of surgeon-performed US and/or IOUS versus use of the ROLL technique on the success of reoperative neck surgery.
In general, pregnant patients should not be given systemic radionuclides, which can cross the placenta (33). Although the dose received by the fetus from ROLL might be well below the threshold dose for deterministic effects, there is always a risk for genetic effects, even at very low doses (34). Therefore, alternative nonradionuclide diagnostic or therapeutic procedures are preferred in pregnant patients whenever possible (33).
In conclusion, the ROLL technique is effective in the peroperative identification of radioisotope-labeled tumoral lesions associated with the thyroid and parathyroid glands in patients who have undergone previous neck operations for thyroid or parathyroid disease. In patients with recurrent thyroid cancer, this technique guides compartment-oriented dissections. The ROLL technique might help decrease the complication rates associated with reoperations, particularly in patients with central neck recurrence, by improving resection completeness without unnecessary dissections. Further studies with a larger number of patients are needed to document the definite impact of this technique on reoperative thyroid and parathyroid procedures.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.