
Abstract

Thursday, September 24, 2009
Molecular Endocrinology Group, Division of Medicine & Medical Research Council Clinical Sciences Centre, Imperial College London, Hammersmith Hospital , London, United Kingdom
Thyroid Hormone Metabolism and Regulation Thursday Oral Basic 11:15 AM
Both hypothyroidism and thyrotoxicosis are associated with increased fracture risk. T4 is the predominant circulating thyroid hormone, but target cell responses are determined by local availability of the active hormone T3. The D1 and D2 iodothyronine deiodinases convert T4 to T3 in peripheral tissues; in bone conversion is restricted to osteoblasts. To investigate the role of locally produced T3 in bone, we characterized mice harboring deletion of Dio2 (D2KO) or both Dio1 and Dio2 (D1/D2KO) in which circulating T3 levels are normal.
Mice were examined during growth and in adulthood between postnatal days 1 and 112. Skeletal samples were analyzed by histology, dynamic histomorphometry, digital X-ray analysis and backscattered electron scanning electron microscopy. Biomechanical characteristics were determined by destructive three point bend tests.
Adult D2KO mice had increased bone mineralization and brittle bones that underwent abrupt high energy fracture without normal plastic deformation following mechanical loading. These biomechanical abnormalities were accompanied only by reduced osteoblastic bone formation whereas skeletal development, linear growth and osteoclastic bone resorption were normal, indicating that D2KO mice have a discrete defect of osteoblast function. Additional deletion of D1 in D1/D2KO mutants did not modify the D2KO skeletal phenotype.
These data identify a novel and essential role for D2 in osteoblasts. The restricted expression of D2 in osteoblasts suggests that their T3 content is enhanced relative to other bone cells and that increased T3 availability is essential for normal osteoblast function. As in other tissues, D2 activity in osteoblasts is increased in hypothyroidism but reduced in hyperthyroidism, thus providing a physiological mechanism to buffer the detrimental effects of altered thyroid status on the skeleton. We propose that optimal bone mineralization and strength are maintained over the physiological range of systemic thyroid hormone concentrations by the regulated activity of D2 in osteoblasts.
Response to Tyrosine Kinase Inhibitors Differs by RET Genotype
Thyroid Cancer Thursday Oral Basic 11:30 AM
Germline and somatic point mutations in the RET receptor tyrosine kinase result in medullary thyroid cancer (MTC). Mutations in the cysteine-rich domain, most commonly C634R, result in RET activation via covalent dimerization. Intracellular tyrosine kinase domain mutations, most commonly M918T, activate RET by inducing conformational changes in the kinase activation loop. Given these differing mechanisms of RET activation, we hypothesize that inhibition of RET activation by different tyrosine kinase inhibitors (TKIs) may vary by RET genotype.
RET mutations were created by site-directed mutagenesis of RET full-length, wild-type (WT) cDNA. Chinese Hamster Ovary cells were transiently transfected with plasmids encoding WT, C634R, or M918T RET isoforms. Cells were treated with TKIs currently in clinical trials for MTC at concentrations of 0-5000 nM, and RET protein was analyzed for activation status (autophosphorylation) by sequential immunoblotting for phospho-RET and total RET. Western blots were quantified using photodensitometry and IC50s were calculated.
Drug sensitivity of RET oncoproteins associated with MTC was determined by inhibition of autophosphorylation. The IC50s of each TKI for treatment of WT RET, C634R, and M918T are presented in Table 1. For all tested drugs, WT RET was the most potently inhibited isoform. With the exception of motesanib, other TKIs were much more potent against C634R than M918T. Vandetanib and sunitinib were both 5-fold more potent on C634R than M918T, sorafenib 3-fold more potent, and axitinib 9-fold more potent. Axitinib and motesanib demonstrated minimal ability to inhibit M918T, even at 5000 nM concentrations.
RET kinase is a therapeutic target for the treatment of MTC. Notably, response in other malignancies successfully treated with TKIs is significantly influenced by tumor genotype. Here, we demonstrate that the type of RET mutation strongly influences in vitro response to TKIs in a cell based system. These findings are similar to those in other malignancies, where mutations in the activation loop of the tyrosine kinase result in reduced sensitivity to TKIs. These data suggest that MTC tumor genotype may be predictive of response to individual TKIs that target RET.
Variables Measured Using Color Doppler and B Mode Ultrasound
Thyroid and Development Thursday Oral Basic 11:45 AM
Thyroid hormones (THs) are important for fetoplacental development. Monocarboxylate transporter 8 (MCT8) is a plasma membrane TH transporter present in the human placenta from 6 weeks of gestation. Human intrauterine growth restriction (IUGR) is associated with increased placental to fetal weight ratios and placental MCT8 expression, but reduced fetal circulating concentration of THs compared to gestationally-matched normal fetuses.
Using the MCT8-null mouse model, MCT8−/0 males and MCT8+/− females were mated and paired male embryo and placental samples [MCT8+/0 (n = 16) and MCT8−/0 (n = 7)] were collected at E18.5. To assess the effect of silencing (siRNA) and upregulating (plasmid transfection) MCT8 in-vitro, primary cytotrophoblasts (CTs) were isolated from human term placentae from normal (nCT) and IUGR (iugrCT) pregnancies. The human cell line SGHPL-4 was used as a model of 1st trimester extravillous trophoblasts.
MCT8−/0 embryos showed an increased placental to fetal weight ratio by 30% compared to MCT8+/0 (P < 0.01). Compared to nCTs, iugrCTs showed increased MCT8 expression, decreased cell survival (MTT assay; P < 0.01) and increased apoptosis (Caspase 3/7 activity assay; P < 0.01) with T3 treatment. In nCTs, MCT8 upregulation decreased cell survival by 20% (P < 0.001) whilst silencing MCT8 increased cell survival by 20% (P < 0.01) and apoptosis by 30% (P < 0.05); all independently of T3. MCT8 did not affect nCT syncytialisation (total HCG secretion). In SGHPL-4s, MCT8 upregulation increased the pro-invasive effect of T3 into Matrigel® by 2-fold compared to control (P < 0.05). Contrary to nCTs, silencing MCT8 decreased apoptosis in SGHPL-4s by 10% irrespective of T3 (P < 0.05).
Findings of increased placental/fetal weight ratios using the MCT8-null mouse model support the hypothesis that MCT8 is likely to play a critical role in placentation. Changes in placental size may be part of a compensatory effect to optimise placental function. Increased MCT8 expression and altered T3-responsiveness of iugrCTs may be a contributory factor to the dysfunction of the fetoplacental unit in IUGR by adversely affecting CT survival. MCT8 may also play a crucial role in trophoblast invasion and placental modelling in early pregnancy.
Inhibition of Nuclear Factor-κb Activity Decreases Cancer Cell Invasion and Promotes TNFα-Induced Apoptosis in Thyroid Cancer Cells
Thyroid Cancer Thursday Oral Basic 12:00 PM
Nuclear factor-κB (NF-κB) activation is associated with tumor survival, proliferation, angiogenesis, and invasion/metastasis. Evidence for a definitive role for NF-κB signaling in thyroid cancer is incomplete. In this study, we have genetically and pharmacologically inhibited NF-κB in an effort to define its role in thyroid cancer growth and progression.
Two anaplastic thyroid cancer cell lines, SW1736 (BRAF V600E) and C643 (H-RAS G13R), and two papillary thyroid cancer cell lines, BCPAP (BRAF V600E) and TPC1 (RET/PTC1) were used. NF-κB activation was assessed via luciferase reporter assay and Western blot analysis. Cell proliferation and survival were determined by viable cell counting and MTT assays. Cell invasion through Matrigel was determined in Boyden chamber assays.
CDDO-Me, a pharmacologic inhibitor of IKKβ, blocked tumor necrosis factor (TNFα)-induced NF-κB translocation and attenuated proliferation and survival of all four cell lines. Invasion was inhibited by 50% in two cell lines tested (BCPAP and TPC1). As a complementary genetic approach, the canonical NF-κB pathway was inhibited via over-expression of dominant-negative IκBα (mIκBα), resulting in diminished NF-κB transcriptional activity and TNFα-induced NF-κB translocation in the four cell lines. However, NF-κB inhibition by this method had no effect on proliferation or survival of cells cultured in 10% or 0.5% serum, indicating that the effects of CDDO-Me on cell proliferation was not through the classical NF-κB pathway. Invasion assays demonstrated that mIκBα expression in these cell lines resulted in a 50% decrease in only SW1736 and TPC1 cell invasion. Finally, while these cell lines were resistant to TNFα-induced apoptosis under basal conditions, measurement of cell viability in response to TNFα treatment and mIκBα expression demonstrated a two-fold increase in apoptosis in SW1736 and TPC1 cells.
These findings show that NF-κB inhibition may be of therapeutic utility in thyroid cancer. While the antiproliferative effects observed with CDDO-Me are likely due to alternative mechanisms, these studies clearly demonstrate that NF-κB inhibition may block cancer cell invasion and promote apoptosis under conditions requiring NF-κB for survival.
Thyroid Cancer Research Laboratory, Endocrine Surgery, Massachusetts General Hospital, Harvard Medical School , Boston, MA
Thyroid Cancer Thursday Oral Basic 12:15 PM
B-RafV600E is the most frequent genetic alteration (29-83%) in papillary thyroid cancer (PTC); transforms normal thyroid cells and does not require Ras function to induce cell-growth. However, mechanisms by which B-RafV600E induces tumor aggressiveness are not fully understood. We aimed to identify and validate a B-RafV600E genome-wide signature associated with tumor progression in PTCs.
We applied a new genome-wide microarray analysis to identify gene sets with the same function associated with PTCs-B-RafV600E vs. PTCs-wild type (wt) B-Raf, and normal thyroid (NT) tissue samples. Gene validation was performed with real time-PCR, and for some genes using short-hairpin-RNAs (sh), three dimensional cultures (3D), and a novel orthotopic mouse model using the human thyroid cancer cell line 8505c (B-RafV600E+/+). Seven of 17 (41.1%) up-regulated gene sets were mainly enriched in functionally interconnected genes that belong to extracellular matrix (ECM) remodeling: cell-adhesion molecules (integrins, CD44 and fibronectin-1), or key-regulators of ECM (TSP-1 and TGF-beta1), or proteases (cathepsins). PTCs-B-RafV600E showed higher mRNA expression levels of these genes vs PTCs-wt-B-Raf and NT. Importantly, the only down-regulated gene set included genes involved in the establishement of cell-polarity in epithelial cells. In vitro knockdown of B-RafV600E by sh in the 8505c cells resulted in a dramatic reduction of cell adhesion, and migration/invasion in 3D assays. In addition, B-RafV600E over-expression in normal human cells conferred invasive properties. Finally, sh-B-RafV600E 8505c cells were implanted orthotopically into the thyroid of immunocompromised mice. Five weeks post-tumor implantation, animals with orthotopic tumor implants using B-RafV600E-sh 8505c cells have significantly smaller tumor volume and less lymph-node and lung micro-metastases than those injected with sh-control 8505c cells. B-RafV600E's role in aggressive PTCs may be linked to the expression of ECM genes, which may represent new molecular markers and therapeutic targets in this type of cancer.
Medicine, Obstetrics & Gynecology, Touro University College of Medicine , Hackensack, NJ
Thyroid Diseases Thursday Oral Clinical 11:15 AM
Whether or not all women should be screened for thyroid disease during pregnancy is controversial. The goal of the present study is to determine if treatment of thyroid disease during pregnancy decreases the incidence of adverse outcomes, and to compare the impact of universal screening (US) versus case-finding (CF).
Women were recruited from two ambulatory clinics in Southern Italy. Women in the first trimester were randomly assigned to the US group or CF group. Women in both groups were stratified as high-risk or low-risk based on risk factors for thyroid disease. All women in the US group, and high-risk women in the CF group, were immediately tested for fT4, TSH and TPO antibody Low-risk women in the CF group had their sera tested postpartum. Out of 4657 women, 95 were excluded on the basis of known thyroid disease and 46 women dropped out. Women were randomly assigned by computer program to the US (n = 2257) or CF group (n = 2259). Intervention consisted of levothyroxine in women with a TSH above 2.5 mIU/l in TPO-Ab+women and antithyroid medication in women with a suppressed TSH and elevated fT4. The primary outcome measure was the total number of adverse outcomes during pregnancy or in the immediate neonatal period to the mother or fetus, controlling for clustering of outcomes within women.
3590 women (78%) were classified as low risk (1808 in the case-finding group, 1782 in the screening group). Low-risk women in the screening (treated) group were less likely to have adverse outcomes than those in the case-finding (untreated) group (OR = 0.48, 95% CI = [0.33,0.71]). The number needed to screen to detect one hypo- or hyperthyroid woman in the low-risk group was 36 [28,49]; the number needed to treat to prevent one hypo- or hyperthyroid woman from experiencing adverse outcomes was 1.8 [1.4,2.6]. Overall, screening low-risk women prevented 2.48% of adverse events that would have otherwise been expected (p = .012). Treatment of thyroid hormonal abnormalities during pregnancy results in a significant decrease in adverse outcomes. All high-risk women should be screened for thyroid disease in the first trimester and serious consideration should be given to universal screening.
Ultrasound Pattern Recognition of Benign Thyroid Nodules: What Not to Biopsy?
Thyroid Imaging Thursday Oral Clinical 11:30 AM
Several studies have attempted to analyze the relationship between specific sonographic features of thyroid nodules and malignancy, all limited in specificity and sensitivity. Rather than individual features, we evaluated the accuracy and reproducibility of a “pattern” approach, in the identification of benign, rather than malignant, thyroid nodules.
In 1232 FNA biopsies, between 2005 and 2007, 500 random nodules were reviewed for accuracy of individual sonographic features and of ten discrete patterns in the prediction of benignity. Following this, 75 consecutive biopsied nodules were shown to three blinded readers, trained in this pattern approach. The results of their analysis was compared to the biopsy results.
We found that the grouping of thyroid nodules into patterns of morphology was extremely accurate in the identification of benign nodules. 4 patterns were identified: spongiform, cyst with colloid clot, giraffe pattern, and diffusely hyperechoic, which had a 100% specificity for benignity. The performance of the three blinded readers confirmed these findings, leading us to believe that this approach is reproducible.
Recognition of morphologic patterns is an accurate method to identify benign thyroid nodules. Since benign nodules greatly outnumber malignant, this approach may allow for a substantial decrease in the number of unnecessary biopsies.
Screening Pregnant Women for Thyroid Dysfunction
Thyroid Diseases Thursday Oral Clinical 11:45 AM
Thyroid dysfunction during pregnancy has been shown to be associated with various adverse pregnancy outcomes. Therefore, it is imperative to screen pregnant women for thyroid diseases. However, the screening strategy is a debate. The objective of our study was to investigate the differences of identifying pregnant women with thyroid dysfunction and autoimmune disorders between universal screening strategy and targeted high-risk case-finding strategy of pregnant women.
We tested thyroid-stimulating hormone (TSH), total thyroxin (TT4), free thyroxin (FT4) and thyroid peroxidase antibodies (TPOAbs) in 271 pregnant women during their first antenatal visit (second trimester), thyroglobulin antibodies (TgAbs) were checked in 222(81.9%). Based on the high-risk factors of case-finding strategy recommended by the Endocrine Society clinical practice guideline for the management of thyroid dysfunction during pregnancy, 52 pregnant women with more than one of the high-risk factors were classified as a high-risk group, others without high-risk factors were divided into a low-risk group. We assessed thyroid function based on the second trimester-specific reference ranges of thyroid function and antibodies established by our laboratory.
The prevalence of elevated TSH (>4.00 mIU/L) in the high-risk group was 13.5%, higher than that in the low-risk group (RR 7.370, 95%CI 2.241–24.243, P = 0.0006). There were higher TPOAb positive rate (TPOAb > 25.50 IU/ml) and TgAb positive rate (TgAb > 27.60IU/ml) in euthyroid pregnant women in the high-risk group, than those in the low-risk group(RR 7.019 and 6.357, respectively, 95%CI 1.733–28.438 and 2.615–15.455, respectively, P = 0.0069, <0.0001, respectively). Nonetheless, there were 36.4% of women with elevated TSH, 37.5% of TPOAb-positive euthyroid women and 38.9% of TgAb-positive euthyroid women in the low-risk group.
Targeted thyroid diseases detecting of only the high-risk population would miss about 36% of pregnant women with overt/subclinical hypothyroidism and about 38% of euthyroid pregnant women with thyroid antibody positive.
Neuroscience and Mental Health Program, Research Institute, The Hospital for Sick Children , Toronto, Canada
Thyroid and Development Thursday Oral Clinical 12:00 PM
Extensive animal research has shown low pre- and postnatal thyroid hormone (TH) levels affect vision and memory and lead to brain abnormalities. Behavioral findings are supported by human studies of children with congenital hypothyroidism (CH) or hypothyroxinemia of prematurity or offspring of women with hypothyroidism in pregnancy. While our recent studies show hippocampal atrophy in CH, we still do not know if the other conditions are similarly affected and where effects are localized within brain systems dedicated to vision and memory abilities.
Fifteen children with CH and 21 normal controls (C, 10–16 yrs) underwent neuroimaging (1.5T scanner). T1-weighted images were analyzed using voxel-based morphometry (VBM), an advanced neuroimaging tool parcellating brain into grey and white matter and CSF tissue subcomponents to identify significant clusters differentiating groups.
CH showed 37 regions of reduced grey matter and one region of increased grey matter relative to C. For C vs CH, VBM identified two very large clusters of >30,000 voxels in each frontal lobe as well as more grey matter in bilateral hippocampus (near entrorhinal cortex and subiculum), multiple regions belonging to visual pathways (e.g., left calcarine sulcus, bilateral occipital/parietal sulcus, right cuneus, right fusiform gyrus, right MT), and bilateral amygdala and putamen. For CH vs C, CH showed more grey matter only in a region of unknown function.
Statistical parametric map showing regions of reduced grey matter volumes in CH compared with Controls.

In CH, neurogenesis is reduced in brain regions subserving cognitive abilities on which these children consistently show difficulty. This effect likely reflects their lack of TH from onset of disease until euthyroidism is achieved following early treatment. Although children with CH do not typically manifest executive function difficulties, which normally reflect frontal lobe abnormalities, the large frontal clusters observed presently may signify disrupted functioning of larger systems (e.g., frontal/parietal, frontal/hippocampal circuits) versus localized frontal deficits. Additionally, these system deficits may be contributing to observed visuospatial and memory deficits.
Internal Medicine, Federal University of Parana , Curitiba, Brazil
Thyroid Nodules and Goiter Thursday Oral Clinical 12:15 PM
The efficacy and safety of an intramuscular (i.m.) injection of modified-release recombinant human TSH (MRrhTSH) 24 h before oral 131I to achieve shrinkage of symptomatic benign multinodular goiters (MNG) was evaluated in a global, randomized, single-blinded trial.
One hundred forty one goiter patients were screened to randomize 96 patients, of whom 95 received either a single i.m. injection of placebo (n = 32), 0.01 mg MRrhTSH (n = 30) or 0.03 mg MRrhTSH (n = 33), followed the next day by 131I therapy calculated to deliver 100 uCi/mL based on the thyroid 131I uptake prior to the i.m. injection. The primary endpoint was goiter shrinkage by CT at 6 months compared to baseline goiter volume. The mean patient age was 57 yrs (85% females, 83% Caucasians), with baseline goiter volumes of about 100 mL (range 32–242 mL). The average 131I dose was 36 mCi.
For the placebo and the 0.01 and 0.03 mg MRrhTSH groups, the mean goiter shrinkages at 6 months were 23%, 23% and 33%, respectively (placebo and 0.01 mg MRrhTSH vs. 0.03 mg, P < 0.05). A responder was predefined as a patient who achieved ≥28% goiter shrinkage at 6 months, a number determined by literature review. The percentages of responders in the three groups were 25%, 37% and 64%, respectively. There were no related serious adverse events.Transient hyperthyroidism occurred in 6%, 27% and 30% of the patients in the groups, respectively.
MRrhTSH at the dose of 0.03 mg i.m. plus oral 131I achieved significantly more goiter shrinkage at 6 months than did placebo or the 0.01 mg dose. Although transient hyperthyroidism occurred in some patients, MRrhTSH was well tolerated.
Inhibition of Eat Development by Thyroid Antigens Administered in a Novel TH1 Mucosal Adjuvant
Autoimmunity Thursday Poster Basic
Experimental autoimmune thyroiditis (EAT) is a mouse model of human autoimmune thyroiditis. Several approaches have tried to regulate the development of EAT, often by the repeated administration of a small dose of native or denatured antigen. However, the effect of a novel nanoemulsion (NE) adjuvant on mouse thyroglobulin (mTg)-induced EAT is still unknown.
In the present study, we investigated the effect of administering antigen in a novel NE adjuvant on the development of mouse thyroglobulin (mTg)-induced EAT. NE is a surface active, soybean oil emulsion that can deliver antigen to nasal mucosal dendritic cells, producing systemic TH1 immunity to exogenous antigens. CBA/J female mice received either NE or NE with mTg twice by nasal administration two weeks apart. One week after the second nasal delivery, mice were immunized intravenously with mTg and LPS twice. The levels of anti-mTg IgG antibodies, IL-4, IL-10, IL-17 and IFN-gamma were measured.
Compared with NE-treated animals, NE/mTg treated mice developed a milder form of the disease with a significant decrease in mononuclear cell infiltration in the thyroid. T cell proliferation was significantly lower in NE/mTg-treated mice than in mice receiving NE alone. The production of anti-mTg IgG antibodies, as well as subsets of IgG1, IgG2a, IgG2b were significantly decreased in NE/mTg-treated mice compared to NE-treated mice. The production of serum cytokines was determined by Luminex assay and the result was compared between NE and mTg/NE groups. Compared with NE treatment, NE/mTg treatment significantly increased the level of IL-10 but reduced the level of IFN-gamma. There was no difference in IL-4 and IL-17 levels between NE treatment and NE/mTg treatment.
Taken together, these results indicate that low dose autoantigen in NE effectively increases Th2 (IL-10) and decreases Th1 (IFN-gamma) cytokines, leading to suppression of the autoimmune response and the progression of EAT.
School of Medicine & Dentistry, University of Rochester , Rochester, NY
Autoimmunity Thursday Poster Basic
Thyroid Eye Disease (TED) is an autoimmune process primarily associated with Graves' Disease. Imaging is used to classify patients into 2 groups: Type I with expansion of the fat compartment and Type II with enlargement of the extraocular muscles. Some patients have both components. We tested the hypothesis that orbital fibroblasts (OFs) from Type I TED were prone to adipogenesis, whereas OFs from Type II TED were prone to proliferation.
CT scans and tissue samples were obtained from TED and non-TED patients undergoing orbital surgery. OFs from 3 Type I, 3 Type II, and 2 non-TED patients were treated with transforming growth factor beta-1 (TGFβ1) and/or insulin-like growth factor-1 (IGF1), 10% fetal bovine serum (FBS), co-culture with autologous T-cells, pioglitazone, or 15d-prostaglandin J2 (15d-PGJ2). Proliferation and adipogenesis were measured using the tritiated thymidine assay after 72 hours and the AdipoRed assay after 8 days, respectively. A mixed effects model was used to compare proliferation and adipogenesis of OFs from the three groups.
There was a trend toward more proliferation in Type II OFs compared to Type I OFs with autologous T-cell co-culture (P = 0.0633). Type II OFs proliferated more with 5 ng/ml TGFβ1 (P < 0.0001) and 10% FBS (P < 0.0001) than Type I OFs. Type I OFs proliferated more than Type II OFs with combined 5 ng/ml TGFβ1 and 5 ng/ml IGF1 (P = 0.044) treatment. However, proliferation was lower with TGFβ1 and IGF1 in combination than with TGFβ1 alone for all groups. Type I OFs had more adipogenesis than Type II OFs with 5 μM 15d-PGJ2 (P = 0.0259) and 10 μM pioglitazone (P = 0.006) treatments.
Type II OFs were driven to proliferate more than Type I OFs, while Type I OFs were driven to adipogenesis more than Type II OFs. Further studies are needed to understand IGF1's role in modulating TGFβ1's effects on OFs. This study demonstrates the heterogeneity of OFs from Type I and Type II TED patients. Further investigation is required to determine if factors that influence the fate of TED OFs are genetic, environmental, or a combination of the two. Hopefully, this line of research will provide a basis for more targeted therapies based on the type of TED. Research supported by: RO1 EY11708, TL1 RR024135.
Dept. of Medicine I, Gutenberg University , Mainz, Germany
Autoimmunity Thursday Poster Clinical
Disfiguring proptosis and dysthyroid optic neuropathy (DON) lead to cosmetic impairment and loss of vision in severe Graves orbitopathy (GO). Surgical decompression of the crowded orbit offers a valid therapeutic option.
150 consecutive patients (median age 54 years, 113 female, 96 smokers, 280 orbits) with severe GO had a novel endonasal bone and transpalpebral fat decompression surgery at a university joint thyroid-eye-clinic. A complete multidisciplinary endocrine and ophthalmic assessment was performed pre, three and 12 months post-operatively.
Cosmetic reasons (196 orbits, 73%), DON (67, 24%), and one corneal ulceration (0.4%) were the indications for surgery. The medial orbital wall and the palpebral adipose tissue (median 8 ml, range 3–21 ml) were removed. Preoperatively, relative afferent pupillary defects and vision field defects were noted in 16% and in 43% of DON-patients but in 8% only after 12 months (p < 0.001). Proptosis decreased from 23 mm (13–32) to 20 (10–30) and 19 mm (11–30) at 3 and 12 months, respectively (p < 0.001). Lid fissure width decreased by 2 mm, p = 0.0001. Upgaze intraocular pressure dropped from 23 mmHg (10–44) by 4 mmHg at 12 months (p < 0.001). Median severity score (NOSPECS) declined from 7 points (2.5–13) to 4 (1–11) and 3.5 points (1–7) at 3 and 12 months (p < 0.001). Subjective eye signs significantly decreased in 89% of the patients and satisfaction rate was >90%. NOSPECS and intraocular pressure decreased less in GO smokers vs. non-smokers (both p < 0.001). Two patients (1.3%) only complained about new-onset constant diplopia three months after decompression, while 22/150 (15%) patients reported de-novo inconstant or intermittent diplopia. Prisms and/or subsequent squint surgery corrected all cases of diplopia. Preoperative coexistent sinusitis (n = 97, 65%) was successfully treated by decompression surgery in all cases. No major side-effects were registered.
The combined endonasal bone and transpalpebral fat orbital decompression is a safe and efficient therapy for severe GO.
PPAR-Alpha Agonists Are Stronger Inhibitors Than PPAR-Gamma Agonists in Modulating Alpha and Beta Chemokines in Thyrocytes, Fibroblasts and Preadipocytes from Patients with Graves' Ophthalmopathy
Autoimmunity Thursday Poster Clinical
Human thyrocytes, orbital fibroblasts, and preadipocytes from Graves' ophthalmopathy (GO) patients produce large amounts of CXCL9, CXCL10, CXCL11 when stimulated by IFN-gamma and TNF-alpha; furthermore, PPAR-gamma agonists dose-dependently suppressed IFN-gamma+TNF-alpha-induced CXC chemokines release, and it has been demonstrated that PPAR-alpha agonists may have an anti-inflammatory action.
The effects of IFN-gamma and TNF-alpha stimulation and of increasing pharmacological concentrations of PPAR-alpha agonists (ciprofibrate, fenofibrate, gemfibrozil) or PPAR-gamma agonists (pioglitazone, rosiglitazone) on alpha-chemokines CXCL9, CXCL10, CXCL11 and beta-chemokine CCL2 secretion in primary cultures of thyrocytes, fibroblasts, and preadipocytes from GO patients were tested.
In primary thyrocytes, fibroblasts and preadipocytes cultures, from patients with GO, CXCL9, CXCL10 and CXCL11 were undetectable in the supernatant. IFN-gamma dose-dependently induced CXCL9, CXCL10 and CXCL11 release, whereas TNF-alpha alone had no effect on CXCL9, CXCL10 and CXCL11. However, the combination of TNF-alpha and IFN-gamma had a significant synergistic effect on CXCL9, CXCL10 and CXCL11 secretion. IFN-gamma or TNF-alpha or the combination of TNF-alpha and IFN-gamma significantly stimulated also the secretion of CCL2. Treatment of thyrocytes with ciprofibrate, fenofibrate or gemfibrozil (added at the time of IFN-gamma and TNF-alpha stimulation) dose-dependently inhibited (p < 0.001) the release of CXCL9, CXCL10 and CCL2 at a stronger (p < 0.001) level than PPAR-gamma agonists (pioglitazone, rosiglitazone). Similar results were observed in fibroblasts or preadipocytes. PPAR-alpha agonists alone had no effect and did not affect cell viability or total protein content in thyrocytes, retrobulbar fibroblasts and preadipocytes.
In GO: 1) thyrocytes and retrobulbar cell types participate in the self-perpetuation of inflammation by releasing CXCL9, CXCL10, CXCL11 and CCL2 chemokines under the influence of cytokines; 2) PPAR-alpha activation plays an inhibitory role in this process, stronger than that of PPAR-gamma agonists.
UOC di Medicina Generale , PO S. Giovanni Bosco, Naples, Italy
Autoimmunity Thursday Poster Clinical
Aim: The Helicobacter Pylori (HP) infection is worldwide diffused. In the civilized countries is present in nearly 50% of the population. In many studies, the rate of HP recurrence, after the drug eradication, is about 3% for one year. Recently, we have demonstrated the high rate of prevalence of the HP infection in patients with the ongoing Graves' Disease. The aim of our work was to investigate if the autoimmune disease increases the rate of HP recurrence after a successful drug regimen of eradication.
Materials and Methods: The HP presence was investigated on a fresh stool sample using an immunoassay amplification technology test (IDEIA Hp StAR, DakoCytomation). In an HP-positive group of hyperthyroid GD patients at first diagnosis and control subjects we performed the standard eradication therapy with amoxicillin 1 gr, clarythromicin 0,5 gr and esomeprazole 20 mg b.i.d. for one week. After five weeks we tested the obtained HP eradication on the stool sample. We selected 15 HP-eradicated GD patients (medium age 38 ± 2 SD years) and 19 HP-eradicated subjects as control (medium age 40 ± 2.1 years). After at least six months (13 ± 3.2) we tested newly both the GD patients, now euthyroid under methimazole treatment, and the controls for the presence of HP. We analyzed the obtained results using statistical test such as the Fisher Test.
Results: Seven of 15 GD patients resulted newly infected by HP versus 1 of 19 in the control population. The rate of recurrence of the infection was significantly different between the patients affected by GD (46,6%) versus the respective controls (5,2%, P = < 0.001).
Conclusions: The GD is an important predisposing factor, probably independent by the hormonal status, for the HP infection and its recurrence.
Iodine Status of the U.S. Population, Nhanes 2005–2006
Iodine Uptake and Metabolism Thursday Poster Basic
Since 1971, the general U.S. population has been monitored for dietary iodine sufficiency by urinary iodine (UI) measurements through the National Health and Nutrition Examination Survey (NHANES). This report presents the UI levels for the population participating in NHANES 2005–2006.
In 2005–2006, approximately 5,000 participants per year were selected to participate in NHANES. Household interviews and physical examinations were performed. Urinary iodine-level assessments were determined on a random subsample of 2649 participants aged 6 years and older.
The median UI level for the general U.S. population in 2005–2006 was 164 μg/L (95% confidence interval [CI] 154–174). Children had a higher UI level than adolescents and adults. Among all (pregnant and non-pregnant) women of reproductive age, the median UI level was 120 μg/L (95%CI 108–138), 37.1 ± 17.6 % of pregnant women had a UI level <100 μg/L and 10.7 ± 10.4% of pregnant women had a UI level <50 μg/L.
These findings affirm the stabilization of the UI level and the adequate iodine nutrition in the general U.S. population since 2000. However, subgroups of the population have medium urinary levels either excessive or insufficient with regards to iodine status. Children 6–11 and adults 70 years and older have urinary iodine levels in excess of levels determined by WHO to be adequate and may put them at risk of hyperthyroid induced iodine disorders. While women of child bearing age, and in particular pregnant women have urine iodine levels that are inadequate, thus placing this group at high risk for iodine deficiency disorders. Learning Objectives: 1. Define the current iodine status of the US population, to include sub-populations of children and women of child-bearing age. 2. Identify health outcomes related to insufficient iodine nutrition in women of child-bearing age. 3. Describe health outcomes related to elevated iodine nutrition.
Health Sciences Group, Exponent, Inc. , Menlo Park, CA
Iodine Uptake and Metabolism Thursday Poster Basic
Three investigators of this abstract had cats that developed hyperthyroidism, similar to human toxic nodular goiters (TNG), and were treated with I-131 or thyroidectomy. The etiology of TNG in cats remains unknown although it is considered multifactorial. Since there are no reports of RAIU values in thyrotoxic cats, we speculated that iodine excess (Jod-Basedow) might be one cause.
Iodine content was measured in 71 randomly-selected canned, pouched, and dry cat foods from three areas of the U.S. to determine whether iodine concentrations in current commercial cat foods meet recommendations for supplementation, whether regional differences in iodine concentrations exist, and whether seafood ingredients are associated with iodine concentrations.
Canned foods' iodine concentrations ranged from 0.9 to 67.7 mg/kg dry weight, nearly an 80-fold variation, while pouched and dry foods each varied over 3-fold between minimum and maximum values. Iodine concentrations in cat foods from Northern California, Florida, and Indiana did not differ overall, with mean± standard deviation values of 8.5 ± 15.7, 8.1 ± 15.3, and 7.5 ±14.7 mg/kg dry weight, respectively. However, iodine concentrations for specific foods varied across the three locations, with a 13-fold variation in one brand of dry food (0.2–2.6 mg/kg dry weight). The highest iodine concentrations were associated with “fish”, salmon, and salmon broth as the first five ingredients, though the lowest concentration among cans had salmon as the fourth ingredient.
A previous review of iodine supplementation for cat foods revealed that recommendations for feline iodine intake changed in the 1970s, when this disease was first reported. Recommendations were revised again in 2006: under these, a 4-kg cat would consume 87.5 mcg iodine/day based on a 350-mcg iodine/1000-kcal metabolizable energy diet. The dramatic variation here among canned foods (resulting in possible ingestion of approximately 62–4643 mcg iodine/day) suggests that the disparity in iodine concentrations may lead to development of nodular hyperplasia and later clinical hyperthyroidism, if cats consume diets that are at first iodine deficient and later contain excessive iodine, as the human experience has shown.
Pathology, University of Verona , Verona, Italy
Thyroid and Development Thursday Poster Basic
thyroid follicles develop from aggregates of unpolarized precursor cells. Pax8 belongs to a family of developmental control genes that encode transcription factors. It is expressed at the most immature stage of the thyroid anlage and plays a fundamental role in thyroid cell differentiation, maintenance of the differentiated state and cell proliferation. Tight junctions (TJs) are dynamic structure, that at different stages of epithelial tissue development play an essential role in maintaining integrity and physiological function of thyroid follicles. Claudins (CLDNs) are the major components of TJs. Tissues are characterized by distinctive CLDNs patterns changing during differentiation and tumor formation. CLDNs expression during thyroid ontogenesis is unknown. The aim of this study was to examine CDLNs-1,3,4,5,7 and Pax8 immunohistochemical staining pattern in human foetal thyroid glands.
18 thyroid glands were obtained from human foetuses (gestational age range: 15–22 weeks). Immunostaining was performed using a panel of polyclonal (CLDNs-1 and 3) and monoclonal (Pax8 and CLDNs-4,5,7) antibodies.
CLDN7 was constantly expressed showing strong, diffuse and linear basolateral positivity. CLDN4 and 5 staining was similar to CLDN7 but weaker. CLDN1 exhibited a weak, focal membranous staining at the gland periphery. CLDN3 immunoreactivity was negative. Pax8 was diffusely observed in a nuclear pattern in all samples.
CLDN7 and 4 are constitutively expressed in thyroid epithelium during ontogenesis at a similar level from foetal up to adult thyroid tissue, thus suggesting an essential role in architectural stability of follicular cells. CLDN1 was expressed at the border of the foetal gland where the first follicles, containing colloid, are localized. Conversely, CLDN1 was absent in adult normal tissue while up-regulated in thyroid cancer, thus emerging as an oncofetal antigen and a potential marker of thyroid cancer. Our study demonstrates CLDN5 expression in thyroid gland, suggesting its possible role in normal and neoplastic adult thyroid tissue. We also confirm that Pax8 is expressed at an early stage of thyroid cell differentiation playing a key role in embryogenesis.
Neuroscience and Mental Health Program, Research Institute, The Hospital for Sick Children , Toronto, Canada
Thyroid and Development Thursday Poster Clinical
Adequate thyroid hormone (TH) is needed in gestation and postnatally for normal hippocampal development. Animal research shows type or location of hippocampal abnormality is linked to timing of TH insufficiency. Children of women with hypothyroidism (HYPO) or hyperthyroidism (HYPER) in pregnancy or having congenital hypothyroidism (CH) present distinct human models of timing of TH insufficiency: HYPO has earliest TH loss since these children experienced TH insufficiency in early gestation before onset of fetal thyroid function; HYPER has later pregnancy TH insufficiency because although exposed to normal maternal TH levels, thyroid functioning was blocked in late gestation by maternal anti-thyroid medication; CH, still later TH deficiency in late gestation and postnatally until replacement TH took effect. We queried whether these groups differ in hippocampal structure (size, shape), chemical constitution, integrity, and function. This study describes our findings on hippocampal volumes.
Participants are 45 children (15 per group) and 15 controls (C) who have been followed longitudinally since birth. At 10–12 years, they receive extensive memory testing and structural and functional magnetic resonance imaging. Hippocampal volumes are determined with Analyze 7.0 by tracing according to set landmarks <80 right and left hippocampi per child.
Preliminary findings for 43 cases (9 HYPO, 5 HYPER, 14 CH, and 15 C) indicate smaller volumes in HYPER and CH (3068 and 3070 mm3) than HYPO and Control (3463, 3266 mm3). However, one HYPO whose mother had severe hypothyroidism in second and third trimesters (TSH > 25) had a very small hippocampus (2547 mm3).
TH insufficiency during late gestation and early infancy is associated with reduced hippocampal size in late childhood. The implications of these findings on memory functioning and in terms of hippocampal subcomponents specifically affected will also be evaluated.
Endocrinology & Metabolism, USC/Keck School of Medicine , Los Angeles, CA
Thyroid and Development Thursday Poster Clinical
CH is screened for at birth and has largely been eradicated in the developed world. However, CH remains a major health risk in developing countries. If CH is unrecognized and untreated, devastating neurological and developmental consequences result. A unique case of untreated CH and myxedema coma is presented.
A 36 year-old female with untreated CH, who emigrated from Mexico 5 years ago, presented in myxedema coma secondary to a URI. The patient was 81 cm in height and weighed 16.5 kg corresponding to the 5th percentile in height and the 95th percentile in weight for a 3-year old child. Baseline functional development corresponded to that of a 10-month old child. Physical exam on presentation revealed a BP of 123/72, HR ranging between 60–70 BPM (normal SBP and HR for a 3 year-old child are 86–111 mmHg and 110–115 BPM, respectively), and T of 97.80F. Initial TFT's included a TSH of 208, a FT4 <0.4 and a FT3 <1.1. Work-up of CH consisted of a thyroid U/S, which showed no thyroid tissue, and a TG of 4.2.
Besides receiving supportive care, the patient was loaded with 150 mcg of LT4 IV followed by maintenance dose of 25 mcg LT4 daily. Over the ensuing 72 hours after LT4, SBP decreased from the 120's to the 100's, HR increased to the 90's to 100's (consistent with those expected of a three year old) and T increased to 98–990 F. At her 6 month follow-up visit the patient has grown 13 cm and lost 2.7 kg. She is now more active and able to walk, has grown hair after initial hair loss, and eruption of secondary teeth has occurred. Her most recent TFT's include a TSH of 56.53 and a FT4 of 1.08
1. CH was due to agenesis of the thyroid, 2. Untreated CH produces severe neurological and physical impairment, 3. This is a unique presentation of a largely extinct disease and the oldest patient on record with untreated CH. It gives us the exceptional opportunity to study and observe changes in response to L-T4 therapy and perhaps better understand the role of thyroid hormone in development.
Glucagon-Like Peptide-1 Receptor Agonists Activate Rodent, but Not Human, Thyroid C-Cells Causing Calcitonin Release and Proliferation
Thyroid Cancer Thursday Poster Basic
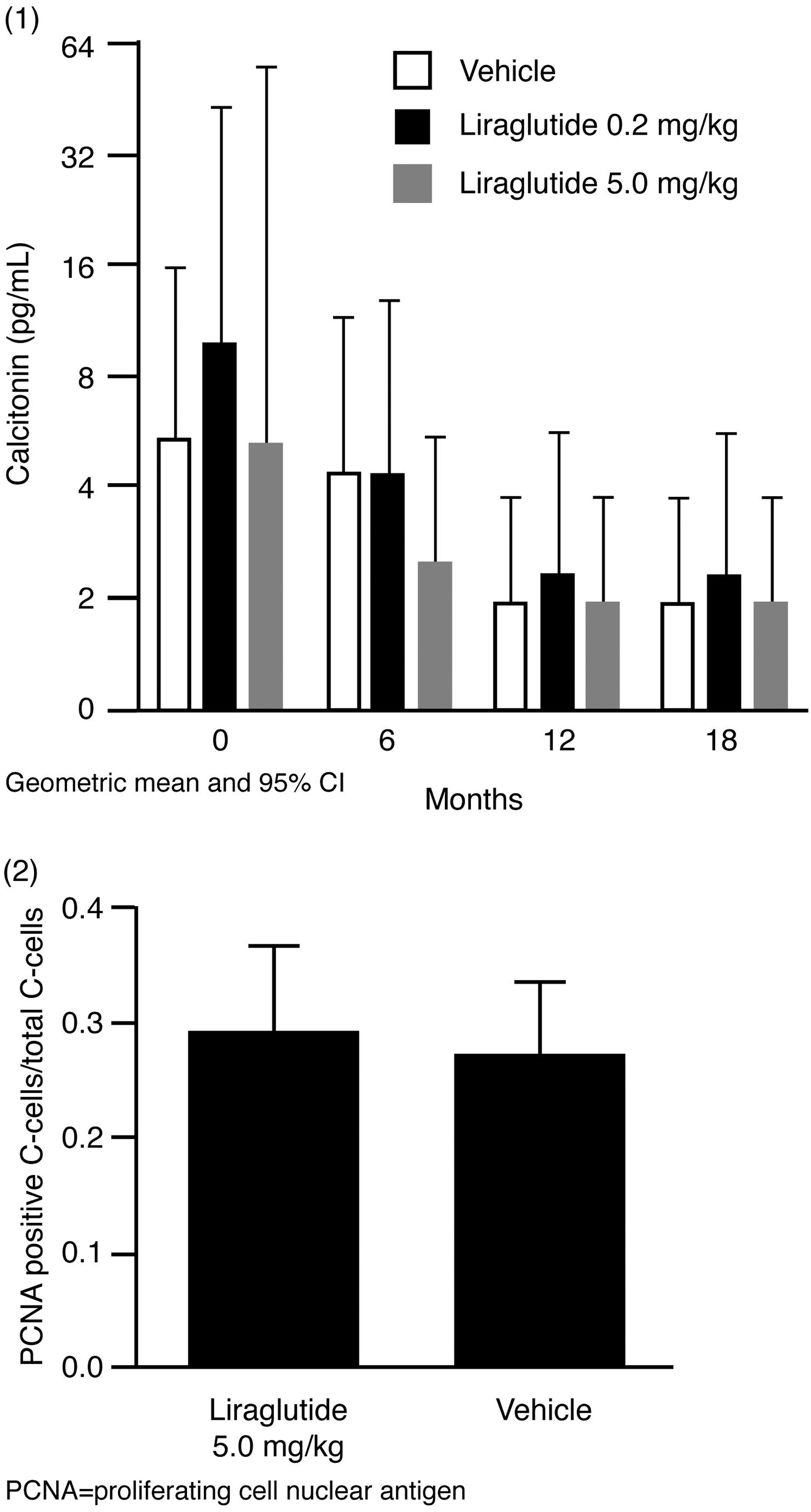
Liraglutide is an analog of human glucagon-like peptide-1 (GLP-1) developed for the treatment of type 2 diabetes. Long-term (2-year) exposure in rodents was associated with an increased frequency of thyroid C-cell tumors, which raised the question of GLP-1's effects on the C-cell and whether this might be clinically significant in humans.
A comprehensive series of in vitro and in vivo experiments were conducted to determine the effects of three GLP-1 receptor agonists (GLP-1, liraglutide and exenatide), explore the role of the GLP-1 receptor in C-cell proliferation in rodents, and determine potential clinical significance.
GLP-1 receptor agonists potently activated rodent C-cell lines in vitro, causing cAMP generation and calcitonin release. In vivo, GLP-1 receptor agonists caused calcitonin release in rodents, except for GLP-1 receptor knockout mice. Furthermore, long-term continuous receptor activation in rodents was followed by calcitonin mRNA upregulation, C-cell proliferation and, in some animals, tumor formation. Any human relevance of these findings was explored using human thyroid tissues, a human C-cell (TT) line, a non-human primate model, and clinical studies in patients with type 2 diabetes. The human C-cell (TT) line and human C-cells had far fewer GLP-1 receptors than rodent C-cell lines and C-cells, and GLP-1 receptor agonists did not cause cAMP or calcitonin secretion in the human C-cell line. Liraglutide did not stimulate calcitonin release in cynomolgus monkeys (up to 87 weeks' exposure; Fig. 1) or humans (up to 2 years' exposure), nor was there any evidence of C-cell hyperplasia in cynomolgus monkeys in these studies (Fig. 2).
Taken together, these data strongly support a role for the GLP-1 receptor in modulating acute calcitonin secretion from rodent C-cells and, over time, promoting C-cell hyperplasia and neoplasia. Data from non-human primates and humans indicate that the effects of GLP-1 on the C-cell are specific to rodents and cannot be demonstrated in primates, including humans.
Medicine, Endocrine Division and Otolaryngology, Head & Neck Surgery, Mount Sinai Hospital and University of Toronto Medical School , Toronto, Canada
Thyroid Cancer Thursday Poster Basic
Identification of molecular signatures of aggressive cancers will facilitate the discovery of specific biomarkers for predicting their anticipated clinical course and the development of non-invasive blood-based biomarkers. Herein, we have explored the conditioned serum-free media of several thyroid carcinoma cell lines which may be enriched by secreted/shed proteins or the adjacent disease-relevant cells of human thyroid thyroid carcinomas. Studies on such surrogate proteins secreted by these cells could identify biomarkers which could be further evaluated in biological fluids.
Conditioned serum-free media was obtained for three thyroid cancer cell lines (WRO, MRO and TPC-1) for secretome analysis. Using liquid chromatography-tandem mass spectrometry, the secreted proteins for the two aggressive thyroid cancer cell lines (WRO and MRO) were compared with those secreted by the non-aggressive cell line (TPC-1).
From these analyses, we observed that there were 77 non-redundant proteins identified. Among these 77 proteins, there were 7 that were identified in all the cell lines, while 9 were unique for the aggressive carcinoma cell lines and 35 proteins were detected only in the non-aggressive cell line TPC-1. Integration of these proteins into a cellular context using Ingenuity Pathway Analysis software revealed that secretome proteins are interconnected with several intracellular canonical pathways known to be associated with cancer development. The detected pathways included: glycolysis, gluconeogenesis, ERK/MAPK, PI3K/Akt, Oncostatin M and IL6 signaling pathways.
Using liquid chromatography-tandem mass spectrometry for secretome analyses has demonstrated in cultured human carcinoma cell lines: (1) the feasibility of detecting protein biomarkers which can distinguish between aggressive and non-aggressive thyroid carcinomas, (2) unravel novel pathways and cross-talks that can lead to rational biomarker discovery through linkage with cancer relevant pathways, and (3) facilitate the development of a selective non-invasive blood-based platform of biomarkers for predicting the clinical course and responses to treatment in thyroid carcinomas.
Surgery, Boston University , Boston, MA
Thyroid Cancer Thursday Poster Basic
MicroRNAs (miRNAs) are small noncoding RNAs that may act to modulate gene expression at the posttranscriptional level and act as factors contributing to cancer progression. mir222 has been shown to affect the proliferation potential of prostate carcinoma cell lines and regulate p27kip1 in human thyroid papillary carcinomas; NPA, a human papillary thyroid carcinoma cell line, has been shown to overexpress mir222. The aim of this study was to evaluate mir222 inhibition on NPA cells and its' implication for the proliferation and invasive potential.
NPA cells were transfected with antimiR 222 using the AMAXA nucleofector; cell growth was assessed using the MTT assay and invasiveness was investigated using a Boyden chamber assay. Comparison was made to an antimiR scramble control. Gene expression was evaluated by qRTPCR using primers for mir222 and mir221 normalized to rnu44 and E-cadherin normalized to GAPDH.
NPA cells transfected with antimir222 showed a 13-fold reduction in mir222 expression and a 10-fold reduction in mir221 expression, while mRNA levels for E-cadherin rose 5-fold by 96 hours. There was no reduction in cell proliferation but a 46% and 38% reduction in invasiveness at 72 and 96 hours respectively. Inhibition of mir222 expression in NPA cells caused no alteration in cell proliferation but a marked reduction in cell invasiveness.
Our data might suggesting a oncogenic function of mir222 and a potential therapeutic target for use in patients with papillary thyroid carcinoma.
Endocrinology, VA Greater Los Angeles Healthcare System , Los Angeles, CA
Thyroid Cancer Thursday Poster
Recombinant human TSH (Thyrogen®, Genzyme), 4–12 IU/mg, is approved for use in a 0.9 mg dose/day for 2 consecutive days for diagnosis and treatment of differentiated thyroid cancer. It is recommended that it be injected IM immediately after reconstitution in the distilled water diluent supplied. However, Thyrogen has been used off-label in doses less than the standard 0.9 mg dose for stimulation of radioiodine uptake in the treatment of multinodular goiter. In order to determine whether the biologic activity of Thyrogen can be preserved after dilution, we designed experiments to assess the biologic stability of Thyrogen under different durations and temperatures of storage. Proving the stability of reconstituted Thyrogen would allow practitioners to store aliquots for future use, thus lowering the cost per use.
Thyrogen was diluted in 1% BSA in PBS to a concentration of 0.9 mg/ml and further diluted to 0.1mg/ml. Aliquots of 0.5 ml were stored at room temperature, 4°C, −11°C, and −60°C for various lengths of time. In addition, Thyrogen aliquots were subjected to several more extreme temperature conditions: incubation for 1 hour at 50°C and, in another experiment, 10 cycles of freezing in dry ice alternating with thawing at 37°C. Bioassays were performed in FRTL5 cells that were down-regulated in media lacking TSH for 5 to 7 days. Thyrogen was added to the media at a final concentration of either 5 ng/ml or 20 ng/ml and the cells were then incubated for 48 hr. Potency was assessed by measurement of 125I-iodide uptake in comparison to cells also treated with perchlorate to block iodide uptake.
Samples stored at 4°C and −60°C retained activity after storage periods up to 59 days. Samples subjected to the freeze-thaw cycle retained activity similar to those of samples that were not frozen. Samples heated to 50°C for 1 hour also stimulated iodide uptake more than that of non-stimulated cells. Thyrogen kept at 4°C, −11°C, and −60°C maintained good biologic potency for 59 days of storage.
The biologic activity of Thyrogen is very stable. The data provide reassurance that storage in the cold for at least one month does not result in loss of Thyrogen's biologic activity.
Dept of Endocrinology, University of Pisa , Pisa, Italy
Thyroid Cancer Thursday Poster Clinical
In the last two decades, a marked increase in the prevalence of differentiated thyroid cancer (DTC) has been observed worldwide. The aim of the present study was to evaluate the changing features of DTC referred to our institution between 1969 and 2004.
Epidemiological, clinical, pathological features and prognostic factors were analyzed in 4187 DTC patients, subdivided into two groups: Group1 (n = 1215) and Group2 (n = 2972) diagnosed before and after 1990, respectively. The series was characterized by a considerable homogeneity in treatment and follow-up strategies, a very low percentage of patients lost at follow-up (<6%) and an almost unique long-term follow-up, with more than 500 patients followed for more than 20 years.
Group2 was characterized by an increased proportion of papillary carcinoma, especially of small size (<1 cm) with a concomitant decrease of follicular carcinoma. Male percentage was greater in Group2, while age at diagnosis was unchanged. DTC of Group2 were more frequently associated with multinodular goiter or autoimmune thyroiditis (AT), many were unexpected findings and only a few patients had a history of neck irradiation. Typical features of aggressiveness were much less frequent in Group2. The survival rate of Group2 (98.7%) was significantly greater than in Group1 (91.4%) (P < 0.0001). Gender, age, histotype, tumor size, extrathyroidal macro-invasion, lymph node and/or distant metastases and clinical class were found to be prognostic factors in both groups using univariate analysis. With multivariate analysis, we found that only age (>40 years), advanced stage (Class III/IV) and the time of diagnosis (before 1990) were independently correlated with a lower survival both in Group1 and Group2.
DTC patients diagnosed after 1990 were more likely to have small tumors, less advanced stage and a better prognosis than those diagnosed before 1990. Interestingly, a higher prevalence of DTC associated with AT was observed in Group2. However, despite these sharped differences, an advanced age and/or an advanced stage at diagnosis are still the most poor prognostic factors for survival as well as they were in the past.
Hospital Pathology, Seoul St. Mary's Hospital, The Catholic University of Korea , Seoul, South Korea
Thyroid Cancer Thursday Poster Clinical
Many attempts have been made to predict the occurrence of lymph node metastases from papillary thyroid carcinoma. Despite these efforts, there is at present no reliable means to accurately predict cervical nodal metastasis. We present a new prediction system, based on the histological and immunohistochemical features.
We analyzed the clinicopathological factors in 123 consecutive patients who underwent total thyroidectomy and central neck dissection for papillary carcinoma and also evaluated the cyclin D1 expression and exon 15 BRAF mutation in tumor tissue.
Seventy-one (57.7%) of all patients had lymph node metastasis. Cyclin D1 was constantly expressed at invasive tumor front and revealed well-defined isolated glands of tumor cells in extra-tumoral region and laterally spreading tubular growth along the fibrous septa around the invasive front of the tumor. On univariate analysis, age (p = 0.014), tumor size (p = 0.011), isolated gland (p < 0.001), tubular growth (p < 0.001), and tumor multiplicity (p = 0.027) predicted lymph node metastasis, whereas patient gender, extrathyroidal extension, and BRAF mutation did not. On multivariate analysis, age (p = 0.035), isolated gland (p < 0.001) and tubular growth (p < 0.001) proved to be strong independent predictors of lymph node metastasis.
The cyclin D1 staining of papillary thyroid carcinoma is very useful for identifying the intrathyroidal spreading of the tumor. Tumor growth patterns verified by cyclin D1 staining can be used in identifying papillary thyroid carcinomas with metastatic potential.
Surgery, St. Joseph Mercy Hospital , Ann Arbor, MI
Thyroid Cancer Thursday Poster Clinical
Routine CLND in PTC treatment is controversial, because of possible increased operative morbidity and uncertain clinical impact.
Retrospective cohort study comparing total thyroidectomy (TT) to TT plus CLND. Inclusion criteria: initial thyroid operations for clinically node-negative PTC ≥1 cm. Endpoints: complications, staging, and post-treatment thyroglobulin (TG) levels.
From 5/02–12/07, of 270 patients operated for thyroid cancer, 103 patients met inclusion criteria. Surgeon and patient preference dictated that 52 underwent TT and 51 TT+CLND. Tumor size and MACIS (metastases/age/completeness-of-resection/invasion/size) scores were equivalent. Temporary hypocalcemia was more frequent with CLND (40.4% vs. 19.2%; p = 0.02). Three TT+CLND patients with normal PTH levels continue calcium/vitamin-D supplements >6 months after surgery (5.8%) versus none after TT (p = 0.11). Permanent nerve injury rates were equivalent (TT:1/52 vs. TT+CLND:0/51). 59% of TT+CLND patients had positive nodes (30/51). Node involvement was equivalent between those with suspicious nodes (58%) and non-suspicious nodes (59%). Node pathology results upstaged 11/22 TT+CLND patients over 45 y (TT: 3/22 stage III vs. TT+CLND: 12/22 stage III; p < 0.01). Mean serum TG levels were equivalent after radioiodine ablation (TT: 4.7 ng/mL vs. TT+CLND: 2.0 ng/mL; p = 0.51) as was the fraction of patients with undetectable TG levels (77% vs. 73%). Recurrences affected two TT (one central neck) and one TT+CLND patient.
Routine CLND during TT does not change the permanent complication rate for primary thyroid cancer surgery. Intraoperative clinical node assessment was inaccurate. Routine dissection upstaged 50% of patients over 45 y. To date, disease outcome is similar and excellent.
Department of Internal Medicine, University of Pisa , Pisa, Italy
Thyroid Cancer Thursday Poster Clinical
Dedifferentiated papillary thyroid carcinoma (DPTC) is characterized by aggressive growth, metastatic spread and loss of iodide uptake ability, making the tumor resistant to radioiodine. Agonists (TZD) of peroxisome proliferator-activated receptor-gamma (PPARg) induce apoptosis and exert antiproliferative effects on continuous thyroid carcinoma cell lines. Until now, no study has evaluated the possible antiproliferative effect of TZD in “primary cultured human DPTC cells” (DPTC-cells), that could be very useful to identify patients responsive to therapy, and no comparison has been reported with the antiproliferative effect of antiblastics, or about a possible additive antiproliferative effect.
The proliferation of DPTC-cells was evaluated by: 1) cell counting; 2) a proliferation assay (WST-1). DPTC-cells were incubated with increasing concentrations of two different PPARg agonists (rosiglitazone, pioglitazone), or four different antiblastics (bleomycin, cisplatin, gemcitabine and etoposide), or the combination of PPARg and antiblastics.
The results of WST-1 assay in DPTC-cells, mean of 7 different experiments, showed a reduction of proliferation by TZD with respect to the control both with rosiglitazone (20 and 30 mcM; respectively, −23% and −29%; p < 0.001) or with pioglitazone (20 and 30 mcM; respectively, −22 and −26%; p < 0.001). Bleomycin, cisplatin, etoposide and gemcitabine significantly (>40%) inhibited DPTC-cells proliferations. An additive antiproliferative effect (p < 0.05) was observed with rosiglitazone 30 mcM in combination with etoposide, and with pioglitazone 30 mcM in combination with bleomycin. Cell counting confirmed the above mentioned results.
TZD exert an antiproliferative effect in DPTC-cells in vitro; an antiproliferative effect of antiblastics was observed, too; TZD in combination with antiblastics have additive antiproliferative effect in human DPTC-cells.
Surgery, Buddhist Tzu Chi General Hospital , Taipei Branch, Taipei, Taiwan
Thyroid Cancer Thursday Poster Clinical
Vascular endothelial growth factor D (VEGF-D), being one of the most potent directly acting lymphangiogenic factors, induces lymphatic endothelial proliferation and facilitates nodal metastases. Although tissues VEGF-D have been shown to contribute to tumor metastases in PTC, the clinical relevance of serum VEGF-D remains unknown. The aim of this multicenter study is to evaluate the clinical relevance of serum vascular endothelial growth factor D (VEGF-D) in papillary thyroid carcinoma (PTC)
This prospective study consisted of 77 primary PTC and 15 benign thyroid nodules patients, treated during the years 2008–2009. Preoperative serum samples were collected and serum levels of VEGF-D were compared with the clinicopathologic features and lymph node metastases.
There is no difference of serum VEGF-D levels between PTC and benign thyroid nodules group (223.17 vs 238.84 pg/ml respectively, P = 0.286). In PTC group, serum VEGF-D levels was significantly increased in patients with lymph node metastases (246.65 vs 212.62 pg/ml respectively, P = 0.008). Age, gender, and tumor size had no impact on the serum VEGF-D expression.
Serum VEGR-D concentration correlated significantly with cervical lymph node metastases in PTC patients. Further study is necessary to evaluate the clinical application.
Detection of RET/PTC Rearrangements in Papillary Thyroid Carcinoma
Thyroid Cancer Thursday Poster Clinical
Genetic testing of thyroid nodules offers a new tool to diagnose thyroid cancer in cases where cytology does not provide a conclusive diagnosis. The chromosomal rearrangements of the RET protooncogene and PTC gene result in the formation of a fusion gene, which is detected in 11–43% of sporadic papillary thyroid carcinoma (PCT) but not in other thyroid malignancies. Many research assays are available, but most are not sufficiently validated for clinical purposes. Our goal was to develop and validate a clinically robust method for the detection of the most common RET/PTC rearrangements in histological thyroid specimens
Total RNA is extracted from paraffin-embedded tissue and the rearrangement transcript detected by RT-PCR. The PCR primers are designed to amplify three common RET/PTC rearrangements (RET/PTC1, RET/PTC2 and RET/PTC3), as well as one housekeeping gene. The forward primers are labeled with a unique fluorescent dye. Amplified fragments are analyzed using capillary electrophoresis in an ABI3130 genetic analyzer. The specific fusion transcript is determined based on the fragment size and color.
A total of 59 thyroid tissue specimens including 27 PTC's, 24 follicular adenomas (FA) and 8 follicular thyroid carcinomas (FTC) were used to validate this assay. RT-PCR results showed the RET/PTC rearrangement in 3/27 (11%) of PTC, in 0/24 (0.0%) of FA and in 0/8 (0.0%) of FTC. Accuracy was assessed by testing 20 (5 positive and 15 negative) thyroid tissue samples by RT-PCR and sequencing versus RT-PCR and fragment analysis to detect the RET/PTC rearrangements. The concordance between the assays was 100%.We were able to detect rearrangement in 50 ng and 500 pg positive RNA in a background of 500 ng of negative RNA, showing the limit of detection of 1 positive cell in 100–1000 normal cells.
We have developed an RT-PCR based method for detection of RET/PTC rearrangements in thyroid tissue specimens, which proved to be fast, specific, accurate, reproducible and amenable to established workflows in a clinical genetic laboratory. Its detection sensitivity is sufficient to allow it to be applied to many additional sample types, such as fine needle aspirate biopsy specimens, or various body fluids (e.g. blood).
Endocrinology, Hospital Churruca Visca , Buenos Aires, Argentina
Thyroid Cancer Thursday Poster Clinical
We have previously reported the TSH levels in patients with end-stage renal disease and thyroid cancer after different doses of rhTSH (Pitoia et al. Endocr Pract 2008:961–6) We are now completing this previous report with a new rhTSH dosage.
We administered five rhTSH different schemes of dosage in four hemodialysed patients with renal failure. Three received rhTSH to administer a radioiodine dose (100 mCi, 60 mCi and 70 mCi 131I). Two patient received rhTSH for the assessment of the disease status.
The first patient, who received two rhTSH 0.9 mg injections, administered in day 1 and 3, presented persistent elevated serum TSH levels during 17 days. The peak serum TSH measured at day 5 after the first injection was 644 mUI/L. Only a self-limited diarrhea was observed. Patients 2,3 and 4 who received 0.45 mg of rhTSH in two consecutive days also had a persistent elevated serum TSH level during 15 days. The serum TSH surge reached a peak level around 400 to 500 mUI/L at day 3 after the first rhTSH injection. The fourth patient was again evaluated with the administration of two 0.225 mg rhTSH injections. Peak TSH levels at day three was 178 mUI/L, similar to that obtained in subjects with normal function. No adverse events were observed in these patients.
Two rhTSH doses of 0.225 mg might probably be the optimal dosage in hemodialized patients with end-stage renal disease.
Surgery, Tulane University School of Medicine , New Orleans, LA
Thyroid Cancer Thursday Poster Clinical
Harmonic technology (Ethicon endosurgery) using the CS 14 endoshears for the control of thyroid vessels during thyroidectomy was proved to be safe, and to shorten the operative time. However, to our knowledge, no previous study has evaluated the effect of the new Harmonic-Focus hemostat dissection technique without supplementary ligation at the ligament of berry in a homogenous group of patients with papillary thyroid cancer undergoing total thyroidectomy +/− central lymph node dissection to evaluate the resulting radioiodine uptake (I-123) postoperatively.
This is a nonrandomized, prospective analysis of a series of papillary thyroid cancer patients undergoing total thyroidectomy +/− central lymph node dissection at a teaching institution. Twenty nine consecutive patients underwent total thyroidectomy +/− central lymph node dissection by the senior surgeon. Demographics, pathological characteristics, thyroid size, operative time, intra operative and postoperative complications and (I-123) uptake following surgery were collected.
Twelve patients out of twenty nine patients underwent surgery with the Harmonic Focus Dissector “no tie” technique. The 2 groups were similar regarding age, sex, thyroid size and primary tumor size. Mean ± SD operative time (minutes) was shorter in the harmonic focus group compared with the conventional technique group (210 ± 49 vs. 246 ± 97, p = 0.20). There was no difference between the 2 techniques regarding the intraoperative or postoperative complication rate. I-123 percentage uptakes following surgery were similar between the Harmonic Focus Dissector Group and the conventional technique group. (0.22 ± 0.25, versus 0.43 ± 0.48, p = 0.15).
The use of the Harmonic Focus dissector without supplementary ligation is safe, and significantly reduced the operative time compared to the use of the conventional hemostatic techniques in patients with papillary thyroid cancer undergoing total thyroidectomy+/−central lymph node dissection. Moreover, postoperative percent radioactive iodine uptake is similar to that seen with conventional hemostatic techniques.
Indications for and Complications Associated with Re-Operative Thyroid Surgery
Thyroid Cancer Thursday Poster Clinical
Re-operative thyroid surgery remains challenging and has a higher morbidity when compared to initial thyroidectomy. It is essential to know the indications for re-operative surgery and to recognize associated complications, so that they can be avoided.
A retrospective review of 1041 patients undergoing thyroid surgery at a single institution between 1996 and 2008 was performed. Data on patients who underwent re-operative thyroid surgery was collected with regards to indications, pathology and complications. Completion thyroidectomies included operations involving the ipsilateral side performed after previous subtotal thyroidectomy, or for recurrence of cancer or goiter. Secondary lobectomies were noted as operations performed to remove the contralateral lobe.
Ninety one patients (8.7%) underwent re-operative thyroid surgery. Re-operative procedures included completion thyroidectomies in 33 (36%), secondary lobectomies in 45 (49%) patients, neck exploration in 1, central lymph node resections in 1, and lateral neck dissections in 2 patients. Four patients underwent 2 re-operations and 2 patients had 5 re-operations. Five of the 6 patients having greater than 1 reoperation had thyroid cancer. Review of pathologies requiring re-operations showed papillary cancer in 41, multi-nodular goiter in 34, follicular cancer in 6, follicular adenoma in 6, medullary cancer in 2, anaplastic cancer in 1 and Graves' disease in 1. Complications included temporary hypocalcemia in 5, permanent hypocalcemia in 3, temporary recurrent laryngeal nerve (RLN) paresis in 2, RLN paralysis in 2, hematoma in 2 and thoracic duct injury in one case. Complications were more common after completion thyroidectomies (12) as compared to lobectomies (3).
Most common pathology requiring re-operative thyroid surgery is papillary thyroid cancer (45%), followed by multi-nodular goiter (37%). Completion thyroidectomy has a significantly higher morbidity than secondary lobectomy (p < 0.01). Most common complications are hypocalcemia, followed by recurrent laryngeal nerve injury.
Surgery, Tulane University , New Orleans, LA
Thyroid Cancer Thursday Poster Clinical
Black thyroid is a rare pigmented change seen mainly in patients on minocycline ingestion. Black thyroid is previously thought to be a benign disease. There are 61 reported cases of black thyroid and 13 cases in association with thyroid carcinoma. To date, no study has reported the incidence of black thyroid and the incidence of associated thyroid cancer. The aim of the current study is to analyze retrospectively the incidence of black thyroid pigmentation in thyroid surgery specimens and examine the relation to thyroid carcinoma.
This is a retrospective study of 560 Consecutive patients, all of who underwent thyroid resection surgery at our institution. Data on patients' demographics, preoperative fine needle aspiration (FNA), clinical and pathology reports were collected. Patients with black thyroids and thyroid cancers were identified.
Forty-one patients (7.3%) had evidence of black thyroid pigmentation in their surgical specimens. The mean age (±SD) was 52 (±25) years. All patients were clinically and biochemically euthyroid. Black pigmentation was never diagnosed in preoperative FNA, and only one patient had a preoperative diagnosis of papillary thyroid carcinoma. Other patients underwent surgery for various reasons. Twenty-four patients (58.5%) had incidental thyroid carcinoma associated with black pigmentation of the thyroid. Thirteen of these patients (54.2%) had papillary carcinomas, and multifocal disease represented 61.5% of cases.
FNA does not diagnose black thyroid. Black thyroid pigmentation is not always a benign disease. Black thyroid is associated with different types of thyroid cancers, mainly papillary thyroid carcinomas. There is increase incidence of multifocal disease with black thyroid pigmentation. Thyroid glands with black pigmentation deserve through pathologic examination, which should include increase in the number of blocks sampled from each specimen to rule out multifocal disease. Further studies are necessary to confirm these data.
Cigarette Use as a Negative Risk Factor for Thyroid Cancer: Does Association Hold True
Thyroid Cancer Thursday Poster Clinical
In the past few years, there has been a rise in Thyroid Cancer incidence. In light of our current emphasis on preventive health, coupled with our limited understanding of the modifiable factors that increase an individual's risk of Thyroid Cancer, more extensive risk factor analysis is indicated. Present study was done to determine if cigarette smoking continues to be a risk factor in the development of thyroid neoplasia.
This is a secondary data analysis of the National Health and Nutrition Examination Surveys (NHANES) from 2003–2006, encompassing data from 20,470 subjects. For the purposes of data analysis, study participants were categorized into two groups, those who never smoked cigarettes and those who had ever smoked cigarette. Presence of Thyroid Cancer was determined based on subjects' self-reports regarding their health history. Statistical analysis was performed using SAS version 9.1, and applying a proc-survey methodology.
After filtering out ineligible NHANES subjects, and analyzing survey data only for those individuals 20 years of age or older, our initial survey sample included 8528 participants. Of this group, sixteen individuals identified themselves as having had Thyroid Cancer, 4514 indicated that they had never smoked cigarettes, and 4014 reported current or past cigarette use. Using a logistic regression model, adjusted for gender, race, education, marital status, body-mass index, and alcohol ingestion; tobacco use was associated with an odds ratio of 2.719 (95% CI of 0.77–9.62).
Our analysis supports the fact that smoking has no relationship to the development of Thyroid Cancer. This finding is contradictory to that found in many other studies, which have shown that cigarette use is inversely related to risk of developing Thyroid Cancer. The literature on the association between cigarette smoking and Thyroid Cancer remains controversial. Drawing an exact association between cigarette use and Thyroid neoplasia is made difficult due to the relatively low prevalence of this disease. Thus, more detailed analysis, such as through a retrospective, world-wide cancer registry or through a prospective cancer study is warranted.
Limited Response to Redifferentiation Therapy with a Combination of Valproic Acid and Rosiglitazone in Patients with Thyroid Cancer
Thyroid Cancer Thursday Poster Clinical
Treatment of dedifferentiated thyroid cancer has a few alternatives at this moment. External beam radiotherapy, chemoembolization, chemotherapy and the new kinase inhibitors have been of limited utility in this setting. Rosiglitazone is a peroxisome proliferator-activated receptor gamma agonist that has been shown to induce differentiation, cell cycle arrest, and apoptosis in a variety of human cancers including thyroid cancer. On the other side, valproic acid was shown to inhibit histone deacetylace and also induce apoptosis in thyroid cancer cells.
Three patients with differentiated thyroid cancer (2 papillary and one folliculary of insular variant, all with distant metastasis in lungs) were enrolled in an open-label trial of oral valproic acid (200 mg increased to 1000 mg 16 weeks before a radioiodine dose) and rosiglitazone treatment (8 mg daily for 8 weeks, started 8 weeks after valproic acid and kept until the radioiodine dose).
Only one patient had an increase in the uptake in lungs, in the post dose radioiodine scan after drug combination therapy. Thyroglobulin level increased while redifferentiation therapy was performed. After treatment, Tg level decreased in this patients, and increased in the remaining two. No patient developed clinically important toxicity.
Our findings suggest that this treatment may induce radioiodine uptake in some but not all patients with dedifferentiated thyroid tumors.
Case Study: Rare Presentation of Metastatic Papillary Microcarcinoma of Thyroid: Small but Dangerous!!
Thyroid Cancer Thursday Poster Clinical
Background: Papillary Thyroid Microcarcinoma (PTMC), previously called occult papillary carcinoma, is a variant of Papillary thyroid carcinoma with a diameter measuring less than 1 cm in size. It is a novel clinicopathological entity, with high incidence and good prognosis. Here, we report a rare case of metastatic unifocal PTMC of 2.5 mm size in one lobe of the thyroid.
Case Description: A 51 year old Caucasian male with sixty pack year history of smoking and chronic cough presented with worsening cough and shortness of breath over a three month period. Review of systems was significant for difficulty swallowing, and easy fatiguability. There was no history of head and neck radiation in the past. Family history was not significant for thyroid cancers. On physical examination, no discrete thyroid nodules or adenopathy were palpable. Chest X-ray done to evaluate his chronic cough revealed mediastinal widening. A Follow-up CT scan of the chest confirmed mediastinal adenopathy. He then underwent mediastinoscopy, which showed metastatic Papillary thyroid cancer. His Thyroid Stimulating Hormone, Free T4, and Calcitonin were normal. Ultrasonography of the thyroid revealed no focal lesion. PET scan of neck and chest reported a hypermetabolic focus just below the main thyroid bed, in addition to the hypermetabolic lymph nodes in central mediastinal compartment and perihilar region. Total thyroidectomy and central compartment dissection were done. Pathology revealed Papillary carcinoma of 2.5 mm size confined to the left lobe of thyroid gland. Central compartment lymph node was positive for metastatic thyroid cancer in 1 of 17 lymph nodes. The pathological stage was pT1,N1,Mx. Patient received adjuvant radioiodine therapy six weeks after the thyroid surgery.
Significance: Tumor size has traditionally been viewed as an important prognostic factor in Papillary thyroid carcinoma. PTMC is usually clinically occult and has an indolent course. It is therefore frequently considered to be of no clinical importance. However, this case contests the generally seen trend and warrants extensive studies of the prognostic factors, and surveillance guidelines for Papillary thyroid carcinoma.
NIDDK/Clinical Endocrinology Branch, National Institutes of Health , Bethesda, MD
Thyroid Cancer Thursday Poster Clinical
Primary thyroid lymphoma constitutes <2% of thyroid neoplasia. It is most frequently observed in long-standing Hashimoto's thyroiditis and in the presence of anti-thyroid peroxidase (TPO) antibodies. We report a case of rapidly-progressive primary thyroid lymphoma in the absence of thyroid autoantibodies.
N/A
Case: A 59 year old female with an 8 year history of hypothyroidism presented for evaluation of an incidental thyroid nodule and increased L-T4 requirement. Anti-TPO and anti-thyroglobulin antibodies were negative. Thyroid ultrasound revealed a poorly differentiated 2.3x1.7 cm mixed lesion in the context of an inhomogeneous gland. Fine needle aspiration (FNA) showed lymphocytes with atypia of likely reactive origin and neutrophils in the setting of proteinaceous and necrotic debris. Grocott Methanamine Silver and Fite stains ruled out fungal and acid fast bacilli infections. 8 weeks later, she noticed a diffuse enlargement of the nodule. Ultrasound showed a heterogeneous mass anterior to the trachea, with loss of overall thyroid echotexture. A large superficial lymph node (LN) was noted in the lateral cervical area. FNA of the mass and lymph node were thus performed. Cytology showed large atypical lymphoid cells with enlarged irregular nuclei and scant basophilic cytoplasm with lymphoglandular bodies in the background. Flow cytometry revealed a population of large abnormal B cells expressing CD19, CD20, CD22 and CD45, and negative for surface immunoglobulin; findings consistent with a B-cell lymphoma. Excision biopsy of the superficial LN confirmed the diagnosis of diffuse large B-cell lymphoma. Imaging (CT of the neck, chest, abdomen, and pelvis) confirmed the thyroid as the primary site, excluding extra-cervical disease. The patient was started on Rituximab+CHOP chemotherapy.
Thyroid lymphoma is a rare and aggressive neoplasm of the thyroid. The occurrence of thyroid lymphoma in the absence of TPO antibodies is a particularly uncommon event. Nonetheless a high index of suspicion should be kept for this condition in the presence of a rapidly growing thyroid mass. Aggressive early medical intervention represents the cornerstone in the management of thyroid lymphoma.
Surgery, St. Martin De Porre Hospital , Chia-Yi, Taiwan
Thyroid Cancer Thursday Poster Clinical
Clinical diagnosis of cancer metastatic to the thyroid is extremely rare, and more commonly diagnosed at autopsy. The more common primary sites for metastasis to the thyroid are kidney, breast, lung, colon, esophagus and uterus. Thyroid metastasis from stomach (including carcinoma and sarcoma) were only reported in 3 cases in English literature.
Herein we report a 71 year old man with the presentation of growing neck mass, tarry stool and progressive dyspnea for 2 months. Bilateral thyroid multinodular lesions and four tiny (0.3 to 0.5 cm) lesions were noted on computed tomography. A 3.5 cm ulcerated mass lesion was noted at the body of stomach by fiberoptic esophgogastroscopy.
Bilateral near-total thyroidectomy was performed due to airway compression with related symptoms. Wedge resection on one of these pulmonary nodules was performed through video assisted thoracoscopic surgery (VATS) for diagnosis, and the lesion on the stomach was diagnosed by trans-endoscopic biopsy. Poorly differentiated adenocarcinomas with the same histological profiles were noted on these three sites. The immunohistochemical staining for thyroglobulin of them were also negative. The I-131 imaging of the residual lung nodules and stomach was also negative. Patient underwent subsequent chemotherapy and the condition was stable.
For any patients with other sites of malignancy, appearance of synchronous or metachronous thyroid nodule cannot exclude the possibility of a metastatic lesion. Aggressive surgical and medical therapy might be beneficial for some of these patients.
A Case of Metastatic Struma Ovarii in a Clinically Euthyroid Patient
Thyroid Cancer Thursday Poster Clinical
Metastatic struma ovarii is very rare, seen in only 5–10% of cases of patients with struma ovarii. We describe an unusual case of metastatic struma ovarii in a clinically euthyroid patient.
NA. This is a clinical vignette
Clinical Case: A 55 year old female with a history of ovarian teratoma presented with abdominal discomfort and underwent ultrasound of her abdomen which revealed a dermoid cyst in the right ovary. She underwent resection of the right ovary which was consistent with struma ovarii, a dermoid cyst, and papillary thyroid carcinoma of the right ovary. The left ovary was resected which revealed a small mature teratoma measuring 1.0 cm with focal mature thyroid follicular tissue however no papillary thyroid carcinoma. Thyroid function tests were normal. She subsequently underwent an US of the thyroid revealing a heterogeneous hypoechoic nodule in the right upper pole measuring 1.1 cm and a 2 cm heterogeneous hypoechoic nodule in the left mid lobe. The patient denied a family history of thyroid malignancy or radiation exposure. No signs or symptoms of hypo- or hyperthyroidism. No compressive signs or symptoms. Physical exam was only significant for a dominant left nodule of approximately 2 cm in the left lobe and 1 cm right upper lobe nodule. Thyroid peroxidase and thyroglobulin antibodies were negative. Ultrasound guided fine needle aspiration of the right thyroid nodule was unable to be performed. However ultrasound guided fine needle aspiration of the left thyroid nodule revealed findings consistent with lymphoid tissue. A total thyroidectomy was recommended to the patient as it was unclear if the papillary thyroid carcinoma represented a primary lesion or metastasis and also for ease in following for recurrence of her papillary thyroid cancer and subsequent treatment with radioactive iodine therapy, however the patient declined surgery.
This case demonstrates a rare case of metastatic struma ovarii in a clinically euthyroid patient and lymphoid tissue in the thyroid gland which are both rare findings.
Department of Clinical Biochemistry, Royal Free Hospital , London, United Kingdom
Thyroid Diseases Thursday Poster Clinical
Thyroid dysfunction (TD) is a recognised side effect of Interferon-α (IFNα) therapy in the treatment of hepatitis C (HCV) infection, with incidence reported between 5 and 33% in different studies worldwide. No data exist for a UK cohort. This retrospective study has determined the incidence of TD in a UK cohort of patients with HCV treated with IFNα and Ribavirin combination therapy (CT).
A retrospective analysis of 275 patients treated at the Royal Free Hospital London in a two year period from January 2006. Thyroid function, viral load, HCV genotypes and liver function were assessed during a 6 or 12 month course of CT. Pre-treatment serum TSH measurements were available for 62% of the cohort. Liaison occurred between the Hepatology Specialist Nurse team and the Department of Endocrinology regarding those patients who developed TD. All those with an undetectable serum TSH had a diagnostic thyroid isotope scan.
20% (n = 56; 15% of men, 32% of women) developed TD within 1–11 months of commencing CT. The mean time of presentation of TD was (mean ± standard deviation) 3.8 ± 2.7 months. In the total cohort 9% (n = 24) developed an initially suppressed serum TSH (1% Graves', 8% transient thyroiditis) and 12% (n = 32) developed an initially elevated serum TSH (2% permanent hypothyroidism, 10% transient hypothyroidism). The relative risk of developing TD was 2.14 (95% confidence interval between 1.35 and 3.36; p = 0.002) for women. No statistically significant differences in risk were observed between ethnic groups. HCV genotype status, abnormalities of liver enzymes and success of CT as determined by sustained viral response were not associated with an increased risk of progression to TD. The mean pre-CT serum TSH was 1.65 ± 1.31 mU/L for those remaining euthyroid and 2.89 ± 1.36 mU/L for those developing hypothyroidism (p = 0.0003). ROC curve analysis (see figure) determined a serum TSH of 2 mU/L as the optimal cutoff for the prediction of hypothyroidism (Sensitivity = 79.2%, Specificity = 78.1%, PPV = 37.3%, NPV = 95.8%).
Although there was a relatively high incidence of TD in this UK cohort, only 3% required long-term treatment for TD at the completion of CT. A pre-CT serum TSH ≥2 mU/L predicted the development of hypothyroidism.

Association Between Oxidative Stress and Thyroid Diseases of Pregnant Women
Thyroid Diseases Thursday Poster Clinical
There is supporting evidence to hypothesize that oxidative stress may contribute to thyroid dysfunction. Thyroid diseases during pregnancy have been shown to be associated with various adverse pregnancy outcomes. The aim of our study was to evaluate the presence of oxidative stress in pregnant women with thyroid diseases and autoimmune disorders through determination of oxidative stress peripheral markers.
Oxidative stress peripheral markers, including glutathion peroxidase (GPx), superoxide dismutase (SOD), malonaldehyde (MDA) and hydrogen peroxide (H2O2), were determined in 62 pregnant women with thyroid diseases (including overt hyperthyroidism, overt hypothyroidism, subclinical hyperthyroidism, subclinical hypothyroidism, hypothyroxinemia and euthyroid pregnant women with thyroid antibody positive), as well as in 84 euthyroid pregnant women with thyroid antibody negative as controls. Women with thyroid diseases were matched with healthy controls by age, body mass index and gestational age. We assessed thyroid function of pregnant women by thyroid-stimulating hormone (TSH), total thyroxin (TT4), free thyroxin (FT4), thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TgAb) and used the trimester-specific reference ranges for the assessment of thyroid diseases and autoimmune disorders in pregnancy.
Significantly decreased plasma GPx and SOD activities were measured in pregnant women with thyroid diseases compared with controls [GPx activity 27.77 (18.10) vs. 84.30 (59.01) U/0.1ml, P < 0.0001; SOD activity 45.81 (13.46) vs. 101.05 (23.16) U/ml, P < 0.0001]. Pregnant women with thyroid diseases had significantly higher levels of plasma MDA and H2O2 than controls [MDA level 7.21 (2.2) vs. 3.24 (1.18) nmol/ml, P < 0.0001; H2O2 level 9.84 (1.35) vs. 6.02 (1.05) mmol/L, P < 0.0001].
Our study indicated the presence of oxidative stress in pregnant women with thyroid diseases, which suggested oxidative damage to thyroid tissue might play an important role in thyroid diseases during pregnancy.
Changes of Serum Concentrations of ADMA, NT-PROBNP, Leptin and Adiponectin in Graves Patients
Thyroid Diseases Thursday Poster Clinical
GD patients had a higher risk of cardiovascular diseases (CVD), the endothelial dysfunction and abnormalities of adipocytokines are involved in its pathogenesis. Asymmetric dimethylarginine (ADMA) is a new marker of endothelial function, while NT-proBNP could reflect fluid volume and vascular stiffness. The purpose of this study was to investigate the relationships between the serum levels of ADMA, NT-proBNP, leptin, adiponectin and thyroid hormones in Graves patients.
269 GD (F: 202,M:67) patients and 81 gender, age and BMI matched normal controls were enrolled in this study. Serum concentration of thyroid hormones, ADMA, NT-proBNP, leptin and adiponectin were all measured. OGTT and insulin releasing tests were performed in a subgroup of patients (N = 68).
Serum levels of ADMA were in positive relationships with FT3(r = 0.593, p < 0.001), FT4(r = 0.569, p < 0.001), TRAb(r = 0.475, p < 0.001). It was also correlated with serum NT-proBNP levels (r = 0.2829, p < 0.001), but showed no association with serum concentration of leptin and adiponectin. Serum NT-proBNP levels were significantly in positive association with FT3(r = 0.260, p < 0.001), FT4(r = 0.297, p < 0.001) and heart rate (r = 0.251, p < 0.02) and were independent of age, sex, smoking and BMI. The elevation of serum ADMA and NT-proBNP levels were present even in patients with controlled hyperthyroidism. Multiple regression analysis revealed that the changes of serum ADMA levels in GD patients were independent of age, sex, smoking and BMI, and were not influenced by serum NT-proBNP levels or parameters in glucose and lipid metabolism, such as fasting and 2h postprandial plasma glucose, serum insulin, HOMA-IR and lipid profiles. FT4 was the only parameter affecting the changes of serum ADMA concentration in GD.
Serum FT4 is an important factor determining serum NT-proBNP and especially ADMA concentrations in GD patients. The changes of serum ADMA levels were not influenced by sex, BMI, adipocytokines and parameters in lipid and glucose metabolism. Circulating ADMA levels may be an independent CVD risk factor in GD patients.
Section of Endocrinology, Boston University School of Medicine , Boston, MA
Thyroid Diseases Thursday Poster Clinical
Weight gain is a common complaint in patients being treated for hyperthyroidism.
We conducted a retrospective chart review of 111 patients who underwent radioactive iodine treatment (RAI) for hyperthyroidism during 2002–2005. We collected data on age, sex, race, and etiology of hyperthyroidism. Weights (kg) and TSH values (uIU/L) were obtained at diagnosis, at time of RAI, and at 0–4 months, 4–8 months, 12 months, and 24 months post treatment. Absolute and percent weight increase were calculated. We conducted subgroup analyses by sex, race, and etiology of disease. We also compared TSH values at each time point.
Mean age of our cohort was 49 with 86 females and 25 males. Of these, 38% were black, 48% white, and 14% Hispanic. 72% of the patients had a diagnosis of Graves disease. Mean weight was 74.4+/−16 kg at time of RAI (median TSH 0.03). There was a statistically significant absolute weight increase of 1.57+/−0.3 kg 0–4 months after RAI (median TSH 1.43), 2.72+/−0.4 kg 4–8 months after RAI (median TSH 1.72), 3.19+/−0.5 kg 8–12 mo after RAI (median TSH 2.48), and 3.78+/−0.7 kg two years after RAI (median TSH 1.25). Percent weight increase was statistically significant at each time point (p < 0.01). Subgroup analyses showed a significant difference in absolute and percent weight gain by sex, with males gaining more weight than females. Blacks gained significantly more weight than whites. We did not find a difference in absolute and percent weight gain when comparing Graves vs. other etiologies for hyperthyroidism. We did not find a correlation between degree of TSH elevation and observed weight gained.
Our data support prior studies suggesting weight gain following RAI for hyperthyroidism. In addition, we make the new observation that male patients and blacks are at higher risk for weight gain following RAI. The etiology for the patient's hyperthyroidism does not seem to play a role in weight gain. Likewise, the degree of hypothyroidism immediately post treatment does not seem to affect the eventual weight gain.
The Prevalance of Nodular Thyroid Disease in Autoimmune Thyroid Disease
Thyroid Diseases Thursday Poster Clinical
There are conflicted results about association of autoimmune thyroiditis and differentiated thyroid carcinoma. The aim of study was to evaluate retrospectively the coexistence of nodular thyroid disease (NTD) with autoimmune thyroid disease (ATD).
Five hundred patients were analyzed retrospectively. Thyroid ultrasonography was performed in all patients with fine needle aspiration biopsy for the thyroid nodule when necessary. After second or third ND biopsy patients underwent operation.
Among 500 with ATD (400 women and 100 men; mean age = 42.4 years), 60% (n = 300, 90% women and 10% men) had Hashimoto's thyroiditis (HT), 40% (n = 200, 65% women and 35% men) had Graves' Disease (GD). One hundred forty nine nodules underwent FNAB (37,8% had GD and 19,6% had HT, p < 0.001). Mean thyroid nodule volumes were 0.26+–0.6 vs. 1.5+–5.5 in patients with GD and HT, respectively (p < 0.001). The results of the cytologic examination were non-diagnostic (ND) cytology, benign, malignant and indeterminate in 19.4%, 73.8%, 2% and 4.5% of the nodules respectively. Twenty nine nodules with ND biopsy underwent a repeat FNAB. The second biopsy showed 3,5% nondiagnostic cytology. There was no difference between HT (19.8%) and GD (18.1%) nodules with regard to ND cytology. The incidence of thyroid carcinoma was similar between subjects with GD (n = 3, 1,5%), and HT (n = 2, 0,6%) (p = 0,706). Histologic examination revealed papillary microcarcinoma. Mean diameters of carcinoma was 0,64 ± 0,29 cm (range, 0,10–1,50 cm). When preoperative FNAB cytology was considered, among 5 cases with thyroid carcinoma, 3 were from malignant, and 2 were from insufficient groups.
In this study, we observed that thyroid nodules in patient with GD were higher and larger than patient with HT. There is a need for large scale studies comparing frequency of thyroid nodules in GD and HT individuals. Patients with autoimmune thyroiditis must be evaluated carefully for the presence of coexisting nodular thyroid disease with ultrasonography and even with FNAB as necessary.
Dept. of Medicine and Endocrinology, Aarhus University Hospital , Aarhus, Denmark
Thyroid Diseases Thursday Poster Clinical
Surgical treatment of substernal goiter occasionally involves sternotomy. Classification and handling of these operations are widely discussed. Objective: To review surgical results after thyroid operations including median sternotomy.
A retrospective review of all thyroid operations performed from 01.01.95 to 31.12.08. In 48 of 1573 thyroid operations (3%) median sternotomy was performed. Indications for sternotomy were substernal malignant lymph nodes in 2 cases (4%) and signs of mechanical compression from substernal goiter in 46 (96%).
Pathologic examinations discovered malignant disease in 5 patients (10%) and multinodular goiter in 43 patients (90%). Mean operation time was 4 hours and 8 minutes (n = 43). Mean estimated blood loss was 433 ml (n = 42). Blood transfusion was given in 5 operations (10%). Median duration of postoperative hospitalization were 7 days (range 4 to 27 days). Radical resection was not possible in one patient (male, 73 years) with an anaplastic carcinoma and severe tracheal compression. This patient died postoperatively due to pneumonia and septicemia. Pulmonary complications occurred in 11 patients (23%): pneumonia or atelectasis (6), pneumothorax (3) and pleural effusion (2). Three patients (6%) had postoperative hypocalcaemia (permanent in 2 patients (4%)). Vocal cord paresis was not observed in this series of patients.
Thyroid operations with sternotomy are complicated procedures accompanied with considerable pulmonary complications, but in experienced hands the risk of the specific complications hypoparathyroidism or recurrent laryngeal nerve injury is not increased.
Is Percutaneous Methylpredonisolone Acetate (MA) Injection a New Option for the Treatment of Patients with Prolonged Subacute Thyroiditis?
Thyroid Diseases Thursday Poster Clinical
Predonisolone (PSL) has a special efficacy for subacute thyroiditis (SAT). However, it is sometimes difficult to taper it when SAT is prolonged. Ultrasound (US) is useful not only for the diagnosis but also for the evaluation of the activity of SAT. In order to avoid continuing PSL for long time, the injection of MA to hypoechoic areas of SAT was attempted using US guided technique.
Indication of the injection of MA was as follows: development of recurrence or creeping (n = 4), the presence of multicentric hypoechoic areas with swelling of both lobes, development of side effects of PSL (n = 3), and mild or moderate activity. MA was injected in doses of 0.1∼0.2 ml for several times with a 25 gauge needle. Ten cases of SAT were included in this study. After diagnosis, 8 of the 10 cases were treated with PSL for 2 weeks starting with15 mg or 20 mg per day. After stopping PSL, MA was injected to hypoechoic areas in 7 of the 8 cases and non-steroidal drugs were administered per os at the same time. The remaining one of the 8 cases continued 5 mg PSL along with the additional injections 2 times. In the remaining 2 of the 10 cases, in which SAT was mild, just MA was injected without non-steroidal drugs.
The areas to which MA was injected could be clearly observed with US. Exacerbation of SAT could easily been predicted by US. All cases were followed up for more than 8 months. Local tenderness disappeared within 2 weeks in almost all cases, and the inflaming lobes were greatly reduced in 9 of the 10 cases. Transient hypothyroidism developed in 8 of the 10.
MA injection to inflaming areas may be a new option for the treatment of prolonged SAT to make it possible to stop PSL earlier than before.
Who Will Enter Remission of Graves Disease?
Thyroid Diseases Thursday Poster Clinical
The use of thionamide antithyroid drugs (ATD) for Graves' disease (GD) is effective for control thyrotoxicosis, but the remission rates is not high. Although the remission rate was improved by long-term ATD treatment, we are unclear for how long to give antithyroid drugs. We compared the remitted patients (R) and non-remitted patients (A) to evaluate the treatment duration.
Patients with GD were treated with the Titration regimen of ATD in which dose was tapered as the patient becomes euthyroid and applied long-term low-dose continuous ATD for keeping euthyroid more than 1 year. Remission defined when a patient keeping euthyroid more than 2 years after withdrawal of ATD. 308 patients who has been used MMI more than 2.5 years and could not reduce the dosage to keep euthyroid or remission (A). 199 patients were achieving remission (R).
The duration of treatment was 8.0 years (1–30) for R and 9.2 (2.5–37) for A, respectively. The remission rates were 32% who started ATD in their 30s. That of 10s, 20s, and 60s was about 45%. In 30s, the duration of treatment was 9.4 years in both R and A, initial TRAb was 38% in R and 54% in A. The initial TRAb was 46% in R and 56% in A. In 30s, 40s, 50s and 60s, the initial TRAb in A was higher than R.
One of the reasons for poor remission rate in the 30s is stress-related exacerbation such as childbirth. Although the initial TRAb titers had not predicted therapeutic outcome, the risk of relapse was higher in older onset and higher TRAb. While longer treatment did not achieve remission, keeping euthyroid life long would contribute patient's QOL.
Endocrinology, Georgetown University Hospital/Washington Hospital Center , Washington, DC
Thyroid Diseases Thursday Poster
Graves' disease is a common cause of hyperthyroidism. Uncommon manifestations include thyrotoxic periodic paralysis, thymic hyperplasia and hypercalcemia. We describe a case with all the above manifesting concomitantly, as an initial presentation of Graves' disease.
A 27 year old African-Amercian male patient presented with acute onset bilateral lower extremity weakness, tachycardia, hypertension, thyrotoxic orbitopathy and enlarged thyroid gland. Laboratory findings revealed hypokalemia, hypomagnesemia, hypercalcemia, hyperthyroidism and high thyroid stimulating immunoglobulin levels. Chest CT scan showed a homogeneous thymic mass >6 cm in dimension. Lower extremity weakness resolved after normalization of potassium. It was likely that his Graves' hyperthyroidism had precipitated the paralysis, thymic hyperplasia and hypercalcemia. Hence, he was prescribed methimazole and propranolol. One month later, he was euthyroid and normocalcemic. 15 weeks later, CT scan of the chest showed a significant decrease in the thymic mass to less than 2 cm confirming the initial diagnosis.
Thyrotoxic periodic paralysis (ThPP) is a rare complication of hyperthyroidism characterized by various degrees of muscle weakness and hypokalemia due to a massive intracellular shift of potassium. It has a predilection for young Asian males. Treatment consists of potassium, non-selective beta-blockers and anti-thyroid drugs. Thymic hyperplasia is a benign enlargement of thymic tissue, thought to result from a combination of hyperthyroidism and autoimmunity in Graves' disease, and typically regressing with its treatment. Hypercalcemia in hyperthyroidism is usually due to activation of osteoclastic bone resorption by excess thyroid hormone and is not thought to be PTH mediated.
Thymic hyperplasia Image 1 (Before treatment of Graves' disease).

To our knowledge, this is the first report of Graves' disease complicated by the simultaneous manifestation of ThPP, thymic hyperplasia and hypercalcemia. African-American males have only rarely been described to suffer from ThPP. Clinicians should consider Graves' disease in their differential when they see occurrence of ThPP, thymic hyperplasia or hypercalcemia either in isolation or in combination.
Endocrinology, University of Vermont , Burlington, VT
Thyroid Diseases Thursday Poster Clinical
A 47-year old woman was sent to the Endocrinology clinic by her primary care because of abnormal thyroid functions, thyroid enlargement and weight loss. The patient complained of difficulty swallowing for 4 months and had lost ten pounds. Her TSH was 69, and she was started on 25 mcg/d of L-thyroxine by her primary care. Four weeks later, this was increased to 50 mcg/d. A thyroid scan and uptake was done by her primary care which revealed a low uptake of 0.5%. An ultrasound showed the gland to be diffusely enlarged at 56 × 23 × 29 mm on the right and 51 × 21 × 14 mm on the left. The gland had a heterogenous echotexture with two nodules on the right, both measuring 15 mm. The patient had no previous history for thyroid problems, no family history of thyroid disease and no exposure to radiation.
Blood tests were ordered for thyroid autoantibodies and TSH. The patient underwent a fine-needle aspirate of the right-sided thyroid nodules, and then due to non-diagnostic findings, a core biopsy.
Blood testing revealed partially-corrected hypothyroidism with a TSH of 26 (normal = 0.35–5.5) and a free T4 of 0.9 (normal =0.8–1.8). Thyroid antibodies were very elevated: Anti-thyroglobulin >9000 IU/mL (normal: 0–40 IU/ml) and Thyroperoxidase Ab 2560 IU/mL (normal: <35 IU/ml). The FNA was non-diagnostic, showing only fibrous tissue and blood; no follicular cells seen. The core biopsy showed predominantly fibrotic tissue with entrapped atrophic follicles, lymphocytic infiltrate, and squamous metaplasia. Staining for amyloid was negative.
This patient presented with goiter, hypothyroidism and autoimmune markers consistent with Hashimoto's thyroiditis, but her weight loss and the hard texture of the gland, only apparent during the fine needle aspiration were unusual features. The core biopsy revealed fibrotic tissue and atrophic follicles, which in this clinical setting is consistent with Riedel's thyroiditis. The patient was placed on steroids, and experienced almost immediate clinical improvement in terms of being able to eat.
Parathyroidectomy-Induced Thyroiditis
Thyroid Diseases Thursday Poster Clinical
Subacute granulomatous thyroiditis which is characterized by transient hyperthyroidism has been thought to be due to the destruction of thyroid follicles with subsequent leakage of thyroid hormone stores more commonly as a result of a viral or postviral illness. Parathyroid surgery is a less recognized cause of subacute thyroiditis.
This is a report of two cases with a review of relevant literature.
Two women (84 and 55 years old) without any prior history of thyroid disease developed symptoms of hyperthyroidism 1 week post-parathyroidectomy for primary hyperparathyroidism. The first patient had bilateral cervical exploration with removal of a right inferior parathyroid adenoma while the second patient had a 3½ parathyroidectomy for 4-gland hyperplasia. Both surgeries were uncomplicated. None of them received any iodinated contrast agents or medications such as lithium or amiodarone prior to presentation. Laboratory results showed elevated free thyroxine, suppressed TSH levels, very low radioactive-iodine uptake (first patient), and an elevated thyroglobulin level (second patient). Both were treated symptomatically with beta-adrenergic antagonists. Thyroid function normalized and symptoms improved spontaneously after 1–2 months.
The development of transient hyperthyroidism is common after parathyroidectomy but is under-recognized. Except for the extent of operation, clinical parameters have not been able to predict which patients are at risk for post-parathyroidectomy thyroiditis. Although most patients are asymptomatic and spontaneous recovery is expected, clinically significant thyrotoxicosis can also occur. Thus, patients should be informed regarding this complication and assessment of thyroid function should be performed if clinically indicated.
Analyses of 131-Iodine Therapy Hyperthyroidism Complicating Hepatic Function Lesion in 89 Cases
Thyroid Diseases Thursday Poster Clinical
Observating the turnover of thyroid and hepatic functions of 131-iodine therapy in hyperthyroidism complicating hepatic function lesion.
Patients of hyperthyroidism complicating hepatic function lesion 89 cases, men 16 cases, women 73 cases, age range of 21∼69, average 41.1. All cases are final diagnosis as hyperthyroidism by clinical symptom, physical examination, sero-FT3, FT4, TSH, thyroid iodine uptake and thyroid scanning, as well as hepatic function detection. All patients intake dose of 131-iodine on the basis of formula (omission here), peros once. Patients are requested to intake liver aid continuously one month after peros 131-iodine (Taigan, Creatinine, etc).
Recheck thyroid and hepatic functions after 131-iodine therapy 3 month and 6 month. It demonstrates that 60.67% (54 cases) and 85.39% (76 cases) patients' thyroid function recover normal, meanwhile, 91.01% (81 cases) and 93.26% (83 cases) patients' hepatic function recover normal.
131-iodine therapy is not only effectively in hyperthyroidism, but also in relieving hepatic function lesion. It's a convenient and effective method.
Pharmaceutical Research Institute, Albany College of Pharmacy and Health Sciences , Albany, NY
Thyroid Hormone Action Thursday Poster Basic
Tetrac (tetraiodothyroacetic acid) is a deaminated analogue of L-thyroxine (T4) that inhibits the actions of T4 and 3, 5, 3′-triiodo-L-thyronine at the cell surface receptor for thyroid hormone on integrin αvβ3. The integrin is expressed on cancer cells and on endothelial cells and vascular smooth muscle cells and tetrac blocks the proliferative effects of thyroid hormone on tumor cells and the pro-angiogenic actions of the hormone on tumor-relevant vasculature. In the absence of thyroid hormone, tetrac also blocks angiogenesis induced by vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), and other pro-angiogenesis factors. Tetrac as a nanoparticle (tetrac NP), covalently linked to poly (lactide-co-glycolide), does not gain access to the cell interior and acts exclusively at the integrin receptor. Human pancreatic cancer is an aggressive, progressive tumor that is poorly responsive to current treatment modalities.
In the present studies, the activity of tetrac and tetrac NP against human pancreatic cancer cells (PANC-1) was studied in the nude mouse xenograft model. Subcutaneous implantation of 107 PANC-1 cells in the left and right flanks of each animal was carried out in control animals and tetrac-treated and tetrac NP-treated mice (n = 6 each for group). Tumor volume was 200–250 mm3 by 15 d, at which time treatment was introduced for 15 additional d.
Tetrac or tetrac NP resulted in significant suppression (P < 0.01) of tumor growth and of tumor angiogenesis. Tumor volume in treated mice was reduced by 15 d to less than the implantation volume and decrease in tumor size was apparent and significant at 5 d. Tetrac NP was at least 10-fold more potent than tetrac. Tumor vasculature was estimated by tumor hemoglobin content and was reduced by treatment by 60%. Animal weight gain was comparable in the control and treatment groups.
These observations document the anti-tumor and anti-angiogenic effectiveness of tetrac NP against human pancreatic cancer xenografts.
Primary Hypothyroidism and Breast Cancer: Case Control Study of Clinical and Pathological Risk Reduction Correlates
Thyroid Hormone Action Thursday Poster Clinical
A link between thyroid dysfunction and the natural history of breast cancer [BC] risk is controversial but retrospective studies suggest that primary hypothyroidism [HYP] is associated with a biologically less aggressive disease. Supporting molecular studies show that in model tumor sytems L-Thyroxine (TH) is permissive, stimulates mitogenesis and neo-angiogenesis and inhibits -apoptosis acting via a receptor for thyroxine on cell membrane aνβ-3 integrin. The potential for TH levels to impact on prognosis in cancer is of interest since dosage of supplemental L-thyroxine (L-T) in hypothyroid cancer patients may have consequences for the prognosis of such individuals.
2,044 electronic and paper charts were reviewed in a hospital based retrospective case-control study on 159 female patients with AJCC stage 1–4 invasive BC patients (infiltrating ductal (129), lobular (19) carcinoma- the majority) over 10 year. 68 cases of invasive BC with primary HYP on L-T supplementation (prescribed by an endocrinologist or internist ) were compared to 91 matched controls . Differences in age of diagnosis and clinico-pathological variables were analyzed. TH blood levels and L-T dosage were generally unavailable.
Compared to euthyroid patients those with HYP were diagnosed with breast cancer 4.7 years later (mean age at diagnosis 68.12 vs. 63.44 years, p < 0.035). The primary tumor measured less than 1 cm in 27.4% of HYP vs. 11.4% of euthyroid patients, p < 0.047. HYP patients were also less likely to have lymph node involvement (21.6 vs. 40.5, p < 0.28) and more likely to have low S phase fraction (79.4 vs. 60.4, p < 0.21). There was insufficient data for thyroid function correlation and survival analysis-a weakness in this study.
In women with L-thyroxine supplemented primary HYP, breast cancer is diagnosed over 4 'asymptomatic' years later than in a euthyroid cohort and is a less aggressive disease. A four year period of 'latency' until diagnosis in the HYP cohort has similarly been observed in similar retrospective studies. Prospective clinical and thyroid function correlative studies are indicated to validate these findings.
Explaining Diminished Circadian Rhythms in Extreme Primary & Central Hypothyroidism
Thyroid Hormone Metabolism and Regulation Thursday Poster Basic
Two hallmarks of normal TSH dynamics are high sensitivity to small changes in circulating thyroid hormone (TH) and oscillatory behavior. TSH changes in profound primary hypothyroidism include heightened secretion, slowed degradation, compensatory changes in deiodinase activity—particularly D2 up-regulation in brain, and diminished or absent circadian rhythms. Though the mechanism is unknown, diminished circadian rhythms also are observed in central hypothyroidism, and are speculated to be a cause of the disease. We examined whether TSH secretion saturation, previously suggested in extreme primary hypothyroidism, might explain diminished circadian rhythms in both disorders.
We adapted our published feedback control system simulator to reflect changes in profound primary hypothyroidism, including TSH secretion saturation, and quantified and validated it using multiple clinical data sets—TSH data in thyroid cancer patients following thyroidectomy and T3-only replacement, as well as circadian rhythm studies in patients with varying degrees of primary hypothyroidism. We simulated central hypothyroidism by reducing overall TSH secretion, and also simulated normal TSH secretion without circadian oscillation, maintaining plasma TSH at constant normal levels.
Central hypothyroidism simulations yielded low TH levels and low-to-normal daytime TSH levels, as well as predictively reduced circadian rhythms using the expanded model. However, simulated TH levels remained normal in our constant (oscillation-free) TSH secretion simulations, suggesting that loss of rhythmicity alone is not enough to cause hypothyroidism. This result is supported by evidence in humans with altered sleep schedules, yielding a loss of circadian rhythm but normal plasma T3 and T4 levels, as well as in rats with suprachiasmatic nucleus lesions, which exhibited a lack of circadian rhythm but not hypothyroidism.
Diminished circadian rhythms in central and extreme primary hypothyroidism can both be explained by pituitary TSH secretion reaching maximum capacity.
Pharmaceutical Sciences, College of Health Sciences , Kuwait, Kuwait
Thyroid Imaging Thursday Poster Basic
Hyperthermia may be a consequence of environmental conditions, bacterial or viral infections and/or thyroid storm. The aim of this study is to investigate the acute effect of body temperature elevation on thyroid function and on its radionuclide evaluation.
Thyroid scintigraphy studies were performed on fifteen New Zealand White rabbits weighing approximately 3–3.5 kg. Each rabbit was injected with 115 MBq (3.1 mCi) technetium-99m pertechnetate (99mTc pertechnetate). Static images were acquired using Gamma camera. Two days later the same protocol was repeated for the same rabbit after increasing the body temperature by 2°C. The experiment was repeated again after a 2 day interval at 3°C, and then after another 2 day interval at 4°C. Plasma Free thyroxine (FT4), free triiodothyronine (FT3) and thyroid stimulating hormone (TSH) were measured at control and at different hyperthermic temperatures (+2, 3, 4°C). Isometric tension of isolated rabbit thyroid artery strips were also recorded in organ baths during stepwise temperature elevation.
During hyperthermia the significant decrease in thyroid function and thyroid scintigraphy studies were proportional to body temperature. The reduction was nearly 50%. The recording of isometric tension in rabbit thyroid artery strips in organ baths, showed vasoconstriction during hyperthermia which is significantly proportional to the heating temperature, (n = 10; *p < 0.05). Plasma FT4 and FT3 level were decreased while TSH levels were not affected by acute fever.
Our results indicate that acute hyperthermia causes a transient decrease in thyroid gland function and scintigraphic patterns on radionuclide studies. Thus, body temperatures must be measured before radionuclide studies in order to ensure that interpretation of data is not influenced by hyperthermia.
Surgery, Tulane University School of Medicine , New Orleans, LA
Thyroid Imaging Thursday Poster Clinical
Ultrasound-guided (US) fine-needle aspiration biopsy (FNAB) sampling of the thyroid represents a standard diagnostic procedure in the evaluation of thyroid nodules. The biopsy specimen is usually acquired using two different techniques. In the first technique, short axis is used with observation only of the tip of the needle whilst in the nodule. In the second technique a biopsy needle guides using the long axis to observe the entire needle. Either technique is usually used according to the operator's preference. We performed a retrospective review to compare these two techniques with regard to specimen adequacy.
We performed sonography-guided FNA in 105 thyroid nodules between May 2008-May 2009. The biopsy specimen was acquired using the two different methods after localization by one single operator. The type of technique was correlated with diagnostic accuracy.
63 out of 105 thyroid nodules were biopsied using long axis technique. The rates of inadequate material for long axis and short axis were significantly different (p < 0.05). Interestingly, the difference was more for lesions deeper than 3 cm from the skin (p < 0.05).
This is the first study to compare long and short axes techniques with regard to specimen adequacy for neck lesions. Long axis technique decreased the rate of inadequate material; number of required needle sticks and provides more accurate cytologic evaluation. We consider long axis technique using a biopsy needle guide easier and superior to traditional short axis technique.
The Value of Surgeon-Performed Intraoperative Ultrasound in Patients Undergoing Thyroid Surgery
Thyroid Imaging Thursday Poster Clinical
Introduction: The role of office neck ultrasound (OUS) for evaluating thyroid pathology has been well established. However, the benefits of intraoperative US (IUS) in this setting are unknown. We hypothesized that IUS in this setting would be useful for determining surgical strategy.
Methods: From a prospective database, medical records of 758 patients undergoing thyroid surgery within an 8-year time period were reviewed. All of these patients underwent OUS, followed by IUS by the same surgeon at the time of neck surgery 2–6 weeks later. The ultrasound findings were entered into the database prospectively. IUS was performed after general endo-tracheal anesthesia, with the neck hyper-extended by using a bean bag. All ultrasound exams were performed by the operating surgeons.
Results: In all patients, IUS facilitated the surgical procedure by defining the pathology and aiding in surgical strategy. By guiding a precise incision placement based on the location of pathology, IUS enabled the use of smaller incisions in these patients (4 cm or less in most patients). In 2% of the patients, (n = 13) IUS demonstrated pathology in addition to the OUS that affected the conduct of the operation. The new information included either demonstration of new or resolved central or lateral neck lymphadenopathy (85%), significant increase in size of goiter (8%) and new local invasion (8%). The benefit was most for patients undergoing surgery for recurrent thyroid cancer.
Conclusions: Intraoperative neck ultrasound is useful in mapping out thyroid pathology which allows the surgeon to determine an accurate surgical strategy before the incision is made. This is a new concept of image-guided surgery for endocrine surgeons, which might also change the conduct of the operation in recurrent thyroid cancer procedures.
Endocrinology Unit, Catholic University School of Medicine , Rome, Italy
Thyroid Nodules and Goiter Thursday Poster Clinical
Hemithyroidectomy is the surgical treatment of choice in patients with benign monolobar nodular disease. Nodular recurrence after lobectomy is a frequently observed event especially in iodine deficient areas. Although patients affected by diffuse non-toxic goitre often experience a reduction of the thyroid volume when treated with LT4, the role of LT4 in the management of nodular thyroid disease and prevention of nodular recurrence after lobectomy is still controversial. The aim of this retrospective study was to investigate whether post-operative treatment with LT4 reduces the incidence of nodular recurrences in patients who had undergone hemithyroidectomy for benign monolobar nodular diseases.
233 patients (38 males, 195 females; age 49.9 ± 13.1 years) with no post-surgical evidence of nodular disease in the remnant, were followed-up yearly with serum TSH and ultrasound (US). Nodular recurrence was defined as a lesion of at least 5 mm at US. Patients were divided in two groups: Group 1 (45 patients) who did not receive any LT4, and Group 2 (188 patients) treated with LT4. Group 2 was further subdivided in Group 2a (123 patients) receiving LT4 substitutive therapy (TSH ≥ 0.5 and ≤3 mUI/l) and Group 2b (65 patients) receiving LT4 at TSH-suppressive dose (TSH < 0.5 mUI/l). Mean observation period was 5.8 ± 4.7 years.
71 out of 233 (30.5%) patients experienced recurrence of thyroid nodular disease: 29 patients (64.4%) in Group 1, 24 (19.5%) patients in Group 2a, and 18 (27.7%) patients in Group 2b. The recurrence rate was significantly lower (p < 0.001) in Group 2 compared with Group 1, but no significant difference was observed between Groups 2a and 2b. TG levels showed an inverse relationship with recurrence. Indeed, the within-group difference was statistically significant in Group 1 and Group 2b, but not with 2a, which had the lowest overall recurrence rate among all three groups (64.4%, 27.7% and 19.5%, respectively).
In patients who have undergone hemithyroidectomy for benign monolobar nodular disease, LT4 therapy may prevent recurrence of nodular disease. TSH suppression may not be required for prevention of nodular recurrence in the remnant thyroid tissue.
Radiology, University of North Carolina , Chapel Hill, NC
Thyroid Nodules and Goiter Thursday Poster Clinical
Fine needle aspiration of thyroid nodules is a common procedure performed at UNC by the Departments of Endocrinology and Radiology. We aim to document the added value of on-site pathology for ultrasound guided thyroid fine needle aspiration biopsies. This will be measured in terms of specimen adequacy and number of needle biopsy passes required in two groups: biopsies performed by radiology which use pathology on-site and biopsies performed by endocrinology (without pathology). Both sets of biopsies are reviewed by the same pathologists, allowing for a well-controlled study.
This is a retrospective chart review study of all ultrasound guided adult thyroid biopsies performed at UNC by staff of the Departments of Radiology and Endocrinology. 100 cases performed by radiology and 100 cases performed by endocrinology have been reviewed for specimen adequacy and number of passes required. All cases were performed under ultrasound guidance with a 23G biopsy needle. All pathology samples were reviewed by the UNC Department of Pathology.
The primary data analysis compares specimen adequacy (measured as yes or no) within the endocrinology data subset and radiology data subset. The number of passes required in each group is also assessed. Analysis demonstrates a 6% inadequacy rate with onsite pathology versus a 14% inadequacy rate without onsite pathology. A student t-test analysis demonstrates that this is a statistically significant difference (P < 0.05). Our analysis indicates that there would be an approximate 57% reduction in the number of callback or repeat biopsies by having onsite pathology.
Success of ultrasound guided biopsy in acquiring an adequate tissue sample is significantly improved when performed under the supervision of a radiologist with on-site pathology. Clinical implications include a potential marked reduction in number of repeat biopsies.
Department of Surgery, Massachusetts General Hospital , Boston, MA
Thyroid Nodules and Goiter Thursday Poster Clinical
Fine needle aspiration biopsy (FNAB) of thyroid nodules can yield atypical cytology results in some patients. In this study we aimed to identify different variables affecting the management of patients with atypical FNAB to determine an algorithm of management, including timing of repeat FNA.
An IRB approved retrospective search of the MGH Cytology clinical database identified 254 patients with “atypical” FNAB between 1/2005–12/2007. Clinical, cytological and imaging variables were reviewed, and data was analyzed using SPSS statistical software.
Of the 254 patients with atypical FNAB, 203 patients had data available for analysis, 80% females and 20% males. Further subclassification included: 19% predominantly microfollicular lesions, 21% macrofollicular, 30% mixed cellularity and 30% other. 62% of patients went directly to surgery (group I), 25% had a repeat FNAB (group II) and 13% were followed up (group III). Significant differences between these 3 groups included: younger patients were more likely to go directly to surgery; 2.4% of males had follow-up only vs. 16% of the women; 76% with predominantly microfollicular cellularity went directly to surgery and only 2.6% were followed-up vs. 46.5% and 32% of those with macrofollicular cytology, respectively; 32% of nodules with cystic component were followed-up vs. 9% without. No influence on management was associated with age, history of radiation, Hashimoto's thyroiditis and other US characteristics. Analysis of repeat FNAB timing revealed that 59% of patients had repeat FNAB in <3 months and 41% ≥3 months, with the only variable significantly different between those groups being history of radiation- all those patients had repeat biopsy within 3 months. Repeat FNAB <3 months did not alter the results of the second FNAB, nor change the rate of malignancy on final pathology compared to repeat FNA ≥3 months. Overall rate of malignancy was 15%.
Atypical FNAB cytology constitutes a management dilemma. Current practice relies mainly on established prognostic factors such as gender, age, and cytological features. There seems to be no difference in outcome whether repeat biopsy is performed within or later then 3 months.
Malignancy Rate of Nondiagnostic Fine Needle Aspiration Biopsy
Thyroid Nodules and Goiter Thursday Poster Clinical
Tyhroid nodules are especially common in iodine deficient countries. Fine needle aspiration biopsy of thyroid is an accurate and minimally invasive method. However nondiagnostic fine needle aspiration biopsy (ND-FNAB) of the thyroid leads to unnecessary thyroidectomy. The aim of this study to determine the risk of malignancy in ND-FNAB and evaluate ultrasonographic features of nodules with ND-FNAB.
A total of 1462 patients who underwent FNAB were evaluated in our endocrinology clinic. FNABs were perfomed under ultrasonographic guidance. After second or third ND biopsy patients underwent operation.
A total of 62.2% women and 37.8% men underwent FNAB. Among 3371 FNABs 585 (17.4%) yielded ND cytology The results of the cytologic examination were benign, malignant and indeterminate in 78.4%, 2% and 2.2% of the 3371 nodules respectively. 564 nodules with ND biopsy underwent a repeat FNAB. The second biopsy showed 30.5% nondiagnostic cytology. The third biopsy was perfomed to patients who accepted this approach which yielded 13.7% ND cytology. There was no difference between infracentimeter (18.8%) and supracentimeter (17.1%) nodules with regard to ND cytology. The ND cytology rates were 17.7% in solid, 11.1%. in cystic and 16.7% in mixed nodules. There were no significant relationships between ND cytology and either nodule size or echo pattern. Vast majority of nodules with ND cytology were localized posteriorly (71.9%). Twentyone patients did not accept operation, and 65 patients with ND cytology underwent operation. Malignancy rate was 21.5% (14/65) in ND cytology. Among these 13 were papillary carcinoma one was medullary carcinoma. All ultrasonographic features were similar between benign and malignant nodules with ND-cytology (p > 0.05 in all).
High rate of malignancy necessitates careful management of the patients with ND-FNAB.
Zenker's Diverticulum Presenting as a Thyroid Nodule: A Case Report
Thyroid Nodules and Goiter Thursday Poster Clinical
The incidental discovery of a thyroid nodule by sonography occurs in 19–67% of the general population. These nodules require a work up that often involves fine needle aspiration. An occult Zenker's diverticulum may present as a thyroid nodule on sonography with strong echogenic foci that resemble calcifications but are in fact air within the diverticulum. The difficulty in diagnosing an occult Zenker's by sonography alone is reflected in case reports where the diagnosis is made only after fine needle aspiration or thyroid lobectomy.
We present a case of a 54-year old woman with fullness in her neck for several months. An ultrasound showed a heterogeneous 2.0 cm nodule in the posterior aspect of the left thyroid lobe. Fine needle aspirations yielded follicular cells, squamous cells, filamentous bacteria, and vegetable matter. A CT scan showed air and calcium within the nodule. The patient underwent a neck exploration and left thyroid lobectomy where a 3.5 cm Zenker's diverticulum was identified, resected, and an esophagomyotomy completed.
Transverse ultrasound image of left thyroid nodule.

Surgical pathology confirmed a Zenker's diverticulum.
Sonographic left sided thyroid nodules that exhibit squamous cells, bacteria, or foreign material on fine needle aspiration biopsy should raise the suspicion of an occult Zenker's diverticulum.
Institute for Experimental Endocrinology, Charité-Universitätsmedizin Berlin , Berlin, Germany
Thyroid Hormone Metabolism and Regulation Thursday Oral Basic 1:45 PM
Thyroid hormone biosynthesis requires oxidative iodination of tyrosine residues. Thus, thyrocytes need antioxidant protection against hydrogen peroxide. Oxidative DNA damage is implicated in the formation of thyroid nodules and cancer. Low dietary supply with the trace element selenium (Se) is associated with increased thyroidal damage and exacerbates inflammatory thyroid conditions. Conversely, Se supplementation ameliorates Graves' and Hashimoto's disease. The effects of Se are likely mediated by the expression of selenoproteins, proteins containing the rare amino acid, selenocysteine (Sec).
We have genetically abrogated selenoprotein biosynthesis in thyrocytes by conditional deletion of the gene encoding tRNA(Sec), Trsp. Recombination during thyroid differentiation was mediated by Pax8-Cre. Tamoxifen-inducible Trsp inactivation in the adult was achieved by Tg-CreER. Thyroids were dissected for histological examination, including morphometry of epithelial extension and follicle size. Expression of selenoproteins Gpx1 and Dio1 was assessed by immunohistochemistry and enzyme assay, respectively. The thyroid hormone axis was characterized according to serum hormone levels and T3-regulated transcripts in target organs.
Expression of Gpx1 and Dio1 activity were significantly reduced in the thyroids in both models. Despite the loss of thyroidal Dio1 expression, thyroid hormone serum levels or pituitary TSH-beta were not changed. Likewise, hepatic Dio1 expression was not altered in the Trsp-mutant mice. Thyroid morphology was not changed up to 6 months after recombination, but epithelial extension was diminished in Trsp-deficient thyroids and the mean follicle size increased significantly. In order to increase oxidative stress in the thyroids, animals were treated with perchlorate together with a low iodine diet. However, no indication of increased cell death or tissue disintegration were found.
We conclude from our experiments that, unexpectedly, selenoproteins including Dio1, are not essential for thyroid function. Possibly, non Se-dependent redox systems maintain protection of thyrocytes in the mutants. Reported beneficial Se effects may rest with the immune system and not with the thyrocytes.
Medicine, Baystate Medical Center , Springfield, MA
Thyroid Hormone Metabolism and Regulation Thursday Oral Basic 2:00 PM
We reported that mice with deletion of TRα gene (Thra-0/0) have a cold-dependent increase in energy expenditure. Wild type (WT) and Thra-0/0 mice have D2 mRNA in muscle. In both, levels were ≈10-fold higher in aerobic (Type-I) than fast muscle, but D2 mRNA was 2–3xhigher in Thra0/0, while activity in mouse muslcle has been questioned.
We used microsomes prepared by differential centrifugation. Initial experiments with 2 nM 125I-rT3+1 mM PTU showed activity in proportion to RNA levels, with highest levels in soleus and red fibers of gastrocnemious, and lower levels in Type-II muscle fibers. Because spurious deiodination of 125I-rT3 has been a concern, we validated the assay measuring 125I-T3 production from outer-ring labeled 125I-T4 by HPLC. Results showed production of 125I-T3 in equimolar amounts with 125I-. Activity was resistant to 1 mM PTU.
Using 125I-rT3 as substrate, 125I- production was inhibited in a concentration-dependent manner by T4 in vitro, and activity was reduced by in vivo T4 injections. Activity was increased about 2 fold in Thra-0/0 mice (P < 0.001); it was stimulated about 3-fold by cold and about 8-fold by 2 days of oral cholic acid. The effect of cold was reduced by prazosin or propranolol. Using outer-ring 125I-T4, fractional 125I- production was reduced by increasing concentrations of unlabeled T4 and by T4 administered in vivo. Since D3 activity has been reported in muscle, we added 100nM T3 to reduce T3 degradation. Apparent Km was 2.38 nM, in agreement with measurements in BAT and brain homogenates or microsomes, while Vmax was 240 fmol/h/mg microsomal protein (Lineweaver-Burk plot). Two-day treatment of WT and Thra-0/0 with 0.8 μg T4/100 g every 12h nearly normalized UCP3 mRNA in Thra-0/0 soleus but not in WT.
D2 is expressed in skeletal muscle of mice, substantially more in Type-I than in Type-II fiber muscle. With a sensitive method, D2 activity is demonstrable in muscle microsome with either 125I-rT3 or 125I-T4. Activity is proportional to the mRNA, and its manipulation and responses of T3-dependent genes in muscle to T4 suggest that D2 contributes to the hypermetabolism of Thra-0/0 mice and is a local source of T3 for muscle thermogenesis.
Identification of Organic Anion Transporting Polypeptide 1C1 Amino Acid Residues Required for Thyroxine Transport
Thyroid Hormone Metabolism and Regulation Thursday Oral Basic 2:15 PM
Organic anion transporting polypeptide 1c1 (Oatp1c1) is a high affinity thyroxine (T4) transporter expressed in blood-brain barrier endothelial cells. In the present study we sought to identify Oatp1c1 amino acid residues critical for T4 transport.
2-dimesional topology was predicited and 3-dimensional Oatp1c1 structures were produced using SWISS-model with glycerol 3-phosphate transporter as a template. With these structures as a guide, 10 amino acid mutations were generated using site-directed mutagenesis based on conservation, localization in the putative transmembrane domains, and side chain character. 125I-T4 uptake characterization and cellular localization was carried out with transport assays and immunofluorescence in transiently transfected HEK293 cells.
Wild-type (WT) Oatp1c1 was expressed at the plasma membrane and displayed an uptake profile suggestive of two T4 binding sites (Km1 = 9.6 nM, Km2 = 85.1 nM). Polar and charged amino acids in putative helix 2 including Asp85 Glu89, and Asn92, appear critical for proper Oatp1c1 folding or membrane trafficking. When mutated to Ala, these mutants displayed perinuclear expression and no transport activity. In helix 5, a conservative Trp277Phe, Trp278Phe mutation maintained Oatp1c1 transport activity, but replacing Trp at both of these positions with an Ala abolished Oatp1c1 T4 transport. A Gln365Ala mutation in helix 7 abolished T4 transport, but maintained WT expression patterns. In helix 8, two fully conserved Glys at positions 399 and 409 mutated to either Val or Ala resulted in no change in transport activity in T4 uptake time courses, but displayed apparent substrate inhibition at higher T4 concentrations in kinetic assays. Finally, two mutations in helix 12, Arg601S and Pro609Ala, displayed partial T4 transport activity.
The current study identified specific amino acids involved in Oatp1c1 T4 transport. This information, combined with additional mutations and molecular modeling of Oatp substrates, will map the Oatp1c1 substrate binding sites, and facilitate the prediction of novel Oatp1c1 substrates.
Medicine, Otolaryngology, Pathology and Laboratory Medicine, Mount Sinai Hospital , Toronto, Canada
Thyroid Hormone Action Thursday Oral Basic 2:30 PM
In a previous report, we have shown that PIAS3 (protein inhibitor of activated STAT3) with putative sumoylation properties is a thyroid hormone (TH)- dependent coactivator of hTRβ1 (79th Annual Meeting of the American Thyroid Association, Abstract #88). In the present report, we have performed further studies to elucidate the molecular mechanisms accounting for its coactivator functional effects.
Protein-protein interaction assays were performed in vitro and in vivo using GST pull-down and mammalian two-hybrid assays respectively to determine the interaction of PIAS3 with hTRβ1 in the presence or absence of TH. In vivo studies were performed in HeLa cells for reporter gene activation effects and dual immunofluorescence labeling analyses, while coimmunoprecipitation analysis utilized 293T cells. The role of several post-translational modifications of phosphorylation by protein kinase A (PKA), histone deacetylation inhibition by trichostatin A (TSA), and histone acetyltransferase inhibition by Garcinol were also studied in HeLa cells. The specific roles of SRC1 and PIAS3 were determined by siRNA knockdown and replacements in HeLa cells.
We show that the hormone binding domain of hTRβ1 is essential for a TH-dependent interaction with PIAS3 and that intact RING finger and serine-rich domains are required for PIAS3 binding and coactivator function. PIAS3 complexes in vivo with hTRβ1 and is severely impaired by a siRNA knockdown of PIAS3, but can be reversed by replacement of wild-type PIAS3 coexpression. In wild-type HeLa cells, coexpression of PKA or addition of TSA increases PIAS3 mediated transcriptional activity, whereas added Garcinol dramatically inhibits increased PIAS3 induced coactivator function by SRC-1 but not TIP60. Similarly, a SRC1 knockdown prevents PIAS3 coactivator function. In vitro GST pull-down assays demonstrate that a SRC1/PIAS3/hTRβ1 trimeric complex is induced by the presence of TH.
1) PIAS3 functions as a potent TH-dependent coactivator which facilitates the formation of a trimeric complex with SRC1 and hTRβ1. 2) This TH-dependent trimeric complex can also be modulated by post-translational changes in phosphorylation, histone acetyltransferase and deacetylase pathways.
Division of Endocrinology and Metabolism, University of Pittsburgh , Pittsburgh, PA
Thyroid Cancer Thursday Oral Clinical 1:45 PM
RAS is the most frequently mutated oncogene in human cancer and strongly contributes to neoplastic transformation. The prevalence, clinical significance and predictive utility of RAS mutations in the diagnosis of thyroid cancer have not been established. We report results of prospective molecular analysis performed between April, 2007 and May 2008 on 485 thyroid nodules tested for the most common RAS mutational hotspot codons: NRAS 61, HRAS 61 and KRAS 12/13.
Molecular evaluation was routinely performed on thyroid aspirates from cytologically malignant, indeterminate and non-diagnostic nodules and on selected benign specimens using real-time PCR and fluorescence melting curve analysis.
RAS mutations were found in 39 of 485 nodules (8%) from 37 patients. Of these, 29 were positive for NRAS 61, 8 for HRAS 61 and 2 for KRAS 12/13. Cytopathologic diagnoses included: 2 benign, 20 follicular lesion of undetermined significance (FLUS), 5 atypical or suspicious, 11 non-diagnostic, and 1 malignant nodule. Lobectomy or total thyroidectomy was subsequently performed in 30 of the 37 patients with RAS-positive nodules. Final histopathology was benign in 3 patients (10%) demonstrating 2 follicular adenomas and 1 hyperplastic nodule. Malignancy was confirmed in 27 patients (90%) consisting of 1 follicular carcinoma, 1 oncocytic (Hürthle cell) carcinoma, and 25 papillary thyroid carcinomas (PTC) (21 follicular variant (FV), 4 conventional type). Histologic tumor size ranged from <0.1 to 4 cm. None of the 25 PTCs demonstrated angiolymphatic invasion or extracapsular spread.
In this study we show that detection of a RAS mutation in a thyroid aspirate predicts malignancy in 90% of cases. This includes specimens with non-diagnostic and indeterminate cytology such as FLUS that comprised over 50% of our cohort. Malignant tumors were most commonly FVPTCs and typically occurred at an early stage without extensive invasion or extrathyroidal extension. However, 1 follicular and 1 oncocytic carcinoma were also present. The presence of RAS-positivity is therefore a highly reliable predictor of malignancy and should prompt consideration of surgical management even when the cytologic diagnosis is not definitively malignant.
Spectrum and Prevalence of Novel Types of Activating BRAF Mutations in Thyroid Cancer
Thyroid Cancer Thursday Oral Clinical 2:00 PM
Papillary carcinoma (PC) is the most common type of thyroid malignancy. BRAF mutations are found in 40–45% of these tumors. In addition to the most common point mutation, BRAF V600E, several other mutations in this gene have been reported. In this study, we investigate the spectrum and prevalence of BRAF mutations detected in a large series of thyroid cancers and provide functional characterization of two novel BRAF mutations.
We analyzed 551 papillary thyroid carcinomas for mutations in codon 600 and adjacent codons of the BRAF gene by real-time PCR and post-PCR melting curve analysis on LightCycler (Roche). Direct nucleotide sequencing was used to confirm the mutation type. Each novel mutations was evaluated for the effects on the MAPK cascade by transient expression in HEK293 cells and immunoblotting with phosphospecific MEK and ERK antibodies.
Overall, 196 BRAF mutations were identified in 551 consecutive cases of papillary carcinoma studied. Of these mutations, 190 (97%) were the usual BRAF T1799A (V600E) mutation, and 6 (3%) were various rare types of BRAF mutation. The rare mutation types included a BRAF K601E point mutation (1) and complex mutations BRAFV600E, T599R (2); BRAF T599I, K601E (1); BRAF T599I, V600delinsAL (1); and BRAF V600_S605delinsVD (1). These tumors were a follicular variant (1), solid variant (1), tall cell variant (2), and classic PC (2). Functionally, the novel BRAF T599I, V600delinsAL and BRAF V600_S605delinsVD mutations were characterized by the increase in phosphorylation of MEK and ERK, and therefore appear to be gain-of-function mutations.
Whereas V600E accounts for the vast majority of BRAF mutations found in papillary thyroid cancer, approximately 3% of tumors have other, rare BRAF mutation types. The rare mutations types, including two novel complex BRAF mutations, contribute to cancer development by activating the MAPK signaling. These unusual types of BRAF mutation occur in papillary carcinomas and their detection can contribute to cancer diagnosis in thyroid nodules.
Internal Medicine, University of Pisa , Pisa, Italy
Thyroid Cancer Thursday Oral Clinical 2:15 PM
BRAFV600E gene mutation represents the most common genetic event in papillary thyroid cancer (PTC). Claudin 1 (CLDN1) gene expression is frequently altered in several human cancers, including thyroid carcinoma. The modulation of the purinergic receptor P2X7 may be involved in human carcinogenesis. Recently, we observed a relationship between the 1513A/C loss-of-function polymorphism of the P2X7 receptor gene and either the PTC follicular variant (PFV) or an aggressive cancer behavior. The aim of the current study was to analyze CLDN1 expression and the frequency of both BRAFV600E mutation and the 1513A/C polymorphism of P2X7 receptor in different thyroid carcinoma samples and, to evaluate their potential role as suitable markers of the disease.
57 PTC [34 classical variant (PCV), 12 PFV, 7 tall cell variant (PTCV) and 4 PTC with poorly differentiated areas (PD)], with diverse TNM staging (class I/II: 50.9%; class III: 32.1%; class IV: 17.0%) were immunostained using a polyclonal CLDN1 antibody. 1513A/C polymorphism was evaluated by PCR amplification followed by RFLP analysis and BRAFV600E mutation by PCR-single-strand conformational polymorphism and sequencing. Non-neoplastic thyroid tissue was also investigated.
CLDN1 expression was significantly reduced in PTCV and PD samples (p = 0.01 vs PCV and PFV). 1513A/C polymorphism resulted significantly increased in PFV, PTCV and PD samples (p = 0.003 vs PCV). A significant relationship was found between 1513A/C polymorphism and either CLDN1 expression (p = 0.04) or BRAFV600E mutation (p = 0.0006). BRAFV600E mutation and 1513A/C polymorphism were associated with an advanced TNM stage (p = 0.04 for both), just BRAFV600E relating to lymph node metastasis (p = 0.05). Moreover, considering the joint presence of reduced CLDN1 expression and BRAFV600E mutation, a significant correlation was found with the histological aggressiveness (p = 0.03).
Overall, our preliminary data suggest that the combined use of these molecular markers may represent a potential tool in the early selection of PTC patients with aggressive clinical outcome and, in planning their therapeutic approach.
Prospective Evaluation of Prevalence, Clinicopathologic Features and Somatic Genetic Mutations in Hereditary versus Sporadic Non-Medullary Thyroid Cancer
Thyroid Cancer Thursday Oral Clinical 2:30 PM
Although hereditary non-medullary thyroid cancer (HNMTC) is recognized as a distinct and isolated familial syndrome the precise prevalence and genetic basis are poorly understood. Moreover, whether HNMTC has a more aggressive clinical behavior is controversial.
A prospective clinical trial of patients being evaluated for thyroid nodule(s). The prevalence of HNMTC, clinicopathologic features between sporadic and hereditary, and tumor genotypes were determined. The presence of 6 somatic mutations (RET/PTC1, RET/PTC3, and NTRK1 rearrangements, BRAF, KRAS and NRAS hotspot mutations) in thyroid tumor samples were determine by nested PCR for gene rearrangements and by direct sequencing for hotspot mutations.
402 patients with 509 thyroid nodules were enrolled in the study and 30 patients (7.4%) had a family history of a thyroid disorder in 2 or more first-degree relatives. 18 of the 30 patients with a family history had benign neoplasm on pathology. 12 of 136 (8%) patients with thyroid cancer had a family history. There was no significant difference in gender, tumor size, lymph node metastasis, and overall stage between sporadic and hereditary case (2 or more affected members). Patients with HNMTC were younger at diagnosis than patients with sporadic disease (p = 0.0017). On age and gender-matched comparison of sporadic to hereditary cases (3:1 matched), there was no significant difference in extent of disease (tumor size, extrathyroidal invasion, lymph node or distant metastasis). 79 of the 504 thyroid nodules had somatic genetic mutations (29 BRAF V600E, 29 NRAS, 8 KRAS, 1 NTRK1, 4 RET/PTC1, 8 RET/PTC3). There was no significant difference in the number or type of somatic mutations between sporadic and hereditary cases.
To our knowledge this is the first prospective study evaluating prevalence, and extent of disease and tumor genotype of sporadic versus HNMTC. We found a relatively high prevalence of HNMTC and that these patients present at a younger age. The similar somatic mutation profile and extent of disease observed between sporadic versus hereditary cases suggests a heterogeneous genetic basis for HNMTC.
Friday, September 25, 2009
Association of FCGRIIA with Graves' Disease: A Potential Role for Dysregulated Autoantibody Clearance in Disease Onset
Autoimmunity Friday Poster Basic
Most of the susceptibility loci determined for Graves' disease (GD) to date encode products involved in antigen presentation to T cells/or molecules that control T cell activation, with many genes producing odds ratios (OR) >1.40, demonstrating the importance of disrupted T cell activity in GD onset. One notable exception is association of the thyroid stimulating hormone receptor (TSHR), the major autoantigenic target in GD. Although autoantibody production is key to GD onset it is still unknown whether variation in pathways controlling autoantibody production/clearance could play a role in disease susceptibility. The Fc Gamma Receptor IIa (FcGRIIa) molecule is involved in the clearance of autoantibodies. Association of the rs1801274 single nucleotide polymorphism (SNP), which has been shown to affect autoantibody clearance, has been found with a number of autoimmune diseases including systemic lupus erythematosus and type 1 diabetes.
This study aimed to screen six Tag SNPs within the FcGRIIa region, including rs1801274, to determine if any were associated with GD in a large UK Caucasian dataset consisting of 2504 GD patients and 2784 controls.
Association between the rs1801274 (P = 0.008, OR = 1.13 [95% CI = 1.04–1.23] and rs6427598 (P = 0.015, OR = 1.12 [95% CI = 1.03–1.22]) SNPs and GD was observed. Some haplotypic associations were also observed but appear to be driven by the presence of rs1801274. No other SNPs showed association with GD. No correlation was seen between any of the SNPs and a range of GD clinical phenotypes investigated.
This study has identified FcGRIIa as a new susceptibility loci for GD and added further evidence that FcGRIIa plays a role in autoimmunity. The size of effect detected (OR = 1.12–1.13) suggests that disruption in autoantibody production/clearance could also be playing a small role in disease onset although disruption in antigen presentation/T cell signalling still seems to be key in triggering GD.
R&D, Diagnostic Hybrids, Inc. , Athens, OH
Autoimmunity Friday Poster Basic
Current methods for the detection of Thyroid Hormone Receptor Autoantibodies (TRAbs), such as the KRONUS TSH Receptor Autoantibody Coated-Tube RIA Kit, do not distinguish between TSI and other TRAbs that bind but do not stimulate. TSI are of particular importance because of their role in Grave's hyperthyroidism, where they mimic the function of thyroid stimulating hormone. The development of a cell line and standardized protocol that could be used to specifically detect and differentiate TSI from other TRAbs would be a powerful tool to assist physicians in the diagnosis of Grave's disease.
This novel cell line was developed by stably transfecting Chinese hamster ovary cells with a human thyrotropin/rat luteinizing hormone (LH) chimeric receptor and a firefly luciferase reporter gene. Selection of the clone was based on luciferase expression in response to TSI and results from cell passage stability data. A standardized assay protocol was developed based on results from analytical performance studies which included precision and reproducibility studies.
Stability studies showed that the cell line retained a constant level of luciferase activity in response to TSI over twenty-six passages regardless of the presence or absence of selection media. Results from our cross-reactivity and interference studies showed that that follicle stimulating hormone, LH, and other hormones did not interfere or cross-react at clinically relevant levels. A reproducibility study was conducted at 3 sites between 4 four technicians in order to ascertain the coefficient of variation (CV) for a panel of specimens containing various levels of TSI. The average CV was shown to be 20.8%. In a precision study involving 1 technician who performed the assay over 20 days, the average CV of a panel of specimens was 12%. The experimental CHO cell line was compared to the KRONUS TSH Receptor Autoantibody Coated-Tube RIA Kit using a series of clinical specimens. This set of clinical specimens showed an overall agreement between the two methods of 94.6%.
Our results show that this cell based reporter system is stimulated by TSI, is stable, and performs significantly similar to an FDA cleared predicate device.
Dept. of Medicine I, Gutenberg University , Mainz, Germany
Autoimmunity Friday Poster Clinical
Discrimination between immunoglobulins that bind TSH-R from those with functional autoantibodies that play a relevant role in Graves disease (GD) is warranted. Thus, a validation trial was performed to compare the anti-TSH-R binding assays (TRAb) vs. a novel thyroid stimulating immunoglobulin (TSI) bioassay.
Sera of 200 GD patients (median age 46 yrs/range 13–80 yrs, 162 female) and of 40 euthyroid controls (21 yrs/13–68 yrs, 20 fem) were twice tested for TRAb (RIA and ELIA) and for TSIs in the Mc4CHOluc, a reporter cell line designed to measure the immunoglobulins that bind the extracellular domain of TSH-R and transmit the signals for cAMP-dependent activation of luciferase gene expression. The amino acid residues 262–335 of human TSH-R are replaced by the rat luteinizing receptor to confer greater sensitivity to TSIs than wild type TSH-R. The cAMP/CREB/CRE complex induces luciferase that is quantified after lysis of the cells in the presence of luminescent substrate.
Overall agreement of 91% was reached between the anti-TSH-R binding assays and the TSI Mc4CHOluc bioassay with a positive and a negative predictive agreement of 92% and 87%, respectively. All control sera were TSI negative. The results of the TRAb-confirmed discordant reactivity were 11/200 (5.5%) TSI pos/TRAb-neg as well as 6/200 (3%) TSI neg/TRAb-pos. Patients testing TSI pos/TRAb-neg were hyperthyroid and all had extra-thyroidal manifestations of GD: e.g. orbitopathy (GO, dermopathy, acropachy, and myxomatous cardiac valves. TSIs positively correlated with the clinical severity and activity scores of GO (p < 0.001). Also, TSIs were significantly more prevalent in patients with optic neuropathy and in smokers. Patients testing TSI neg/TRAb-pos were euthyroid and did show a mild course of GD.
TSIs closely correlate with clinical severity and activity of GD and GO. The utility of TSIs for both the monitoring of drug therapies as well as for the prediction of relapse in GD is now prospectively evaluated.
Clinical Evaluation of Thyroid Stimulating Autoantibody [TSAB] Reporter Assay Using Chimeric TSH Receptor Transfected CHO Cell Line: Comparison with Radio Receptor Binding Assay
Autoimmunity Friday Poster Clinical
TSH receptor [TSHR] autoantibodies [TRAbs] are hall mark of Graves' disease (GD). TRAbs are heterogeneous; some bind and activate [thyroid stimulating antibodies (TSAb)] and others bind and block TSHR [thyroid blocking antibodies (TBAb)]. TSAbs are detected by their ability to stimulate (TSAb) cAMP in in-vitro cell bioassay. Both TSAb and TBAb are capable of inhibiting TSH binding to solubilized TSHR [TBI] and are detected by radio receptor assay [RRA]. We evaluated a new TSAb assay that utilizes CHO cells co-transfected with a humanTSHR/LHR chimera [replacing the TSHR C- terminal region known as the primary site for the binding of TBAb with LHR] and a firefly luciferase reporter gene under the control of cAMP response element [Thyretain™ from Diagnostic Hybrids Inc.] and compared it with TBI radio receptor assay [RRA].
The TSAb assay was performed following the manufacturer's protocol. Briefly, the cells were seeded in micro-titer plate and incubated overnight in humidified incubator. Next day appropriately diluted controls and patient samples were added to the wells and incubated for 3 hrs at 37°C. Cells were then lysed and luciferase activity was measured in luminometer and% increase over reference control is calculated. The inter-assay coefficient of variation (%CV) was 5.1 [N = 8]. A total of 117 patient samples (52 GD and 65 other thyroid diseases) were analyzed for TSAb and TBI.
All 65 subjects without GD had levels of <140% [manufacturer defined cut off] for TSAb [Mean ± SD, 32.7 ± 11.3%] and <1.0 U/L for RRA [specificity for both 100%]. Among 52 patients with GD; 35 had active[untreated] disease and 28 of these were positive for TSAb (Sensitivity = 80%) The positive predictive value was 100% and the negative predictive value was 90.3%. Only 22 of these were positive for TBI [sensitivity = 63%]. Combined sensitivity for TSAb and/or TBI was 91.4%. Seventeen patients were on antithyroid drugs at the time of testing among these 8 were euthyroid [1 TSAb, 2 TBI positive] and 9 were considered hyperthyroid TSH <0.1 [7 TSAb and 9 TBI positive].
The new TSAb cell bioassay is simple and reproducible and has a better diagnostic sensitivity than the RRA for the detection of active Graves' disease.
Dept. Bioregulation, LRC, NIID , Tokyo, Japan
Cell Biology Friday Poster Basic
Thyroglobulin (Tg) is a major product of the thyroid gland and is an essential substrate for thyroid hormone biosynthesis. It was shown that in addition to its classical function, Tg regulates thyroid follicular activity by modulating thyroid gene transcription. Tg also regulates cell growth in thyroid cells, lung epithelial cells, and kidney mesangial cells in culture. We have previously identified a fragment of Tg mRNA in cultured mesangial cells.
We have cloned and characterized a novel Tg variant expressed in mouse kidney.
Transcription of kTg starts in the middle of intron 41 of the Tg gene and results in the generation of a novel 13 amino acid segment. Real-time PCR and Western blot analysis indicated that kTg is expressed in the kidney and heart, but not in the thyroid. The presence of a predicted signal peptide in the kTg sequence was supported by the demonstration of a secreted protein from HEK293 cells expressing this gene. Sera from patients with Hashimoto's thyroiditis possessed IgG that recognized kTg.
The present study suggests that organs other than thyroid express a variant form of Tg that could serve both physiological and pathological roles, including that of an autoantigen in tissues where the variant is expressed.
Neurogranin Potentiates Synaptic Transmission
Cell Biology Friday Poster Basic
It has been increasingly recognized that hypothyroidism is associated with memory deficits and abnormal synaptic plasticity, which is thought of as the cellular correlate of learning and memory. However, the mechanism(s) underlying these hypothyroidism-induced synaptic plasticity deficits is far from clear. Neurogranin, which is one of the direct target genes of the thyroid hormone, is enriched in the hippocampus and plays an important role in synaptic plasticity. Decreased levels of neurogranin are highly correlated with synaptic plasticity and memory deficits in various disorders and mental diseases. For example, hypothyroidism is associated with impaired synaptic plasticity and diminished neurogranin levels. In this study, we explored the role of neurogranin in synaptic plasticity. Our data show that overexpression of neurogranin potentiates synaptic transmission in an activity-dependent manner. In addition, neurogranin-mediated potentiation of synaptic transmission mimics and occludes long-term potentiation (LTP), a well-studied form of synaptic plasticity. Moreover, knocking down neurogranin blocked LTP induction. Taken together, our data provide a strong evidence of the critical role of neurogranin in synaptic plasticity.
Electrophysiology Simultaneous double whole-cell recordings are obtained for nearby pairs of infected (fluorescent) and uninfected (non-fluorescent neurons) under visual guidance using differential interference contrast (DIC) illumination. Synaptic responses were evoked with two bipolar electrodes placed on the Schaffer collateral (presynaptic axonal) fibers.
1. Neurogranin potentiate synatpic transmission in an activity-dependent. 2. This potentiation is NMDA receptor-dependent. 3. Neurogranin expression results in CaMKII activation specifically at synaptosomes. 4. Ng-mediated insertion of AMPA receptors at synapses is dependent on calmodulin-CaMKII interaction, which results in CaMKII activation.
The main conclusion of this study is that neurogranin enhances neuronal sensitivity and potentiates synaptic transmission in an LTP-like manner (which is the cellular model of learning and memory). This implies that neurogranin may enhance learning and memory.
Medicine and Medical Science, University College Dublin , Dublin, Ireland
Iodine Uptake and Metabolism Friday Poster Basic
Iodide transporter in the in human placental is known to be at least in part dependent on the anion transporters sodium iodide symporter (NIS) and Pendrin (PDS). A role for the placenta in iodine accumulation and storage and the former's possible control in a dose dependent manner by varying concentrations by of the pregnancy related hormones hCG (up to 60% increase), Oxytocin (up to 45% increase) and Prolactin (up to 32% increase) has been demonstrated by our group. The effect of these hormones in combination was even greater with the most effective combination of 17β Estradiol-Progesterone-Prolactin-Oxytocin increasing uptake by 82%. The aim of this study was to determine the mechanism by which these increases in uptake occur.
RNA was isolated from placental trophoblasts which had been pre-incubation with various hormones both alone and in combination using the quiagen RNA extraction kit. Taqman real time RT-PCR with NIS and PDS probes was carried out to determine the levels of expression of both transporters. NIS and PDS were normalised against the 18s RNA endogenous control.
In all treatments where iodide uptake was increased there were corresponding significant increases in expression level of NIS mRNA as compared with control non-treated trophoblast mRNA (hCG 1.42 ; Oxytocin 1.28 & Prolactin 1.26). There were also increases in NIS expression levels in the combination hormone treated cells(17β Estradiol -Progesterone-Prolactin-Oxytocin 1.56). There were no significant increases in the expression levels of Pendrin in any of the hormone treated cells indicating that the increased iodide uptake observed was solely due to increased NIS expression.
This study suggests a role for pregnancy associated hormones in promoting placental iodide uptake and indicates that modulation of NIS expression may provide protection against iodine deficiency in the fetus.
Endocrinology, Walter Reed Army Medical Center , Washington, DC
Iodine Uptake and Metabolism Friday Poster Clinical
Iododerma is a rare skin eruption that was more commonly reported in the first half of the 20th century when iodide was used as an expectorant, in asthma remedies, and as an antithyroid agent. It was later infrequently reported after the systemic use of iodide-containing radiographic contrast medium or treatment with oral potassium iodide. It has been rarely reported to occur following topical application of iodine. We herein report a 34 year old male with an adrenal mass, who developed an acneiform reaction over the chest and back with subjective swelling of the throat, shortly after treatment with supersaturated potassium iodide (SSKI).
SSKI containing 1g/mL (Upsher-Smith Labs, MN) was administered for protection of the thyroid gland during I123-metaiodobenzylguanidine scintigraphy to evaluate for pheochromocytoma. Though instructed to take only 2 drops twice daily, the patient administered 0.6mL twice per the manufacturer's instructions, with symptom onset the next day. Cessation of SSKI was accompanied by regression of all lesions. The patient's history showed no previous reaction to multiple iodide-containing compounds. As such, Lugol's solution was started, as it was speculated the syndrome was due to an additive in the SSKI, vice iodide itself. Lugol's solution was well tolerated without syndrome recurrence through the procedure and for 3 days post imaging. On the 3rd night, the patient enjoyed a crab and shrimp dinner. The next morning, the acneiform rash recurred, and the patient discontinued the medication. 3 weeks later, he was rechallenged with SSKI to evaluate for recurrence, and within 6 hours developed the same syndrome.
The diagnosis of iododerma was made. A skin punch biopsy was performed to confirm the diagnosis.
This case not only illustrates an adverse effect rarely encountered by endocrinologists, but reiterates the need for clear dosing instructions. Patients should receive explicit SSKI dosing instructions as the manufacturer label states an alternate dose.
A rarely seen iododermic pustular eruption on the trunk one day following SSKI ingestion. This is thought to represent a hypersensitivity reaction to iodine. Resolution is usually spontaneous following cessation of iodide exposure.

Pharmacy Practice and Pharmaceutical Sciences, University of Minnesota Duluth , Duluth, MN
Thyroid and Development Friday Poster Basic
Micronutrients play a critical role during late mammalian brain development. Copper (Cu), iron (Fe), and iodine deficiencies lead to similar defects in late brain developmental processes including reduced myelination of axons, and aberrant hippocampal structure and function, suggesting that these micronutrient deficiencies share a common mechanism that contributes to these derangements. Studies in both rodents and humans indicate that Cu and Fe deficiencies affect the hypothalamic-pituitary-thyroid (HPT) axis, leading to altered thyroid hormone (TH) status. Importantly, the relationship between Fe or Cu deficiencies and thyroidal status has not been assessed during the TH-sensitive period of perinatal mammalian life. We hypothesized that Cu and Fe deficiencies lead to reduction in circulating and brain TH levels during development and that this reduction contributes to the defects in brain development associated with these deficiencies.
To test this hypothesis we rendered pregnant Sprague-Dawley rat dams Cu-, Fe-, or TH-deficient from early gestation through weaning. Metal deficiencies were induced by feeding the dams Cu- or Fe-deficient diets and were confirmed by serum, liver, and brain metal analysis. TH deficiency was induced by addition of 10 ppm PTU in the drinking water. Thyroxine (T4) and triiodothyronine (T3) levels were subsequently measured in the serum and brains (T3 only) of rat pups at postnatal (PN) day 12.
Copper deficiency reduced serum total T3 by 48% (p < 0.05), serum total T4 by 21% (p = 0.06), and whole brain T3 by 10% at PN12. Iron deficiency reduced serum total T3 by 43% (p < 0.05), serum total T4 by 67% (p < 0.05), and whole brain T3 by 25% (p < 0.05) at PN12.
These results indicate that some of the brain defects associated with Fe and Cu deficiency may be mediated through reduced circulating and brain TH levels. We are currently assessing the expression of TH-responsive genes in PN12 Fe and Cu deficient brains to determine the physiological effect of the measured T3 reductions.
Otolaryngology, Head/Neck & Facial Plastic Surgery, HELIOS Kliniken Leipziger Land , Borna, Germany
Thyroid and Development Friday Poster Clinical
Refinements in the surgical technique and intraoperative neuromonitoring have lowered the complication rates of thyroidectomy in the past decades dramatically. Nevertheless the risk of transient recurrent laryngeal nerve palsy (RLNP) is 3.9%, those for permanent RLNP 1.9% respectively; local immediate and intermittent haemorrhage occurs in 1.5%, wound infections in 0.4% as well as postoperative dysphagia still count for 1.3% of the postoperative complications. Therefore in the last 20 years attempts were undertaken to reduce surgical access trauma by minimal-invasive techniques (MIVAT, extracervical accesses: axillary, ABBA). Due to extensive dissection especially in the extracervical routes these procedures do not compile with the term minimal-invasive.
Endoscopic minimal-invasive thyroidectomy (eMIT) should access the surgical field nearby in anatomical defined surgical spaces with minimal operative trauma (Img. 1). The eMIT-technique is defined by a sublingual (optic trocar) and bi-vestibular (working trocars) access to the subplatysmal space with standard instruments (3.7 mm diameter) for minimal-invasive surgery. Under endoscopic magnification the thyroid is reached after opening of the pretracheal muscles. The isthmus is dissected and the thyroid mobilized from medial to lateral. Vessels are identified, separated and dissected by the harmonic scalpell. The recurrent laryngeal nerve is tested by neuromonitoring for integrity. Resected thyroid is removed through the sublingual incision in the midline. Surgical plane is controlled finally.
Anatomical studies (8 embalmed humans) and an experimental study on 5 pigs with short-time survival showed the safety and feasibility of the method. Clinical application in the first 5 humans (first operation on 18th of March 2009) were successful and will be presented.
Benefits of the eMIT-technique are: direct access to anatomically performed spaces (subplatysmal plane), preparation under endoscopic magnification, expected lower RLNP-rate comparable to microscopic techniques (0.6%), lower local infection rates, avoidance of postoperative dysphagia caused by local scar formation and at least removal of the thyroid pathology without visible scar formation.
Preventing Maternal Hypothyroidism: A Moral Imperative
Thyroid and Development Friday Poster Clinical
There is still debate over prophylactic screening for maternal hypothyroidism, despite clear evidence and consensus that gestational hypothyroidism should be avoided, leads to poor neonatal outcomes and impaired neuropsychological development in childhood. Cost-benefit analyses notwithstanding, healthcare providers have a clear ethical duty to prevent certain, probable, or imminent harms to a developing fetus. Screening pregnant women does not make sense; most women do not discover they are pregnant until intervention is too late. In women with regular periods, the typical pregnancy is discovered after the first missed period. Typically, women are advised to purchase a home pregnancy test one week after the first missed period, resulting in a first physician visit 1–3 weeks later following a positive result. This makes it difficult to ascertain maternal hypothyroidism before the first 8 weeks of embryonic development, the critical time. In women who are not planning a pregnancy and/or in women with irregular periods, pregnancies may be discovered much later. Even if a pregnancy is discovered within the first 1–2 weeks, it takes approximately 4–6 weeks for levothyroxine sodium to reach full therapeutic effectiveness.
Using a clinical ethics framework, this presentation provides the moral argument for routinely screening all fertile women for hypothyroidism.
Clinical practice guidelines that fail to recommend routine screening of all fertile women for hypothyroidism are based solely on a cost-benefit analysis. Strong precedents for a preventative ethics approach to screening already exist. Screening for neonatal hypothyroidism has eliminated it as a significant cause of developmental impairment in industrialized countries. Folic acid supplementation became public health policy when it was found to prevent neural tube defects.
This analysis establishes that beneficence-based ethical duties are owed to potential mothers and their unborn children, while the specific principle of nonmaleficence obligates healthcare practitioners not to do harm, and to prevent imminent or known harms. Screening for gestational hypothyroidism is thus a moral imperative that trumps cost concerns.
Pediatrics, Uniformed Services University of the Health Sciences , Bethesda, MD
Thyroid Cancer Friday Poster Basic
Triggering receptor expressed on myeloid cells (TREM) molecule is a mediator of inflammatory response and is considered as a biomarker for sepsis. TREM signaling plays an important role in the regulation of tumor microenvironment, development of metastases and is considered as a prognostic marker for lung metastases from solid malignancies. In this study we examined the possible involvement of TREM signaling in thyroid cancer metastases.
We examined thyroid cancer cell lines that derived from primary thyroid cancer (FTC133) and metastases (FTC236 and FTC238) by real time PCR, Western blot and immunostaining. Gene silencing experiments and pharmacological inhibition of TREM signaling were performed. Human thyroid cancer samples were examined by immunostaining.
TREM expression and activation of TREM downstream target SYK (spleen tyrosine kinase) was detected in all examined cells with highest level in metastases-derived thyroid cancer cell lines (FTC236 and FTC238). Consistently, expression of genes coding for pro-inflammatory cytokines, chemokines and reactive oxygen species (ROS) were increased in FTC236 and FTC236 cells compared to FTC133 cells. Activation of TREM signaling was associated with increased resistance to serum deprivation inducible apoptosis in the metastatic cell lines. Treatment with a SYK pharmacological inhibitor (Emodin) decreased Akt activation and was associated with inhibition of cancer cell growth. In human thyroid tissue samples, TREM expression was increased in cancer compared to normal thyroid tissue and correlated with the presence of metastases as well as multifocal patterns of growth. SYK expression correlated with the level of Akt activation and staining of serial tissue samples showed co-localization of SYK and activated Akt.
Activation of TREM signaling occurs in metastatic cancer cells and correlates with activation of anti-apoptotic signaling. Targeting TREM/SYK pathway using currently available pharmacological compounds could represent a new therapeutic strategy for the treatment of metastatic thyroid cancer.
Medicine, Endocrine Division, Mount Sinai Hospital and University of Toronto Medical School , Toronto, Canada
Thyroid Cancer Friday Poster Basic
Identification of surface biomarkers for predicting aggressive cancers could assist in the improved management of thyroid carcinoma and the designing of relevant diagnostic and therapeutic strategies. In this report, we have performed studies using human thyroid cancer derived cell lines to assess the utility of epithelial cell adhesion molecule (EpCAM) as a potential surface biomarker in the detection of aggressive human thyroid carcinoma.
Using immunocytochemistry, Western blot, FACS and qRT-PCR technology, we have studied the differential expression of EpCAM in several cultured human thyroid cancer derived cell lines consisting of aggressive follicular (WRO, MRO), medullary (TT), anaplastic colon cancer (ARO) compared to a non-aggressive papillary thyroid carcinoma cell line (TPC-1). Additionally, we have compared the results of these studies to the effects in these cultured cell lines of in vitro administration of an immunotoxin (generously supplied by Vivientia Biotechnologies Inc) which links the Fab fragment of EpCAM monoclonal antibody to Pseudomonus exotoxin A (ViciniumR) versus the effects of a full-length EpCAM monoclonal antibody MOC-31 (purchased from AbD seroTec).
Using these investigational techniques, we demonstrate that EpCAM is over-expressed in WRO, MRO and TT thyroid carcinoma and ARO cell lines but not in TPC-1. Treatment with ViciniumR in increasing concentrations added to cell cultures dramatically impaired the growth of not only WRO, MRO and TT, but also ARO cell lines (IC50 = 5pM) whereas much higher concentrations of ViciniumR to 125pM failed to significantly inhibit TPC-1. Addition of full-length MOC-31 EpCAM monoclonal antibody had no significant growth-inhibiting effects on any of the cultured cell lines at concentrations as high as 250pM.
1) These studies in cultured human carcinoma cell lines demonstrate that EpCAM is a potential surface biomarker which can predict aggressive thyroid cancer. 2) Further studies are warranted to determine the role of EpCAM as a potential diagnostic and therapeutic target in the management of aggressive thyroid carcinomas unresponsive to traditional surgery and radioactive iodine therapy.
Research and Development, Diagnostic Hybrids Inc. , Athens, OH
Thyroid Cancer Friday Poster Basic
In 2007, Chia et al. developed a qRT-PCR assay which detects TSHR mRNA in peripheral blood. This assay has since been shown to be highly sensitive and specific for the detection of both preoperative and recurrent DTC and could provide an alternative method for detection and diagnosis. While previous studies have demonstrated that TSHR mRNA is expressed in white blood cells, we wanted to identify the particular white blood cell fractions that express TSHR as a potential means for reducing that background. In addition, we needed to determine the baseline level of TSHR expression in samples obtained from subjects with thyroids, and no known thyroid disease, in addition to subjects without thyroids.
A total of 31 subjects with thyroids and 33 subjects whose thyroids had been removed as a result of thyroid disease were analyzed for TSHR mRNA. Total RNA was prepared from whole blood and 250 ng was analyzed in our qRT-PCR assay using target specific primers. Flow cytometry was used to determine whether lymphocytes, granulocytes or monocytes express TSHR when compared to the TSHR positive control cell line.
Our preliminary results show that using a real time qRT-PCR protocol the mean for TSHR mRNA expression in normal subjects with thyroids (29.9+/−0.3 Cts; 95% CI) was approximately the same as that from subjects without thyroids (30.1+/−0.3Cts). Results from the flow cytometry studies show that the TSHR mAbs recognize this marker in the thyroid cancer control cells. However, the lymphocyte, granulocyte and monocyte fractions were negative for TSHR.
These data demonstrate that a baseline can be established for TSHR mRNA expression in peripheral blood and that this baseline is approximately the same in the two subject populations we studied. Our studies also indicate that while TSHR mRNA is expressed in peripheral blood, the receptor either exists in a form that is not recognized by our mAbs or at a significantly lower concentration than the positive control. In future studies, fluorescent activated cell sorting (FACS) will be used to isolate lymphocyte, granulocyte and monocytes cells followed by preparation of total RNA and testing in our qRT-PCR assay.
Relationship Between BRAF Mutation and Clinicopathlogic Features in Thyroid Cancer Patients-Preliminary Study
Thyroid Cancer Friday Poster Basic
Recently, studies about BRAF v600E mutations are actively underway concerning thyroid cancers. Most of these researches are related to clinicopathologic features and which are regarded as poor prognostic factors. However, some researchers reported that BRAF mutation has no relationship with poor prognosis. In this study, we tried to find out the relationship between the presence of BRAF mutation and clinicopathological features after the operation.
From October 2008 until February 2009, in Seoul St. Mary's Hospital, Catholic University of Korea, we carried out gene studies in 126 patients who underwent the operation after getting an informed consent about the gene studies including the BRAF gene. The operative method was total thyroidectomy with central compartment dissection. We studied clinicopathologic factors of all patients. BRAF mutation analysis was done using the Direct sequencing method.
126 patients underwent operation. 112 patients (88.9%) agreed with performing gene studies. BRAF mutation was found in 75 patients (67%). Age, lymph node metastasis, tumor size, multifocality and tumor number showed no statistical significance between the BRAF positive and the negative group. Extrathyroidal extension and p53 was slightly high in BRAF mutation group (p = 0.04).
In this study, thyroid cancer patients were fully explained about performing the genetic study and underwent with BRAF gene study with those who agreed. BRAF mutation group showed relatively low distribution except extrathyroidal extension and had little statistical significance with the pathologic features representing poor prognosis. Although limitations of a small number of patients and short follow-up period, further investigations seem to be needed to prove that BRAF mutation, which was considered as a poor prognostic factor.
Section of Endocrinology, Diabetes, and Nutrition, Boston University Medical Center , Boston, MA
Thyroid Cancer Friday Poster Clinical
Predictors of well-differentiated thyroid cancer (WDTC) persistence or recurrence have been inconsistent. No single scoring system is superior in predicting WDTC outcomes.
We conducted a retrospective chart review. Patients with ICD-9 code 193 (thyroid carcinoma) seen between 1979–2007 in a large Boston-area multispecialty group practice (Harvard Vanguard Medical Associates) were identified. Of these 1,025 patients, 670 WDTC subjects met study eligibility criteria. Cox proportional hazards models were used to assess predictors of WDTC persistence/recurrence. Independent predictors were gender, age, ethnicity, tumor size, surgical histology, extent of surgery, use of radioiodine, and clinician (endocrinologist or other) managing follow-up. Local extension of disease and lymph node involvement were not assessed. The primary outcome was WDTC persistence/recurrence, defined by either elevated thyroglobulin (Tg) levels in Tg-antibody negative patients or positive imaging. Study entry was the date of surgery. Follow-up was accrued until the first occurrence of the primary outcome or study termination.
Table 1 describes the cohort. There were 5051 total person-years of follow-up; 146 subjects (21.8%) had WDTC persistence/recurrence at a median of 4.2 years (range 0.02–42.5 years) after thyroid surgery. In multivariate regression models, age, sex, ethnicity, number of tumors, surgical histology, radioiodine use, and type of managing clinician were not predictive of the primary outcome. Tumor size ≥1 cm had a protective effect on WDTC persistence/recurrence (hazard ratio 0.49; 95% CI, 0.31 to 0.78; p = 0.002), which persisted after adjustment for extent of surgery and post-operative radioiodine use (hazard ratio 0.56; 95% CI, 0.3 to 0.98; p = 0.04). More complete surgery was also protective (hazard ratio 0.56; 95% CI, 0.34 to 0.91; p = 0.02).
Subject Demographics, Tumor Characteristics, and Management Factors
Total n for each descriptor may not equal 670 due to missing data, and total percentages may not equal 100 due to rounding.
Despite more complete surgery in subjects with tumors ≥1 cm, tumor size <1 cm was a predictor of WDTC thyroid cancer persistence/recurrence. Contrary to other studies, age and sex were not significant predictors of a worse prognosis. Further research is needed to better understand which factors and staging systems predict differentiated thyroid cancer persistence/recurrence.
Thyroid Cancer Friday Poster Clinical
Claudins (CLDN), integral membrane proteins, are the major components of tight junction. CLDN1 is expressed at higher levels in papillary thyroid carcinoma (PTC) compared to other histotypes while CLDN7 gene expression is reported in both normal and neoplastic thyroid tissue. Galectin-3 (GAL3) is a well recognized PTC marker and its overexpression may be associated with invasive and metastatic properties. E-cadherin (E-CD) is a cell adhesion molecule that has a critical role in the establishment of cell polarity and maintenance of the epithelial phenotype. In PTC, reduced E-CD expression has been associated with a poor outcome. The aim of this study was to evaluate CLDN1,7, GAL3 and E-CD protein expression in different PTC subtypes with aggressive course (persistent disease, locoregional/distant metastases) and to analyze the relationship with BRAFV600E mutation.
94 PTC [53 classic (PCV), 25 follicular (PFV), 11 tall cell variant (PTV), and 5 PTC with poorly differentiated (PD) areas] were selected for immunohistochemical analysis. BRAFV600E mutation was examined by SSPC-PCR and DNA sequencing in 84 samples.
most of PCV and PFV showed strong, diffuse, linear and membranous CLDN1 positivity. CDLN1 staining was decreased in PTV and in PTC with PD areas. CLDN7 immunoreactivity showed high heterogeneity both between and within different tumor subtypes. GAL3 was expressed in 92,5% of PTC with variable intensity from weak to strong. Expression was slightly decreased in PFV including solid growth pattern areas. E-CD display a reduced heterogeneous expression at membrane level with positive areas side by side with negative areas. More frequently diffuse staining was observed in areas of follicular architecture. No relationship was detectable with BRAFV600E mutation.
Our study confirms that CLDN1 is upregulated in PTC and may represent a novel marker for this tumor as well as GAL3. No significant association between CLDN7, GAL3 or E-CD protein expression and histological PTC subtypes was observed. Conversely, decreased CLDN1 reactivity was associated with PTC “aggressive” histological variants (p = 0.003), thus suggesting a possible prognostic role of this membrane protein in PTC.
Medical University Vienna , Vienna, Austria
Thyroid Cancer Friday Poster Clinical
Secondary hypercalcitoninemia, the occurrence of elevated calcitonin concentrations in patients with chronic kidney disease in absence of medullary thyroid carcinoma, appears with a prevalence of up to 46%. Up to 54% men with chronic kidney disease stage 5 on dialysis presents with elevated calcitonin concentrations, while in women only up to 28% show hypercalcitoninemia. It has been seen that kidney transplantation leads to a decrease of elevated calcitonin concentrations, but an investigation of a large cohort of chronic kidney disease patients has not been conducted before.
We investigated a group of 133 patients with chronic kidney disease stage 5 awaiting kidney transplantation. We studied whether elevated calcitonin concentrations would decrease one, two, or three years after transplantation. Responding to earlier results in gender-specific analysis, we divided the cohort in two subgroups, separating men from women.
48 (54%) of the men and 12 (28%) of the women with chronic kidney disease stage 5 presented secondary hypercalcitoninemia. Three years after successful kidney transplantation around 82% of men returned to normal calcitonin concentrations. In women secondary hypercalcitoninemia completely resolved within that time. 18% of men continued to have hypercalcitoninemia, although they presented rather low calcitonin levels compared to pre-transplantation values.
The present data show an almost complete reversibility of secondary hypercalcitoninemia in patients with CKD stage 5 after kidney transplantation. All patients with elevated calcitonin concentrations above 30 pg/ml presented declining calcitonin concentrations after kidney transplantation.
Endocrine Surgery, Cleveland Clinic , Cleveland, OH
Thyroid Cancer Friday Poster Clinical
The detection of circulating TSH receptor (TSHR) mRNA is indicative of thyroid cancer (TC). This bloodtest has shown early promise for differentiated TC diagnosis and long-term surveillance, but false negative results do occur. The purpose of this study was to describe a series of TC patients with negative TSHR-mRNA values.
From 251 samples in 176 patients, 30 false negative results in 28 patients were identified. Their clinical records were reviewed to determine TC-related diagnostic tests, operative findings and pathology.
Of 30 false-negative samples, 23 were collected preoperatively and 7 were collected during surveillance <6 months (n = 2) or ≥6 months (n = 5) after surgery. In the preoperative group, 11 patients (48%) had papillary microcarcinomas <1 cm, 7 patients (30%) had aggressive histologies (tall cell, angioinvasive follicular or poorly-differentiated cancers), and only 5 (22%) had classical papillary TC. All patients had clear indications for surgical treatment either by abnormal biopsy results or symptomatic goiter, hence negative mRNA did not impact treatment decisions. These 23 patients contributed a 50% NPV value to a cohort of 94 patients where preoperative TSHR mRNA had sensitivity 67%, specificity 96%, and PPV 98%. In the surveillance group, 5 patients had 7 negative TSHR mRNA samples in a cohort of 60 patients with 96% specificity, 95% NPV, and 50% sensitivity and PPV. Aggressive histology was present in 80% (4 of 5 patients). Recurrence was evident by biopsy-confirmed locoregional recurrence, stimulated thyroglobulin elevation, and either US, CT scan or FDG-PET imaging.
False negative TSHR mRNA values are associated with small papillary microcarcinomas preoperatively, but during surveillance typically occur in patients with aggressive cancers. This pattern may reflect unique determinants of circulating tumor cell biology and bears further study. False negative results did not deter appropriate clinical management, thus TSHR mRNA should continue to be viewed as a useful component of multimodality thyroid cancer care.
Lower Incidence of Anaplastic Carcinoma After Higher Iodination of Salt in Slovenia
Thyroid Cancer Friday Poster Clinical
Anaplastic thyroid carcinoma (ATC) may arise de novo or from a pre-existent differentiated carcinoma. It is well known that higher iodine intake in a diet causes higher frequency of papillary thyroid carcinoma, while the frequency of follicular carcinoma decreases. However, it is not known how the change in iodine intake influences the frequency of ATC. The aim of our study was to compare the frequency of ATC during the periods when the intake of Kalium Iodide in salt was 10 mg/kg and 25 mg/kg.
A total of 205 patients with ATC (140 females, 65 males; median 69 years) were treated in the Republic of Slovenia between 1972 and 2008. In Slovenia, a country with a population of 2 million people, the salt was iodinated with 10 mg of Kalium Iodide/kg and with 25 mg of Kalium Iodide/kg during the periods 1998–2008 and 1972–1997, respectively. The frequency of ATC during these two periods and the characteristics of the patients during these periods were compared.
The mean frequency of ATC during 1998–2008 and 1972–1997 was 6.5 (range 3–12) and 3.8 (range 2–10) patients per year, respectively. During the period 1998–2008 and 1972–1997, the mean patients' age was 72.2 and 66.7 years (p = 0.02) and the mean tumor diameter was 8.6 cm and 9.6 cm (p = 0.21), respectively. However, the median survival of patients was in both periods 3 months.
The frequency of ATC decreased after higher iodination of salt. The patients with ATC in the period of higher iodination of salt period were older in comparison to the period with lower iodination of salt.
Tiroides, Fundación Dr. José Luis Novelli , Rosario, Argentina
Thyroid Cancer Friday Poster Clinical
Papillary thyroid carcinoma (PTC) accounts for 80% of this gland's cancers. It shows very good prognosis, with a 10-year survival in 95% of patients. However, a specific feature is that it develops early metastasis in cervical ganglia.
55 patients operated on between March 2007 and May 2009 with PTC diagnosis. Two groups of patients were studied. Group A: 39 patients without palpable cervical adenopathies and Group B: 16 patients with palpable adenopathies. All patients' necks were examined with DCAP before initial treatment. The echographic features suspicious of malignity were the following: a) cephalo-caudal diameter similar to anteroposterior diameter and >10 mm in size, b) anomalous vascularization, c) heterogeneous cystic parenchyma, d) microcalcifications. Aspiration puncture with fine needle (PAAF) was performed under echography in patients with ecographically suspicious nodes.
DCAP reported suspicious nodes in 7/39 patients in Group A (18%) and in 6/16 patients in Group B (37,5%). PAAF found positive cytology for PTC in 4/7 in Group A (57%) and in 6/6 in Group B (100%), all confirmed by deferred biopsy.

The use of DCAP enabled neck treatment in the first surgery in 10,3% more patients (4/39) without palpable nodes. Not all palpable nodes are metastatic, in Group B only 6/16 had suspicious nodes for DCAP, confirmed cytologically. This prevented the overtreatment of patients.
Is There a Relation Between Hashimoto's Thyroiditis and Papillary Thyroid Carcinoma?
Thyroid Cancer Friday Poster Clinical
Hashimoto's thyroiditis (HT) is often associated with malignant lymphoma and occurs with papillary thyroid carcinoma (PTC). Since the first report by Daily et al in 1955 the relation between HT and PTC has been frequently discussed. Studies to date establish 1% to 36% of patients with coexistent HT/PTC disease. The aim of our study was to evaluate the correlation between HT and PTC.
We retrospectively analyzed the data of 442 patients who underwent total thyroidectomy at the Ankara Numune Training and Research Hospital between December 2008 and May 2009. We recorded ultrasonographic, histopathological and laboratory features of these patients. HT was defined by histopathological examination after the operation. Group 1 consists of patients with HT and group 2 consists of patients without HT.
Mean age and sex distribution were similar in both groups (age: 47,9+–11,0 and 47,6+–14,4 years, male/female: 56/7 and 302/76 respectively). Sixty-three of 442 patients had HT (14.3%). Sixty nine of 442 patients had papillary thyroid carcinoma. PTC ratio was 9.5% (6/63) in patients with HT and 16.7% (63/379) in patients without HT, but this difference was not statistically significant (p = 0,190). All of PTCs in patients with HT were microcarcinoma while 68.2% (43) of PTC in patients without HT were microcarcioma. The thyroid carcinoma was from the parenchyme in 2 patients with diffuse HT, and from the nodule in 4 patients with nodular HT. Tumor size was similar in both groups.
Our results show similar rates of thyroid carcinoma in patients with and without HT. It is important to carefully follow up patients with HT for the development of thyroid cancer, and perform US and FNAB particularly in the presence of nodules.
International Centre of Thyroid Disease, The International Fund “Help for Patients with Radiation-Induced Thyroid Cancer ‘Arnica’” , Minsk, Belarus
Thyroid Cancer Friday Poster Clinical
Since 1992, 247 young Belarusian patients with advanced radiation-induced thyroid cancer (TC) after the Chernobyl accident have received radioiodine therapy in Germany. Today, 84% of them are in complete disease remission, and 79 patients (32%) already have their own children. Other patients will wish to have children, and the confirmation of the disease-free status before planning pregnancy is therefore very important.The goal of this study is to validate for the first time the use of Recombinant Human Thyrotropin (rhTSH) in Belarus during follow up of young women with TC in the period of pregnancy planning.
The study group consisted of 30 females under observation in the National Dispensary of Medical Rehabilitation (Belarus). Inclusion criteria for the cohort-study were: well-differentiated TC; complete surgery; more than 1 yr since the last course of radioiodine therapy, undetectable (<0.2 ng/mL) basal serum Tg and no clinical or US evidence of residual disease. Patients were given rhTSH, 0.9 mg (Thyrogen; Genzyme Corp., Cambridge, MA) as im. injections on 2 consecutive days on levothyroxine therapy. On day 1, 3 and 5, blood samples were drawn for determination of baseline and stimulated serum TSH (DPC, Germany), Tg (Brahms, Germany), and Tg-antibody levels (Pharmacia, Germany). An urine pregnancy test was performed a few days before rhTSH administration.
The mean age of patients at the time of the study has been 23.9 ± 1.8 yr, at the time of the Chernobyl accident 1.6 ± 1.6 yr and 12.7 ± 3.6 yr at the time of thyroid surgery. The peak TSH level after two injections of rhTSH was 111.5 ± 37,1 mU/L sharply decreasing to 10,2 ± 4,3 mU/L on day 5. All 30 patients had baseline Tg below 0.2 ng/ml. Serum Tg increased slightly after rhTSH stimulation to 0.4–0.9 ng/ml in three patients and was stable below 0,2 ng/ml in 27 patients.
Our data have shown that rhTSH can be successfully used in young female patients with TC for proof of complete remission in the phase of pregnancy planning. Under this regimen patients need no thyroid hormone withdrawal and so hypothyroidism with its possible unfavorable impact on the course of the disease and later cognitive development of the offspring can be prevented.
Thyroid Unit, Massachusetts General Hospital-Harvard Medical School , Boston, MA
Thyroid Cancer Friday Poster Clinical
Follicular thyroid carcinoma (FTC) is often diagnosed only after hemithyroidectomy for suspicious cytology of a thyroid nodule. FTC patients usually need completion thyroidectomy to prepare for radioiodine scan and treatment.
In this retrospective study, we have analyzed the long term outcome for 39 FTC patients treated with I-131 (30–32 mCi) to ablate the remnant thyroid lobe (Group LA), as an alternative to completion thyroidectomy. This group was compared to 73 patients (CT) who underwent completion thyroidectomy and to 29 patients who underwent total thyroidectomy (TT) initially. Age, gender, tumor size and grading were not significantly different among groups. All groups underwent I-131 WBS while hypothyroid, after either lobe ablation or total thyroidectomy. Select cases then underwent standard I-131 ablation, based on clinical findings.
After lobe ablation or total thyrodectomy, neck uptake was significantly lower in LA (0.6%) than in CT (2.0%-P < 0.005) and in TT (1.3%-P = 0.054). TSH and Tg levels were not significantly different between groups. TSH was >25 mcU/mL in all patients. Seventy-two percent of LA patients received I-131 ablation, compared with 88% in CT and 93% in TT. Median follow-up was 87 months in LA, 47 in CT, 53 in TT. There was one FTC related death each in LA and TT and no deaths in CT. At the end of follow-up there were 2 living patients with detectable disease in CT, 2 in TT and none in LA (P = NS). As patients without detectable disease were followed over decades, not all had follow-up stimulated Tg's. Of those measured, stimulated Tg's were <2 in 92% of LA (n = 12) and 100% of CT (n = 25) and TT (n = 11). Stimulated or suppressed Tg's <2 were found in 97% of LA (n = 30), 94% of CT (n = 65) and 100% of TT (n = 22). However, in 40% LA patients low level Tg (<2 ng/mL) was detectable at the end of follow-up, compared to 9% in CT and 15% in TT (p < 0.05).
Remnant lobe ablation with I-131 is an effective alternative to completion thyroidectomy in patient with follicular thyroid carcinoma, with similar long-term outcome in terms of survival and disease-free status. Persistence of very low level Tg is more common after this procedure, but this does not indicate an adverse clinical outcome.
Internal Medicine, School of Medicine, Catholic University of Daegu , Daegu, South Korea
Thyroid Cancer Friday Poster Clinical
Papillary thyroid cancer (PTC) is the most common malignancy in the thyroid. Several molecular mechanisms are involved in the development and progression of PTC. BRAF V600E point mutation has been identified in the majority of PTC. BRAF mutation is more prevalent in Korea than other country. We investigated distinct genetic profiles in Korean PTC using cDNA microarrays analysis.
Transcriptional profiles of five PTCs and corresponding normal tissues were generated using cDNA microarrays. The tumors were genotyped for BRAF V600E point mutation. The results of gene expression of cDNA microarrays were confirmed by real-time PCR in 36 PTCs.
Four patients had BRAF V600E point mutation. Expression was increased for 93 genes, was decreased for 16 genes in cDNA microarrays of five PTCs. Realtime-PCR showed high expression of SLC34A2, TM7SF4, COMP, KLK7, KCNJ2 genes, showed low expression of FOXA2, SLC4A4, LYVE-1, TFCP2L1 genes in 36 PTCs. Among these genes, COMP, LYVE-1 KLK7 were previously unidentified genes in microarray of PTC. TM7SF4 gene was previously known to be overexpressed in microarray of PTC with BRAF V600E point mutation.
These findings demonstrate our result is similar to previous result, but show some different results compared with previous result. These findings may reveal clues to the molecular pathways involved in Korean PTC.
Tumor Size Predicts Lymph Node Involvement in Hürthle Cell Carcinoma
Thyroid Cancer Friday Poster Clinical
Hürthle cell cancer (HCC) is a rare tumor that tends to metastasize to the lymph nodes. Some studies have correlated size of Hürthle cell tumors with the risk of malignancy. Whether the size of HCC correlates with the risk of lymph node (LN) metastases, to our knowledge has not been addressed.
A retrospective analysis was performed on all patients diagnosed with HCC on final pathology between 1997 and 2008. The tumor size and lymph node status was obtained for each patient. The data were analyzed utilizing Student's t-test and the Fisher's exact test to calculate the two-tailed p-value.
Out of 39 patients diagnosed with HCC 3 (8%) had LN metastases; 1 had ipsilateral central LN metastases and 2 had ipsilateral central and lateral LN metastases. LN dissection was performed in patients with known metastases (2 were evident on preoperative ultrasound and 1 intraoperatively). Patients with LN metastases were older than those without (mean age: 86.7 and 56.4 years, respectively, p < 0.0001), had larger tumors (mean size: 6 and 4 cm, respectively, p < 0.0001) and were commonly male (2 of 3). No tumor <5 cm presented with lymph node involvement (0/24 with <5 cm cancer had node metastasis and 3/15 with >5 cm cancer had node metastases, p = 0.049).
Similar to what has been found in patients with papillary thyroid cancer, older male patients with Hürthle cell carcinomas greater than 5 cm are more likely to have lymph node metastases. Our data suggest that these patients may benefit from a prophylactic ipsilateral central neck dissection at the time of their initial operation.
Clinicopathologic Features of Follicular Variant in Papillary Carcinoma of the Thyroid
Thyroid Cancer Friday Poster Clinical
Papillary carcinoma of the thyroid(PTC) consists of above 80% all of the thyroid cancer. It has several subtypes besides classic type. Among these, follicular variant is well-known most common but yet is open to dispute in treatment and prognosis when compared with classic type. In this study, we investigated the clinicopathologic features of follicular variant and the differences between the two.
From January 2007 until August 2008, in Seoul St. Mary's Hospital, Catholic University of Korea, 417 patients diagnosed as PTC in preopeative or intraoperative setting and underwent surgery were studied. we make it a rule to perform total thyriodectomy and ipsilateral central lymph node dissection. If a patient was young with micropapillary confined to the thyroid and there was no enlarged lymph node in ultrasonography, we peformed lobectomy of thyroid. we investigated the clinicopathological features of variants of PTC through final histopathology.
Follicular variant was 47(11.3%) of 417 patients. LN metastasis was in 9 patients (19.1%) and was significantly lesser when compared with classic type (137 patient, 37.0%). (P = 0.015) In contrast, tumor encapsulation was 9 patients (19.1%) and was significantly high than classic type (31patients, 8.4%). (P = 0.031) However, there was no significant difference in the multifocality, extrathyroidal extension, thyroid capsular invasion and tumor size. If beyond suspicious malignancy in FNA, two types demonstrated the malignancy, 83.1% and 83.3% respectively. In Galectin-3 test follicular variant was negative in 10 patient (32.3%) but classic type in 29 patient (12.4%) and showed a statistical significance. (P = 0.012)
The follicular variant of PTC have a relatively low rate of LN metastasis and more tumor encapsulation in comparison with classic type, so they have a predictable factor for good prognosis and high accuracy in preoperative FNA. However in Galectin-3 test, follicular variant type represents comparatively higher negative than classic type. Therefore if we found the atypical cells in FNA, we should pay close attention to diagnosis during or after operation.
Department of Otorhinolayngology-Head and Neck Surgery, Korea University College of Medicine , Seoul, South Korea
Thyroid Cancer Friday Poster Clinical
In papillary thyroid carcinomas (PTCs), extracapsular spread (ECS) is seems to be one of the indications of total thyroidectomy. Preoperative radiologic findings may be helpful for detecting ECS,. Many patients, however, undergo completion thyroidectomy according to the results of postoperative permanent section (PS), especially ECS. We investigated the value of frozen section (FS) for detecting ECS.
Medical records of 81 patients with PTC who underwent thyroid surgery and between June 2005 and June 2007 were reviewed. 19 patients were males and 62 were females. Median age was 52 years (range, 17–87). We compared the ECS results of FS to PS.
In 47 patients with ECS negative results on FS, only 18 patients (38.3%) were ECS negative on permanent section. In 34 patients with ECS positive results on FS, all patients had capsular invasion of cancer in final PS. (sensitivity: 54%; specificity: 100%, positive predictive value: 100%, negative predictive value: 38.3%).
Positive result of FS for ECS should be a reliable indicator to determine the extent of thyroid surgery. FS for detecting ECS is thought to be a helpful method to decrease the rate of completion thyroidemtomy.
Surgery, UMDNJ-Robert Wood Johnson Medical School , New Brunswick, NJ
Thyroid Cancer Friday Poster Clinical
Metastatic disease to the thyroid is a rare clinical occurrence. The most common primary sites include the lung, breast, and kidney. Prostate cancer metastasis to the thyroid has only rarely been reported in the literature as it most frequently metastasizes hematogenously to the bone, lung, liver, pleura, and adrenals.
We present a case of an 87 year old man that presented with a palpable thyroid mass and significant weight loss. Fine needle aspiration of the left thyroid mass was suggestive of papillary thyroid carcinoma. A total thyroidectomy was performed showing a 2 cm papillary carcinoma with a second separate small focus of what appeared to be follicular variant papillary carcinoma.
Because of suspicion of prostate cancer, the slides were stained for thyroglobulin and prostate-specific antigen. The smaller focus was a prostate adenocarcinoma metastasis to the thyroid gland.
To our knowledge, this is the first report of a patient with a papillary thyroid carcinoma and a prostate cancer metastasis.
Case of a 70 Year Old Female with a Left Sided Neck Mass
Thyroid Cancer Friday Poster Clinical
The patient is a 70 year old female with a past medical history significant for renal cell carcinoma who was referred to endocrinology for a presumptive diagnosis of metastatic thyroid cancer. In the mid to late 1970's a number of her family members were diagnosed with renal cell carcinoma (RCC) and a genetic predisposition was suspected. Our patient was screened and ultimately diagnosed with RCC in 1977. Genetic testing was performed on most living family members. Affected family members were found to have a balanced translocation of chromosomes 3 and 8. It has since been deduced that 18 adults in 4 consecutive generations have/had the translocation. Eleven of these family members have subsequently been diagnosed with RCC. In 1984, our patient's sister (who also had RCC associated with the 3–8 translocation) was diagnosed with thyroid cancer. Because of concern that thyroid cancer could also be associated with the 3–8 translocation our patient underwent a prophylactic total thyroidectomy. Pathology of her thyroid revealed 2 microscopic foci of papillary carcinoma. The patient presented to endocrinology clinic in early 2009 after her PCP noted a prominent left sided neck mass. An MRI of the neck revealed a 10 × 14 mm mass in the left posterior cervical space. An FNA of the primary mass was performed and pathology revealed cells consistent with metastatic papillary thyroid cancer. In March 2009, she underwent a left modified radical neck dissection. Pathology revealed metastatic papillary thyroid carcinoma. In addition, 6/32 lymph nodes tested were positive for metastatic disease. We have recommended radioactive iodine ablation.
Conclusion: The incidental finding of a left sided neck mass lead to the diagnosis of metastatic thyroid cancer in a patient who was 32 years s/p a prophylactic total thyroidectomy. Given her personal and family history of an autosomal dominant RCC resulting from the translocation of chromosomes 3 and 8, we postulate that the concomitant thyroid cancer in two family members may be linked. All family members are currently being screened with thyroid U/S's and further genetic testing is planned.
Case Report Anaplastic Sarcomatoid Cancer of Thyroid
Thyroid Cancer Friday Poster Clinical
Sarcomas are very rare thyroid cancers (<1%). Anaplastic thyroid carcinoma is an infrequent histological type. The tumor is one of high aggressiveness a rapid course and poor prognosis. Most patients do not live longer than a few months after diagnosis. The presence of sarcomatoid cells requires the performance of differential diagnosis between anaplastic sarcomatoid thyroid cancer and true sarcoma. We present the case of one patient with anaplastic sarcomatoid thyroid cancer.
A 70-year old man was evaluated due to goiter, dysphagia and an increase in his habitual dyspnea. He reported the complaints had begun two months before and had gradually aggravated. He had had previous hemithyroidectomy for nodular goiter and was under treatment with levothyroxine 100 mcgr/day.
In the physical examination he had hard fixed giant goiter. Thyroid ultrasound: right lobe 104 × 100 × 80 mm with cystic areas and calcifications; left lobe with image 20 × 14 mm. The hormonal testing was normal. Broncheal fiberoscopy showed compression and tracheal deviation to the left, and compression of vocal cords. Total thyroidectomy was performed and its histological report was Anaplastic Sarcomatoid Thyroid Cancer with immunohistochemistry positive for Ki 67 (30–40%), vimentin and thyreoglobulin. In the studies of staging metastatic lesions in brain, lungs and local invasion of tumor with compression of trachea were observed. He did not respond to radiotherapy. He died two months later.
Discussion: The above described case showed that this type of cancer is very aggressive and of rapid course despite treatment.
Low Peroxidase Enzymatic Activity of Mutant P.GLN660GLU Thyroperoxidase Identified in Patients with Congenital Hypothyroidism with Organification Defect
Thyroid Diseases Friday Poster Basic
Mutations of TPO gene have been reported as being the most frequent abnormality in thyroid hormone biosynthesis causing congenital hypothyroidism. We identified the heterozygous missense mutation 2068C > G that change a glutamine to glutamic acid at the 660 TPO position (p.Gln660Glu) in two patients with 62% and 48% of iodine discharge in the perchlorate test. Previous report has shown that this mutant protein is expressed properly and localized in the apical membrane. The objective of this study was to evaluate the functional activity of the mutant TPO protein harboring the p.Gln660Glu mutation.
pCMV expression vector containing TPO cDNA was used to introduce the 2068C > G substitution using site-directed mutagenesis and properly design primers. HEK293 cells were transiently transfected using Fugene (Roche). Cotransfection of a pGL3 plasmid for determination of transfection efficiency by luciferase activity was performed to normalize the results. Thyroid peroxidase iodide-oxidation assays were performed to determine TPO activity. These experiments were carried out on spectrophotometer at 353 nm.
The activity of p.Gln660Gln mutant protein was 20,5 + 0,08% of that of the native one.
In conclusion the p.Gln660Gln TPO mutation may contribute to iodide organification defects in congenital hypothyroid children.
School of Clinical and Experimental Medicine, University of Birmingham , Birmingham, United Kingdom
Thyroid Diseases Friday Poster Clinical
Hyperthyroidism is common and the clinical presentation of patients varies widely. Absence of symptoms and signs may result in delayed diagnosis and treatment in 0.5–1.5% of cases.
We investigated 3049 patients with hyperthyroidism simultaneously analyzing the influence of patients' age & gender, disease etiology & severity, symptom duration, and smoking on clinical symptoms and signs. All patients were evaluated using a standard proforma noting classical manifestations of hyperthyroidism. Patients were divided into quartiles according to age [16–32y (n = 766); 33–44y (n = 772); 45–60y (n = 779); ≥61y (n = 732)].
There was a higher prevalence of males (18.4%; 19.2%; 21.3%; 26.6%, p < 0.001) and toxic nodular disease (2.1%; 5.1%; 13.9%; 28.1%, p < 0.001) in older patients. Younger patients had more severe hyperthyroidism (mean fT4: 56.6; 51.7; 45.5; 40.6 pmol/l, p < 0.001). Overall, weight loss (60.7%), heat intolerance (54.9%), tremor (53.9%), palpitation (50.8%) and anxiety (41%) were the most common symptoms. The majority of patients ≥61y were asymptomatic (35.6%; 32.4%; 29.8%; 54.4%, p < 0.001) and the lowest proportion of subjects reporting ≥5 symptoms was found in the elderly (28.3%; 34.9%; 33.9%; 14.8%, p < 0.001). Increasing age was independently associated with reduced odds ratios for the presence of most classical symptoms except weight loss (AOR:1.02, p < 0.001) and shortness of breath (AOR:1.02, p < 0.001). Older age (AOR:1.08, p < 0.001), higher fT4 (AOR:1.01, p = 0.03), male gender (AOR:1.73, p = 0.03) and toxic nodular disease (AOR:3.13, p = 0.01) were independently associated with risk of atrial fibrillation. Higher fT4 and smoking were associated with tremor (AOR:1.01, p < 0.001 & AOR:1.27, p = 0.02) and goiter (AOR:1.01, p < 0.001 & AOR:1.29, p = 0.03) whereas older subjects were less likely to present with goiter (AOR:0.96, p < 0.001). Symptoms and signs of ophthalmoplegia were associated with increasing age (AOR:1.02, p = 0.006 & AOR:1.02, p = 0.001) and smoking (AOR:1.63, p = 0.03 & AOR:1.57, p = 0.002).
Symptoms and signs of hyperthyroidism are more prevalent in younger patients, smokers and those with more severe biochemical hyperthyroidism. We propose a lower threshold for performing thyroid function tests especially in the elderly.
Endocrinology, Mayo Clinic , Rochester, MN
Thyroid Diseases Friday Poster Clinical
Amiodarone-induced thyrotoxicosis (AIT) is a well recognized complication of treatment with this anti-arrhythmic agent. It occurs abruptly, often after many months of treatment. Unfortunately, management options for AIT are limited. In contrast to amiodarone-induced hypothyroidism, no predisposing factors have thus far been identified, yet a higher prevalence was reported in the group of patients with congenital heart disease (CHD). We analyzed a cohort of adult CHD patients on amiodarone in order to determine the prevalence of AIT development and identify risk factors.
A historical cohort study was conducted. We included all Mayo Clinic patients seen in our CHD Clinic over the last 25 years that were treated with Amiodarone for ≥3 months. Baseline data were collected and patients were followed until diagnosis of AIT, discontinuation of amiodarone or last thyroid assessment on amiodarone. The diagnosis of AIT was made by identifying biochemical thyrotoxicosis during ongoing amiodarone therapy.
We evaluated 221 patients. Outcome assessment was possible in 172 patients. AIT developed in 22 patients, which represents 12.79% of the cohort (95% CI: 8.6 to 18.6%). AIT developed after a median of 1033 days on amiodarone (IQR 819–1463 days). The patients that did not develop AIT were followed on amiodarone for a median of 1098 days (IQR 415–2323 days). Women did not have a higher risk then men for AIT development, RR = 0.72 (95% CI: 0.34–1.51). Autoimmunity (any non-thyroidal autoimmune conditions or positive anti-thyroid antibodies) was not statistically associated with the development of AIT (RR = 1.64 with 95% CI: 0.46–5.82). In contrast a significantly lower BMI was present in the group that developed AIT (mean 21.91) by comparison with the rest of the cohort (mean BMI 25.31) for p = 0.0002.
AIT appears more likely to develop in the CHD population exposed to amiodarone than in patients with other varieties of cardiac disease. While autoimmunity does not appear to increase the risk for AIT in this population a lower BMI at initiation of treatment appears to be a strong risk factor. Therefore BMI may be a consideration in determining amiodarone dosing schedules.
Internal Medicine, University of Leipzig , Leipzig, Germany
Thyroid Diseases Friday Poster Clinical
The assessment of tumor vascularisation by colour flow doppler sonography (CFDS) has been suggested for the distinction between benign and malignant thyroid nodules. As microvessels are increased in cancer our objective was to investigate if the perfusion type determined by CFDS reflects the percentage of histologically determined microvessels in adenomas (A) & adenomatous nodules (AN) and papillary carcinoma (PC).
Tissue sections from 10 adenomas, 8 adenomatous nodules and 13 PC and surrounding tissue of 10 PCs and 2 benign nodules were immunostained for CD34. A computerized image analysis was used to determine the microvessel density in four hot spots and ten systematically selected fields. Preoperatively colour flow doppler sonography was performed for all thyroid nodules and classified according to Frates et al.
A ROC analysis on the basis of the histologically determined number of microvessels demonstrated 70% microvessels as an optimal cutpoint for the diagnosis of PC with the highest sensitivity of 92% and highest specificity of 89%. The analysis of the CFDS-classification IV by Frates for the distinction between PC and A & AN showed a sensitivity of 62% with a specificity of 100%.

We found a consistent increase of the CD34 stained percentage of microvessels in PC (83% and 96%) as compared to adenomas & adenomatous nodules (38% and 49%) determined by the hot spot analysis and systematic field analysis. A ROC analysis on the basis of the histologically determined number of microvessels demonstrated 70% microvessels as an optimal cutpoint for the diagnosis of PC with the highest sensitivity of 92% and highest specificity of 89%. The analysis of the CFDS-classification IV by Frates for the distinction between PC and A & AN showed a sensitivity of 62% with a specificity of 100%.
The lower sensitivity of the CFDS-classification as compared with the immunohistologic determination of the microvessel density indicates that the CFDS-classification detects the pathognomonic intranodular microvessels only incompletely. The higher CFDS specificity is most likely due to the detection of other aspects of malignancy in addition to intranodular vascularisation.
Medicine, Obstetrics & Gynecology, Touro University College of Medicine , Hackensack, NJ
Thyroid Diseases Friday Poster Clinical
Postpartum thyroiditis (PPT), an autoimmune disease, occurs in 5–10% of all women. The incidence of PPT in women with Type 1 diabetes mellitus, another autoimmune disease is 25%. Individuals with systemic lupus erythematosus (SLE), yet another autoimmune disorder, have an increased incidence of autoimmune thyroid disease. The goal of the present study is to determine the incidence of thyroid disease during pregnancy and postpartum in women with SLE.
Sixty-three women who participated in the Hopkins Lupus Cohort and who had sera frozen during pregnancy and/or the first year postpartum were included in the study. As the study was retrospective, the timing of the samples during pregnancy and postpartum was not standardized. All samples were assayed for TSH, thyroid peroxidase and thyroglobulin antibodies. Extensive demographic and laboratory data from the Hopkins Lupus Cohort was available (i.e. sedimentation rate, steroid use, etc).
Twenty-four percent of the 63 women were positive for thyroid antibodies. Eight of the 63 women (13%) were on levothyroxine prior to becoming pregnant. Six of the remaining 55 women (11%) were diagnosed with hypothyroid based on their first pregnancy sample. Six of the remaining 49 women had a serum sample available only during pregnancy leaving 43 women who were evaluated for PPT. On average, each woman had 2 postpartum samples available for analysis. The incidence of PPT was 14% (6/43). Only one of the women who developed PPT was thyroid antibody positive either during pregnancy or the postpartum. Analysis of demographic and laboratory data revealed no correlation with the presence of thyroid disease.
The percentage of women with SLE who either had levothyroxine treated thyroid disease prior to pregnancy, who were diagnosed with hypothyroidism during pregnancy, or who developed PPT was 38%. It can be concluded, that women with SLE have a marked increased incidence of autoimmune thyroid disease. It is recommended that all women with SLE should have a TSH and thyroid antibodies performed prior to pregnancy.
Biyokimya, Acibadem University , Istanbul, Turkey
Thyroid Diseases Friday Poster
Thyroid disorders are known to disrupt fertility and reproduction in women and environmental contaminants that are seen as “endocrine disruptors” are thought to affect reproduction through their action on thyroid hormone systems. However, little is known about links between thyroid, reproductive function, and endocrine disrupting chemicals in nonhuman primates.Thyroid status was measured in adult female rhesus monkey breeders at the beginning of the breeding season.
Three related studies were conducted; screening of a group of indoor breeders for thyroid status; comparison of thyroid status to colony records on health and reproduction in a subsample of breeders, and administration of perchlorate and measurement of thyroid status in three lactating breeders. In additional work, three healthy lactating rhesus monkeys were given three different doses of environmental contaminant and thyroid iodine uptake inhibitor, ammonium perchlorate (0.006, 0.34, 12.8 mg/kg/day, respectively) in food for two weeks. Thyroid status variables (TSH, T4, T3, thyroid radioactive iodine uptake) were then measured.
The 95% confidence intervals for TSH, T4 and T3 (N = 66–80) were similar to those previously reported in smaller samples of macaque monkeys. Based on human criteria, 10 of 80 monkeys (12%) were hypothyroid (TSH > 2.0 μIU/mL. Because hypothyroxinemia can be a risk factor in pregnancy, T4 status was compared to past breeding history, breeding outcome for that season, and general health records in a subset of 42 breeders. T4 concentrations were significantly associated with the number of missed menstrual cycles during the previous breeding season. In the monkey receiving the highest perchlorate dose, iodine uptake was suppressed relative to baseline.
The study shows the availability of tools to study thyroid status in rhesus monkeys, the variability of thyroid status in the breeder colony, and the potential ability of environmental factors to influence thyroid status.
Another Strike Against PTU?
Thyroid Diseases Friday Poster Clinical
After 2 yrs of therapy with propylthiouracil for Graves disease, a 39 y.o. Asian female noted pink urine. Hematuria was confirmed. Work-up showed 1.8g prot/24 hrs with serum Cr 1.27 mg/dl. Complement, SPEP, LFT's and electrolytes were normal. ANA and hepatitis screen were negative. ANCA PR-3 antibody was negative; MPO antibody was strongly positive (>100). Renal biopsy confirmed a pauci-immune necrotizing crescentic glomerulonephritis consistent with an ANCA+glomerulonephritis probably related to the PTU therapy. PTU therapy was discontinued, and she has remained in remission from Graves for 6 months.
The duration of PTU therapy is usually 1 year before development of ANCA+vasculitis and often more than 2 years. PTU ANCA+vasculitides show a female predominance with renal involvement the most common manifestation. One study showed that ANCA can be detected in as many as 40% of patients taking PTU with none of these developing vasculitis. Of those who do develop ANCA+vasculitis, MPO positivity is more frequent than PR-3 positivity. ANCA titers do not aid in monitoring the status of the vasculitis once diagnosed.
Methimazole causes the same phenomenon although much less frequently than PTU. Methimazole-induced ANCA+vasculitis causes primarily cutaneous manifestations in the form of a lupus-like syndrome. Treatment of PTU-induced vasculitis ranges from cessation of PTU alone to steroids, immunosuppressant therapy and plasmapheresis. PTU should be discontinued in all cases. In patients without organ involvement, no other treatment may be required. In patients with hematuria but no renal insufficiency, steroids alone may be sufficient whereas if significant disease is present on renal biopsy or more than one organ system is involved, immunosuppresants may be required. Currently, no data supports any particular treatment regimen over another.
The patient stopped PTU when diagnosed with glomerulonephritis and received a course of combined corticosteroid and immunosuppressant, then corticosteroid alone. Her creatinine returned to normal, but she continues to have a mild degree of microscopic hematuria. She is euthyroid off anti-thyroid drugs.
Fibrous crescent typical of crescentic glomerulonephritis.
Department of Endocrinology and Metabolic Diseases, Rui-Jin Hospital, Shanghai Jiao-Tong University School of Medicine, Shanghai Institute of Endocrinology and Metabolic Diseases, Shanghai Clinical Center For Endocrine and Metabolic Diseases , Shanghai, China
Thyroid Diseases Friday Poster Clinical
We reported two unusual cases of hyperthyroidism who were unrespond to almost all kinds of antithyroid treatments: ATDs, corticosteroid hormone, radioiodine, thyroidectomy, lithium, etc. and were both finally effectively controlled by short-acting octreotide.
Case 1 and case 2 were both middle-age women. They presented with thyrotoxicosis with low serum concentration of TSH and very low RAIU values. The underlying causes, such as thyroiditis, iodine-induced or factitious hyperthyroidism, metastatic thyroid cancer and struma ovarii have been explored and ruled out. In spite of good compliance, their thyrotoxicosis could not be controlled with PTU (1000 mg/d in case 1) or MMI (60mg/d in case 2). B-blocker, lithium, methylprednisolone (in both cases) and radio-iodine therapy (in case 2) were all tried and failed. Even after total thyroidectomy in both cases, the hyperthyroidism recurred 5 months later in case 1 and 2 weeks later in case 2. Then short acting octreotide 0.1 mg q8h subcutaneously were first tried in case 2 and then in case 1.
The thyroid function improved greatly 3 days later in both cases. The doses of octreotide were decreased to 2 times a week gradually with consistent efficacy. After one month of octreotide treatment, case 1 developed hypothyroidism and needed L-T4 therapy. But 2 months later, L-T4 had to be discontinued and octreotide was re-started at the dose of 0.1mg qod because of the recurrence of hyperthyroidism in case 1. The thyrotoxicosis was again controlled and she again developed hypothyroidism. Under the preparation of this abstract, case 1 is treated with 100 ug L-T4, case 2 is under the therapy of octreotide 0.1mg twice a week with normal thyroid function.
Although the real cause of hyperthyroidism in these two patients is not identified, the mechanism of short acting octreotide in treating thyrotoxicosis with relative long term effect is not elucidated, and the definite conclusion on the usefulness of somatostatin analogue in treating hyperthyroidism could not be drawn, it provides us an alternative method to rapidly control thyrotoxicosis in patients resistant to different modalities of anti-thyroid therapy.
Neuroendocrinology, Cincinnati Cognitive Collaborative , Cincinnati, OH
Thyroid Diseases Friday Poster Clinical
Toxic metals contribute to pathophysiology of dialysis dementia (Al), autism (Hg), neurodegeneration/neuropathy (As), Parkinson's/Lyme (Mn) and Alzheimer's disease (Al, Hg, Zn). Thyroid disease impairs cognition, likely via immunopathology after euthyroidism is achieved, and is associated with depression, especially bipolar. Urine porphyrins are associated with neuropathophysiology, perhaps via direct porphyrin toxicity. Symptomatic porphyria is rare; however, even low levels of toxic metals, particularly Hg, Pb or As, individually or in combination, often cause/s abnormal quantitative urine porphyrins whose association with thyroid disease or its related neuropsychiatry is unknown.
Urine samples were collected in dark containers, usually after achieving euthyroidism in thyroid patients. Brain SPECT used Tc-99m-HMPAO or Tc-99m-ECD IV in a quiet, dark room, to monitor cerebral pathophysiology with indices of cortical metabolism (CMi) and stimulated perfusion (CPi). Results were felt statistically significant if p < 0.05 using appropriate multiple component regression or standard two parameter comparisons, including thyroid disease or its subsets vs. other neuroendocrine patients, such as diabetics and traumatic brain injured (TBI).
Thyroid patients had significant (p < 0.05) correlation of abnormal corproporphyrins (likely due to Hg toxicity) and CPi which was more robust than noted for diabetics. Depressed patients were nonsystematically but confidently identified and especially thyroid disease associated bipolar patients trended toward marked Hg toxicity. Patients with history of Hg and other metal or other neuropathology were more severely affected. Patients treated with dimercapto-propane sulfonate (DMPS) and agents to enhance brain perfusion, such as omega 3 fish oil or cilostazol, and immune modulators such as vitamin D, statins and antihypertensives, stabalized or improved SPECT indices and clinical symptoms.
Toxic metals, particularly Hg body burden, identified by fractionated, quantitative urine prophyrins, correlate with thyroid associated cognitive impairment and possibly neuropsychiatric disorders, particularly bipolar depression.
TSH Secreting Pituitary Adenoma in an 24-Year-Old-Man
Thyroid Diseases Friday Poster
We report a case of hyperthyroidism due to TSH secreting pituitary adenoma in 24-year-old man. Computerized tomography (CT) scan and magnetic resonance (MRI) reveal a pituitary tumor. Elevated alpha TSH-subunit levels confirmed the diagnosis. After operated the patient became euthyroid.
Thyroid ultrasonography confirmed slightly enlarged isoechogenic thyroid gland. The thyroid scintiscan with Tc pertechnetate showed uniform uptake of radioactivity. Thyroid autoantibodies were negative. After two months the therapy was stopped, because of elevated values of serum TSH which suggested the presence of TSH induced hyperthyroidism. Computerized tomography (CT) scan and magnetic resonance confirmed a intrasselar mass with supra and parasellar extension (Fig. 1). The diagnosis was confirmed by elevated μ- subunit serum levels 4.9 mlU/ml (normal values for man 0–0.8 mlU/ml).
The following endocrine tests were performed to confirmed the diagnosis of hyperthyroidism induced with TSH secreting pituitary adenoma: TRH - test: 200 μg TRH i.v. was administered with blood samples collected in 0, 15, 30, 60 and 90 min. and an absent TSH response to TRH was noticed (0' = 8.6 μU/ml TSH, 15' = 9.1 μU/ml TSH, 30' = 8.6 μU/ml TSH, 60' = 8.6 μU/ml TSH, 90' = 8.6 μU/ml TSH). TSH suppression test: performed with T4 orally and failure of T4 to reduce the serum TSH was noticed. So autonomous secreting of thyrotropin was demonstrated by these two dynamic tests. Serum growth hormone, cortisol, testosterone, FSH, LH and prolactin were measured and their concentrations were normal. After the confirming of the diagnosis the patient was operated. A week later the patient was euthyroid FT3, FT4 and TSH levels return to normal values. Five months after the operation the patient is still euthyroid.
This case we report as a rare form of hyperthyroidism, first reported case in Macedonia. Also, this case demonstrates the needs for determination of TSH levels in all cases of clinical hyperthyroidism.
Toxic Nodule Masking Thyroid Hemiagenesis: Case Report
Thyroid Diseases Friday Poster Clinical
Thyroid hemiagenesis is a rare anomaly with a prevalence of 1 in 2000. Agenesis of the left lobe occurs more frequently. While earlier studies found females were affected more than males, a large ultrasound study of unselected school children showed no prevalence difference between sexes. It can be associated with other thyroid disorders, most commonly, hyperthyroidism due to Graves'. We report an unusual case of hyperthyroidism due to toxic adenoma in a patient with thyroid hemiagenesis.
A woman aged 17 with no past medical history presented with 26 lb weight gain over 3 months, increased appetite, jitteriness and palpitations. She denied bulging eyes. A paternal aunt had Graves' disease. Vital signs were normal. Right eye was slightly proptotic with no stare or lid lag and extraocular movements were intact. Thyroid was normal in size with a 2 cm palpable nodule in the right lobe. There was mild tremor of outstretched hands. Given the patient's age, thyrotoxic symptoms, and unilateral proptosis, Graves' disease was suspected.
Labs showed TSH 0.01 (0.47–4.68 uIU/ml), free T4 1.5 (0.9–1.4 ng/dl) and free T3 of 642 (287–455 pg/dl), TPO and Tg abs negative, TSI normal. A thyroid uptake and scan showed elevated uptakes with a hyperfunctioning nodule on the right with a small area of decreased activity in the mid to upper right lobe. Left lobe activity was absent. Ultrasound revealed the absence of left thyroid lobe, normal isthmus, normal-sized right lobe with a large, hypoechoeic 2.64 cm nodule. Treatment with methimazole and propranolol resulted in clinical and biochemical euthyroidism.
Thyroid hemiagenesis is a rare and potentially confusing finding. The cause is unknown, although a genetic basis is suggested by the occurrence in monozygotic twins and siblings. The characteristic hockey stick appearance on scintigraphy must be distinguished from other causes of unilateral uptake including an autonomously functioning nodule with suppression of the rest of the thyroid, unilateral inflammatory or infiltrative diseases. Ultrasound now easily establishes the diagnosis.
Thyroid Hormone Negatively Regulates the Myosin Heavy Chain β Promoter by Interference with the Activity of Transcription Enhancer Factor Family
Thyroid Hormone Action Friday Poster Basic
The expression of cardiac myosin heavy chain (MHC) β gene, a molecular marker for heart failure, is repressed by thyroid hormone (T3) and its receptor (TR). However, the mechanism for this negative regulation is unknown. Human MHCβ gene promoter was reported to harbor two M-CAT elements and an A/T-rich sequence which can be recognized by the transcription enhancer factors (TEFs). It is also known that stimulation of α1-adrenergic receptor signaling, which mimics the pathophysiology of heart failure, enhances the activities of TEFs.
We studied the functions of TEF family (TEF-1, DTEF-1 or RTEF-1) and T3-bound TR on the activity of human MHCβ promoter (nt. −295/+125) using CAT-based reporter analysis in CV1 cells, gel shift assay and immunoprecipitation.
Gel shift assays revealed that TEF-1 recognizes two M-CAT elements and an A/T-rich sequence in MHCβ promoter and reporter analyses indicated that all these elements are required for the full activation by TEFs. Another transcription factor, MEF2 (myocyte enhancer factor-2), involved in cardiac morphogenesis also enhanced the MHCβ promoter activity and co-expression of TEF and MEF2 dramatically increased it. Their synergistic effects may be via protein-protein interaction, since the DNA binding of MEF2 is not proven. Interestingly and importantly, T3-bound TR suppressed the TEF-induced activation of MHCβ promoter in a dose-dependent manner of the ligand and receptor. Deletion analyses showed that the DNA-binding domain of TR is critical for the suppressive activity. Immunoprecipation study using CV1 cell extracts expressed with FLAG-tagged TR and myc-tagged TEF-1 demonstrated in vivo association between TR and TEF-1.
These data suggest that T3-bound TR interferes with the function of the activator TEFs, resulting in inhibition of the MHCβ promoter activity.
Comparison of Antithyroid Drugs Efficacy on P Wave Changes in Patient with Graves' Disease
Thyroid Hormone Action Friday Poster Clinical
Some precursor P wave changes can be seen in electrocardiogram (ECG) before the atrial fibrillation (AF) rhythm occurs in the hyperthyroidism. Our aim was to evaluate the influence of hyperthyroidism on P wave duration and dispersion, to investigate the effect of two antithyroid drugs on P wave duration and dispersion.
Fifty patients (13 men, 37 women; mean age 39.2 ± 13.2 years) with newly diagnosed overt hyperthyroid patients with Graves Disease were enrolled in the study. The maximum P wave duration (P max) and the minimum P wave duration (P min) were measured in all 12-lead surface ECGs. The P wave dispersion (PWD) was defined as the difference between the Pmax and the Pmin. The patients were randomized to propylthiouracil (PTU) (n = 24) and methimazole (MMZ) (n = 26) groups respectively. After patients became euthyroid, ECG was repeated.
The maximum P wave duration (P max) was 90 (80–110) and 90 (90–110) msec, (p = 0.586), minimum P wave duration (P min) was 60 (50–70) and 60 (50–62.5) msec, (p = 0.824) and PWD was 35 (22.5–48.7) and 40 (30–40) msec, respectively (p = 0.952) in PTU and MMZ groups. After euthyroidism was enhanced, P max was 80 (80–90) and 87,5 (80–90) msec (p = 0.676), P min was 60 (50–65) and 60 (58.7–65) msec (p = 0.404) and PWD was 27.5 (20–35) and 27.5 (20–30) msec in PTU and MMZ groups, respectively (p = 0.540). In both of PTU and MMZ groups after antithyroid treatment PWD decreased (p = 0.009 and p < 0.001, respectively). However effects of antithyroid drugs on PWD change were similar (p = 0.486).
P wave duration and PWD are found to be prolonged in hyperthyroid patients with Graves disease. Thus, we can conclude that improvements in P wave alterations is not associated with the type of antithyroid drug but with only achievement of euthyroidism.
Thyrotoxicosis After Parathyroid Surgery: 2 Case Reports
Thyroid Hormone Action Friday Poster Clinical
In 1975, a phenomenon known as “palpation thyroiditis” was described by JA Carney et al. as a separate entity from other inflammatory thyroid diseases. Also known as a multifocal granulomatous folliculitis, it is characterized by certain histopathological features, including: scattered follicular involvement; inflammatory infiltrate consisting of macrophages, lymphocytes and plasma cells; presence of vascular lesions such as hemorrhages and hemosiderin-laden macrophages. Since then, reports of thyrotoxicosis thought to result from physical manipulation of the thyroid gland have been described in patients undergoing parathyroid exploration for hyperparathyroidism. In most cases, the degree of thyrotoxicosis is mild and transient, and it resolves without medical intervention. However, it has rarely been associated with symptomatic thyrotoxicosis.
Herein we present two recent cases of thyrotoxicosis following parathyroid exploration.
A 74 year old man with Parkinson's disease, who underwent parathyroid surgery for primary hyperparathyroidism, was admitted five days post-operatively with severe muscle tremors and jerks. Although his neurologic symptoms were ultimately attributed to mild hypocalcemia, his thyroid function tests were significant for thyrotoxicosis and a four-hour uptake performed was low. A 70 year old woman with a history of osteoporosis and kidney stones was admitted two days after undergoing parathyroid exploration for primary hyperparathyroidism with palpitations and lightheadedness due to a new-onset of atrial fibrillation. Her thyroid function tests were also notable for thyrotoxicosis, but no uptake was performed. Notable similarities between the two patients include normal thyroid function pre-operatively, diagnosis of multiple gland involvement after four-gland exploration, and resolution of the thyrotoxicosis within six weeks of the surgery.
This is, therefore, a potential complication that should be considered in patients who develop symptoms suggestive of thyrotoxicosis after undergoing parathyroid surgery.
Medicine, Schulich School of Medicine and Dentistry, University of Western Ontario , London, Canada
Thyroid Hormone Metabolism and Regulation Friday Poster Clinical
The individual levothyroxine (T4) dose requirement varies highly between patients and is difficult to predict. Recent studies indicate that transporters are required for thyroid hormone as shown by the role of Monocarboxylate Transporter 8 for levothyroxine uptake in the brain. We hypothesized that T4 transporters in the liver facilitate T4 uptake, and that variation in hepatic uptake due to genetic polymorphisms of the Organic Anion Transporter 1B1 (OATP1B1, gene SLCO1B1) may contribute to the interindividual T4 dose variation. In this study we focused on the SLCO1B1*5 (521T>C) variant of OATP1B1, which has been suggested to have decreased transporter activity.
We recruited patients with previous thyroidectomy for thyroid cancer. They were 18 years or older, and had no signs of persistent or recurrent disease. They had a stable T4 dose for at least 3 months and a TSH at target below 1 mIU/L. The T4 daily dose was adjusted per kg body weight, and a blood sample obtained to determine TSH, Free T4, Free T3 and thyroglobulin. Genotyping for OATP1B1 was performed using a TaqMan Real Time SNP Assay.
We included 112 patients, 83 women and 29 men. Genotyping identified 73 carriers of SLCO1B1 TT (wild-type), 34 of SLCO1B1 TC, and 5 of SLCO1B1 CC. The T4 dose/kg body weight (mean ±SD) in these subgroups was 2.15 ± 0.46, 2.08 ± 0.44, and 2.13 ± 0.32 microg/kg, respectively (P = NS). There was no difference in age, weight, waist, or thyroid function tests among groups.
The 521C variant is not associated with a change in T4 dose requirement. This suggests that OATP1B1 alone is not sufficient to alter systemic exposure to ingested T4, or possibly that expressed levels of other thyroid hormone uptake and efflux transporters compensate for the reduced OATP1B1-mediated hepatic T4 uptake among subjects who harbor the variant allele.
Department of Nuclear Medicine, Clinical Center , Niš, Serbia
Thyroid Imaging Friday Poster Clinical
Medullary thyroid carcinoma (MTC) is a tumor of neuroendocrine origin with multiple somatostatin receptors (sst 2–5) expression, which represent the molecular basis for the clinical use of somatostatin analogues in diagnosis and treatment and their in vivo localisation. The aim of this study was to assess the diagnostic efficiency of 99mTc-EDDA/HYNIC-TOC (Tektrotyd) scintigraphy in the detection and staging of patients with MTC and to analyze its influence on managing strategy.
Nine patients with sporadic MTC, aged 53–70 years, were submitted to radionuclide investigation. Sequential scintigraphy using 99mTc-Tektrotyd was performed 2 and 24 hours after the injection of 740 MBq of the tracer. All the patients were imaged after the surgery during the follow up (2–17 years), whereas three of them were imaged before the surgery as well. Other imaging techniques were also applied and analyzed in individual cases and compared with 99mTc-Tektrotyd scan.
Out of the 3 patients who were imaged before the surgery, one was found to have increased uptake in primary tumor, while the scans of the other two showed cervical and axilar lymph node involvement beside the primary tumor. Scintigraphy using Tektrotyd detected a significantly greater number of lesions in other 5 out of 6 patients during the follow-up after thyreoidectomy, so that the patients were upstaged. In one of these patients, who had Tektrotyd avid metastases in bones, lung and lymph nodes were successfully managed using somatostatin analogue (Sandostatin LAR), while the other two with widespread metastases were selected for 90Y-DOTATOC therapy. In one patient Tektrotyd scan demonstrated mediastinal lymph nodes, but failed to show 4 bone lesions.
It can be concluded that 99mTc-Tektrotyd scan is a sensitive technique for diagnosis and follow-up of patients with MTC which can be used both for preoperative staging and for the detection of local recurrence and distant metastases. Moreover, the patients with widespread somatostatin avid metastatic lesions could be managed using either cold or labeled somatostatin analogues.
School of Clinical and Experimental Medicine, University of Birmingham , Birmingham, United Kingdom
Thyroid Nodules and Goiter Friday Poster Basic
PTTG Binding Factor (PBF) is a poorly characterised transforming gene that is overexpressed in thyroid tumors. However, little is known about the precise role of PBF in vivo. In preliminary studies we assessed PBF expression in multinodular goiters (MNG) harvested at surgical excision. PBF mRNA expression was 2.6-fold higher in MNG tissue (n = 25, p < 0.01) than in normal thyroid tissue obtained during laryngectomy. Western blot analysis confirmed an approximate 2-fold increase in the level of PBF protein in MNG compared with normal thyroid.
We next generated a murine transgenic model of targeted overexpression of PBF in the thyroid to study its function in vivo. Transgenic mice were generated by pronuclear injection of a HA-tagged PBF transgene driven by the bovine thyroglobulin promoter, and founders identified by PCR.
Western blot analysis confirmed elevated levels of PBF-HA in thyroids from homozygote mice compared with wild-type (WT) FVB/N mice, with no significant expression in other tissues. Immunohistochemical staining using an anti-HA rabbit polyclonal antibody also detected extensive PBF-HA expression in thyroid follicular epithelial cells.The mean weight of thyroids from 6–12 week old homozygote mice (4.5 ± 0.8 mg, n = 18) was significantly greater than thyroids from WT mice (1.8 ± 0.2 mg, n = 15, p < 0.0001) of similar age. By 6 months of age the mean weight of thyroids from homozygote mice had increased further to 6.3 ± 1.1 mg (n = 11). Serum analysis by radioimmunoassays indicated no significant difference in thyroid function [serum T4 (3.1 ± 0.9 versus 3.2 ± 0.5 μg/dl, p = 0.207), T3 (118.4 ± 23.6 versus 140.5 ± 17.2 ng/dl, p = 0.128), and TSH (81.3 ± 20.3 versus 74.7 ± 14.7 ng/ml, p = 0.669)] between homozygote and WT mice, respectively.
These results demonstrate that targeted overexpression of PBF causes significant enlargement of the thyroid gland in vivo independent of thyroid hormone status. Given that PBF expression is induced both in human tumors and MNG, these results implicate PBF as having an important role in promoting goitrogenesis as well as thyroid tumorigenesis.
General Surgery, Cerrahpasa Medical Faculty , Istanbul, Turkey
Thyroid Nodules and Goiter Friday Poster Clinical
Fine needle aspiration biopsy (FNA)in thyroid nodules may not always give the correct result for the characteristics of a nodule. We used the diagnostic classification recommended by Papanicolau Society of Cytopathology for increasing the coherence of cytology and histology and for finding the resource of mistakes.
The results of frozen section(FS) and histologic analysis (HA) of 245 patients which had undergone FNA between August and December 2008 were analyzed. FNA results are classified 6 diagnostic categories.
Among the 96 patients who had benign results (BR) after FNA and FS, 69 patients (28%) had BR and 17 patients (7%) had follicular adenoma (FA) in the histological analysis (HA). 100 patients had follicular lesions (FL) or follicular neoplasm (FN). These patients were evaluated in 3 subgroups according to their histological types. I. group: 11 patients were diagnosed as FN and hurthle cell neoplasm (HCN) with FNA and FN(5), HCN(2), papillary thyroid cancer (PTC)(4) in FS and 5(2%) of them had FA in HA and 2 of patients (1%) had HCN and four of the patients (2%) had PTC.II. group:64 patients were diagnosed as FL by FNA and FN(59), HCN (3), hurhtle cell metaplasia in FS. 59 patients (24%) had FA, 3 patients (1%) had hurthle cell adenoma, 2 patients (1%) had BR in the HA.III.group:25 patients were diagnosed as FL by FNA and FN (23), benign (2) in FS. 3patients (1%) had folliculary thyroid cancer(FTC), 2 patients (1%) had PTC, 10 patients (4%) had PTC+FA, 8 patients (3%) had BR and 2 patients (1%) had BR+PTC in HA. 7 patients who had a suspect malignant FNAB result and FS result as PTC were accepted as PTC with histological analysis (2%). All of the 52 patients (21%) with malignant findings at FNAB and FS were diagnosed as PTC with HA.
The success of cytologic results of fine needle aspiration biopsy can be improved by knowledge, experience, technical equipment and by setting a standard terminology for pathology. The Bethesta Classification which is consisted of 6 diagnostic categories is a useful evaluation method for cytologic analysis. Among 6 of the groups the group with the most cytological diversity was the groups with follicular lesion and neoplasm.
Laval University , Quebec, Canada
Thyroid Nodules and Goiter Friday Poster Clinical
To assess the efficacy of ultrasound guided thyroid fine needle aspiration biopsies (USFNAB) performed in the clinic by non-radiologists in patients whose initial FNA were nondiagnostic with palpation guided FNA (PGFNAB). Second, to determine whether patient care can be enhanced by consolidating the diagnostic workup of nondiagnostic thyroid nodules by circumventing the inherent inefficiencies associated with radiological referral.
This is a retrospective analysis of 161 patients followed for thyroid nodules. All USFNABs were performed by a non-radiologist on consecutive patients with a previous non-diagnostic PGFNAB at a University based teaching hospital in Montreal, Canada. Biopsies were performed using a 20-gauge fine needle with a Mylab25 Biosound Esoate ultrasound (US) machine. Samples were then classified according to adequacy of sample and pathological findings.
One hundred and thirty-three patients underwent 161 USFNABs. The specimen adequacy rate was 91.3% (147/161). Among the adequate specimens, 7 were malignant (4.4%), 7 were suspicious for malignancy (4.4%), 86 were benign (53.3%), and 47 were indeterminate (29.2%). An analysis of thyroid USFNAB adequacy rates based on nodule consistency (cystic/complex vs. solid) proved statistically insignificant (P = 0.59). Likewise, there was no significant difference (P = 0.34) in the inadequacy rate between small (<1.5 cm) and large nodules (≥1.5 cm).
Our experience demonstrates that USFNABs performed in clinic by a non-radiologist is a promising tool for improving specimen adequacy for nodules initially classified as nondiagnostic. It also avoids the need for radiological consultation in the majority of cases thus improving efficacy in the work up of nodules. No statistically significant relationship was found between adequacy rate and nodule size or consistency.
Determination of the Proportion of Metastatic Thyroid Cancers Originating from Solitary Nodules Versus Multinodular Goiters
Thyroid Nodules and Goiter Friday Poster Clinical
The belief that a nodule in the setting of multi-nodular goiter (MNG) is less likely to be malignant still prevails despite recent studies that indicate an equal incidence of malignancy compared to solitary nodules (SN). Further, there remains a belief that malignancy in the setting of a MNG is less likely to metastasize. We compared the incidence of metastatic thyroid cancer among patients with MNG, SN and microcarcinomas.
A retrospective chart review of 232 patients with the diagnosis of thyroid cancer currently followed at a thyroid cancer clinic was completed. Preoperative clinical exam and imaging studies, as well as intra-operative and pathological findings were used to determine the number and sizes of thyroid nodules. Patients were divided into two groups: the solitary nodule group (SN) and the multi-nodular goiter group (MNG). A third group of microscopic or occult carcinoma includes small cancers found incidentally at pathological examination.
Of the 232 charts reviewed, 34 were excluded due to incomplete data. 7 cases were categorized micro-occult nodule. Of the remaining 191, 98 (49.5%) were in the SN group and 93 (47%) in the MNG group. The two groups had similar male to female ratios as well as the distribution of the different forms of cancer. The mean age at diagnosis of cancer of the MNG group was 9 years older than the SN group. The SN group had a greater number of local metastases than MNG (31.6% versus 18.3%), however the number of distant metastases was the same in both groups (6%). There were no instances of metastases among those with micro-carcinoma.
Cancers arising from solitary nodules may be more likely to have metastasized locally at diagnosis. However the presence of distant metastases was equal in both groups. Thyroid cancer in the setting of MNG should not be considered less serious and requires systematic follow-up similar to those with MNG.
Conditional Expression of BRAFV600E Induces Poorly Differentiated Thyroid Cancers (PDTC) and Thyroid Dishormonogenesis in Mice That Reverts with Oncogene Withdrawal
Thyroid Cancer Friday Oral Basic 1:45 PM
Advanced human thyroid cancers have high prevalence of BRAF mutations, particularly those that are radioactive iodine (RAI) therapy refractive. Further, BrafV600E downregulates expression of thyroid-specific genes, resulting in iodine uptake impairment and thyroid dishormonogenesis.
In this study, we developed an in vivo model which conditionally expresses BrafV600E in the thyroid postnatally. Transgenic mice carrying the rtTA gene driven by the thyroglobulin (Tg) promoter were generated and crossed with reporter mice carrying BrafV600E under control of a tetracycline responsive minimal promoter (tet)-BrafV600E. Thyroid-specific conditional activation of oncogenic Braf was validated by quantitative PCR analysis of BRAFV600E transgene expression and IHC for phospho-ERK in thyroids excised from bitransgenic mice.
Mice with one week doxycycline-induced overexpression of BrafV600E show PDTC, with an increased thyrocyte Ki67 proliferative index and nested clusters of pERK expression, concordant with clonal expansion of BrafV600E overexpressing cells. Doxycycline withdrawal causes histopathological tumor regression and a return to basal Ki67 and pERK levels. BrafV600E induction abolishes the expression of thyroid differentiation genes such as Tg, Nis, Tshr and Tpo. Oncogenic Braf interferes with the activity of key transcription factors required for their expression. There is a marked decrease in expression of Pax8, Ttf2 (Foxe1) and to a lesser extent that of Ttf1 (Nkx2–1). Doxycycline wash out for 2 and 7 weeks restored expression of these transcription factors to baseline levels and that of their respective target genes, resulting in reversal of hypothyroidism. BrafV600E expression does not result in downstream methylation of CpG islands within the Pax8, Nis, Tshr gene promoter regions, consistent with their expression restoration following oncogene withdrawal.
The mechanisms by which BrafV600E downregulates Pax8 and other thyroid-specific genes are under further investigation. Preliminary data suggest that these effects may not be entirely due to transcriptional repression and may be caused in part by complex competitive interactions with natural antisense transcripts.
Dept. of Experimental Medicine, University La Sapienza of Rome , II Faculty of Medicine, Rome, Italy
Thyroid Cancer Friday Oral Basic 2:00 PM
Galectin-3 (Gal-3) is an anti-apoptotic molecule, essential for thyroid cells transformation in vitro, and useful as a preoperative diagnostic marker of thyroid malignancy. Recently, we demonstrated that Gal-3 gene expression is down-regulated by wt-p53, while it is stimulated by gain-of-function p53 mutants. However, in well-differentiated thyroid carcinomas there is a contradictory concomitant expression of Gal-3 and wt-p53. HIPK2 modulates p53 phosphorylation, acetylation, and localization and is necessary for the activation of p53 transcriptional properties, including Gal-3 repression. We, therefore, asked whether the loss of HIPK-2 expression could explain this paradoxical behaviour of p53 and Gal-3.
The expression of HIPK-2 was analyzed by immunohistochemistry in a total of 62 thyroid tissues, including 5 normal thyroid samples, 26 multinodular goiter (MNG), 26 papillary thyroid carcinomas (PTC) and 5 follicular thyroid carcinomas (FTC). To analyze the possible mechanism of HIPK-2 loss of expression we performed LOH analysis at the HIPK2 gene locus (7q32-34) on laser capture microdisseceted cells from 32 PTC, 7 FTC and 22 follicular adenomas (FA). Our results were also confirmed by in vitro experiments, using the PTC-derived K1 cell line, in which a stable RNA interference (RNAi) of the HIPK2 gene expression was generated. In these cells, the effect of the loss of HIPK2 gene expression on Gal-3 expression was evaluated by western blotting.
We found high levels of HIPK-2 expression in all normal tissues and MNG analyzed. HIPK2 expression was totally absent in almost all PTC (88.5%), and it was expressed at low levels in the remaining cases (11.5%). HIPK-2 expression was also absent in 40% of FTC. We found allelic loss at the HIPK-2 gene locus in 37.5% of PTC, in 13.5% of FTC and in 17.5% of FA. Interference with the HIPK-2 gene expression in K1 cells induced an up-regulation of Gal-3 mRNA and protein levels.
Our results indicate that HIPK2 expression is lost in PTCs and that this event is responsible for the lack of p53 inhibitory effect on Galectin-3 gene expression. HIPK-2 can be considered as a new tumor suppressor gene in well-differentiated thyroid cancers.
Group I P21 Activated Kinases (PAK) Are Overexpressed in Thyroid Cancer and Regulate Thyroid Cancer Cell Migration
Thyroid Cancer Friday Oral Basic 2:15 PM
PAKs are a family of serine/threonine kinases involved in cytoskeletal signaling and epithelial-to-mesenchymal transition (EMT). We previously identified increased representation of PAK signaling and EMT in the invasive fronts of papillary thyroid cancers (PTCs). However, PAK expression and activity have not been reported in thyroid cancer. The six PAK isoforms are divided into group I (PAKs 1-3) and group II (PAKs 4-6) based on structural and functional similarities. Group I PAK activity is induced by Rac1 and cdc42, and also by thyroid cancer-related pathways including PI3K and RAS/RAF/ERK. We therefore hypothesized that PAK represents an important signaling node in thyroid cancer progression.
PAK isoform expression was examined in 6 confirmed thyroid cancer cell lines (BCPAP, KTC1, TPC1, FTC133, C643, and SW1743) by quantitative RT-PCR and Western blot (WB). Protein from 10 PTCs and 3 follicular thyroid cancers (FTCs) and adjacent normal thyroid tissue was examined for PAK 1-3 expression and Thr 423 phosphorylation as a marker of PAK activity by WB. To determine the functional role of group I PAKs in thyroid cancer cell migration, TPC1 and FTC133 cells were transfected with a pEGFP-C1 vector containing the group 1-specific p21 inhibitory domain (PID) or vector alone. Migration and proliferation were measured.
All six thyroid cancer cell lines expressed PAKs 1-3, 4 and 6 mRNA and protein. Increased levels of total group I PAK proteins were identified in 6 of 10 PTCs and all FTCs versus paired normal tissues. Five of the 6 PTCs and 2 of the 3 FTCs with PAK overexpression also had increased levels of Thr423 phosphorylated PAK. Transfection of the PID reduced migration >50% compared to vector control in TPC1 and FTC133 cells (p < 0.05), confirming that group I PAKs play a role in thyroid cancer cell migration in vitro.
Thyroid cancer cells express group I and II PAKs. Inhibition of group I PAKs reduces cell migration in vitro and group I PAKs are overexpressed and overactivated in some thyroid cancers. Further studies using isoform-specific PAK inhibitors and analysis of the invasive fronts of thyroid cancers are ongoing to further clarify the potential role of PAKs in thyroid cancer.
Stimulation of AKT Phosphorylation by TSH and TRAB in Cultured Orbital Preadipocytes from Patients with Graves' Ophthalmopathy
Thyroid Diseases Friday Oral Basic 2:30 PM
TSH receptor (TSHR)-directed autoantibodies (TRAb) and TSH activate the thyroid epithelial cell TSHR via both Gαs-cAMP/protein kinase A/ERK and Gαq-Akt/protein kinase C coupled signaling networks. Recent studies by Davies and colleagues have shown that individual TRAbs have unique molecular signatures that result in variable downstream signal responses within the thyrocyte. In order to begin to characterize TSH and TRAb-induced signaling cascades in preadipocytes from patients with Graves' ophthalmopathy (GO), we assessed the impact of TSH and M22 (a monoclonal TSHR stimulatory antibody having a high affinity for the receptor) on Akt phosphorylation in cultured GO orbital preadipocytes.
GO preadipocytes were grown to confluence,seeded on 96 well plates, and serum starved for 24 hr. Cells were then treated with TSH or M22 (0.001–10 u/L or 0.1–100 ng/ml, respectively) for 1-30 mins. The selective pAKT inhibitor LY294002 (dose 50 uM) was also added to some wells. pAKT levels was measured using an assay kit (CASETM Cellular activation of signaling ELISA assay, SABiosciences).
TSH (10 u/L) increased Akt phosphorylation at 1, 10 and 30 min (p = 0.048, 0.025 and 0.005 respectively). M-22 (5 ng/ml) enhanced p-Akt at 1, 10 and 30 min (p = 0.001, 0.002 and 0.0036, respectively). Stimulation at 5 mins was significant for neither agent. PI3-k inhibition decreased both TSH-induced stimulation at 1, 10 and 30 min (by 55%, 14.2% and 46.8%, respectively) and M22-induced stimulation at the same time points (by 73%, 20.7% and 57.7%, respectively).
Both TSH and M22 stimulate Akt phosphorylation in cultured orbital preadipocytes from patients with GO, with a bi-phasic response pattern. Whether individual TRAbs have unique molecular signatures that may explain clinical subtypes of GO or its selective development in only a subset of Graves' patients awaits further studies.
Medicine, Brigham & Women's Hospital , Boston, MA
Thyroid and Development Friday Oral Clinical 1:45 PM
Maternal thyroid hormone requirement increases approximately 30–40% during gestation. Women with known hypothyroidism must increase levothyroxine to prevent fetal harm, though how and when this should be accomplished is unclear.
We conducted a randomized, prospective, 4-year study enrolling 60 women with treated thyroid dysfunction seeking pregnancy. Once pregnant, women were randomized to proactively increase levothyroxine (LT4) by either 2 extra tablets/wk (29%; Group A), or 3 extra tablets/wk (43%; Group B) from their baseline dose. Thyroid function was tested every 2 wks through mid-pregnancy, and at 30 wks gestation. Levothyroxine was adjusted to maintain TSH between 0.5–5.0 uL/mL (0.1–5.0 uL/mL if cancer). We sought to determine which intervention would best prevent maternal hypothyroidism, while limiting hyperthyroidism.
48 women completed the protocol. Despite initial thyroid testing before 10wks gestation (mean 6.3wks), 13 women had elevated TSH values at study entry. Both interventions prevented further hypothyroidism later in pregnancy (1 of 25 patients - Group A; 1 of 23 patients - Group B). Because of TSH suppression, subsequent LT4 dose reduction was necessary in 8 of 25 (32%) women in group A, compared to 15 of 23 (65%) women in group B (p < 0.01). A higher pre-pregnancy LT4 dose predicted a greater risk for subsequent dose reduction (p = 0.03), while the gestational week of initial LT4 adjustment did not (p = 0.82). Subanalysis of Group A demonstrated that 24 of 25 subjects (95%) required LT4 testing no more frequent than once monthly; and 15 of 25 (60%) remained euthyroid through gestation with no further LT4 modification.
A 29% increase in levothyroxine (2 extra tablets weekly) initiated at confirmation of pregnancy prevents maternal hypothyroidism in 96% of subjects. 60% of subjects require no further LT4 adjustment, though 40% require subsequent dose modification, primarily predicted by higher pre-pregnancy LT4 requirements. Monthly evaluation of thyroid function is recommended through mid-pregnancy.
Management of Thyroid Disorders During Pregnancy: Does the Endocrine Society Impact Care?
Thyroid Diseases Friday Oral Clinical 2:00 PM
In 2007 the Endocrine Society released “Guidelines on the Management of Thyroid Dysfunction during Pregnancy and Postpartum”. It is not clear whether these guidelines reached their target population or influenced care.
Three waves of mail surveys were distributed to 1601 Wisconsin health care providers with a history of providing obstetric care. Survey participants were members of the American College of Obstetricians and Gynecologists or the American Association of Family Physicians. There were 881 returned surveys (55%) and 575 were eligible for the study (adjusted rate 52.5%).
Seventy-six percent of providers schedule their initial prenatal visits between 7–12 weeks gestation. For patients on levothyroxine (LT4), 70% of providers address LT4 dose at first visit while 19% address dose at time of positive home pregnancy test. A minority of physicians (13%) routinely refer patients to endocrinology for management of thyroid hormone replacement. For patients not on LT4, only 36% of providers routinely screen for thyroid disease risk factors. Presence of risk factors is used to determine TSH testing by 66% whereas 15% check TSH on all patients. Although only 11.5% of providers read the Endocrine Society's guidelines, reading the guidelines was associated with increased likelihood of pre-pregnancy counseling on LT4 management (p < 0.0001) and increased likelihood of screening for thyroid disease risk factors (p = 0.0007).
The Endocrine Society's “Guidelines on Management of Thyroid Dysfunction during Pregnancy and Postpartum” reached a minority of providers involved in obstetric care. Reading the guidelines was associated with increased patient education and thyroid disease screening.
Neuroscience and Mental Health Program, Research Institute, The Hospital for Sick Children , Toronto, Canada
Thyroid and Development Friday Oral Clinical 2:15 PM
Extensive animal research has shown that thyroid hormone (TH) is essential for normal development of the hippocampus (H) and if lacking during late gestation or early postpartum, both H malformations and learning and memory impairments are seen. Children with congenital hypothyroidism (CH) detected by newborn screening undergo a brief period of TH insufficiency comparable to when experimental rodents lacked TH. We have previously shown these children exhibit (a) memory problems suggestive of H abnormalities, (b) H atrophy, particularly in posterior H region, (c) abnormalities in H chemical constitution, (d) abnormal integrity of H circuitry, and (e) correlations between memory weaknesses and structural H abnormalities. However H functioning itself has never been directly studied in CH. This study used fMRI, a noninvasive tool to examine brain function based on hemodynamic changes within specific regions during performance of different tasks, and two memory paradigms known to activate H in normal adults.
Studied were 15 children with CH and 15 controls aged 11–14 years. Each child underwent two separate scan sessions on the same day. Following extensive pretraining, two different task paradigms were performed in a 1.5 T scanner. One task used a verbal paired associates learning paradigm (VPAL) requiring learning and remembering novel word pairs and the other task, an object-place learning paradigm (OPL) requiring recall of objects in a grid. Data were processed and analyzed using SPM5.
Preliminary findings based on 9 CH and 12 controls indicate that although groups do not differ in performance during scanning, H activation on correct recognition was more diffuse and bilateral in CH. On VPAL, CH showed increased activation in left and right posterior H relative to controls (p = .018 and .032). On OPL location trials, CH showed increased activation in left and right middle H (p = .002 and p = .007) and on OPL object-pair trials, increased activation in left middle and right posterior H (p = .013 and p = .027).
Early TH insufficiency in children with CH alters how they process aspects of associative memory in H suggesting them may use compensatory, albeit less effective, H mechanisms to support such memory functions.
Iodine Status of Pregnant Women and Role of Iodine in Hypothyroidism of Pregnant Women
Thyroid Diseases Friday Oral Clinical 2:30 PM
Iodine is an essential element for the production of thyroid hormone (TH). Iodine deficiency at critical stages during pregnancy results in impaired development of the fetus. Pregnant women are particularly vulnerable to iodine deficiency because the iodine requirement and excretion increase during pregnancy. There is supporting evidence to demonstrate the potential adverse effects of inadequate iodine intakes on thyroid function. The objective of our study was to assess the iodine status of pregnant women and to examine the correlation between iodine nutrition and thyroid function of pregnant women.
We analyzed thyroid function and thyroid antibodies in 310 pregnant women during their first antenatal visit by the Immuno-chemiluminesence assay (ICMA) and used trimester-specific reference ranges for the assessment of thyroid dysfunction and autoimmune disorders in pregnancy. Each woman provided a spot urine sample for determination of urinary iodine concentration (UIC), which was an indicator of iodine status, by As3+-Ce4+ catalytic spectrophotometry.
The median UIC (MUI) for 310 pregnant women was 134 ug/L, 14.2% of whom had a UIC <50 ug/L. Pregnant women with UIC <50 ug/L were found to have a significantly higher prevalence of hypothyroidism (overt and subclinical) than those with UIC ≥150 ug/L (P < 0.0001), pregnant women with UIC ranging 50–149 ug/L were more likely to develop hypothyroidism than those with UIC ≥150 ug/L (P = 0.0013). No significant difference was detected between pregnant women with UIC ≥500 ug/L and those with UIC ranging 150–249 ug/L (P > 0.05). The P 5 and P 95 of UIC of these 310 pregnant women were 24.2 and 428.5 ug/L, respectively. Pregnant women with UIC ≥428.5 ug/L were found to have a significantly higher prevalence of hypothyroidism than those with UIC ranging 24.2–428.5 ug/L (P = 0.0007).
Pregnant women in our study were mildly iodine deficient. Inadequate iodine intake played a prominent role in hypothyroidism of pregnant women, highlighting the need for ongoing surveillance of iodine status of pregnant women.
Endocrinology and Metabolism, Academic Medical Center , Amsterdam, Netherlands
Thyroid Hormone Metabolism and Regulation Friday Oral Basic 4:30 PM
Acute illness in mice profoundly affects central thyroid hormone metabolism. We have recently shown a prominent role for the TRβ gene in the observed alterations. The thyroid hormone receptor α (TRα) is predominantly expressed in brain. It is unknown at present whether the TRα, like the TRβ, plays an important role in altered central thyroid hormone metabolism during acute illness. The aim of our study therefore is to evaluate the role of TRα in central thyroid hormone metabolism during acute illness by administration of a sub-lethal dose of bacterial endotoxin (LPS) to TRα0/0 and Wild Type (WT, 129/Sv) mice.
Mice were killed at 4, 8 and 24h after LPS; D2 and D3 mRNA expression was measured in the hypothalamic periventricular area (PE) and in the arcuate nucleus region (ARC). TSHβ, D1 and D2 mRNA expression was measured in the pituitary. Liver interleukin (IL)-1β mRNA was measured as a reflection of the inflammatory response.
The inflammatory response, indicated by increased liver IL-1β mRNA expression, was similar in WT and TRα0/0 mice. LPS increased D2 mRNA expression in the PE and ARC to a similar extent in TRα0/0 and WT mice. D3 mRNA decreased upon LPS administration in the PE which was also not different in both strains. D3 expression in the ARC region did not decrease in TRα0/0 mice and was significantly lower at 4h after LPS administration in WT compared to saline and LPS-treated TRα0/0 mice. Pituitary TSHβ and D1 mRNA expression decreased significantly after LPS in both genotypes, but the decrease of both mRNAs was more pronounced in TRα0/0 mice. Pituitary D2 mRNA increased shortly after LPS in TRα0/0 and WT but no difference was observed between genotypes.
The TRα gene is not involved in illness-induced alterations in hypothalamic and pituitary D2 mRNA expression. However, lacking the TRα gene intensifies the LPS-induced decrease of pituitary TSHβ and D1 mRNA despite a similar inflammatory response in TRα0/0 and WT mice. Our results implicate a possible role for TRα in selective LPS-induced alterations in pituitary thyroid hormone metabolism.
Endocrinology, Erasmus University Medical Center , Rotterdam, The Netherlands
Thyroid Hormone Metabolism and Regulation Friday Oral Basic 4:45 PM
Large variations in thyroid hormone (TH) concentrations exist between individuals. Approximately 65% of this variation is due to genetic factors. However, the causative genes and variants are largely unknown. We therefore performed a large scale association analysis of 68 TH pathway genes with TSH and FT4 levels.
68 genes with a role in TH synthesis, transport and metabolism were selected. Single nucleotide polymorphisms (SNPs) in these genes plus 10 kb flanking regions were selected from the Illumina HumanHap 550K SNP array (n = 1372 SNPs). Association analyses for these SNPs with TSH and FT4 were performed in a Dutch cohort of 1121 men and women (age: 69.0 ± 7.6 yrs). Suggestive SNPs (p < 0.01) were genotyped in an independent cohort of 700 Danish twins (age: 36.0 ± 10.6 yrs) for confirmation. All subjects were euthyroid with negative TPO antibodies. Analyses were adjusted for age and gender.
In the initial cohort, 32 SNPs in 11 genes were associated with TSH and 16 SNPs in 7 genes with FT4 (p < 0.01). Associations were replicated for SNPs in DIO1 (deiodinase), PDE8B (phosphodiesterase) and SLC16A10 (TH transporter). (see table).
Results replicated in Danish twin cohort.
We performed an association analysis of 68 TH pathway genes with serum TSH and FT4 levels in a large cohort. Genetic variation in 14 genes was associated with serum TSH and/or FT4 levels. Results could be replicated in an independent sample for DIO1, PDE8B and SLC16A10. Population characteristics (e.g. sample size, iodine status, age) might explain the absence of replication of the other associations. Therefore, additional cohorts will be studied and meta-analyzed for confirmation. These findings identify at least three causative genes and provide insight into the molecular basis of inter-individual variation in serum TH levels.
Thyroid Hormone Action Friday Oral Basic 5:00 PM
The osteoporotic-like characteristics observed within the bones of the TSH receptor knockout mice (TSHR-/-) revealed that thyroid stimulating hormone (TSH) has an important modulatory role(s) in bone remodeling and that both osteoclasts and osteoblasts express the TSHR. We have recently reported that TSH inhibits the differentiation of osteoclasts from mouse embryonic stem (ES) cells and we have now proceeded to determine the influence of TSH on osteoblast differentiation.
We first established a murine ES cell model for osteoblastogenesis by inducing osteoblast differentiation from ES cells using β-glycerolphosphate, ascorbic acid and dexamethazone and vitamin D3.
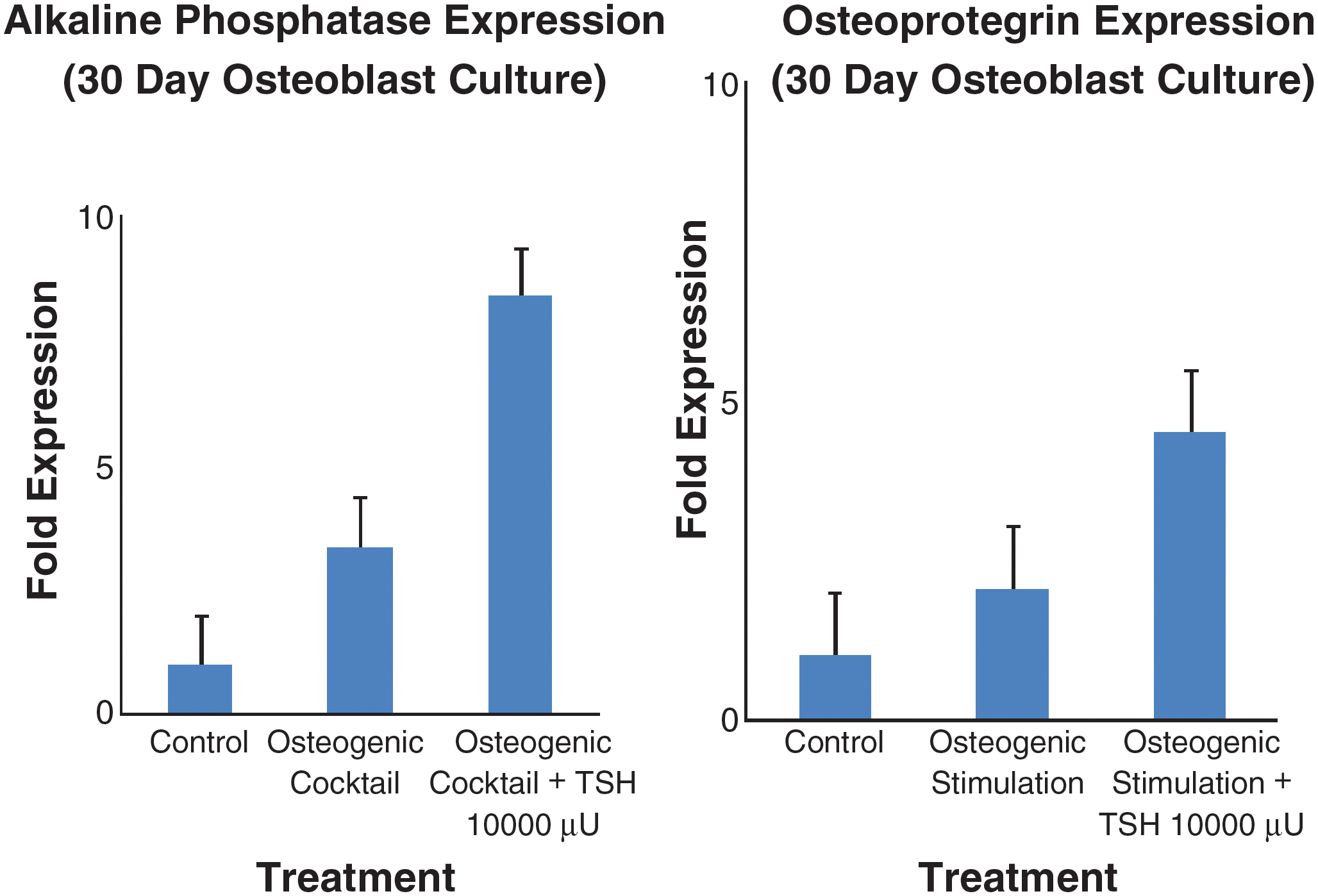
At day 30 differentiation of ES cells into osteoblasts was confirmed by Alzarin Red and von Kassa staining and these data indicated that a high proportion (∼40%) of mineralized cells suggesting osteoblastogenesis. Further confirmation of osteoblast differentiation was obtained by a decrease in stem cell markers (such as Rex1) and an increase in osteoblast markers including alkaline phosphatase (ALP), osteocalcin, osteopontin and osteoprotegrin (OPG)(See Figure). TSH initiated non-canonical wnt signaling as evidenced by >3-fold increase in wnt5a and frizzled receptor gene expression. TSH signaling (10 mU/ml) significantly enhanced mineralization in these cell cultures and qPCR analysis of the TSH treated cells further indicated a transcriptional enhancement of OPG. OPG, a major soluble decoy receptor for RANK Ligand is a major stimulator of osteoclastogenesis. These data suggested that TSH may negatively regulate osteoclast formation through an increase in osteoblast derived OPG.
Our results support the hypothesis that ES derived osteoblasts are an effective model system to study the mechanism of TSH action on bone cell differentiation. Furthermore, these data suggest a novel mechanism of osteoclast regulation by TSH via modulation of OPG expression.
Laboratory of Comparative Endocrinology, K.U.Leuven , Leuven, Belgium
Thyroid and Development Friday Oral Basic 5:15 PM
Thyroid hormones (THs) play a central role in brain development. While experimental proof for their regulatory actions in late brain development continues to increase, experimental data for early brain development remain scarce. We used the chick embryo as a model to study the possible involvement of maternal THs in brain development during the first half of incubation (total duration 21 days).
We first measured the normal expression profile of TH-transporters OATP1c1 and MCT8, TH-deiodinases D1-D3, and TH-receptors TRα and TRβ in telen-, dien-, mesen- and rhombencephalon from 4- up to 12-day-old embryos (E4-E12). Subsequently we induced either hypothyroidism by treating laying hens with 0.05% methimazole or hyperthyroidism by injecting 0.5 μg T3+1 μg T4 into the egg yolk.
During early development OATP1c1 mRNA was mainly present in telen- and diencephalon and levels strongly decreased from E4 towards E12. mRNA levels of MCT8, D2, TRα, and TRβ varied between different brain regions but all expression profiles showed a gradual increase. D3 expression decreased from E4 to E12 while D1 expression showed no clear trend. The presence of active D2 and D3 protein was shown by in vitro deiodination tests while in vivo TH uptake in brain indicated the presence of active TH transporters. Microarray analysis of control and hypothyroid E4 and E8 telencephalon samples showed differential expression of a number of genes, including the homeobox genes Gbx2 and Six3, transcription factors involved in the organization of early brain. qRT-PCR confirmed increased expression of Gbx2 in telen-, dien- and rhombencephalon of hypothyroid E4 but not E8. Six3 expression was increased in hypothyroid E4 and E8 but only in diencephalon. Analysis of hyperthyroid telencephalon again showed increased expression of Gbx2 in E4 but not E8. This was accompanied by increased TRα, TRβ and D3 expression as well as decreased OATP1c1 expression in hyperthyroid E4.
Our results show that the early brain expresses the proteins needed for intracellular TH-uptake, -metabolism and -action in a region- and stage-specific way. They also show that both shortage and excess of THs change the expression of at least some genes involved in early brain organization.
Impact of Post-Surgical Diagnostic 131-I Planar and SPECT-CT Imaging on Staging and Management of Differentiated Thyroid Carcinoma
Thyroid Cancer Friday Oral Clinical 4:30 PM
The aim of this study was to assess the impact of post-surgical diagnostic 131-I scintigraphy, including the incremental value of single photon emission computed tomography (SPECT-CT) over planar imaging, on staging of differentiated thyroid carcinoma (DTC) and on selection of first 131-I therapy activity.
Forty-eight patients (36F:12M, mean age 46.6 y, range 17–83 y) with DTC underwent diagnostic 131-I (planar and SPECT-CT) scintigraphy. Two readers interpreted the studies as showing remnant thyroid tissue, regional metastatic disease, distant metastases, or as equivocal, using planar imaging alone, then with both planar and SPECT-CT information. Patients were staged using the TNM system with three levels of sequential information: 1) histopathology and chest radiograph data (pTNM/CXR), 2) data from 131-I planar scan, and 3) addition of 131-I SPECT-CT data; restaging was based on imaging findings (iTNM). The impact of changes in final staging and on selection of initial 131-I therapeutic activity was examined, including the contribution of SPECT-CT over planar imaging.
Planar images detected unsuspected distant metastases in 4/8 (50%) patients with final M1 score. SPECT-CT changed the planar scan interpretation in 19/48 (40%) of cases, detecting regional nodal metastases in 4 patients, and clarifying equivocal diagnoses on planar imaging in 15 patients by characterization of focal neck activity as remnant thyroid tissue or regional nodal disease. Compared to pTNM/CXR, diagnostic 131-I scintigraphy (planar and SPECT-CT) changed post-surgical DTC stage in 10/48 (21%) patients. Information likely to change the selection of 131-I therapeutic activity was found in 28/48 (58%) patients.
131-I scan in a 49 year-old woman with DTC. Planar (a) and SPECT-CT depict thyroglossal duct (b) and left thyroid bed (c) remnants, cervical nodal (d) and lung metastases (e; f); T4N1M1, stage IV.

Diagnostic 131-I scintigraphy using planar and SPECT-CT imaging provides a more complete post-surgical staging of DTC. SPECT-CT reduces the number of equivocal diagnoses on planar imaging and improves interpretation of the diagnostic 131-I studies. The added scores and staging may influence the selection of first 131-I therapy activity.
Department of Investigational Cancer Therapeutics, [Phase I Clinical Trials Program], Division of Cancer Medicine, MD Anderson Cancer Center , Houston, TX
Thyroid Cancer Friday Oral Clinical 4:45 PM
XL184 is an oral inhibitor of MET, VEGFR2 and RET and exhibits anti-tumor and anti-angiogenic activity in xenograft tumor models.
Adults with advanced malignancies received XL184 in a 3 + 3 study design. Primary objectives include evaluation of safety and pharmacokinetic (PK) parameters and maximum tolerated dose (MTD) determination. RECIST response was assessed on day 28 and every 8 weeks. Pharmacodynamic and tumor markers, and RET mutational status are being analyzed. Adverse events (AEs) for 83 pts and PK results as of the 3/2009 data transfer are reported. Pharmacodynamic data and efficacy are reported for the 37-pt MTC subgroup.
85 pts were enrolled. XL184-related AEs were primarily Grade 1/2. Grade 3 related-AEs in ≥2 pts included palmar-plantar erythrodysesthesia (PPE, 11%); fatigue (10%); diarrhea (5%); increased AST, ALT, lipase and decreased weight (4% each); and hypertension and increased amylase (2% each). There were 2 related Grade 4 AEs; pulmonary embolism and increased lipase. The MTD of 175mg QD was based on DLTs of PPE, mucositis, and increased AST, ALT and lipase. The terminal half life is ∼100 hrs. Changes in PlGF, VEGF-A, sVEGFR2 and EPO were statistically significant and consistent with anti-angiogenic effects. Statistically significant increases in sMET occurred indicating MET pathway inhibition. Inhibition of XL184 targets and downstream signaling pathways was observed in skin samples. Of the MTC pts with measurable disease, 14 of 34 (41%) had ≥30% reduction in tumor measurements, with 9 of 34 (26%) achieving confirmed PR (cPR). The median time to response and preliminary duration of response for pts with a cPR were 28 days and 6.7 months respectively. The disease control rate (PR+SD >3 months) was 84%. Most MTC pts had reductions in plasma calcitonin and CEA. Response in MTC pts appears to be independent of RET mutational status.
XL184 is generally well tolerated; the MTD is defined. In MTC pts with measurable disease, 41% had ≥30% reduction in tumor measurements and of these, 26% achieved a cPR. The majority of MTC pts derived clinical benefit. A global phase 3 pivotal study of XL184 in MTC is ongoing.
Endocrinology, Mayo Clinic , Rochester, MN
Thyroid Cancer Friday Oral Clinical 5:00 PM
Neither the evidence base for the 2006 ATA Thyroid Cancer Guidelines nor a more recently published report (Thyroid 17: 1225–8, 2007) provided convincing data regarding a role for RRA in improving postoperative outcome in PTC patients with AJCC T1 tumors, especially those with diameters of 11 to 20 mm. If a prospective trial was to be designed to answer this question, it would likely involve “low-risk” (eg with MACIS scores <6) patients aged 21 yr or older, with surgically curable T1 disease (ie neither T4 nor M1) completely resected by initial bilateral lobar resection (BLR).
In this retrospective study, our aim was to define outcome in such a cohort of 765 adult patients with MACIS <6 AJCC T1 PTC treated during the 35 yr after the introduction of RRA to our institution, and before the current era of ultrasound-guided nodal biopsies, rhTSH-stimulated Tg testing and central compartment dissection. The 765 patients (545F; 220 M) underwent BLR during 1950–1985 for tumors that were completely resected and neither locally invasive or distant spread.
Median patient age was 45 yr (range 21–72), mean tumor size 12 mm (49% <11 mm); 24% were multicentric and 30% node-positive. Mean follow-up was 27 yr (longest 55); 23% for >35 yr. 170 (22%) received RRA. 35-yr occurrence rates for cause-specific mortality (CSM), local recurrence (LR), regional nodal metastases (RNM) and distant metastases (DM) were 1.1, 2.2, 5.0 and 1.6%, respectively. Comparable 35-yr rates for Group A, (n = 375 tumors <11 mm), were 0.6, 1.8, 4.5, and 0.5%. For Group B, (n = 390 tumors of 11–20 mm), rates were higher at 1.6, 4.3, 5.5, and 2.6%, respectively. RRA's impact was assessed by comparing survival to 4 endpoints in patients undergoing BLR alone versus those receiving BLR+RRA within 18 mos.The 35-yr CSM rates in Groups A and B were after BLR 0.6 and 1.6%, and after BLR+RRA insignificantly different (p > 0.75). Similarly, survival rates to LR, RNM and DM were no different in ablated patients than after BLR alone in both Groups A (p > 0.07) and B (p > 0.33).
These results confirmed the excellent prognosis of AJCC T1 tumors treated by BLR, and did not identify a significant reduction in mortality or recurrence rates in patients with T1 PTC tumors selected for RRA.
Medicine, Endocrine Division, Mount Sinai Hospital and University of Toronto Medical School , Toronto, Canada
Thyroid Cancer Friday Oral Clinical 5:15 PM
We have previously reported on the application of a post-surgical, TSH-stimulated serum thyroglobulin (S-Tg), as a method for radioactive remnant ablation (RRA) selection in low-risk well-differentiated thyroid carcinoma (WDTC) (79th ATA Meeting, Abstract #79). Herein, we report on the serial S-Tg measurements of those low-risk WDTC patients who did not receive RRA.
Forty low-risk WDTC patients were followed after total thyroidectomy and an initial S-Tg ≤5 μg/L, without RRA. Low-risk was defined as tumors with papillary histology confined to the thyroid gland and without multi-level local lymph node involvement. All patients had negative anti-Tg antibodies by two independent assays. Patients underwent repeat S-Tg measurements, neck ultrasound and additional imaging when indicated. The mean follow-up interval was 3.4 years (range = 1.3 to 12.0 years).
All patients had an undetectable serum Tg on thyroid hormone suppression therapy for the duration of the follow-up period. Among the 40 patients, 23 patients (57.5%) had an undetectable S-Tg (<1 μg/L) after total thyroidectomy. Within this subgroup, all patients (100%) had subsequent S-Tg values ≤1 μg/L with no significant imaging abnormalities. The remaining 17 patients (42.5%) had a post-surgical S-Tg of 1–5 μg/L. Within this subgroup, 7 (41.2%) had repeat S-Tg values that declined, 3 (17.6%) had repeat S-Tg values that increased, but did not exceed 4 μg/L, and the remaining 7 (41.2%) had no change in their repeat S-Tg value. None of these 17 patients showed significant imaging abnormalities on follow-up routine ultrasound studies or selected CT scans when indicated.
To date, follow-up of low-risk WDTC patients who did not receive RRA by serial S-Tg measurements has revealed that (1) patients with a post-surgical S-Tg value of <1 μg/L have no evidence of residual/recurrent thyroid carcinoma, and (2) patients with a post-surgical S-Tg value of 1–5 μg/L have not had significant changes in their follow-up S-Tg and imaging studies to justify RRA intervention. (3) These observations add support to our previously proposed RRA selection guidelines in low-risk WDTC based on an initial post-surgical S-Tg value.
Saturday, September 26, 2009
School of Clinical and Experimental Medicine, University of Birmingham , Edgbaston, Birmingham, United Kingdom
Autoimmunity Saturday Poster Basic
Recent genome-wide association studies in Graves' disease (GD) are beginning to reveal a number of novel genetic variants. The Wellcome Trust Case Control Consortium (WTCCC) in the UK recently investigated 900 GD cases and 1500 controls, using a genome-wide set of 14,500 nonsynonymous coding single nucleotide polymorphisms (nsSNPs). Whilst the strongest association signal was unsurprisingly identified in the HLA region (P value <10−20), association was also confirmed at the previously reported thyroid stimulating hormone receptor and Fc receptor-like 3 genes, along with the identification of nine novel possible regions of association (P > 10−4).
The aim of this study was to try to confirm association of these nine novel regions in an extended cohort of 2478 GD cases and 3446 British Caucasian controls (including the original 900 cases and 1500 controls).
Weak association of nsSNPs in JSRP1, TEKT1 and HDLBP (P < 10−3) was determined in the extended cohort. To determine if these weak associations were in linkage disequilibrium with larger effects elsewhere in these genes, 24 Tag SNPs were employed to screen these three genes, with Tag SNPs in HDLBP and TEKT1 providing further weak evidence of association (P < 10−3). Association was not seen between GD and any of the other nsSNPs or Tag SNPs studied.
This study was unable to replicate six of the novel WTCCC associations in an enlarged GD dataset, suggesting these results were likely to be false positives within the original dataset. Weak association signals remain between GD and the JSRP1, TEKT1 and HDLBP nsSNPs in a large extended UK Caucasian cohort, suggesting that although a small effect can not be ruled out at these regions, as these regions did not reach genome wide significant (P < 10−7) replication in further adequately powered datasets is essential before determining if these nsSNPs truly represent novel susceptibility loci.
Endocrinology, Shandong Provincial Hospital Affiliated to Shandong University , Jinan, China
Autoimmunity Saturday Poster Basic
Killer cell immunoglobulin-like receptor (KIR) can modulate the activity of NK and T lymphocyte. To investigate whether the KIR genotype possessing a susceptibility to Graves' disease (GD).
Using PCR-SSP to detect KIR genotype in 96 GD patients and 96 randomly selected healthy controls.
The genotype frequency of 2DS2-,2DL2-, 2DL3+, 2DL1+, 3DL1+, 3DS1-, 2DL5-, 2DS3-, 2DS5-, 2DS1-, 2DS4- was significantly higher in the patient group compared to that of the control group (6.25% vs 0%, P < 0.05). Genotype of 2DS2-, 2DL2-, 2DL3+, 2DL1+, 3DLl+, 3DS1-, 2DL5-, 2DS3-, 2DS5-, 2DS1-, 2DS4+ is the most prevalent in the controls (28.13% vs 10.42%, P < 0.01). Genotypes without activating KIR genes have higher frequency in patient group.
The difference of KIR genotypes between GD patients and healthy controls may explain the pathogenesis of GD.
Department of Biomedical Informatics, Division of Health Sciences, Osaka University Graduate School of Medicine , Suita, Japan
Autoimmunity Saturday Poster Clinical
Interleukin (IL)-1β is a proinflammatory cytokine and has been implicated in the pathogenesis of several autoimmune diseases. IL-1β also has an important role for differentiation and proliferation of IL-17-producing helper T cells (Th17 cells) in human, which increases in patients with autoimmune thyroid diseases (AITD), especially in patients with intractable Graves' disease (GD). The region containing the −31T allele of functional −31C/T polymorphism (rs1143627) in the gene encoding IL-1β is the TATA box, and the change from −31T to −31C in this polymorphism causes potential disruption and decrease in expression of the IL-1β protein.
To evaluate the hypothesis that −31C/T functional polymorphism in IL1B gene is associated with the intractability and the severity of AITD, we genotyped this polymorphism in 64 GD patients who had been treated with methimazole or propylthiouracil for at least 5 years and remained positive for TRAb (intractable GD), 28 GD patients who had maintained a euthyroid state and had been negative for TRAb for more than 2 years without medication (GD in remission), 49 patients with Hashimoto's disease (HD) who developed hypothyroidism before 50 years of age, and were treated daily with thyroxine (severe HD), 28 untreated, euthyroid HD patients who were over 50 years of age (mild HD), and 59 healthy volunteers who were euthyroid and negative for thyroid autoantibodies. We also analyzed the proportion of peripheral Th17 cells in these patients by flow cytometry.
The −31T allele, which is related to high producibility of IL-1β, was significantly more frequent in patients with intractable GD than in those with GD in remission (p = 0.0017; odds ratio, 2.8; 95% confidence interval, 1.5−5.3), although there was no difference in this frequency between the 2 groups of HD patients. Furthermore, the proportion of Th17 cells, whose differentiation and proliferation are promoted by IL-1β, was higher in AITD patients with the T allele than in those with CC genotypes (p < 0.05).
Our data indicated that T allele of −31C/T polymorphism in the IL1B gene was involved in the intractability of GD, and this involvement could arise through the differentiation and proliferation of Th17 cells.
Department of Internal Medicine, Azienda USL Modena , Carpi (MO), Italy
Autoimmunity Saturday Poster Clinical
A higher prevalence of autoimmune chronic thyroiditis (ACT) has been demonstrated in pts with benign paroxysmal positional vertigo (BPPV) than in control subjects. The aim of the present study is to evaluate BPPV prevalence in pts with ACT and in controls.
100 consecutive ACT pts and 100 age- and sex-matched blood donors were recruited in the study. All pts underwent: written questionnaire on vertigo's signs/symptoms; measurement of serum TSH (n.v.: 0.3–4 mcIU/ml), free-T4 (FT4; n.v: 0.8–1.8 pg/ml) and Thyroglobulin (TG-Ab; n.v.: <100 UI/l) and Thyroperoxidase (TPO-Ab; n.v.: <40 IU/l) antibody concentrations; thyroid ultrasound (US). The diagnosis of BPPV was confirmed by Dix-Hallpike manoeuvre in pts with signs/symptoms peculiar to BPPV, as gathered from the questionnaire.
In ACT group, 81 (81%) pts were female and 19 (19%) male, aged 49 ± 6 yrs. Mean serum TSH and FT4 concentrations were 18.2 ± 8.9 mcIU/ml and 0.8 ± 0.3 pg/ml, respectively. Thirty-one (31%) ACT pts had overt hypothyroidism, 38 (38%) subclinical hypothyroidism, 31 (31%) were euthyroid. Mean serum TG-Ab and TPO-Ab levels were 344 ± 116 IU/l and 677 ± 210 IU/l, respectively. All ACT pts had a diffusely hypoechoic thyroid. In the control group (81 females and 19 males aged 48 ± 6 yrs), TSH and FT4 were 2.0 ± 0.5 mcIU/ml and 1.3 ± 0.3 pg/ml, respectively (P < 0.001 and <0.01 vs ACT group, respectively). Mean serum TG-Ab e TPO-Ab levels were 104 ± 5 IU/l and 43 ± 3 IU/l, respectively (P < 0.001 for both vs ACT group). Two pts had subclinical hypothyroidism and 1 Graves disease; high serum TG-Ab and TPO-Ab titres and a diffusely hypoechoic thyroid were detected in all these 3 pts. BPPV was diagnosed in 18 (18%) ACT pts - 13 females and 5 males, aged >40 yrs - and in 1 (1%) 47-yr old control subject, who was hypothyroid and showed high serum TG-Ab e TPO-Ab values.
ACT pts demonstrate a significantly higher BPPV prevalence than controls, strengthening the hypothesis that BPPV and ACT share a common immune-mediated origin.
Surgery, Tulane University , New Orleans, LA
Cell Biology Saturday Poster Basic
Molecular basis of thyroid carcinogenesis is recently expanded, however, CD146 role and its downstream targets have not been yet understood. CD146 is well known to promote certain cancers progression and proved to validate novel target genes. The aim of the current study is to understand the molecular mechanisms and the role of the CD146 and its downstream target tissue carboxypeptidase inhibitor, Latexin (LXN), in the process of invasion and metastasis of thyroid cancer.
We used human papillary, follicular and anaplastic thyroid cancer cell lines; in addition to melanoma SkMel-28, prostate cancer PC3 and vascular endothelial cell lines. Western blot, CD146 transfection, migration/invasion assay, siRNA knockdown were used to investigate the role of CD146 and LXN in thyroid cancer.
CD146 expression increased in SkMel-28, PC3 and endothelial cells. However, the expression of CD146 was significantly suppressed in all human thyroid cancer cell lines. In contrast, induction of CD146 expression in NPA and DRO cells, downstream target LXN expression also increased. CD146 expression additionally significantly suppressed the migration and invasion capacities of thyroid cancer cells. Knockdown of CD146 by siRNA in NPA cells returned the migration and invasion potential to the level of non-transfected cells.
CD146 and its downstream target LXN act as tumor suppressor gene in thyroid cancer and may play an important role in the progression of thyroid cancer. These highly significant findings may lead to validate novel target genes as a marker for thyroid cancer and may be used in therapeutic applications.
School of Clinical and Experimental Medicine, University of Birmingham , Birmingham, United Kingdom
Iodine Uptake and Metabolism Saturday Poster Basic
The BRAF serine-threonine kinase is a component of the MAPK signaling pathway. The constitutively activating BRAF V600E mutation is found in approximately 45% of papillary thyroid cancers (PTC). This mutation has been associated with a reduction in iodide uptake, thought to be attributable to impaired expression and trafficking of the sodium iodide symporter (NIS). Pituitary tumor transforming gene (PTTG) and PTTG binding factor (PBF) are proto-oncogenes over-expressed in thyroid tumors. We have shown previously that, like BRAF V600E, PTTG and PBF reduce NIS expression and iodide uptake in thyroid cells.
We hypothesized that constitutively activated BRAF and high levels of PTTG and/or PBF may act either synergistically or in sequence to reduce iodide uptake in PTC. Gene expression analysis was performed in a series of PTC.
NIS mRNA expression was reduced by 36.6% in cancers with the BRAF V600E mutation (n = 22) compared with wild-type (WT) BRAF (n = 23), although this result was not statistically significant. No significant difference was detected in either PTTG or PBF mRNA expression. PTTG has been shown to upregulate FGF-2 and VEGF expression. A significant 1.8-fold increase in FGF-2 mRNA expression was detected in V600E cancers compared with BRAF WT (p = 0.04). VEGF mRNA expression was found to be significantly lower in the V600E cancers compared with BRAF WT (56% reduction, p = 0.001). Interestingly, FGF-2 expression was significantly correlated with PBF (rs = 0.742, p < 0.001) and PTTG (rs = 0.514, p = 0.012) expression in BRAF WT tumors but not in V600E cancers. Conversely, associations between VEGF expression and NIS, PTTG and PBF expression, and between PBF expression and NIS and PTTG expression, either became significant or increased in significance in the presence of the V600E mutation. This may indicate that the regulation of these gene interactions is altered by the constitutive activation of BRAF. Evaluation of clinical data identified a significant positive correlation between FGF-2 mRNA expression and patient age in V600E tumors (rs = 0.563, p = 0.007) not present in BRAF WT tumors (rs = 0.106, p = 0.627).
Further study is now required to determine whether PTTG and PBF function are altered in BRAF WT vs. V600E PTC.
Division of Otolaryngology Head and Neck Surgery, The George Washington University , Washington, DC
Iodine Uptake and Metabolism Saturday Poster Clinical
The incidence of hypothyrodism in head and neck surgical patients following total laryngectomy varies in the surgical literature. We present the interesting case of a head and neck cancer patient following who became profoundly hypothyroid while being treated for a wound dehiscence with povidone-iodine solution soaked gauze packing. To our knowledge, this is the first reported case of iatrogenic hypothyroidism in a surgical patient caused by supraphysiologic iodine levels.
The retrospective review of one patient's case, followed by a discussion of the literature.
A patient who underwent total layrngopharyngectomy developed a midline wound dehiscence with a superimposed infection on post-operative day 5. The wound was cultured, and treatment with antibiotics and povidone-iodine soaked gauze packing twice daily was begun. On post-operative day 12, the patient began complaining of profound depression and lethargy. A TSH level was obtained, and was noted to be 35 mIU/L. The pre-operative TSH level was within normal limits. The patient was immediately started on 75 mcg of parenteral levothyroxine. He subsequently went on to develop hypothyroidism induced renal-failure. After approximately 5 days of parenteral levothyroxine treatment, the patient's renal failure began to improve, and the patient began to show symptomatic improvement. Once stable, the patient was transitioned to oral levothyroxine, and discharged from the hospital.
The Wolff-Chaikoff effect is well documented for hyperthyroid patients who are treated with iodine for thyroid suppression. To our knowledge, this is the first reported case of surgically induced hypothyroidism after treatment of a wound dehiscence and infection with povidone-iodine packing. We advise caution when using povidone-iodine packing to treat wound related complications in surgical patients, and suggest that alternative materials be used for treatment when possible.
Effects of Effects of Acute and Chronic Maternal Deprivation on HPA Axis in Rats Pups with Hyperthyroidal Mothers
Thyroid and Development Saturday Poster Basic
Hyperthyroidism is common endocrine problem encountered in human pregnancy. It is well known that hyperthyroidism induces an increase in the activity of hypothalamic- pituitary - adrenal (HPA) axis. Between age 4 and 14 day the HPA axis of the rat displays a relative stress hyporesponsive period (SHRP). This study was designed to investigate the effects of acute and chronic maternal deprivation on their pups thyroid function and HPA axis function of Hyperthyroidal mothers and the influence of treatment administration to hypothyroidal mothers from conception to the end of experiment.
30 adult female were used after induction of pregnancy and hyperthyroidism. Maternal deprivation for 24 hours was done at two different ages during postnatal development at mid and outside the SHRP. Also, repeated maternal deprivation was done in another group. Now, pups groups are: Control group, deprived pups with hyperthyroid mother, deprived pups with treated hyperthyroid mother, nondeprived pups with hyperthyroid mother, nondeprived treated hyperthyroid mother.
The plasma thyroxin (T4) levels of treated deprived groups were significantly lower than non treated groups, while, plasma thyroid stimulating hormone (TSH) levels of treated groups were significantly higher than non treated deprived groups. There is no significant difference in plasma T4 between control and treated nondeprived group. There is no significant difference in plasma corticosterone and adreno-corticotropin hormone (ACTH) in treated deprived in comparison to treated nondeprived at pnd 9 and with repeated maternal deprivation. With repeated deprivation plasma corticosterone levels were insignificantly increased in nontreated deprived group in comparison with nontreated nondeprived group.
Maternal deprivation in rats with hyperthyroidal mother depended on the age of pups at which procedure is applied.
ENDOCRINOLOGY, PGIMER , Chandigarh, India
Thyroid and Development Saturday Poster Clinical
The current study is aimed to survey the prevalence of goiter in the post iodization phase and the relationship of goiter with various micronutrient status and thyroid autoimmunity in school children of Chandigarh, an union territory of India.
Two phase study; the first phase is a cross sectional to find out goiter prevalence and the second phase is a case-control study of children with goiter and similar age and sex matched controls. In the first phase, 10,150 children in the age group of 6–16 years from seven schools of Chandigarh were randomized. 2148 children were screened for goiter by two independent observers as per the WHO grading system. In the second phase, 191 children with goiter and 165 children without goiter were compared. Urinary iodine, iodine content of salt, serum levels of T3, T4, TSH, hemoglobin, ferritin, selenium, and anti TPO antibody titer in children included in the case control study were measured.
The prevalence of goiter in the study population was 15.13%. It was more prevalent in girls than in boys (17.2% vs 13.8%, p = 0.02) and this sex difference was more marked in higher age group children (13–16 yrs, p = 0.01). The median urinary iodine excretion in both the groups were sufficient and comparable (137 vs 130 μg/L, p = 0.74). 31.2% children with goiter and 13.04% without goiter had subclinical hypothyroidism (p = 0.01) and 4.9% children in the goiter group and 1.9% of the control group were anti TPO antibody positive (≥34 IU/ml) (p = 0.22). The median serum selenium value were not different in the goiter and control group (181.93 ± 97.97 μg/L vs 193.5 μg/L, p = 0.45). More than half of the goitrous children had anemia (hemoglobin < 12 gm/dl) as compared to control group (52.75% vs 42.03%, p = 0.049) and goitrous children were severely depleted of tissue iron stores (serum ferritin < 12 μg/L) as compared to controls (18.8% vs 10.3%, p = 0.02). On multiple regression analysis, only serum ferritin was negatively correlated with goiter (correlation coefficient = − 0.160, p = 0.008).
Iron deficiency state per se might be playing a role in high prevalence of goiter in this iodine replete population, which needs to be further explored.
P53 Stabilization in a Transgenic Mouse Model of Human PTTG Binding Factor (PBF) Over-Expression
Thyroid Cancer Saturday Poster Basic
Differentiated thyroid cancer is the most common endocrine neoplasm and its incidence is increasing. PTTG Binding Factor (PBF) is a poorly characterised transforming gene that is over-expressed in well-differentiated thyroid tumors. Preliminary experiments by our group using GST pull-down assays have demonstrated specific binding between PBF and p53, tumor suppressor protein, in vitro. However the functional consequence of this is unknown.
We generated a murine transgenic model of targeted over-expression of PBF in the thyroid. Transgenic mice were generated by pronuclear injection of a HA-tagged PBF transgene driven by the bovine thyroglobulin promoter, and founders identified by PCR. Thyroids were harvested from sex-matched wild-type and PBF transgenic mice at 4 weeks of age.
Western blot analysis confirmed elevated levels of PBF in transgenic thyroids compared to wild-type FVB/N mice, with no significant expression in other tissues. p53 protein expression was significantly increased in transgenic thyroids compared to wild-type (3.7 ± 0.9 fold; p = 0.005; n = 4; scanning densitometry corrected for β-actin expression). Further, there was a significant accumulation of the 53kDa splice variant of mdm2, a critical negative regulator of p53, in transgenic thyroids compared to wild-type (1.53 ± 0.14 fold; p = 0.02; n = 8). Real-time PCR did not reveal any significant change in p53 (p = 0.21; n = 8) or mdm2 (p = 0.13; n = 8) mRNA expression levels in transgenic mice thyroids compared to wild-type. Ionizing radiation (15Gy) of wild-type murine primary thyroid culture resulted in increased expression of PBF after 24 hours (1.88 ± 0.09 fold; p = 0.02; n = 3).
Overall, these results suggest that the functions of PBF and p53 are intimately related. Further work needs to be carried out to determine the precise functional effects of PBF on p53 stabilization in thyroid cells.
Department of Cancer Biology, Mayo Clinic Comprehensive Cancer Center , Mayo Clinic, Jacksonville, FL
Thyroid Cancer Saturday Poster Basic
Anaplastic thyroid carcinoma (ATC) is a highly aggressive carcinoma with a mortality rate near 100% and is in need of new therapeutic options. One critical component of drug discovery is the availability of well-characterized cell lines derived from patient tumors for identification of molecular mechanisms related to tumor biology and drug responsiveness. A recent report indicates that up to 42% of thyroid cancer cell lines, including ATC, are redundant or not of correct tissue origin. We report four new ATC cell lines and the methodologies used to characterize the originating tumor tissue and derivative cell lines.
To validate the integrity of our newly derived cell lines, we confirmed histologically the original diagnosis of the ATC tumor tissues and demonstrated identical matching of the short tandem DNA repeats (STR) and mutational status to the tumor-derived cell lines. This is the first time that molecular descriptions of thyroid cell lines are matched to the originating tumor tissues. In addition, we fully characterized the cell lines for proliferative growth, mRNA expression of seven thyroid markers, four oncogenes and array CGH to identify novel deletions and amplifications.
Previously in other cell lines, we showed that RhoB is a key signaling node for the growth inhibition of ATC. Using our new four cell lines, we have now identified five classes of compounds (10 μM FTI-277, 10 μM GGTI-286, 1 μM lovastatin, 1 nM romidepsin, 1 μM UCN-01) that upregulate RhoB and induce inhibition of cell proliferation in a dose-responsive fashion.
In conclusion, we have developed four new molecular characterized ATC cell lines. Our results further implicate RhoB as a molecular target for therapy in genuine ATC cell lines.
Nuclear Medicine, Instituto Português de Oncologia , Lisbon, Portugal
Thyroid Cancer Saturday Poster Clinical
Publications on rhTSH-aided RAI thyroid remnant ablation (rhTSH-A) generally have involved single centers and not reported ablation success rates by T or N status or other potential predictive patient/disease characteristics.
This multinational, multicenter retrospective study seeks to further characterize safety/efficacy of rhTSH-A. The study will include multivariate statistical analysis of factors potentially predicting rhTSH-A success. Also, ablation success rates will be compared for rhTSH-A patients versus historical controls given thyroid hormone withholding-aided ablation (THW-A). Ablation success is defined by institutional criteria, based on diagnostic whole-body scan, serum thyroglobulin assay, or both. Patients must have received a large RAI activity primarily to ablate thyroid remnant and any microscopic residual DTC, and been followed ≥8 months post-ablation. Anonymized data are collected via a standardized Excel spreadsheet pursuant to local ethical requirements. Data collection will close circa 30 June 2009.
We report here selected descriptive statistics for our rhTSH-A group as of 11 May 2009. Data were available on 181 rhTSH-A patients in total from 15 European/Asian centers (64% F, median age 48 yrs, 66% papillary, 20% follicular, 9% mixed, 4% less differentiated histology). Proportions of patients by TNM stages (n = 180) were: T1–2, 62%, T3–4, 34%, TX or T not available, 3%; N0, 57%, N1, 39%, NX, 4%; M0, 83%, M1, 10%, MX, 7%. Median (range) ablative activities were 100 (60–300) mCi/3.7 (2.2–11.1) GBq. Table 1 gives rhTSH-A success rates overall and by tumor stage. Despite frequent locally advanced disease or nodal metastasis in our patients, rhTSH-A success rates appear to be high and within the range of those reported for rhTSH-A or THW-A (75%-100%) in comparative studies using rhTSH in the standard regimen (0.9 mg/day × 2, RAI given 24 hr post-second injection).
rhTSH-A Success Rates (According to Institutional Criteria) Overall and By Disease Stage
TNM staging was according to UICC 5th edition or 6th edition. In addition to 1 patient with no data available on TNM stage, there were 3 patients with no data available on T stage and 3 with TX disease.
rhTSH-A, recombinant human thyrotropin-aided ablation; THW-A, thyroid hormone withdrawal-aided ablation; TSH, thyroidstimulating hormone.
These preliminary ablation success rate data from a multinational, multicenter retrospective study suggest that rhTSH-A is effective in ablating thyroid remnant in DTC patients across the range of T or N stages. rhTSH-A success rates in our study seem similar to rates for rhTSH-A or THW-A in published comparisons.
Thyroid Cancer Saturday Poster Clinical
The role of serial post-op serum Tg measurements in monitoring for recurrent disease in patients with PTC is now well established. This retrospective study was undertaken to determine whether use of a 2G-Tg assay (functional sensitivity 0.05 ng/ml) could provide any additional new information and serve as a reliable tool in the management of PTC.
Patient inclusion criteria: Near-total thyroidectomy at LAC-USC, LT4 suppression Rx (TSH < 0.05 mIU/L), no RAI Rx, TgAb-negative and adequate samples available during study period.
In 19 disease-free (Stage 1/II) patients, an average basal 2G-Tg of 0.25+/−0.12 (SD) ng/mL was attained by 2 months post-op and then remained at that level during long-term follow-up (2–5 yrs). Small variations (<2 fold) in Tg levels in individual patients were seen during this time-frame. In contrast, 15 patients who eventually displayed recurrent disease exhibited a progressive rise in serial follow-up 2G-Tg measurements or an elevated 2G-Tg within the first 2 months (>1.0 ng/mL) that appeared to be related to higher pre-op Tg values.
This retrospective study reveals: 1. 2G-Tg assay provides the greater sensitivity and reproducibility required for early post-operative evaluation. 2. Disease-free (Stage1/II) patients displayed remarkably consistent 2G-Tg values of <0.5 ng/mL that allows indefinite deferral of RAI therapy. 3. Serial 2G-Tg measurements on L-T4 suppression appear to aid early detection of recurrent disease. 4. As pre-op 2G-Tg can be related to the degree of elevation in Tg post-op when recurrence occurs, its routine measurement should be considered in the future. 5. A future prospective study to validate these findings appears justified.
Endocrine Neoplasia and Hormonal Disorders, UT MD Anderson Cancer Center , Houston, TX
Thyroid Cancer Saturday Poster Clinical
Recent publications indicate that sorafenib (SOR) may have clinical activity in patients (pts) with metastatic, differentiated thyroid carcinoma (DTC), with most pts achieving stable disease (SD). Since DTC is often indolent, we sought to determine whether SD is a clinically relevant endpoint for pts on SOR.

Unstimulated (basal) calcitonin levels remained low throughout the 2-year trials and were similar between treatments.
Pts with DTC on SOR-based therapies were identified from our clinical database. Pts with SD as their best response were identified and evaluated for radiographic progression using RECIST. The goal of this analysis was to determine if the rate of change in tumor size differs before and after treatment (tx) activation.
55 pts in our clinical database were treated with sorafenib or sorafenib-containing regimens for DTC. We excluded 28 pts for the following reasons: 17 had either no pre-tx or no post-tx tomographic scan (6 stopped drug due to toxicities before restaging, 3 were followed at home, 3 had SD but no pre-tx scans, and 5 have yet to be restaged); 6 pts had progressive disease (PD) or died before first restaging; 5 had partial remission. This left 27 pts whose best response was SD and who had pre and post-tx scans available. Sixteen/27 pts were male (59%); median age was 60 yrs. Sixteen pts had papillary, 8 follicular, and 3 poorly differentiated thyroid cancer. All pts had metastatic, progressive disease (>/ = 20% increase in target lesions) prior to starting on SOR. Figure 1 shows the pace of tumor growth before and after SOR. The slope of line prior to tx was 0.204 while the slope of the line post tx was 0.003. Of the 30 pts with SD as their best response (includes the 3 pts with no pre-tx scans), 2 pts have died. Median overall survival (OS) has not been reached, however, the OS was 84% at 32 months, compared with a median OS of 12 months in pts with PD as their best response (p < 0.001, log-rank).
Stability of disease in pts with progressive, metastatic, DTC is a clinically relevant endpoint.
Thyroid Cancer Saturday Poster Clinical
Follicular neoplasms represent one of the most important challenge in the diagnostic procedures of thyroid cancer. Several biological markers have been studied in this subgroup of thyroid nodules but none of them, taken individually, has been demonstrated to have sufficient sensitivity and specificity to be employed for diagnostic purposes. Aim of this study was to find a panel of biological markers whose gene expression profile could be so different between benign and malignant thyroid nodules to be used for a better defintion of follicular neoplasms.
By real-time PCR we analysed mRNA expression of 11 genes [6 thyroid differentiation genes (TTF-1, PAX-8, TPO, TSH-R, NIS and Tg) and 5 genes involved in thyroid tumorigenesis (PPARg, Gal-3, EGF-R, MET and onfFN)] in a total of 174 human thyroid tissues (87 tumor samples and 87 corresponding normal tissues) obtained from 72 patients operated on for papillary thyroid cancer (PTC) and from 15 patients operated on for follicular adenomas (FA).
We found that all thyroid differentiation genes and PPARg were significantly less expressed in PTC than in the corresponding normal tissue while onfFN, MET and Gal-3 were significantly more expressed in PTC than in normal tissues. No difference was observed in the level of expression of EGF-R mRNA in PTC and their corresponding normal tissue. A completely different pattern of gene expression was found in FA: in particular a statistically difference between mRNA expression level in tumoral and normal tissue was observed only for PPARg, similarly to PTC. All the other genes were expressed at no different level in FA with respect to their corresponding normal tissue.
Our data showed that 10/11 selecetd genes were differentially expressed (at higher or lower level) in PTC with respect to normal tissue while only 1/11 showed this difference in FA and the corresponding normal tissue. The analysis of the level of expression of these genes in fine needle aspirates might represent a helpful and innovative method for the presurgical definition of follicular neoplasm.
Surgery, Massachusetts General Hospital , Boston, MA
Thyroid Cancer Saturday Poster Clinical
The prevalence of obesity is increasing worldwide. Studies have shown the development of some cancers to be associated with obesity. However, an association between obesity and the development of thyroid cancer has not been established.
The American College of Surgeons' National Surgical Quality Improvement Program (ACS NSQIP) was queried for patients that underwent thyroid surgery during the years 2005–2006. Resource variables included patients age, gender, race, height and weight. Analysis was done using SPSS statistical software.
4,765 patients were identified, of which 81% were females and 19% male. The most common race was caucasian (70%), followed by African Americans (10%) and Hispanic (5%). Body Mass Index (BMI) was available for 4,705 patients with a mean of 29 ± 7.1 (range 8.6–89.8). 1.4% of patients were underweight (BMI < 18.5 Kg/m2), 30.7% normal weight (BMI 18.5–24 Kg/m2), 31.5% overweight (BMI 25–29 Kg/m2), 18.9% obese (BMI 30–34 Kg/m2) and 17.5% morbidly obese (BMI ≥ 35). Final diagnosis included malignant disease in 31% of patients and benign disease in 69%. Overall patients with lower BMI were found to have a significantly higher risk of malignancy in the resected thyroid. The rate of malignancy was 27.6% in patients with BMI ≥ 30 vs. 32.4% in those with BMI < 30 (p < 0.001, Odds ratio = 1.26).
Increased BMI is associated with lower risk of thyroid cancer. Further investigation of biological mechanisms that link obesity with cancer may explain differences between various cancers.
Endocrinology, La Paz Hospital , Madrid, Spain
Thyroid Cancer Saturday Poster Clinical
A family history of non-thyroid cancer (FHC) has been associated with an increased relative risk for papillary thyroid carcinoma (PTC), but little is known about the influence of FHC on differentiated thyroid carcinoma (DTC) prognosis. Our aim was to analyze the prevalence and types of cancer among relatives of patients with DTC and the possible relationship of FHC with histological DTC subtypes and clinical outcome.
200 patients, 32 men and 168 women, with a mean age at diagnosis of 44 ± 16 years and an average follow-up period of 7 years (range 0,5–30 years) were included in this study. All patients underwent total thyroidectomy and pathology revealed 167 PTC, 20 follicular (FTC) and 13 Hürthle cell carcinomas (HCC). A mean total dose of 192 ± 123 mCi of radioiodine was given postoperatively. At the time of the study 84% of patients achieved criteria for cure according to ATA Guidelines and 15% of cured patients showed serum TSH-stimulated thyroglobulin levels (STL) between 0,1 and 2 ng/ml.
Up to 65% of the total group referred a diagnosis of cancer in at least one first- or second-degree relative, being the most frequent breast (36%), stomach (34%), lung (29%), and DTC (20%), followed by colon (19%), uterus and prostate (15% each), lymphoma (12%), larynx and liver (10% each), melanoma (8%), pancreas and leukemia (5% each), ovarian, bone and brain cancer (4% each). FHC group showed a higher rate of HCC (p < 0,001), FTC (p < 0,05), diffuse sclerosing variant of PTC (p < 0,05), multicentricity (p < 0,001), distant metastasis (p < 0,05) and detectable STL (p < 0,05) with no differences in gender distribution, mean age at diagnosis and follow-up period when compared to the non-FHC group. All patients with HCC had detectable STL and more than one first-degree relative with a non-thyroid cancer, and 40% of them had at least one first-degree relative with skin cancer.
Our study suggests that FHC could be considered a new marker of more aggressive histological DTC subtypes and poorer outcome. This may help to select the best management of these patients, identify new inheritable patterns of carcinogenesis and explore the potential role of shared environmental exposures.
Detection Rate of Medullary Thyroid Carcinoma with Calcitonin Immunohistochemistry on Cytospin Preparations
Thyroid Cancer Saturday Poster Clinical
Medullary thyroid carcinoma (MTC) is a parafollicular C cell-derived neuroendocrine tumor with a more aggressive behavior. Currently, the European Thyroid Association consensus guidelines recommend the use of serum calcitonin screening in all patients with thyroid nodules to aid in the early detection of MTC. The American Thyroid Association guidelines recommend fine needle aspiration (FNA) of clinically suspicious thyroid nodules; however, could not recommend for or against the routine use of serum calcitonin. MTC is a diagnostic dilemma on FNA due to its varying cytopathologic features. At our institution, we perform calcitonin immunohistochemistry (IHC) routinely on cytospin preparations of all indeterminate thyroid FNA's. We aim to evaluate the detection rate of MTC with calcitonin immunohistochemistry on cytospins and its use as a potential screening mechanism.
Calcitonin immunohistochemistry was ordered on 57 thyroid FNA's diagnosed as “Indeterminate for Neoplasm”. A cytospin preparation was performed on each sample using routine cytospin preparation protocol. Calcitonin IHC was performed at a 1:300 dilution (Dako North America, Carpinteria CA). The cells on the cytospin were evaluated for either positive or negative reactivity.
Of the 57 cases evaluated with calcitonin immunohistochemistry, three showed strong cytoplasmic staining within the cell groups. All three corresponding surgical resections from these patients were confirmed as MTC by histology. The remaining 54 cases were negative for calcitonin within the cell groups. 17 of these 54 cases have thus far had subsequent surgical resections confirmed as a non-MTC diagnosis.
The routine use of cytospin calcitonin IHC in patients with indeterminate FNA's is useful in screening for MTC. Currently, in the United States, there is not an effective screening mechanism for MTC. The routine use of serum calcitonin screening, as used in Europe, has been challenged due to unresolved issues with sensitivity, specificity and cost effectiveness. Based on our preliminary results, calcitonin IHC on cytospin preparations from FNA's could be used in place of serum calcitonin screening as a low cost alternative for the detection of MTC.
U.O. Chirurgia Endocrina, Università Cattolica del Sacro Cuore - Policlinico A. Gemelli , Rome, Italy
Thyroid Cancer Saturday Poster Clinical
Fine-needle aspiration biopsy (FNAB) is the cornerstone of assessment of thyroid nodules. Cytological criteria for benign and malignant aspirates are well established. When cytology suggests a follicular neoplasm only histological evaluation can differentiate between benign and malignant lesions. We evaluated if there are factors predictive of malignancy in cytologically indeterminate (follicular) thyroid nodules.
The medical records of all the patients who had a diagnosis of follicular thyroid nodule (Thy3 according to the British Thyroid Association classification) between December 2007 and November 2008 were reviewed. Among them, those who had an histological control were included. The following parameters were registered: age, sex, ultrasound characteristics, nodule size, thyroid disease (single nodule Vs multinodular goiter), immunocytochemical stains for HBME-1 and Galectin-3, final pathology.
Among 1585 patients who underwent FNAB, 261 had a follicular nodule (Thy3). Among them, 195 underwent thyroidectomy: 152 females and 43 males (mean age 48.7 years; range: 20–77). Final histology showed 146 benign and 49 malignant nodules (follicular variant of papillary carcinoma in 43 cases, follicular carcinoma in 6). No significant differences were found between benign and malignant lesions for age and sex of the patients, lesion's size, ultrasound characteristics. The malignancy rate in case of single nodules was significantly higher than in multinodular goiter (30/63Vs19/132) (P < 0.001). Positive immunostaining for both HBME-1 and Galectin-3 was observed in 58 cases, negative for both in 137. The malignancy rate was significantly higher in HBME-1 and Galectin-3 positive nodules (42/49Vs16/146) (P < 0.001). The risk of malignancy was 1:4 for the entire series of patients, but it increased to 1:2.1 (47.6%) for single nodules and to 1:1.4 (72.4%) for HBME-1/galectin-3 positive nodules.
One in four patients with cytological indeterminate thyroid nodule has a differentiated thyroid carcinoma. Thyroidectomy is mandatory in all the patients with single and/or HBME-1/galectin-3 positive nodules, because of the increased risk of malignancy, and suitable in all the other cases.
Medicine, University of Toronto , Toronto, Canada
Thyroid Cancer Saturday Poster Clinical
It can be challenging to counsel patients with early stage papillary thyroid cancer (PTC) on adjuvant radioactive iodine (RAI) treatment. Decision aids (DAs) are tools or instruments used to inform patients about treatment options. We have developed a computerized DA to inform future patients with early stage PTC on the potential risks, benefits, rationale, uncertainties, reproductive and other long-term considerations of the decision to accept adjuvant RAI treatment or to have no RAI treatment with close-medical follow-up. The preliminary usability testing results are presented.
This evidence-informed DA was developed by a multidisciplinary team of thyroid cancer specialists and methodologists after performing multiple systematic reviews of the relevant literature. Thyroid cancer survivors, thyroid cancer specialty physicians, and lay individuals with no prior history of thyroid cancer provided feedback on the DA. The DA was evaluated using a questionnaire based on the System Usability Scale for human-computer interaction. Likert scale data was on a scale of 1 to 5, with 5 representing strongest agreement and 1 representing strongest disagreement).
Among the 29 study participants, there were 3 physicians, 5 thyroid cancer survivors, and 21 lay individuals with no prior history of cancer. Approximately 60% (17/29) of the individuals testing the DA were female. Participants generally strongly agreed (mean agreement scores 4 or higher out of 5) with the following statements about the DA: a) it would likely be used frequently by future PTC patients, b) it was easy to use, c) it was easy to retrieve supplemental information, d) printing information was easy, e) most people would learn to use it quickly, and f) I feel confident using the DA. Participants generally disagreed (mean agreement scores lower than three out of 5) with the following statements about the DA: a) it is unnecessarily complex, b) the support of a technical person would be needed to use it, c) there was inconsistency in the format, and d) it is cumbersome.
Complex information about decision making on adjuvant RAI treatment may be feasibly presented within a computerized DA intended for PTC patients.
Quantitative Analysis of Dynamic Power Doppler Sonograms in Patients with Nodular Thyroid Disease
Thyroid Cancer Saturday Poster Clinical
The superficial location and the distinctive echogenenic pattern of the thyroid make it an ideal organ for the study by sonography. However, currently, few studies report the objective parameters in differentiating benign and cancer, but they are criticized about the interobserver variability and only “static” information on thyroid vascular perfusion was collected without details on hemodynamics. To improve the shortcomings of traditional perfusion index, in this study, a novel thyroid vascular perfusion index (VPI) and a power Doppler correlation-map are proposed to study the “dynamic” thyroid vascular perfusion, which would be also quantitative analysis method, may be useful tool for routine examination of thyroid tumors.
169 patients who have thyroid tumors were included in this study. The images were obtained on power Doppler Sonography recorded through dicom format which contains 45 frames of 24 Bits continuous images. Quantification of vascular power Doppler signal was automatically performed by a special software (TDVI, Institution of Applied Mechanics, Taiwan University). Diagnosis was further confirmed by aspiration cytology and resected specimens.
The AUC of single attribute is around 0.72 to 0.78, we use the Fisher Discriminant to combine the attributes together. And the objective parameters can reach high sensitivity and specificity with AUC to 0.8057.
Our newly quantitative analysis of power Doppler sonograms, which gives more “hemodynamics” aspects, can significantly improve the accuracy of thyroid cancer diagnosis.
Medullary Thyroid Cancer: A Pain in the Neck!
Thyroid Cancer Saturday Poster Clinical
Unlike the more common well-differentiated thyroid cancer, medullary thyroid cancer (MTC) is more aggressive, commonly presents with lymph node (LN) metastases and has a worse prognosis. Tumor size and LN involvement have been shown to affect stage of disease; however, this is to our knowledge the first study that attempts to correlate neck pain on presentation with extent of disease.
A retrospective analysis was performed on all patients operated on from February 1998 to December 2008 with a diagnosis of MTC. A questionnaire addressing presenting symptoms was completed by each patient during the initial encounter and was prospectively collected. The presence or absence of neck pain was compared to the extent of disease, both clinically and pathologically. Patients operated on for papillary thyroid cancer (PTC) were the control. The data were analyzed utilizing the Fisher's exact test to calculate the two-tailed p-value.
Of the 109 patients with medullary thyroid cancer who were operated on at UCSF, 50 (46%) met our inclusion criteria. MTC patients presented with neck pain more frequently than the PTC control group (11/50 and 3/50, respectively, p = 0.041). Of the 11 MTC patients with pain, 9(82%) had LN involvement on final pathology, compared to 14(36%) out of 39 without pain (p < 0.002). Stage of disease was also impacted by the presence of pain; 18% of patients with pain were diagnosed at stage 1–2 and 82% as stage 3–4c compared to 64% and 36%, respectively for those without pain (p < 0.009). The presence of pain in patients with PTC did not correlate with either LN involvement or stage.
This study demonstrates that neck pain at presentation correlates with extent of disease in patients with MTC. MTC patients with neck pain were more likely to have lymph node involvement and a worse stage at presentation compared to those with PTC. These findings suggest that a more aggressive surgical approach may be considered in patients presenting with pain and medullary thyroid cancer.
Radioiodine Therapy of Metastatic Disease in DTC after Preparation with Recombinant Human TSH
Thyroid Cancer Saturday Poster Clinical
Several studies reported effectiveness and safety of recombinant human TSH (rhTSH) as a preparation for radioiodine (RAI) administration for thyroid remnant ablation and also for treatment of persistent or recurrent disease in DTC. We present a retrospective evaluation of DTC patients with rhTSH-assisted RAI treatment.
16 therapeutic rhTSH-assisted doses were administered in 13 CDT (11 papillary, 2 follicular) patients (3M/10F, mean age 48 years). Diagnosis was established between 1992 and 2007. TNM staging showed 3 patients stage I, 3 patients stage II, 3 patients stage IVa and 4 patients stage IVc. Total thyroidectomy and RAI remnant ablation was the initial treatment, and positive I131 4 mCi WBS and thyroglobulin (TG) measurements demonstrated metastatic disease in all cases. Time from 1st iodine dose was 7–72 months. RhTSH was used because of the patient's advanced age in 3 cases, advanced disease in 3 cases and patient refusal for T4 withdrawal in 7 cases.
WBS 7 days after rhTSH assisted RAI treatment was positive in 11/13 patients: 6 cases in the neck, 2 in lung, 1 in mediastinum and 2 in spine. Nowadays 5/13 patients are considered disease-free (stage I-II), 2/13 died during the first post-treatment year (stage IVc with pleural metastases). 6/13 (all of them stage IV at diagnosis) still present persistent disease assessed by positive TG levels or imaging techniques, although 3 cases remain stable: 1 case with positive neck RAI uptake shows decreasing TG levels and negative imaging, other patient reduced lung metastasis up to 50% of the initial size by CT scan and TG is decreasing. In a third case TG remains stable ∼6 ng/ml. RhTSH was well tolerated in all cases.
Effectiveness of RAI therapeutic doses in patients con advanced DTC is difficult to assess because of the disease progression. In our experience, young patients with local or distant metastasis stage I and II presented good outcome and are currently in disease-free state. In patients with high risk stages, outcome is similar to those who received treatment with LT4 withdrawal. Although this is a retrospective study, we suggest that rhTSH-assisted RAI treatment becomes a choice to LT4 withdrawal in selected DTC patients.
Dipartimento Clinico Sperimentale di Medicina e Farmacologia, Sezione di Endocrinologia, AOU Policlinico “G. Martino”, Università di Messina , Messina, Italy
Thyroid Cancer Saturday Poster Clinical
Single or multiple ITM of extra-thyroid primary tumors are reported to be rare. Malignancies that metastasize to the thyroid include cancers originating from lung, breast, gastrointestinal tract and kidney.
We report two men of 67 and 79 years with ITM from RCC that had appeared 1 and 18 years after the diagnosis of RCC. This long lag-time between RCC diagnosis and appearance of ITM is known from the literature.
In the first patient, abdominal ultrasonography (US) and contrasted CT-scan showed an 8-cm mass in the upper pole of the left kidney. Cytological examination of a fine needle aspirate (FNA) from the kidney mass revealed a low grade RCC. One year later, he noticed a mass in the neck. Physical examination revealed a multinodular goiter. US showed a thyroid gland increased in size, with the left lobe occupied by a solid nodule of 52 mm containing hypoechoic areas. There were also a number of solid nodules in the right lobe and isthmus. All nodules showed a moderate perinodular blood flow at Color-Doppler. All thyroid nodules were cold at a thyroid scintiscan with I-131. Serum TSH, FT3 and FT4 were normal. Cytological examination of the US-FNA of the nodule in the left thyroid lobe revealed a pattern nearly identical to that of the specimen from the renal mass. The patient underwent medical therapy with INF-alpha+IL-2, followed by a rescue therapy with bevacizumav. Past history of the second patient was relevant only for a total left nephrectomy for RCC that had been performed 18 years earlier. Physical examination revealed a multinodular goiter. Neck US showed a multinodular goiter with hypoechoic nodules in the left and right lobe with an intra- and perinodular blood flow in all nodules. Serum TSH, FT3 and FT4 were normal. The patient refused FNA evaluation of the thyroid nodules. After thyroidectomy, histopathologic examination allowed a diagnosis of bilateral ITM from RCC.
History of patients with thyroid nodule(s) should include inquiring about extra-thyroid malignancies, especially RCC, that may have been diagnosed even many years earlier. As a corollary, given the relatively long life expectancy of RCC patients, their follow-up should include periodic thyroid US.
Department of Internal Medicine, University of Pisa , Pisa, Italy
Thyroid Cancer Saturday Poster Clinical
We had the opportunity to evaluate children suffering from differentiated thyroid cancer (DTC), all from Gomel region in Belarus (where the diagnosis of DTC was made following the Chernobyl's accident) in our hospital at the University of Pisa in october 1994. In 19 of the examined cases, the surgical treatment had consisted of a hemithyroidectomy.
These 19 patients were reoperated with completion thyroidectomy; the mean latency from the first operation was 2 years. Histology revealed a residual DTC in 3 (16%) and lymph node metastases in one child. All patients operated in Pisa underwent 131-I therapy one month after surgery.
The post therapy WBS, performed in 18 out of 19 of the patients treated with completion of thyroidectomy was negative in 7/18 (39%), showed lung metastases in 5/18 (28%) and lymph node metastases alone in 6/18 (33%). One patient refused 131-I therapy and was not evaluated by WBS. In October 2008 (after 14 years) 18/19 patients previously submitted to completion thyroidectomy were re-evaluated by neck ultrasonography and rhTSH-stimulated serum Tg. Among them, 17 had rhTSH-stimulated serum Tg <1 ng/ml and negative neck ultrasonography, while the one (the same who refused 131-I therapy) had residual thyroid tissue on the left side at neck ultrasonography and rhTSH-stimulated serum Tg was 32 ng/ml.
In conclusion, after 2 years from the initial operation completion thyroidectomy permitted to diagnose a residual DTC in 22% of patients and to treat by 131-I lung or lymph node metastases in more than 60% of patients, who were all free of disease after a 14 years follow-up.
Preoperative Screening of Thyroid Nodules ≥3 cm with Ultrasonographic-Guided FNA: Retrospective Study
Thyroid Cancer Saturday Poster Clinical
In patients with thyroid nodules is possible to discover carcinomas by US-guided FNA from 9% up to 13%. Our study analyzes the casuistics of patients underwent on total thyroidectomy for benign pathology, in particular patients with thyroid nodules >/= 3 cm valued by FNA and after underwent on operation in order to verify the reliability of FNA in big thyroid nodules.
A retrospective study was performed at Department of Surgical Science of Rome (La Sapienza University) from 1998 to 2008.
We consider in our study only patients with single or multiple thyroid nodules >/= 3 cm underwent on US-guided FNA. The patients were 1047. The definitive histologic diagnosis was benign in 1009 patients (96,37%) whereas a malignant lesion was discovered in 38 patients (3,63%).
Our study verified a small percentage (3,63%) of false negative (FNA vs definitive histologic diagnosis). In our opinion is important to make a critical and careful study on thyroid nodules >/= 3 cm not only considering the cytologic diagnosis.
Unusual Presentation of Papillary Thyroid Microcarcinoma: Metastases of Bone and Lung
Thyroid Cancer Saturday Poster Clinical
Thyroid cancer is among the most common endocrine malignancies. The incidence of thyroid cancer appears to be rising. Papillary thyroid microcarcinoma (PTMC) had a benign clinical course, only 5–10% of the patients having distant metastases at the time of diagnosis.
Case
A 35-year-old woman consulted our outpatient clinic of endocrinology. She was clinically asymptomatic. She had undergone a subtotal thyroidectomy due to euthyroide multinodular goitre without fine needlle aspiration biopsy. The histological examination demonstrated multifocal PTMC (follicular variant, maximum diameter 0.7 cm). There was no vascular or capsule invasion, or extrathyroideal extention. Her serum thyroglobulin level (Tg) was 1000 ng/ml (0.2–70) when thyroid-stimulating hormone (TSH) level was 38 uIU/ml (0.34–5.6). Thyroglobulin antibodies were negative (0.8 IU/ml, normal range: 0–4). Thyroid and neck ultrasonography showed residual thyroid tissue and lymphadenopathy. Iodine-131-whole body scan (WBS) showed markedly iodine retention in the neck, lung and pelvis. Chest CT and X-ray showed multiple metastases in the lung. Pelvic MRI demonstrated a 5 cm mass in the ischium pubis. She underwent completion thyroidectomy and bilateral neck dissection. She is going to have high dose radioactive iodine ablation therapy after resection of pubic lesion.
Although most patients with PTMC had a benign clinical course, distant metastases causing mortality were occasionally observed. Therefore, it is important to treat PTMC as early as possible with extensive surgery, radioactive iodine therapy and, thyroxine suppression.
Department of medical Endocrinology PE 2132, National University Hospital , DK-2100 Copenhagen, Denmark
Thyroid Diseases Saturday Poster Clinical
Background: Reliability of quality of life measures can be evaluated in several ways, two of which are internal consistence reliability and test-retest reliability. A reliability coefficient (i.e. estimated ratio of true to total (i.e. true plus random) variation, ranging 0 to 1) above 0.70 is the usual threshold for use in clinical studies.
Aim: To investigate internal consistency reliability and test-retest reliability of the thyroid-specific quality of life questionnaire, the ThyPRO.
Methods: A cross-sectional sample of 907 thyroid outpatients completed the 13-scale ThyPRO questionnaire. A retest completion after two weeks was obtained from 107 patients. Internal consistency reliability was evaluated by standard Cronbach's α using MAP-R for SAS. Test-retest reliability was evaluated by the intraclass correlation between test-retest responses from 87 of the 107 in the retest sample, who rated themselves as stable between the two measurements, using SAS PROC GLM.
Results: Internal consistency reliability for the 13 scales were: Goitre symptoms 0.89, Hyperthyroid symptoms 0.82, Hypothyroid symptoms 0.70, Eye symptoms 0.84, Tiredness 0.94, Cognitive complaints 0.93, Anxiety 0.90, Depressivity 0.92, Emotional susceptibility 0.93, Impaired social life 0.82, Impaired daily life 0.94, Impaired sexlife 0.92 and Cosmetic complaints 0.84. Test-retest reliability (intraclass correlation) was: Goitre symptoms 0.87, Hyperthyroid symptoms 0.89 Hypothyroid symptoms 0.80, Eye symptoms 0.86, Tiredness 0.85, Cognitive complaints 0.88, Anxiety 0.77, Depressivity 0.88, Emotional susceptibility0.87, Impaired social life 0.84, Impaired daily life 0.83, Impaired sexlife 0.86 and Cosmetic complaints 0.85.
Conclusion: All coefficients were above the required 0.70. Most coefficients were above 0.85 or even 0.90, which is very good for these kinds of measures. Generally, test-retest reliability coefficients were lower than the corresponding Cronbach's α's, which may be due to patients actually undergoing change during the two-weeks inter-test period. Thus, we found appropriate reliability for the ThyPRO questionnaire, which is now ready for use in clinical studies.
Results of Chernobyl Catastrophe Radiation Exposure Effect on Thyroid Function in Young Belarusian Patients
Thyroid Diseases Saturday Poster Clinical
A dramatic increase of the incidence rate of thyroid carcinoma in children and adolescents is the greatest consequence of the Chernobyl accident. In Belarus, the Russian Federation and Ukraine nearly 5 000 cases of thyroid cancer have now been diagnosed to date (2006) among children who were aged up to 18 years at the time of the accident. However, the other effects of radiation exposure on thyroid are not well proven yet.
Since 1990 regular screenings examinations are performed in contaminated regions of Belarus. In 2007, we examined a cohort of 768 subjects in Stolin, Brest region. It consisted of 444 not irradiated subjects (group 1), 140 irradiated “in utero” (group 2) and 184 being less than 3 years old at the moment of catastrophe (group 3). All patients passed ultrasonic examination of thyroid gland with morfometry, analysis for thyroid function (FT4, TSH, TPO-AB).
The mean age of subjects at the time of the study has been 19.9 ± 1.8 yr. We revealed a general increase in thyroid pathology incidence - Autoimmune thyroiditis was detected in 7,7%-7,8%-5,2% of patients in groups 1, 2 and 3 accordingly. Higher incidence of hypothyroidism was observed in groups 2 and 3 (6,9% and 6,7%) in comparison to 3,4% in group 1. Same was observed for nodular pathology (5,9% and 5,2% vs 2,8% for groups 2, 3 and 1 respectively). A dramatic increase of thyroid hypoplasia incidence was detected among irradiated “in utero” subjects: 11,8% and up to 15% for those ones irradiated in the 1st trimester of gestation, against 3,4–3,7% in the other comparison groups.
Our data have shown, that irradiated subjects suffer from higher incidence of thyroid hypoplasia, hypothyroidism and other thyroid diseases comparing to the non irradiated persons. The more thorough screening studies with larger amount of participants are still required to prove that radiation exposure “in utero” and at the first 3 years of age can lead to a significant increase of thyroid non malignant diseases incidence in young patients.
Surgical Oncology, Endocrine Surgery, University of Pittsburgh , Pittsburgh, PA
Thyroid Diseases Saturday Poster Clinical
Thyroid paraganglioma (TPG) is reported in the literature in < 35 patients, only 3 of whom have been men. We present the clinical and pathologic characteristics of 4 TPG from a single institution.
Under an IRB-approved protocol, we searched the pathologic records of all patients from 1981–2008 who underwent thyroidectomy with a final histologic diagnosis of paraganglioma. Histology was reviewed by a single pathologist.
TPG accounted for 4 of 6782 (0.06%) patients undergoing thyroidectomy. Mean age at diagnosis was 60 y (40–74) and 2 patients were men. Presenting features included stridor with endotracheal invasion in 2 patients, compression of the great vessels in 1 patient and hemoptysis in 1 patient. The diagnosis of TPG was unsuspected preoperatively in all 4 patients. In 2 patients, fine needle aspiration (FNA) cytology was inadequate for diagnosis due to excessive vascularity. Intraoperative frozen section results suggested medullary thyroid cancer in 2 patients, Hurthle cell carcinoma in 1 patient, and were deferred in 1 patient. TPG was managed by thyroid lobectomy in 1 patient and total thyroidectomy in 3 patients; local invasion required concurrent tracheal resection in 2 patients. Histopathologic review confirmed primary TPG in 3/4 patients. The fourth patient received thyroid lobectomy with TPG completely replacing the left thyroid lobe. Local invasion was seen histologically in 3/4 patients and TPG was well-encapsulated in one patient. In all 4 cases, immunohistochemical analysis was negative for cytokeratin AE1/3, calcitonin and thyroglobulin but positive for S100 highlighting sustentacular cells. Long-term follow-up was available for a 67-year old woman who after resection of a large TPG with vascular and tracheal invasion, experienced a 7-year disease-free interval until demise from metastatic colon adenocarcinoma.
Primary TPG is indeed rare, occurs in males, frequently presents with compressive symptoms, and can be clinically aggressive. FNA is often non-diagnostic and TPG are difficult to diagnose on frozen section. Despite local invasion of adjacent structures, aggressive resection can achieve a long disease-free interval.
Preoperative Evaluation of Thyroid Disease in Primary Hyperparathyroidism
Thyroid Diseases Saturday Poster Clinical
Some authors suggest that thyroid disease is even more prevalent among patients with primary hyperparathyroidism (pHPT) than in the general population. In recent years minimally invasive approach has been preferred to conventional parathyroidectomy. Furthermore, preoperative ultrasonography (US) has been advocated as necessary in the evaluation of patients with pHPT and has been believed to be valuable not only for localizing parathyroid(PT) adenomas but also for detecting accompanying thyroid nodules (THNO).
This study involves 245 patients with primary hyperparathyroidism. Preoperative thyroid and PT US are performed in all patients with fine needle aspiration biopsy for the THNO when necessary.
Of the patients 89,4% was euthyroid, 4,5% was hypothyroid and 6,1 was hyperthyroid. Minimal invasive approach was preferred in 147 of the patients while 98 underwent conventional parathyroidectomy. Fifty five percent of the patients had THNOs. There was no thyroid disease in 89 patients, and 156 patients (63.7%) had a sort of thyroid disease: 37 had euthyroid nodular goiter, 82 had euthyroid multinodular goiter, 15 had Hashimoto thyroiditis (5 with nodules), 7 had toxic multinodular goiter, 2 had toxic adenomas, 5 had Graves disease (4 with THNO), and 6 patients had previous thyroid surgery. Of the 210 THNO from 137 patients, FNAB revealed 6 malignant, 19 indeterminate, 145 benign, and 25 insufficient cytology. Postoperatively 16 cases (6.5%) of thyroid carcinoma (14 papillary, 1 follicular, and 1 medullary) has been found. When preoperative FNAB cytology was considered, among 16 cases with thyroid carcinoma, 4 were from indeterminate, and 2 were from insufficient groups. Thyroid carcinoma was incidental in four cases (1 medullary, 1 follicular and 2 papillary). Of the thyroid carcinoma cases 6 was contralateral and 10 were ipsilateral with parathyroid adenoma.
Our study demonstrated that thyroid and parathyroid disease do coexist and thyroid cancer rate was 6.5%. Patients with primary hyperparathyroidism must be evaluated carefully for the presence of coexisting thyroid disease with ultrasonography and even with FNAB as necessary.
Endocrinology and Nutrition, Hospital Dos de Maig , Barcelona, Spain
Thyroid Diseases Saturday Poster Clinical
Most of the studies performed in Spain in the last decade, regarding urinary iodine levels (UIL), showed a significant improvement. Probably changes in the composition of daily diet contributed to this improvement. A survey was undertaken together with an information campaign for the general population on iodine intake importance and hypothyroidism in four Spanish cities. The goals were: 1/To obtain information about the consumption of iodine containing foods of the population of these four cities. 2/To measure UIL and to evaluate the prevalence of thyroid dysfunction in this population.
Non pre-selected population attending to the information campaign centers located in Barcelona, A Coruña, Málaga and Madrid. People with previously known thyroid disease were excluded. A questionnaire regarding fish, milk and iodinated salt consumption (ISC) was undertaken. UIL (Pino's method) and TSH (Whatman 903 dry paper method) were measured.
A total of 872 individuals were evaluated (40% in Madrid, 27% in A Coruña, 19% in Málaga and 14% in Barcelona). Mean age was 51 years (SD 16), and 81% were females. Gender, education or work, were not related to ISC. Fish consumption was low in young people and immigrants while milk consumption was high among young and retired people. The median of UIL was 143.2 μg/L. The prevalence of UIL < 50 μg/L was 8%. The prevalence of thyroid dysfunctions was not different by gender.
Following WHO criteria, the global, as well as the per city UIL median indicates an optimal iodine intake. Considering that only 60% of the population evaluated referred an active ISC, the intake of products such as milk and fish may contribute to the achievement on these acceptable results of the median UIL. Prevalence of hyper and hypothyroidism in this sample population is low. (Project supported by an unrestricted grant of Merck-Serono Spain).
Endocrinology, Royal Free Hospital , London, United Kingdom
Thyroid Diseases Saturday Poster Clinical
Cytokines play a key pathogenic role in thyroid-associated ophthalmopathy (TAO). Orbital connective tissue remodeling in TAO results from cytokine-dependent fibroblast activation with accumulation of glycosaminoglycans (GAG). In vitro studies suggests that TNF-α and IL-1 stimulate GAG production but have opposite effects on adipogenesis in orbital fibroblasts. Anti-cytokine therapy has been proposed as a treatment for active TAO. Clinical trial data suggest that Etanercept, which blocks TNF-α mediated processes, may suppress clinical signs of TAO.
We report a 56-year-old woman who was diagnosed with hypothyroidism in 1988 soon after a successful twin pregnancy. She was replaced with thyroxine 75mcg daily until 2006 when the dose was increased to 100mcg so that she was euthyroid (FT4 21.0pmol/l (12–22) and TSH 0.70mU/l (0.3–4.2), TPO antibodies positive at 208iu/ml (<60)). In 2005 she presented with pleurisy secondary to a rheumatoid arthritis/overlap syndrome. She failed to respond to steroids and Methotrexate. Etanercept therapy was begun in March 2008.
Within one month of commencing Etanercept she developed bilateral eye pain, peri-orbital oedema and proptosis more marked in the left eye. Exophthalmometer readings were 19mm in the right eye and 23mm in the left eye. A MRI scan of orbits documented increased retro-orbital fat consistent with TAO but no other characteristic muscle or soft tissue changes. She was TSH-receptor antibody mildly positive at 1.31iu/ml (0–0.4). Following withdrawal of Etanercept, the eye pain and oedema improved within two months. The proptosis improved and was confirmed by exophthalmometer readings of 17mm in the right eye and 19mm in the left eye.
This case report has suggested that Etanercept therapy has induced TAO in a patient with a background of long-standing Hashimoto's thyroiditis on thyroxine replacement. It would appear to confirm the in vitro data that Etanercept has differential effects on orbital connective tissue remodelling in TAO by adipocyte stimulation. Careful monitoring is required for all patients with a history of thyroid autoimmunity if commenced on anti-cytokine therapy.
Deartment of Surgery, Lund University Hospital , Lund, Sweden
Thyroid Diseases Saturday Poster Clinical
With growing economic pressure on the healthcare systems, it is of utmost importance to monitor the efficacy of methods and strategies for disease treatment. Ideally, knowledge should come from the collection of well designed randomized trials. However, differences between groups of patients can often be expected to be small. Collecting a large number of patients, from several different types of centers by the means of a prospective audit, is one way to try to answer this problem.
Scandinavian Quality Register for Thyroid- and Parathyroid Surgery is an on-line database (www.thyroid-parathyroidsurgery.com), with the aim to improve the quality of diagnostics, surgical treatment and follow-up for patients with surgical disease in the thyroid and parathyroid glands. The register also supports clinical research. The register offers user friendly reports with statistics and graphics, enabling the individual department to compare its results to the total data. An annual report in English is also published.
From January 1st 2004 until March 26th 2009, 10.067 operations were registered by 45 departments; 6677 thyroid operations, 3153 operations for primary HPT and 237 for secondary HPT. Of the thyroid patients, 81% were women and the median age was 47 years. 39% of the thyroid operations were performed as total thyroidectomy and 51% as lobectomy. 1217 patients had Graves'disease, and 1189 had a postoperative histological diagnosis of malignancy. External audit (by sample) of participating departments, shows good data validity with an error of less than 5%.
Quality Registers are important for the evaluation of strategies and results for disease treatment. They could prove to be an ideal tool to complement the results from randomized controlled trials. The results from the thyroid-and parathyroid database have identified several issues for further studies.
Internal Medicine, Mount Sinai Medical Center , Miami Beach, FL
Thyroid Diseases Saturday Poster Clinical
Toxic thyroid adenoma can lead to well known cardiovascular manifestations. Here we report a case in which a toxic adenoma was diagnosed after radio-frequency catheter ablation for Wolff-Parkinson-White (WPW) syndrome. WPW is caused by the existence of an alternative accessory pathway directly connecting the atria and ventricles. To our knowledge, WPW is rarely associated with thyrotoxicosis.
A 26 year-old white woman presented to the hospital complaining of palpitations. One week earlier she underwent radio-frequency ablation for WPW diagnosed with an ECG that revealed supra-ventricular tachycardia, a short PR interval, and a delta wave. On exam patient was tachycardic (140 bpm), and had a systolic ejection murmur (2/6). There was a painless mass on the left thyroid lobe. Neurological exam revealed fine postural tremor and brisk deep tendon reflexes bilaterally.
ECG showed narrow complex sinus tachycardia without preexcitation. 2D-echocardiogram showed normal left ventricular function. Thyroid function tests revealed a TSH of 0.00 uIU/ml, a free T4 of 1.75 ng/dL with T3 of 349 ng/dL. A 5h-radioactive iodine uptake was 54% in the area corresponding to the mass seen by u/s of the thyroid, leading to the diagnosis of toxic adenoma. Patient was started on propranolol and prednisone with clinical improvement; she then underwent radioactive iodine ablation. Five months following the diagnosis the patient was clinically euthyroid on no medications.
Prior observation that treatment of the hyperthyroidism lead to resolution of WPW suggested that the excess of thyroid hormones could possibly potentiate the anomalous pathway function. Our patient was still complaining of palpitation after being treated with radio-frequency ablation, but no preexcitation was seen in the ECG. This implies that the activation of the anomalous pathway reflected a hyperactivity of the sympathetic nervous system instead that a direct effect of thyroid hormones. Nevertheless, the diagnosis of hyperthyroidism should always be considered in patients with palpitations, including those with signs of preexcitations, since treatment of the thyrotoxicosis could result in possible cure of the arrhythmia.
A Case of Struma Ovarii and Coexisting Graves' Disease
Thyroid Diseases Saturday Poster Clinical
A 46 year old female presented with a pelvic swelling. CT imaging of her abdomen and pelvis revealed a complex pelvic mass of uncertain etiology and she underwent an uncomplicated total hysterectomy and bilateral oophrectomy. Histological examination demonstrated one ovary as a mature monodermal teratoma composed entirely of thyroid tissue (struma ovarii. Post-operatively she was noted to have persistent tachycardia and on questioning admitted to an awareness of palpitations for 5 weeks. On examination she was found to be mildly hyperthyroid with no palpable goitre, lymphadenopathy or evidence of thyroid eye disease. Thyroid function tests confirmed hyperthyroidism with a TSH < 0.03 miU/l and serum free T4 and free T3 concentrations of 61.6 and 13.4 pmol/l respectively. The presence of hyperthyroidism raised the possibility of either functional metastases or co-existing Graves' disease.
Further histological examination of the ovary, technetium scan of the thyroid and TSH receptor autoantibodies were performed.
The histological sample was reviewed and was confirmed to be benign. A technetium scan of her thyroid revealed a bi-lobed gland with diffuse raised uptake into both lobes with a 20 minute uptake of 6.6% (normal < 3%). In addition, her TSH receptor antibodies were positive, confirming the diagnosis of co-existing Graves' disease. She was treated with a block and replace regimen of carbimazole and thyroxine for a period of 6 months and three months after stopping her antithyroid medication is clinically and biochemically euthyroid.
Most cases of struma ovarii are benign although malignancy may be present. Hyperthyroidism may occur due to coexisting Graves' disease or the presence of functioning metastases in malignant struma ovarii. This case demonstrates a rare finding of coexisting benign struma ovarii and Graves' disease and highlights the need for considering the possibility of coexisting hyperthyroidism in patients with struma ovarii and performing appropriate investigations to determine its underlying cause.
Significance of Changes of Serum FT3, FT4, S-TSH, TRA, TPO-AB Levels before and after 131I Treatment in Patients of Different Dietary Habits with Graves' Disease
Thyroid Diseases Saturday Poster Clinical
To study the iodine effect on thyroid function and immunoreaction in people on different iodide intake.
Patients 159 patients proven GD disease that recepted 131I treatment were enrolled. Patients were divided into three groups, group of having seafood habits, group of having animal foods habits, group of having Plant habits The paper investigation 1 age, gender, address, etc 2 Nutrition Survey: The human body needs at least 60 μg–100 μg iodine a day. The supply of iodine should be 100 μg − 200 μg. Due to the diversity complexity of the foods, according to the iodine healthy people need daily and iodine content of various types of food, evaluate the iodine intake of the patients. Statistical Analysis Using statistical software SSPS11.0. FT3; FT4; 2h, 24h RAIU and T/NT value is normal distribution, using X ± S. A student's t-test used to compare the groups. TSH, TPOAb, TGAb are non-normal distribution, using median and quartile distance, Rank sum test was used. Chi-square or Fisher test was also used.
1 2h, 24h RAIU is normal distribution,using X ± S, The results showed that 2h, 24h RAIU is reduced with the increase in iodine intake. G1 and G3 group, G2 and G3 group, G1 and G2 group, 2h and 24 RAIU was significant. (P < 0.05). 2 TRAb positive rate of Groups before treatment were 98%, 96%, 94%. There was not significant difference between groups. TPOAb positive rate of G1, G2 and G3 Group before treatment were 80%, 88%, 86%. There was not significant difference between each group. 3 There was 23 cases in G1 group, 26 in G2 group, 31 in G3 group which have complete information before and after 131I treatment. Each group of FT3, FT4 values have a clear statistical significance before and after 131I treatment, 4 The early Hypothyroidism rate of each Group were 30.4%, 30.7%, 43.8%. There is no difference in groups. (P > 0.05) 1 patients from Foshan region have eating fish habits, 2 131I treatment is one of the effective means. 3 80–90% of hyperthyroid patients with TRAb,TPOAb is positive, 4 there was an trend that early Hypothyroidism rate was increasing.
Post-Partum Thyroiditis with Myxedema Madness
Thyroid Diseases Saturday Poster Clinical
A 39 year old woman, with a 2 year history of Hashimoto's disease and prior history of psychosis, presented with 4th episode of psychosis with thyroiditis,6 months post-partum.
1st episode-post 9/11/01-patient presented with delusions, agitation, memory loss, wandering the streets and difficulty sleeping, and was found to have profound hypothyroidism.rx: thyroxine and SSRI 2nd episode-after father died 2005 stopped taking thyroid medication and became profoundly hypothyroid, with agitation and hallucinations, treated with SSRI 3rd episode 2006-milder episode 10/07 euthyroid on thyroxine during pregnancy 2/08 Delivery by C/S 8/08 Menses returned despite daily nursing 1x/d 9/08 6 months post-partum profound hypothyroidism (T4 0.7, TSH 53) delusional, hallucinations, delirium, paranoia, grandiosity, abnormal appetite, sleep disorder, weight gain 40–50 lbs.
Non-contrast CT brain, MRI brain normal. TPO Ab < 10, Anti-TG Ab + 129 (normal 0–100), TBII 8.0 normal < 16). wbc 13.7 11,300 neutrophils. Patient treated with olanzepine, Lamictal, L thyroxine, triiodothyronine with recovery.
Post-partum thyroiditis may present as “myxedema madness” in a predisposed individual, with prior history of psychotic episodes linked to bipolar disorder and profound hypothyroidism.
Ordway Research Institute , Albany, NY
Thyroid Hormone Action Saturday Poster Basic
Tetraiodothyroacetic acid (tetrac) is a ligand of the thyroid hormone receptor on integrin αvβ3. At this receptor site, tetrac blocks actions of L-thyroxine (T4) and 3, 5, 3′-triiodo-L-thyronine (T3) on tumor cell proliferation (HY Lin et al., Am J Physiol Cell Physiol 296:C9980–991, 2009) and on angiogenesis. The tetrac-targeted integrin is found primarily on cancer cells and on endothelial and vascular smooth muscle cells. Covalently-bound to a poly (lactide-co-glycolide) nanoparticle, tetrac does not gain access to the cell interior and acts exclusively at the plasma membrane integrin receptor.
We explored the possibility that tetrac and nanoparticulate tetrac (tetrac NP), in the absence of T4 and T3, affected gene expression in cancer cells according to an anti-proliferative, anti-angiogenic formula. ERα-negative MDA-MB-231 human breast cancer cells, in which we have shown tetrac to be anti-proliferative, were exposed to tetrac (10−7 M) and tetrac NP (10−7) M tetrac equivalent) in hormone-stripped serum for 24 h. Expression of ∼54,000 transcripts was analyzed in control and drug-treated cultures, using Affymetrix Human Genome U133 plus 2.0 microarrays. Subsequent analysis was focused on genes affected by treatment at P < 0.01.
There was 93% concordance between tetrac and tetrac NP in terms of genes affected. Where there was coherence, tetrac NP was more potent that tetrac. Thrombospondin is a potent anti-angiogenic protein that is often underexpressed in human cancers. Underexpressed in MDA-MB-231 cells, the thrombospondin gene was strongly induced by tetrac NP and tetrac. Expression of apoptosis effector caspase-2 was induced, whereas expression of apoptosis inhibitor XIAP was repressed. CBY1 is a potent inhibitor of β-catenin and the Wnt/β-catenin system is a major survival pathway in cancer cells. CBY1 expression was induced by tetrac and tetrac NP.
In summary, the actions of tetrac and, particularly, tetrac NP on thrombospondin, caspase-2, XIAP and CBY1 gene expression in MDA-MB-231 cells yield a desirable anti-proliferative, anti-angiogenic and pro-apoptotic therapeutic blueprint.
Department of Surgery, University “G. D'Annunzio” , Chieti, Italy
Thyroid Hormone Action Saturday Poster Clinical
Hypocalcemia is the major complication after total thyroidectomy (TT), presenting phenomena which can delay or complicate timely patient discharge. We prospectively evaluated the value of PTH measured at different times after TT in order to determine which was the best predictor for post-surgery hypocalcemia.
Sixty-five consecutive patients (14 (21%) men and 51 (79%) women, mean age 44 years) who had undergone TT for benign pathologies were enrolled. PTH was measured prior to surgery and one, six and 24 hours after surgery. Hypocalcemia was defined as a calcemia under the threshold of 8.0 mg/dL. Differences in gender distribution and age between the normocalcemic and hypocalcemic groups were tested using Fisher's Exact test and Student's t-Test, respectively. ROC analysis was used to evaluate the Area Under Curve (AUC), sensibility and specificity of the four PTH measurements for the occurrence of hypocalcemia.
ROC curves of PTH measurements at the four time points for determining hypocalcemia.
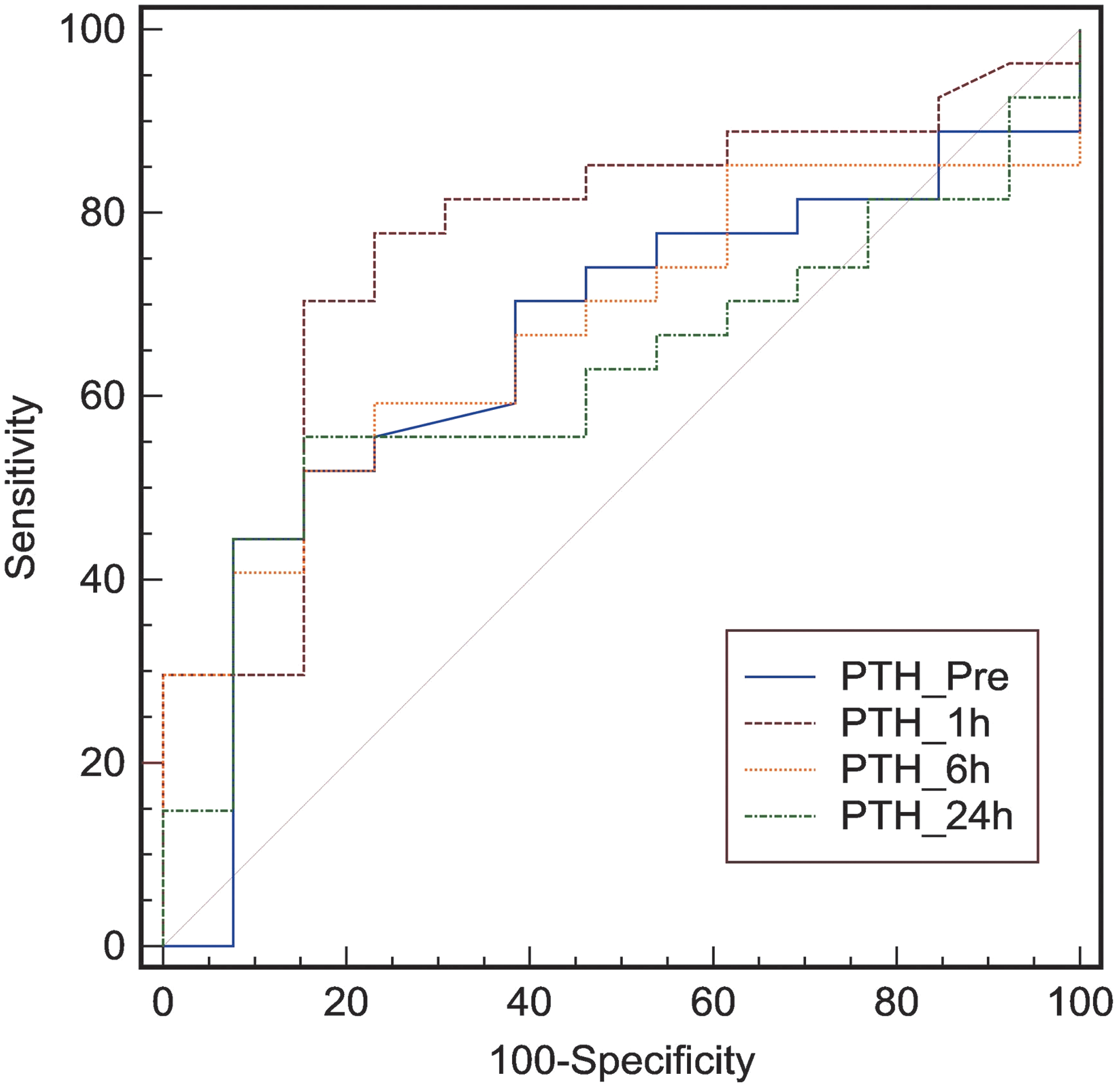
Thirty (46%) patients presented episodes of hypocalcemia: only 12 (18%) with clinical symptoms. The two groups did not present differences in gender or age. Only the PTH measured one-hour after TT yielded a statistically significant AUC (0.0654; p = 0.03; 95% CI: 0.519–0.733) at a cut-off of 39.8. This result was confirmed using Pearson's Chi-Squared Test (p = 0.001).
A value of PTH less than 40 pg/dl one hour after TT is predictive for hypocalcemia, which when present indicates that supplemental therapy should be implemented in order to favor a timely discharge.
Laboratory of Endocrine Neurobiology, Institute of Experimental Medicine , Hungarian Academy of Sciences, Budapest, Hungary
Thyroid Hormone Metabolism and Regulation Saturday Poster Basic
Thyroid hormone- and liver X-receptors (LXR) are master regulators of lipid metabolism. Both receptors can heterodimerize with RXR and thus signaling through both pathways is influenced by retinoic acid (RA). A double LXR knock-out mouse is resistant to Western diet-induced obesity and exhibit ectopic liver expression of the thyroid hormone activating type 2 deiodinase (D2). Notably, D2 is not normally expressed in the mammalian liver, and thus we hypothesized that the LXR/RXR signaling pathways inhibit hepatic D2 expression.
We studied the human dio2 promoter (hdio2) in human hepatic HepG2 cells using the 6.9 kb 5′ FR cloned upstream of a luciferase expression vector. We also studied the chicken dio2 promoter (cdio2) given that, in contrast to mice, chicken liver normally expresses D2.
22(R)-OH-cholesterol negatively regulated the hdio2 promoter in a dose dependent manner (100 uM, ∼2-fold), while it failed affect cdio2. A series of truncations in the hdio2 promoter identified the region −117 to −3.9 kb as critically necessary for the negative regulation to occur.
Furthermore, RA also negative regulated hdio2 (1 uM, ∼4-fold) in a dose-dependent manner while co-expression of the inactive mutant RXR abolished this effect. It is unlikely that RXR homodimers are mediating these changes in dio2 expression given that mutagenesis of the −506 DR1site in hdio2 6.9 kb 5′ FR did not interfere with the RA effects.
Our data indicate that hdio2 expression is negatively regulated by LXR/RXR at the transcriptional level. In vivo, the cholesterol/RA inhibition of D2-mediated T3 production could function as a negative feedback loop given that T3 decreases hepatic cholesterol levels.
Impact of Prescription Drugs on Thyroid Physiology and Thyroid Hormone Therapy: A Comprehensive Literature Review
Thyroid Hormone Metabolism and Regulation Saturday Poster Clinical
Thyroid dysfunction ranks among the most prevalent metabolic derangements, and thyroid hormone preparations are among the most commonly prescribed medications. Medical literature abounds with reports of drugs interacting with thyroid gland regulation and function, and thyroid hormone absorption, transport, and clearance. Although a few drugs have been studied extensively, evidence implicating others has been weaker.
We conducted a comprehensive search of MEDLINE for manuscripts published between 1990 and 2008 describing effects of FDA-approved drugs on thyroid physiology, thyroid hormone therapy, and thyroid function tests in man. We categorized the reported drug interactions and assessed the strength of supporting evidence according to USPSTF-proposed guidelines.
Based on review of 37,170 citations, we identified 416 describing relevant interactions with 176 pharmaceutical agents. Many drugs were noted to have multiple effects, with the following number of references to these modes of interference: hypothalamic-pituitary function (82; 19.7%); iodine handling (24; 5.8%); and thyroid hormone synthesis (45; 10.8%), bioavailability (39; 9.4%), deiodination (46; 11%), and degradation (40; 9.6%). Direct and TBG level-mediated drug interactions with thyroid hormone therapy were reported in 52 (12.5%) and 33 (7.9%) studies, respectively. Isolated interference with thyroid function tests was detected in 27 studies (9.6%). Only 39 (9.4%) were deemed insignificant. The levels of supporting evidence ranged from placebo-controlled studies in 14% (level I) and prospective interventional studies in 38.8% (level II) to purely observational data in 19% (levels III and IV). Relevant in vitro studies comprised 9.8%.
A large number of FDA-approved drugs have been implicated as altering thyroid gland function, hormone homeostasis, and therapy, as well as thyroid function tests. Many of these effects are clinically significant. A comprehensive and critical review of recent literature describing these drug interactions has identified a variety of potential mechanisms and a spectrum of supporting evidence validity. The medical community would benefit from creation and maintenance of an up-to-date database of such agents.
Radiology, New York University School of Medicine , New York, NY
Thyroid Imaging Saturday Poster Clinical
Atypical or cryptic findings on planar I-131 whole body scans (WBS) may result in an “educated guess” approach to interpretation and can cause dilemmas in patient management. Therefore I-131 therapy may be administered needlessly. New imaging technology combining I-131 single photon emission computed tomography (SPECT) and computed tomography (CT) allows fusion of functional and anatomic images (SPECT/CT).
Sixteen post-thyroidectomy thyroid cancer patients were reviewed in whom an I-131 SPECT/CT was performed because of cryptic or atypical findings on WBS.
Examples of ways in which the SPECT/CT scans contributed to the interpretation of the WBS as well as patient management included identification of: a) physiologic inorganic I-131 iodide or I-131 labeled T-4 in the circulation and I-131 iodide in the breasts; b) I-131 activity in the head due to localization of I-131 in periodontal disease; c) I-131 accumulation in an extremity due to a soft tissue infection that had been suspected as a bone metastasis; d) pelvic activity from physiologic blood flow in menstrual blood, a vascular lesion (uterine fibroid), and thyroid tissue in a struma ovarii (to the exclusion of bladder urine, rectosigmoid fecal excretion or bone lesion).
In thyroidectimized thyroid cancer patients, uptake of I-131 on WBS that is not clearly attributable to physiologic anatomic sites is usually treated with I-131. We demonstrate that SPECT/CT can disclose that some cryptic uptake sites are not metastases and instead represent benign accumulations of I-131 iodide or I-131 labeled thyroxin. SPECT/CT has the potential to spare patients from unnecessary I-131 therapy.
Section of Endocrinology, Ospedale Israelitico , Rome, Italy
Thyroid Imaging Saturday Poster Clinical
Few papers have shown that a hypoechoic appearance of the thyroid gland at ultrasonography (US) is related to a hypofunction and serum positivity of thyroid antibodies (T-Ab). However, it is not ascertained if normal thyroid morphology and appearance at US correspond to normal thyroid laboratory tests. The aim of this study was to assess the value of normal thyroid at US in predicting normal thyroid hormones and negative T-Ab in a cohort of adult patients.
All patients (37 females and 11 males) were referred to our hospital to undergo their first thyroid US examination, followed by a thyroid function evaluation. All subjects had normal thyroid gland at US. As a control group 65 patients with hypoechoic and inhomogeneous thyroid gland were enrolled.
All 48 patients had normal free-T3 and free-T4 levels. While 41 patients (85.4%) showed normal TSH, in 7 subjects (14.6%) TSH was elevated and a significant (p < 0.001) difference was recorded between the two groups in mean TSH value. Positive T-Ab value was found in 5 patients (10.4%) and the remaining 43 patients (89.6%) had negative T-Ab. TSH was not significantly correlated with age, thyroid volume or BMI. The multivariate model showed that only BMI was significantly correlated to thyroid volume (p < 0.01, r2 = 0.31).
These results showed that normal thyroid recorded by US matches with normal thyroid laboratory assessment to a large degree. These preliminary data need to be confirmed in a prospective study and in a larger series and should suggest the evaluation of thyrotropin and thyroid antibodies in subjects with normal thyroid gland as assessed by US.
Department of Surgery, Massachusetts General Hospital , Boston, MA
Thyroid Imaging Saturday Poster Clinical
Cytology alone is insufficient to differentiate adenoma from carcinoma in thyroid nodules categorized as suspicious for a follicular neoplasm. Vascular flow within the nodule as measured by Doppler ultrasound has been shown to be predictive of malignancy. Our aim was to identify specific Doppler ultrasound vascular and velocimetric patterns that predict malignancy and to measure the inter observer agreement in interpreting vascular flow patterns within follicular neoplasms.
A high resolution pulsed power Doppler and B mode ultrasound was performed prospectively on forty thyroid nodules (n = 40) that on cytology were suspicious for follicular neoplasms. Twelve variables were recorded (Table 1). Each scan was read individually by two radiologists blinded to the original interpretation and final diagnosis. Correlation with final pathology was done for all 40 nodules.
Variables Measured Using Color Doppler and B Mode Ultrasound
Of 40 nodules, 4 were malignant (10%) and 36 (90%) were benign. With regards to graded flow, low or high central flow (Grade 3 and 4 respectively) was demonstrated in 38 nodules (95%); the 2 nodules with peripheral flow only (grade 2) were both benign. The weighted kappa coefficient measuring inter observer agreement in grading flow was 0.37 (values < 0.40 represent poor agreement beyond chance). The mean peak systolic flow was 71.7 cm/sec for malignant and 46.2 cm/sec for benign nodules; this difference neared statistical significance (p value = 0.06). Benign and malignant nodules did not differ significantly with respect to the other variables measured.
The subjective assessment of vascular flow in follicular neoplasms is unlikely to be beneficial, as the majority of both benign and malignant nodules demonstrate central flow and the grading system inevitably is subject to inter observer variability. Objective measures of vascularity such as peak flow velocity may have greater value in identifying malignant nodules and hence determining the necessity and extent of surgery.
Thyroid Nodules and Goiter Saturday Poster Clinical
The aim of this study was to establish pretreatment factors affecting the results of radioactive iodine (RAI) treatment on patients with hyperthyroidism caused by autonomous function thyroid nodule (AFTN).
We retrospectively analyzed AFTN patients with RAI between 2000 and 2008. 113 patients (26 male, 87 female) with hyperthyroidism caused by AFTN were entered in the study and followed up until 12 months after therapy. All patients received RAI based on size, age and clinical findings. The activity dose was calculated by the use of Marinelli's formula. The absorbed dose was 300Gy. Patients clinical status and thyroid hormone levels were evaluated 3, 6, 9 and 12 months after treatment.
When analyzing possible factors affecting post-therapeutic outcome, the incidence of therapy success rate was not significantly associated with age, sex, BMI, nodule size and hyperthyroidism severity (P > 0.05), additionally analysis showed lower probability of treatment success in patients with anti-thyroid drugs (P < 0.01).
131I therapy is a simple, safe, effective and economical treatment of AFTN diseases. In AFTN patients, anti-thyroid medication tended to reduce the therapeutic efficacy. Those patients might need higher 131I doses.
Department of Endocrinology, Sahlgrenska Academy at University of Gothenburg , Gothenburg, Sweden
Thyroid Nodules and Goiter Saturday Poster Clinical
Before introducing a salt iodization program in 1936, goiter was prevalent in Sweden in the inland and across the northern coast of the Baltic Sea. This is the first national surveillance study of iodine status in Sweden (“Swejod”) that infer an adequate level of urinary iodine concentration (UIC) (125 ug/L) according to recommendations by WHO. Thyroid volumes (TV) also reflect the iodine status in a population and are now reported for school children.
A stratified probability proportionate to size cluster sampling method was used to obtain a representative national sample of school children aged 6–12 years from 30 clusters. TV, in millilitres (mL), was calculated according to Brunn et al from the length, width and thickness of each thyroid lobe estimated by a portable echocamera (Aloka SSD-900). The median TV was compared to two previous studies: the international reference standard (Zimmermann, 2004) and a local Swedish survey from the region of Malmö (Svensson, 2004). In addition, the prevalence of enlarged thyroid glands (goiter) defined as TV > 97.5 percentile of the studies of Zimmermann was calculated.
No correlation between UIC and TV was detected but TV correlated to age, body surface area (BSA), weight, height and BMI. The median TV was higher in Swejod than in the two other studies, p < 0.0001. The prevalence of goiter was higher in Swejod than in the study from Zimmerman in relation to age (22.3 vs 2.5%), BSA (15.7 vs 2.5%), weight (17.6 vs 2.5%), height (12.9 vs 2.5%), p < 0.0001 for all.
The Swedish urinary iodine concentration is within the range 100–199 ug/L recommended by WHO to indicate iodine sufficiency in a population. However, thyroid volumes were larger in Swedish school children than in an international reference survey and the prevalence of goiter, as defined from WHO standards, was higher.
Effect of Thyroid Nodules on Preoperative Localization of Primary Hyperparathyroidism
Thyroid Nodules and Goiter Saturday Poster Clinical
Primary hyperparathyroidism (pHPT) is a common endocrine disease, as is nodular goiter. The aim of this study was to evaluate the effect of the presence of thyroid nodule on the sensitivity of sestamibi scintigraphy (MIBI) in patients with parathyroid adenoma.
Two hundred and forty five patients with pHPT who underwent parathyroidectomy were included in the study. High frequency ultrasonography (US) and sestamibi scintigraphy (MIBI) were performed in all patients. Volumes of thyroid lobes and nodules and number of nodules were evaluated.
Of the 245 cases 80,8% was female and 19,2% was male. Of the 245 patients who underwent surgery 225 had adenoma, 4 had hyperplasia and another 4 had carcinoma while 12 cases had no lesions. Two cases had bilateral lesions. Abnormal parathyroid gland could be localized preoperatively in 224 of the cases with ultrasonography, while only in 144 cases with the MIBI-scan. When used together ultrasonography and MIBI-scan could not detect 16 cases. Five of the cases not detected by ultrasonography could be visualized by MIBI-scan. Fifty four of the 85 cases detected with US but not visualized by MIBI-scan had thyroid nodules. The presence and number of thyroid nodules were significantly higher in MIBI-scan unvisualized 101 patients than MIBI-scan visualized 144 cases (p = 0,037); and there was no difference with regard to either ipsilateral thyroid lobe involvement or nodule volume. Volume of the parathyroid adenoma was significantly less in MIBI-scan unvisualized patients (p < 0.001). Sensitivity and specificity of US was 93,6% and 66,7% while corresponding figures for MIBI-scan were 60,17% and 77,7%, respectively.
Our results suggest that ultrasonography has high sensitivity in the detection of parathyroid adenomas, and sensitivity of MIBI-scan decreases in low volume parathyroid adenomas and in the presence of thyroid nodules.
Long-Term Follow-Up of Thyroid Incidentalomas in Elderly Males Over 70 Years Old
Thyroid Nodules and Goiter Saturday Poster Clinical
Retrospectively analyze the onset and development of thyroid incidentalomas in males over 70 years old, in order to provide some practical information. 261 cases were investigated with following up for 0—19 years. The onset year, PE, radiology, thyroid function, concomitant thyroid diseases were recorded.Some sonographic characteristics were analyzed statistically. Other profiles were described.
The incidence is 76.85%,with a trend to be higher. The average onset age is 72.29 ± 8.09, and the range 70—74 possesses the highest proportion. More than 93% glands kept normal in size. 59.39% contained one nodule in the first year, and at last 62.45% were multi-nodular in both lobes. There is statistic significance between the initial and final sizes (P = 0.006). Compared with the onset year, the sizes in the 5th year, 10th year and 15th year are significantly larger respectively (P < 0.05). In 213 nodules followed up for 10 years, the nodules less than 1 cm became larger in the 5th year and the 10th year, and the change in the ones larger than 1 cm is not obvious. However, nodules larger than 1.5 cm become smaller by year. 32 cases were examed by other radiologic methods for 70 times, in which only 32.86% coincided with ultrasonographic reports of the same year. Positive rate of thyroid function test is 16.8%, among which only 7 cases got definite diagnosis (2.68%). No malignance was recorded.
The incidence of thyroid incidentalomas in the elderly males over 70 is high and has a trend to become higher. Most cases may become multi-nodular in both lobes. Observation may be the best treatment the nodules larger than 1 cm in the elderly. It is not necessary to test thyroid function routinely in long-term follow-up. Whether choose tomographic imaging for advanced evaluation is still controversial.
P1 is the comparison between 1st and 5th year; P2 is between 5th and 10th year; P3 is between 1st and 10th year.
Department of Vectorology and Experimental Gene Therapy, University of Rostock , Rostock, Germany
Thyroid Cancer Saturday Oral Basic 1:45 PM
Efficient and specific killing of neoplastic cells, in particular tumor metastases, remains a major challenge of current cancer therapy modalities. Medullary thyroid carcinoma (MTC) based on activating mutations in the RET proto-oncogene, which encodes a receptor tyrosine kinase, is characterized by aggressive growth and early metastasis, and thus represents an attractive model for gene-based therapeutic strategies. A precondition for successfull eradication of speaded tumor cells are cancer targeted gene delivery systems that can be systemically applied. We have previously identified MTC-specific peptides by intravenous injection of a phage display peptide library into RET-C634R transgenic mice carrying orthotopic thyroid tumors.
Here, we chemically linked these peptides to genetically modified (CAR depleted) Ad vectors expressing a dominant-negative truncated form of the receptor (RETDTK), shown to inhibit oncogenic RET autophosphorylation (J Natl Cancer Inst 2004;96; Nat Clin Pract Oncol 2006;3), and analyzed its anticancer capacity compared to AdRETDTK with native tropism and AdGFP linked to specific ligand after systemic vector administration.
Two weeks after virus injection into the tail vein of transgenic mice with growing MTC in their thyroid glands, tumors were strongly reduced in mice treated with specifically-tagged AdRETDTK, whereas the tumor size in mice injected with native AdRETDTK remained stable. In contrast, tumors of mice treated with the AdGFP-peptide-vector continued to grow. Quantitative PCR, Western blotting, and immunohistochemistry of mouse tissues revealed direct binding of the peptide-tagged AdRETDTK to MTC. Biodistribution of the vectors was monitored by in vivo-imaging and intravital microscopy, clearly indicating that gene transfer mediated through peptide-tagged vectors is redirected to neoplastic cells by reducing binding to normal target cells. This suggests that the corresponding receptor is predominantly expressed on cancerous tissue.
Our data indicate that Ad vectors coupled to tumor selective peptides are suitable to improve the efficiency of therapeutic gene transfer to systemic tumor cells, thereby providing the basis for an antimetastatic therapy.
Dept. of Endocrinology, University of Pisa , Pisa, Italy
Thyroid Cancer Saturday Oral Basic 2:00 PM
Medullary Thyroid Carcinoma (MTC) originates from parafollicular C-cells and can be present in sporadic (75%) or familial (25%) form. Germline or somatic activating point mutations of the RET proto-oncogene are present in about 95% of familial and 50% of sporadic tumors. Despite this, about 50% of sporadic MTC remain without apparent oncogenic alteration, although recently, several mechanisms have been suggested. In this study we investigated copy number variations of both RET and chromosome 10 in a large series of hereditary and sporadic MTCs, mutated and not mutated, in order to identify possible alternative mechanisms of RET activation, especially in the RET negative cases.
For this purpose, we studied 63 MTC (13 familial and 50 sporadic): RET mutation analysis on blood and frozen tissue DNA was performed by PCR and sequencing. Gene copy number variation analysis for the RET gene and for chromosome 10 was performed by Fluorescence in situ Hybridization (FISH). Results were finally validated by Real-time PCR gene copy number assay.
A RET germ line mutation was found in 13/13 (100%) familial cases and in 22/50 (44%) sporadic cases. FISH analysis revealed numerical alterations in the RET and/or chromosome 10 ploidy in 18/63 (28.5%) MTC: 4/13 (31%) familial and 14/50 (28%) sporadic MTC (p = NS). Among sporadic MTC, 11/22 (50%) were mutated and 3/28 (10.7%) were not (p < 0.003). The only type of alteration found in familial cases was the RET gene amplification. Data obtained were all confirmed by Real-time PCR analysis.
In conclusion, this large series of MTC showed several numerical alterations either in RET gene or in chromosome 10 and they were significantly more frequent in MTC harbouring a RET mutation. RET activating point mutation might increase the rate of genomic instability causing the alteration of RET gene and chromosome 10 copy number. Moreover, our results demonstrate that RET gene amplification is not an alternative mechanism of RET activation in mutation negative cases.
Dept. of Internal Medicine II, Ludwig-Maximilians-University , Munich, Germany
Iodine Uptake and Metabolism Saturday Oral Basic 2:15 PM
We have recently demonstrated induction of significant tumor-selective iodide uptake activity and therapeutic efficacy of radioiodine in neuroblastoma tumors after systemic sodium iodide symporter (NIS) gene delivery using synthetic non-viral gene delivery vectors. The aim of the current study was to evaluate the efficacy of pseudodentritic oligoamines (G2-HD-OEI) and polyamidoamid dendrimers (PAMAM) for systemic NIS gene transfer in a hepatocellular carcinoma (HCC) mouse model.
For this purpose we used G2-HD-OEI and PAMAM nanoparticle vectors, which are characterized by high intrinsic tumor affinity, to target a NIS-expressing plasmid (CMV-NIS-pcDNA3) to hepatoma (Huh7) cells in vitro and in vivo.
In vitro incubation of Huh7 cells with NIS-conjugated nanoparticles resulted in a 44-fold and 16-fold increase in perchlorate-sensitive iodide uptake activity when using G2-HD-OEI and PAMAM polyplexes, respectively. After establishment of subcutaneous Huh7 tumors in nude mice, NIS-conjugated nanoparticle vectors were injected via the tail vein followed by analysis of radioiodine distribution after i.p. injection of 18.5 MBq 123I using gamma camera imaging. While systemic NIS gene delivery using PAMAM vectors did not result in specific iodide accumulation in HCC tumors, Huh7 tumors showed a perchlorate-sensitive iodide uptake of 9–14% ID/g 123I with a biological half-life of approximately 13 h after systemic NIS gene transfer using G2-HD-OEI polyplexes. In addition, tumors transduced with the control vector showed no specific iodide uptake. Non-target organs like liver, lung, and kidneys exhibited only mild or no significant iodide uptake as shown in ex vivo biodistribution experiments.
In conclusion, transduction efficacy and tumor selectivity of different dendrimeric polymers can vary in different tumor models and therefore have to be evaluated individually. After individual optimization, our results clearly demonstrate the feasibility of systemic NIS gene transfer using non-viral dendritic nanoparticle vectors in HCC followed by targeted NIS-mediated radionuclide therapy.
Dept. of Internal Medicine II, Ludwig-Maximilians-University , Munich, Germany
Iodine Uptake and Metabolism Saturday Oral Basic 2:30 PM
We have recently reported mammary radioiodine accumulation due to functional sodium iodide symporter (NIS) expression in a benign fibroadenoma. These data showed for the first time that functional NIS expression is not restricted to the lactating mammary gland and malignant breast tissue, but can also be detected in benign breast lesions such as fibroadenoma. To elucidate the frequency of NIS expression in benign fibroadenomas of the breast we performed an immunohistochemical study on NIS protein expression in a series of human fibroadenomas.
46 paraffin-embedded fibroadenomas of the breast and 15 normal breast tissue samples (controls) were stained with a mouse monoclonal human NIS antibody and analyzed independently by two experienced pathologists. Levels and localization of NIS expression were evaluated and indicated in four different grades ranging from absent (−) to strong (+++) immunoreactivity. Specimens which exhibited exclusively nuclear NIS staining were considered to be negative.
While all control samples showed no NIS-specific immunostaining, 76% of the analyzed fibroadenomas revealed significant NIS-immunoreactivity with prominent membrane-associated staining in approximately 50%. Moreover, 14 (40%) of the NIS-positive fibroadenomas showed a moderate (++ ) or strong (+++) NIS immunostain-ing. Throughout the series, normal breast or fibrous tissue showed no specific immunostaining in accordance with restriction of NIS expression to the mammary epithelial cells of fibroadeomatous lesions.
In conclusion, this study demonstrates for the first time that significant NIS protein expression is frequently upregulated not only in malignant breast tissue but also in benign fibroadenomas of the breast.
Treatment of Graves Ophthalmopathy with an Antagonist of PPAR-Gamma: A Pilot Study
Thyroid Diseases Saturday Oral Clinical 1:45 PM
Expression of PPAR-gamma( Pg) is significantly increased in the orbital fibro-adipose tissue of active Graves ophthalmopathy (GO). Otherwise agonist use of Pg was considered in developing or worsening GO.OBJECTIVE-The aim of this preliminary report is to evaluate the use of an antagonist of the Pg in the treatment of selected GO.
Thirteen patients without ocular treatment 3 months before the inclusion in this research and classified by CAS index between 2 to 7 from 24 to 66 years old (mean 42.7 ± 14,8), 7 females were selected. Seven patients had hyperthyroidism, 3 hypothyroidism and 3 euthyroidism. The GO duration ranged from 4 to 60 months (mean 31.1 ± 16.9). restriction of each extra-ocular muscle was evaluated by scores from 0 to 4. Total eye muscles scores, proptosis, diplopia and CAS were compared before and after treatment. Sodium Diclofenac an antagonist of Pg was administered orally 50 mg every 12 hours for 6.8 ± 3.6 months. Blood counts and renal function were checked during the treatment. Ointments and lubrication eye drops were administered to all patients.
(table) Ocular pain vanished in 5 of 6 patients. Diplopia disappeared in 4 of 5 individuals and improved in 1.The mean of the total muscle restriction scores decreased significantly from 5.23 ±4.34 to 3.38 ± 4.53. Proptosis unchanged: right eye: 26.04 ± 4.20 to 25.08 ± 3.60 and left eye 23.38 ± 3.57 to 23.00 ± 3.67. The improvement of the CAS index was also significant: 3.61 ± 1.44 and 2.30 ± 1.03 before and after treatment respectively. Only one patient complained of resistant gastric pain relieved by increasing omeprazol dosage.
Mean of the total eye muscle scores restriction.
Mean.
Mean of clinical activity score.
The excellent improvement of ocular pain and relief in diplopia and significant decrease in the CAS index and muscle restriction if confirmed in a greater number of patients may be a safe and less expensive treatment to these uncomfortable symptoms of GO and avoid the many adverse effects of corticosteroids or orbital radiotherapy.
Thyroid Cancer Saturday Oral Clinical 2:00 PM
In rodents, glucagon-like peptide-1 (GLP-1) receptor agonists, acting via the GLP-1 receptor, stimulate calcitonin release. Continuous calcitonin release has been associated with mRNA up-regulation, C-cell proliferation and tumor formation in rodents. Contrary to its effects in rodents, GLP-1 does not appear to activate the nonhuman primate C-cell or human TT C-cell line. The clinical significance of these findings was explored through comprehensive serum calcitonin screening in patients with T2D (or obesity) receiving the investigational human GLP-1 receptor agonist liraglutide.
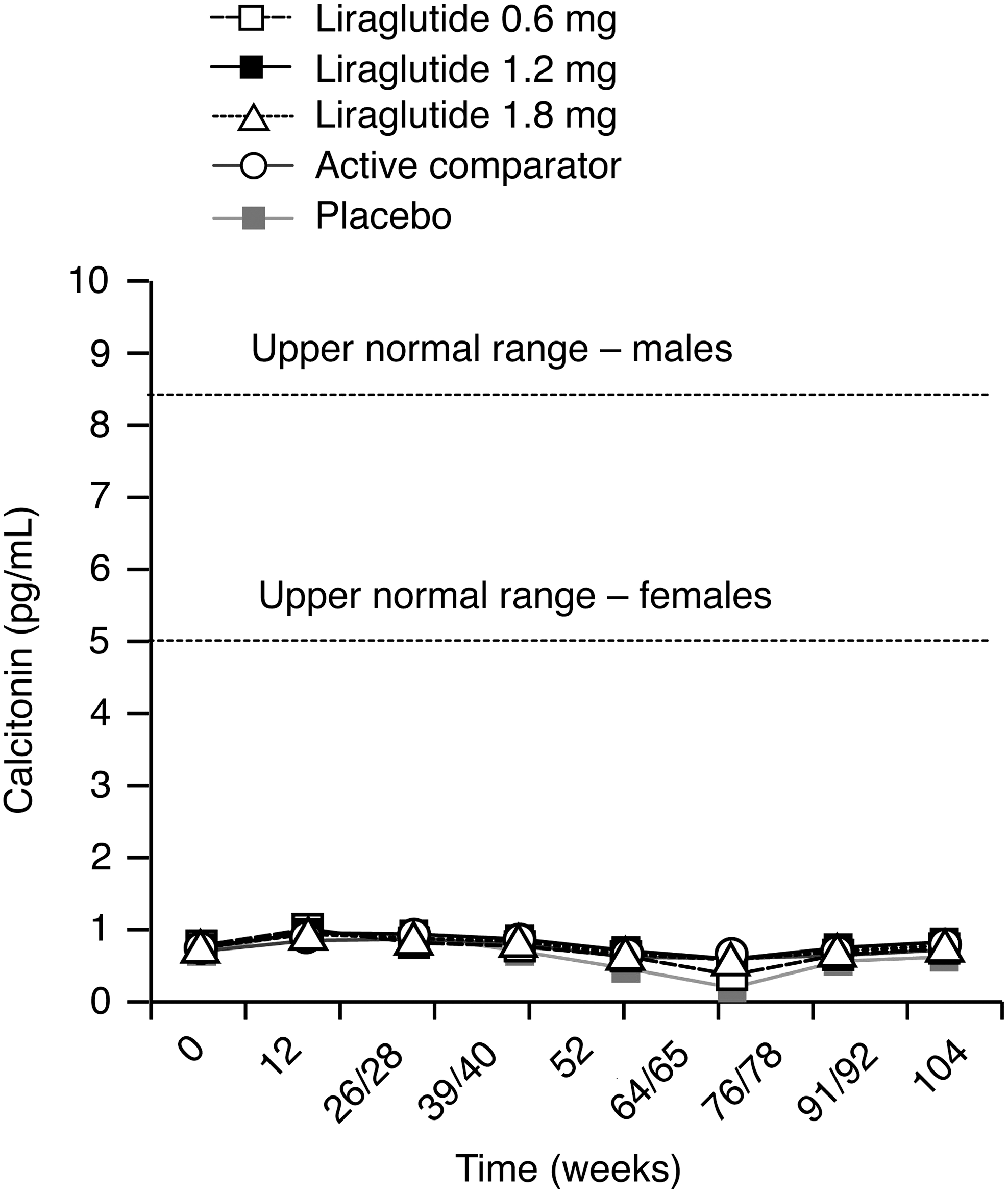
Unstimulated (basal) calcitonin levels remained low throughout the 2-year trials and were similar between treatments.
During the phase 3 clinical development program for liraglutide, unstimulated serum calcitonin levels were measured at 3-month intervals for up to 2 years in 5002 patients receiving liraglutide or control therapy. Calcitonin was measured using a highly specific chemiluminescent enzyme immunoassay (Immunolite; lower limit of quantification, 0.7 pg/mL). The normal range upper limit for women was 5 pg/mL, 8.4 pg/mL for men. Also, 85 patients underwent calcium stimulation tests to further examine a potential calcitonin response to GLP-1.
Basal (geometric) mean calcitonin levels were at the low end of normal range in all treatment groups throughout the trials. Over 2 years, geometric mean values were <1.0 pg/mL, well below upper normal ranges (Fig. 1). Proportion of patients moving above a clinically relevant cut-off of 20 pg/mL was very low in all groups with no difference between treatments and no consistent dose or time-dependent relationship. EOT calcium stimulation testing showed no significant difference between treatments in mean peak/basal ratio of stimulated calcitonin levels (ratio range 9.4–10.5) or mean peak calcitonin levels (mean value range 11.1–14.8 pg/mL).
GLP-1 receptor agonists in humans do not appear to activate C-cell secretory activity. Calcitonin levels followed serially in humans with T2D are low and show no pattern of change. These data do not support any significant risk for activation or growth of C-cells in humans in response to liraglutide and theoretically other GLP-1 receptor agonists.
Thyroid Diseases Saturday Oral Clinical 2:15 PM
Invasive fibrous thyroiditis (IFT), also known as Riedel's thyroiditis, is the rarest form of thyroiditis. In this report, we summarize our experience with all cases of IFT evaluated at our institution since 1976.
Mayo Clinic archives were searched for all cases of IFT seen between 1976 and 2008. Inclusion criteria were: reviewed pathology at our institution and confirmation of extension of fibrosis outside of thyroid capsule. Out of 37 patients with diagnosis 16 were excluded after review because of questionable clinical or pathological diagnosis. 21 qualified for this report.
Mean age was 42. 17(81%) were female. Presenting symptoms included pain (24%), dysphagia (33%), vocal cord dysfunction (29%), tracheal narrowing (48%). 3 had associated hypoparathyroidism. 16 (76%) had history of tobacco use and 10(48%) were current smokers. 7 patients had imaging evidence of major neck blood vessel involvement. Fibrosing mediastinitis was present in 4, orbital fibrosis in 1, retroperitoneal fibrosis in 3 and pancreatic fibrosis in 1. One had Graves' ophthalmopathy and another Graves' hyperthyroidism. 2 had hydrocephalus. 18 had partial thyroidectomy, 7 (39%) of those had surgical complications involving vocal cord and parathyroid. 2 required tracheostomy. 13 had corticosteroid therapy with mean dose of 73 mg and mean duration of 163 days. Six received tamoxifen. Retrospective nature of the study limited assessment of effect of therapies.
1-IFT is associated with systemic extra-cervical fibrotic process in 38%. 2-Association of IFT with tobacco abuse (76%) is of interest and contrasts with our previous report of 21% in Hashimoto thyroiditis. 3-Attempt at thyroidectomy is associated with high degree of surgical complications and should be approached with caution. 4-Standard medical therapy includes corticosteroids and tamoxifen. 5-Rretrospective studies have limitations for evaluation of effectiveness of medical therapies.
Video-Assisted Thyroidectomy: Lesson Learned After More Than 1300 Procedures
Thyroid Diseases Saturday Oral Clinical 2:30 PM
Video-assisted thyroidectomy (VAT) presents significant advantages over conventional surgery (CS) in terms of postoperative pain, cosmetic result and operative outcome. Patients eligibility and learning curve are still regarded as a main limitation of VAT. We reviewed our series of more than 1300 procedures to determine the impact of experience on patients selection and surgical outcome.
One thousand three hundred and fifty-six patients underwent 1370 VAT. They were divided in four groups according to the 36-months period they were performed: Group A (June 1998-May 2001), Group B (June 2001-May 2004), Group C (June 2004-May 2007), Group D (June 2007-May 2009). A comparative analysis of the four groups was performed.
Group A included 38 patients, Group B 194, Group C 639 and Group D 499. The number of VATs performed per month increased over the time (1.0/month for period A, 5.3/month for B, 17.7/month for C, 20.8/month for D), as well as the percentage of patients undergoing thyroidectomy selected for VAT (6.0%Vs17.8%Vs25.3%Vs29.2%). No significant difference was found concerning age, gender, preoperative diagnosis, nodule size, complication rate, postoperative stay and final histology. The lobectomy/total thyroidectomy rate was significantly lower in Group D (12/393) than in Group A (7/29), Group B (54/133) and C (44/593) (P < 0.05, respectively). Mean thyroid weight were significantly larger in Group D (25.9+/−23.8 g) and in Group C (24.5+/−14.6 g) than in Group A (13.7+/−7.8) and Group B (21.7+/−12.3) (P < 0.05). Operative time was significantly shorter in Group D (51.9+/−17.3 min) and Group C (64.1+/−22.3 min) than in Group A (101.8+/−32.3) and Group B (68.2+/−22.1) (P < 0.05, respectively). Conversion rate significantly decreased over the time (10.5%, 0.5%, 0.2% and 0.1% respectively) (P < 0.05).
The number of patients eligible for VAT increases with experience, while operative time and conversion rate significantly decrease. At present VAT could represent a valid option, even preferable to CS, for treatment of about a quarter of patients who require thyroidectomy.