
Abstract
Background:
Chronic urticaria is a common clinical condition whose etiology, in about 75% of cases, is unknown and is therefore called chronic idiopathic urticaria (CIU). A link between CIU and autoimmune thyroid diseases was proposed several decades ago. Here we review this topic.
Summary:
Several studies have been performed to determine if and to what degree there is an association between CIU and autoimmune thyroid diseases, particularly autoimmune thyroiditis. Many of these studies were not well controlled, however. Approximately one-fourth of CIU patients have serological evidence of thyroid autoimmunity, suggesting that these two disorders are associated. The mechanisms for the apparent association between CIU and serological evidence of thyroid autoimmunity are not clear. There are no data regarding the correlations between CIU and histological features of autoimmune thyroiditis or hypothyroidism. Despite this, there are anecdotal reports regarding L-thyroxine administration in patients with CIU.
Conclusions:
Screening for thyroid autoimmunity is probably useful in patients with CIU. More solid evidence, based on still lacking well-conducted controlled studies, is desirable to determine if there is a therapeutic role for L-thyroxine treatment in ameliorating the skin manifestations of urticaria.
Introduction
It is more helpful to classify urticaria by clinical presentation than by etiology, as the latter is often difficult to establish. Based on a chronologic criterion, urticaria can be classified as acute urticaria when it presents as one or more episodes lasting for 6 weeks or less, or chronic urticaria when daily manifestations last for more than 6 weeks (2,3). A schematic classification of urticaria based on etiology is shown in Table 1 (4). The term “chronic idiopathic urticaria” (CIU) applies when the cause of urticaria remains unknown. This is the case in ∼75% of patients (5). Chronic urticaria affects from 0.5% to 1% (1) to 3% (6) of the population at some time of their lives with a peak occurrence in the middle ages and a preference for female gender (female:male ratio ∼4:1) (7).
Source: Pigatto and Valsecchi, 2002 (4).
Antibodies against IgE or the high-affinity receptor for IgE are present in 45% to 55% of patients with CIU (8). The basophil histamine release testing or basophils activation test has been used to measure antibodies to FcɛRI, FcɛRII, or IgE and identify patients with autoimmune urticaria (9). As positive tests for anti-IgE or anti-FcɛRI antibodies correlate with positive tests for the autologous serum skin test (ASST), a positive test for the ASST is regarded as suggestive of an autoimmune pathogenesis in patients with urticaria (10). The ASST is performed by administering an intradermal injection of 0.05 ml of fresh, undiluted serum obtained by centrifugation of the patient's blood sample. The intradermal injection of 0.05 ml of saline solution is used as control. The test is considered positive when, 30 minutes after injection, a serum-induced red wheal with a diameter of ≥1.5 mm larger than the saline-induced is elicited by autologous serum.
A pathogenetical role for anti-FcɛRI antibodies in chronic urticaria has been hypothesized, as they are able to activate complement, generate C5a, and promote activation of both mast cells and basophils (11).
Several reviews reported that from 10% to 40% of patients with CIU have serum antibodies against the high affinity receptor for IgE (anti-FcɛRI Ab) and serological features of thyroid autoimmunity (12,13). One review (12) concluded that skin manifestations and thyroid autoimmunity “most likely are associated, parallel autoimmune events,” whereas another review concluded that (13) “there are no compelling arguments to decide whether or not thyroid autoimmunity plays a significant role in the pathogenesis of chronic urticaria.” Notably there is a wide range of skin disorders that may be associated with thyroid autoimmunity (14). Here we review the evidence regarding the association between thyroid autoimmunity and urticaria, and consider hypotheses regarding pathogenesis and clinical consequences.
CIU and Hashimoto's Thyroiditis
Almost 30 years ago, Leznoff et al. (15) reported increased serum titers of thyroid microsomal antibodies (TMAb) in 12% of patients with CIU. This rate was twofold greater than the 5.6% rate found in control subjects (Table 2). A subsequent study by the same authors noted positive TMAb and/or thyroglobulin antibodies (TgAb) in 14.4% of patients with CIU and angioedema (16). Subsequent similar studies from several countries have been performed in patients with CIU (Table 2). In these reports, which dealt with adults, positive TgAb, thyroid peroxidase antibodies (TPOAb—we use in this review the acronyms TPOAb and TMAb, which indicate the same variable, depending upon what reported by each author), or antibodies against TSH receptor were noted in 8.5% to 57.4% of patients with CIU (15 –38). Levy et al. (39) (not included in Table 2) studied children and adolescents. In this study of 187 patients with CIU, ranging in age from 7 to 17 years, 8 (4.3%) had positive tests for antibodies against at least one thyroid antigen. All of the eight patients were females. Three were hypothyroid, one of whom had been diagnosed and was taking L-thyroxine (L-T4) replacement therapy (39). Another very recent study from Thailand of 94 children aged 4–15 years with chronic urticaria failed to detect any positive TgAb or TMAb test or abnormal thyroid function (40). It may not be coincidental that the adult study (33) from Thailand appearing in Table 2 reports very low rates of positive tests for antithyroid antibodies. Similar low rates are seen in patients from Brazil and Israel, intermediate rates were found in patients from North America (Canada, USA), whereas high rates are seen in patients from Europe (particularly Portugal and Italy), implying that ethnic factors may contribute to the propensity of forming serum autoantibodies against thyroid autoantigens in CIU patients. The highest rates, just above 50%, were observed in two uncontrolled studies with <50 patients from Italy (28) and Pakistan (37).
References are listed in chronologic order.
Data about positivity for at least one antibody not available.
The studies of Laznoff et al. (16), Collet et al. (17), Gaig et al. (19), Zauli et al. (21), Kikuchi et al. (23), Atta et al. (26), Fusari et al. (29), Fernandez-Romero et al. (30), Kulthanan et al. (33), Najib et al. (36), Aamir et al. (37) and Kessel et al. (38) were disregarded because no control group was studied.
CIU, chronic idiopathic urticaria; TgAb, thyroglobulin antibodies; TMAb, thyroid microsomal antibodies; TPOAb, thyroperoxidase antibodies; TSHRAb, antibodies against TSH receptor.
As depicted in Table 2, several studies of the prevalence of thyroid autoantibodies in CIU lacked control subjects, and/or the number of individuals in the study groups was quite small. These limitations preclude any reliable comparison between different series. Nevertheless, Table 2 clearly shows that the prevalence of positive tests for antithyroid antibodies appears to have progressively increased over the years. In the studies published between 1983 and 2000 (15 –19) the prevalence was 14.1%, in those published between 2001 and 2004 (20 –27) it was 19.2%, and between 2005 and 2010 (28 –38) it was 27%. When the prevalence of positive tests for thyroid antibodies is plotted against the year of publication for the data, there is a direct correlation (r = 0.882, p = 0.00014) (Fig. 1). This is in keeping with the increase in prevalence, or at least detection, of autoimmune thyroiditis and autoimmune disorders in world population (41,42).
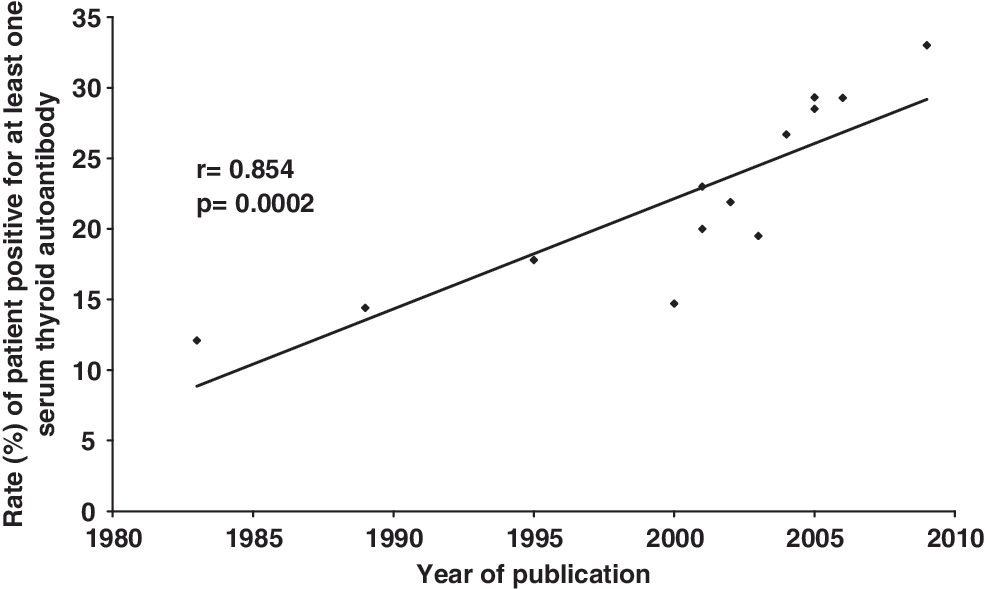
Relationship between the prevalence of positiveness for at least one thyroid autoantibody in patients with chronic idiopathic urticaria, as resulted from the literature reviewed, and the year of publication of the article. Data are from Table 2.
It is likely that there has been a true increase in the prevalence of autoimmune diseases, not simply an improvement in the procedures to ascertain the prevalence of autoimmune diseases. This is suggested by studies by our group in Messina, Italy. In a survey conducted in 2002, the prevalence of positive tests for at least one antithyroid antibody in a group of 62 patients with CIU was 21.9%, a value fivefold greater than control subjects (22); approximately half of these patients (57%) had hypothyroidism and half (43%) were euthyroid. More recently, in 144 patients (95 with CIU and 49 with acute urticaria) hospitalized at the same Division of Allergy and Clinical Immunology, the prevalence of positive tests for at least one antithyroid antibody was 32.6% in the CIU patients and 12.2% in patients with acute urticaria. The prevalence of positive tests in patients with acute urticaria was similar (13%) to that found in 100 healthy blood donors (35). In the later study (35), there was less difference between the prevalence of positive antithyroid antibodies in patients with CIU compared to control subjects than in the earlier study (22). There was about 2.5-fold greater prevalence in the later study compared to a 4.8-fold greater prevalence in the earlier study. Although there were differences in the size of the groups between the two series, we believe that the outcome differences related to the period of recruitment. In the first study (22), patients and control subjects were enrolled in the second half of the 1990s, whereas in the more recent study (35) the subjects were enrolled between 1998 and 2006. The local prevalence of Hashimoto's thyroiditis (HT) progressively increased during the second half of the 1990s (22). This is consistent with the prevalence of positive tests for antithyroid antibodies in control subjects being twofold higher in the later than the earlier study. Notably, the immunometric tests for the measurement of antithyroid antibodies that were used in both studies (22,35) were comparable. Similarly in the 10 case–control studies presented in Table 2, the prevalence of positive antithyroid antibodies in the control groups was 1.8-fold greater (7.6% of a total of 449 individuals vs. 4.2% of a total of 746 individuals) in the years from 2005 to 2010 compared to the years from 1983 to 2004.
The largest subset of patients with urticaria has no known cause for their disorder (i.e., they have CIU). There is little information regarding the prevalence of antithyroid antibodies in patients with identifiable causes of urticaria. In one Italian report (21), 23% of patients with urticaria and an identifiable cause (12 of 52) had a positive test for at least one antithyroid antibody compared to 33% of patients (23 of 70) with CIU (χ 2 = 1.39, p = 0.24). Perhaps, a more powered study would have yielded a statistically significant difference. Nonetheless, the percentage of patients with urticaria that seemed to have an identifiable etiology or trigger who had a positive test for antithyroid antibody seems high. Further studies with adequate power are needed to resolve the question of whether the prevalence of antithyroid antibodies is greater in CIU than in urticaria of known cause and if this prevalence is greater in the latter group than in healthy subjects.
Compared to the many studies dealing with the prevalence of antithyroid antibodies in urticaria, there seems to be less information regarding the prevalence of urticaria in patients with autoimmune thyroid disease. Verneuil et al. (24) compared the frequency of CIU in 32 thyroid autoantibody-positive patients with thyroid diseases [“either a goiter or thyroid nodules and/or hypo- or hyperthyroidism, associated with thyroid autoantibodies—either anti-TG and/or anti-TPO and/or anti-TSH receptor (TSI) antibodies”] and in 22 thyroid autoantibody negative patients with thyroid diseases. All of the patients with thyroid autoantibodies were euthyroid. Although the frequency of thyroid autoantibodies was eightfold higher in CIU than in control subjects (p < 0.01), there was a similar frequency of CIU in patients with thyroid diseases, regardless of the results of tests for thyroid autoantibodies (12.4% in patients with positive tests of at least one thyroid antibody and 9.1% in thyroid antibody negative patients) (24). Feibelmann et al. (34) reported a similar, quite low prevalence of CIU in patients with autoimmune versus nonautoimmune thyroid disease (3.3% vs. 3.4%, respectively). They also reported a 12.2% prevalence of positive tests for at least one thyroid autoantibody, a prevalence that did not differ significantly from control subjects. Further studies in this area are needed using groups with well-characterized thyroid disease.
CIU and Graves' Disease
In the 1950s (43) and 1960s (44) there were studies of patients with CIU and Graves' disease (GD). Additional reports followed (17,19,32,42,45 –54), some of which antidated the first report in 1983 (15) that there was an association between CIU and autoimmune thyroiditis. Some of these articles describe only one or a few patients, however, so are not suitable for determining if there is an association between CIU and autoimmune thyroid disease.
Collet et al. (17) reported that 8 of 45 patients (17.8%) with CIU had autoimmune thyroid disease based on the fact that certain thyroid function tests such as TSH, free thyroid hormones, TMAb, or TPOAb were abnormal. Only one of these eight patients, however, had GD. Gaig et al. (19) noted that 25 of 170 patients with CIU (14.7%) were positive for antithyroid antibodies. Again, only a minority of the patients with positive tests for antithyroid antibodies (n = 2, 8% or 1.2% of the patients with CIU) had GD. In a Turkish study (32) 41 of 140 (29%) patients with CIU had positive antithyroid antibodies, but only 2 had GD (1.4% of the 140 CIU patients). In a study of 154 patients with CIU by Small and Lerman (46), 6 (3.9%) had hyperthyroidism. In summary, in these reports (17,19,32,46) the prevalence of GD in patients with CIU ranged from 1% to 4%, a rate that is close to the ∼1% rate of GD in the general population (55 –57).
As noted above and below, anti-Fcɛ receptor-1 antibodies are thought to be involved in the pathogenesis of a subgroup of CIU, though the link of these antibodies with thyroid autoimmunity remains to be conclusively demonstrated. There are only anecdotal reports (50), however, regarding an association between anti-Fcɛ receptor-1 antibodies and GD.
A problem in determining if there is an association between CIU and GD is that many of the patients with GD may be taking antithyroid drugs (methimazole, carbimazole, or propylthiouracil) that, in themselves, may cause itching and, less frequently, urticaria. Even for positive studies there is the issue of whether hyperthyroidism per se, rather than autoimmunity, causes itching. Thus, there are reports (19,49,53) of improvement of chronic urticaria after normalization of thyroid function in patients with poor response to antihistamines and corticosteroids. There are no blinded, randomized studies, however, to ascertain if treatment of hyperthyroidism improves urticaria. In any case, interpretation of such studies is complicated by the fact that antithyroid drugs decrease the synthesis (and serum levels) not only of thyroid hormones but also of thyroid autoantibodies (58). Altogether, there is much less support for an association between GD and CIU compared to the data supporting an association between CIU and serological evidence for autoimmune thyroiditis (32).
In summary it seems well established that there is an association between CIU and the presence of thyroid autoantibodies. It is much less clear what the significance of these antibodies is. They are not likely to be signs of underlying GD or to predispose to the development of GD. A more compelling question is whether they predispose to or are signs of chronic autoimmune thyroiditis with its risk of developing hypothyroidism. These questions are more difficult to study since the risk of developing thyroid autoantibodies is increasing, paralleling the trend of a worldwide increase in the frequency of autoimmune phenomena in general. At any rate, a clear-cut association of CIU with hypothyroidism of autoimmune origin, or with histological features of HT, remains unproven thus far.
Etiology and Pathogenesis
The mechanism for the association between CIU and thyroid autoantiboides is still unknown, but there are a number of considerations of a theoretical nature (12,13,59). A number of studies (10,11,29,60,61) have been performed to determine if there is an association between autoantibodies against IgE and/or against the high affinity receptor for IgE (FcɛR), or a positive ASST (see above) and autoimmune thyroid disease. The prevalence of positive tests for autoantibodies against ASST or basophils activation test in patients with CIU and HT has ranged from 27.7% to 56% (9,17,23,60,61), with no clear relationship between a positive ASST and thyroid autoimmunity (60,61). In two studies (27,29) a slightly higher, but not significant, frequency of positive tests for ASST was observed in patients with CIU and HT compared to patients with CIU alone. One of such studies reported that after 1-year follow-up, in patients with CIU and HT positive tests for ASST persisted after urticaria subsided, whereas positive ASST tests resolved when urticaria resolved in patients having only CIU (29). One report (23) showed that, in patients with CIU, 27.7% had at least one antithyroid antibody and IgE receptor antibodies. The presence of antibodies to the IgE receptors was assessed by histamine release from human basophils (23).
As previously noted, complement activation mediated by anti-FcɛRI autoantibodies has been hypothesized as a factor in the pathogenesis of autoimmune CIU. However, no data are available on whether there is involvement of the anti-FcɛRI antibody-mediated complement activation in patients with CIU and HT. Since TPOAb and TgAb-mediated complement activation has been observed in some studies (62,63), it might be speculated that different autoantigen-autoantibody systems (anti-FcɛRI, anti-TPO) synergize in generating C5a and triggering mast cells and basophils in patients with HT and CIU. One study (64) described the presence of autoantibodies of IgE class directed against thyroid autoantigens. However, only 2 of 20 patients with HT and CIU had such antibodies (one had IgE TPOAb, the other IgE TgAb); therefore, reliable considerations about their role are not possible.
It has been suggested that L-T4 treatment may improve urticaria in patients with HT (see below) and that this would be independent of the status of anti-FcɛRI antibodies. The hypothesis is that L-T4 would reduce TPO/TgAb-mediated complement activation by decreasing serum TSH and thus reducing thyroid stimulation (13). This hypothesis is unproven, however, and is not supported by the observation of Chiovato et al. (65) that TPOAb and TgAb antibodies persist for several years after total thyroid ablation.
Aversano et al. (59) hypothesized that TSH might drive the production of proinflammatory cytokines by lymphocytes and monocytes, so as to maintain an inflammatory status leading to urticaria manifestations, in addition to stimulating thyroid autoantibody production. However, a correlation between CIU and hypothyroidism has never been demonstrated. In our opinion this argues against a proinflammatory role for TSH in CIU. Notably, the data on the effectiveness of L-T4 therapy in urticaria are not consistent. Some studies report a benefit (19,59,66 –69), but others do not (22,70,71). In fact, most studies included only a small number of patients with only 123 patients studied in total (16,19,59,66 –69) and often there was no untreated group as a control. Moreover, there are no studies that have compared different doses of L-T4 (i.e., L-T4 substitution in either overt or subclinical hypothyroidism and L-T4 doses associated with TSH suppression). More studies are needed. They should be adequately powered and, unlike previous studies, be double-blinded placebo-controlled trials.
Infectious agents are thought to be involved in the pathogenesis of both CIU and HT. Infectious agents have been frequently proposed as one of the environmental factors for thyroid autoimmunity, but direct evidence for a cause and effect relationship between an infectious agent and the onset or worsening of autoimmunity is lacking [reviewed in ref. (72)]. The recently achieved understanding of the close interrelationship between innate and adaptive immune response—the former being crucial as first-line defense from pathogens—has provided new insight about infection–autoimmunity relationships (73). For example, thyroid follicular cells in HT can express surface molecules pertaining to the innate Toll-like receptor family (TLR3) (74). Viral and bacterial superantigens can induce relevant changes in the composition of lymphocyte repertoire (involving >5% of naïve lymphocytes). This induction derives from their ability to interact with most T lymphocytes that express antigen receptors from a particular variable (V) region gene family (75).
Regarding bacteria, Staphylococcus aureus superantigens have been well characterized, and may be taken as an example of potential inducers of thyroid autoimmunity and CIU. Marone et al. (75,76) showed that Staphylococcus aureus protein A is able to activate FcɛRI+ cells to release proinflammatory mediators and cytokines, inducing episodes of urticaria. On the other hand, Wan et al. (77) showed that staphylococcal enterotoxin A superantigen stimulation of thyroglobulin-primed cells resulted in the adoptive transfer of experimental autoimmune thyroiditis in mice.
The association of Helicobacter pylori with both CIU and HT is still controversial. The first hypothesis that there was an association of H. pylori and chronic urticaria was made in late 1990s, a time at which skin manifestations improved after H. pylori eradication was not consistently observed [reviewed in (78 –80)]. It has been suggested (78) that H. pylori may exacerbate urticaria symptoms, rather than trigger urticaria. The prevalence of H. pylori in CIU ranges from 24% to 83% depending on geographic area and patients' age [reviewed in ref. (78)]. Possible explanations for this variability are differences in methods to assess H. pylori infection, different antigenicity and biologic activity of bacteria in a given epidemiological context, and different socioeconomic and genetic background of the population studied (74).
Theoretically, the interactions of H. pylori in chronic urticaria may have several mechanisms, including interaction with mast cells with consequent mediator release, impairment of both gastrointestinal mucosal barrier function and digestion (81), upregulation of the cytotoxic eosinophilic cationic protein from eosinophils activated by H. pylori (82), and complement consumption due to H. pylori–specific antibodies (83,84). In addition, H. pylori may induce the production of pathogenic autoantibodies by molecular mimicry of endogenous proteins (85 –87). Once cross-reactive antibodies have been elicited by H. pylori, their production might continue even after H. pylori eradication, thus explaining the reported lack of urticaria improvement after eradication (79). Clinical data on the association of H. pylori infection with positive ASST tests are controversial (88 –90).
H. pylori infection has also been linked to thyroid autoimmunity, but available data are controversial (91). An increased prevalence of H. pylori infection in patients with autoimmune thyroid disorders and a relationship between H. pylori infection and TgAb and TPOAb has been reported in some studies, but not in others [reviewed in (92)]. A decrease of thyroid autoantibodies after H. pylori eradication was observed in one study (93). Monoclonal antibodies against CagA+ H. pylori strains cross-react with thyroid follicular cells; these H. pylori strains carry a gene encoding for an endogenous peroxidase (94). In the context of the molecular mimicry hypothesis, one of us has reported amino acid sequence homology between region 126–262 of the DNA transfer protein of H. pylori and region 244–365 of TSH-R, the latter being a stretch of the extracellular portion of TSH-R that contains both T-cell and B-cell epitopes (91).
With regard to viruses, hepatitis C virus (HCV) infection was reported to be consistently associated with CIU (95 –97). Marone et al. (75) showed that Protein Fv binding with IgE VH3+ acts as a complete secretagogue on FcɛRI+ cells, stimulating urticaria reactions (75). Protein Fv is a sialoprotein produced in human liver and released during viral hepatitis A, B, C, and E. HCV infection is also strongly associated with thyroid autoimmunity (98 –100), but a possible mechanism has only been described recently (99). HCV receptor CD81, a molecule that mediates viral attachment and entry, is expressed in cells of several tissues, including thyroid follicular cells (101). Akeno et al. (101) showed that incubation of HCV envelope glycoproteins E2 with thyroid follicular cells resulted in E2 binding to thyroid cells and activation of interleukin-8 (IL-8) with sustained proliferation and escape from apoptosis. Therefore, the two HCV envelope glycoproteins, E1 and E2, may engage HCV receptor CD81 even without productive infection, and activate intracellular signaling pathways that trigger a tissue inflammatory response through the release of pro-inflammatory mediators such as IL-8. This would likely induce thyroid autoimmunity by bystander activation (101).
In summary, there are several potential mechanisms whereby infectious agents may trigger both thyroid autoimmunity and CIU. The molecular and epidemiological evidence to date on the involvement of an infectious agent in the pathogenesis of thyroid autoimmunity and CIU is not definitive, however.
Therapy of CIU with L-Thyroxine
Resolution of urticaria after L-T4 treatment, irrespective of the initial thyroid function status, has been reported by some authors (19,59,66 –69). In the study by Aversano et al. (59), 80% of patients had improvement of urticaria (reduction of itching and erythema, and disappearance of wheals with an overall positive effect on sleep) 12 months after starting L-T4 therapy. An overall correlation was also observed between urticaria improvement and decrease of both erythrocyte sedimentation rate values and serum thyroid autoantibodies (TgAb and TPOAb). In another study (66), urticaria improved within 4 weeks from starting treatment in seven patients with high levels of thyroid autoantibodies, but not in three with low levels of thyroid autoantibodies. In five of these patients, symptoms recurred after the treatment was stopped and resolved again after treatment was restarted. Resolution of angioedema after L-T4 therapy has also been the subject of an anecdotal report (102,103). In one patient with HT and CIU the urticaria and angioedema failed to respond to L-T4 treatment but resolved after total thyroidectomy (104).
Data concerning pediatric patients are scanty. In one study (39), none of three hypothyroid children treated with L-T4 experienced remission of urticaria; in addition, one child developed urticaria while under L-T4 treatment (39). Dreyfus et al. (105), reported remission of urticaria after thyroxine treatment in a 9-year-old euthyroid patient with a positive test for TMAb.
In summary, L-T4 treatment may improve CIU associated with HT in some but not all patients. However, we stress that most reports are anecdotal or underpowered, and no double-blind placebo-controlled studies have been performed. Moreover, it must be emphasized that no correlation has been demonstrated between the presence of CIU and the impairment of thyroid function. Thus, it is not surprising that L-T4 as a therapy for CIU has been questioned (80). Definitive studies are needed before a strong recommendation for L-T4 as a treatment for CIU in patients can be made.
Conclusions
The coexistence of CIU and thyroid autoimmunity is frequent, in that at least one-fourth of patients with CIU have serological evidence of autoantibodies against one or more thyroid autoantigens. Such a prevalence of thyroid autoantibodies does not substantially differ from that reported in other autoimmune diseases that may associate with autoimmune thyroid diseases (type III autoimmune polyendocrine syndrome) (106); as an example, a prevalence of about 30% of thyroid autoantibodies was very recently reported in Systemic Lupus Erythematosus (107). The literature provides fair evidence for a relationship of CIU with thyroid antibodies, but not with histological thyroiditis or altered thyroid function. A number of factors (e.g., prevalence of thyroid auto-antibodies higher in females, and increasing with age) are not taken into consideration in many reports. Nonetheless, CIU patients may well represent a group of subjects at risk for thyroid autoimmune disease (particularly autoimmune thyroiditis) and, accordingly, should undergo tests for thyroid autoimmunity and thyroid dysfunction.
The reason for the association between positive serological tests form thyroid autoimmunity and CIU is unclear. Recent literature suggests that exposure to infectious agents induces both urticaria and thyroid autoimmunity, but conclusive information is lacking. Carefully controlled studies are needed regarding the effects of L-T4 treatment in CIU when it is associated with thyroid autoimmunity, as well as the relationship of L-T4 effects to basal thyroid function and the thyroid status achieved by L-T4 treatment.
Footnotes
Acknowledgment
The authors thank Professor Francesco Trimarchi (Endocrinologia, University of Messina School of Medicine) for his careful reading of the article.
Disclosure Statement
The authors declare that no competing financial interests exist.