
Abstract
Background:
In the United States, the prevalence among adults of palpable thyroid nodules is 4%–7%, of which 5%–10% may represent thyroid carcinoma. Despite the success of fine-needle aspiration in reducing the need for thyroidectomy, aspirates are inadequate to render a diagnosis in 20% of cases. Minimizing nondiagnostic samples is an important goal in improving this technique. Our objective was to determine whether bedside-prepared slides improve diagnostic adequacy over standard solution-based samples. We further sought to determine the role of needle size.
Methods:
One hundred sixty-two patients were prospectively enrolled. For each, both bedside slides and standard cytology solutions were prepared; the order of preparation alternated from subject to subject. Needle size (21- or 25-gauge) also alternated from subject to subject. Slides were evaluated by pathologists blinded to needle size. The study took place in the endocrinology clinic at Boston Medical Center, the tertiary referral hospital of the Boston University School of Medicine. Key outcomes were diagnostic adequacy and specimen cellularity.
Results:
Compared to standard solution-based samples, bedside slides provided more cellular specimens (p < 0.01) and fewer nondiagnostic samples (p = 0.016). When standard solution-based samples were used as the sole method of preparation, 21-gauge needles provided improved diagnostic adequacy.
Conclusions:
Bedside-prepared slides offer improved diagnostic adequacy and specimen cellularity over solution-based samples. The difference may be especially important when using smaller (25-gauge) needles to perform fine-needle aspiration. When solution-based samples are used, larger (21-gauge) needles provide more diagnostic specimens.
Introduction
FNA is therefore the cornerstone of evaluation for solitary thyroid nodules. When performed by experienced providers, FNA is diagnostic in 80% of cases, typically with two to four passes of the needle (3,6). Despite the overall success of FNA, aspirates are inadequate to render a diagnosis in 20% of cases. Nondiagnostic FNAs can lead to repeat procedures, additional testing, and significant patient anxiety. Therefore, minimizing nondiagnostic samples is an important goal that will further enhance this invaluable tool.
A reasonable hypothesis is that specimen cellularity will correlate with diagnostic adequacy (rate of samples sufficient for diagnosis). That is, if more cells are aspirated, the likelihood that a definitive diagnosis can be made increases. Therefore, modifications in FNA technique that lead to increased cellularity of aspirate might reasonably be expected to improved diagnostic adequacy. A previous study (6) at our institution looked at needle gauge as a factor in specimen adequacy in thyroid FNA. In that study, 21-gauge needles provided more cellular specimens than did 25-gauge needles, but did not improve diagnostic adequacy (i.e., both needle gauges produced the same rate of sufficient samples). It was thought that larger needle gauge might not result in increased diagnostic adequacy.
The current study focused on a different variable in FNA: mode of preparation of aspirates. Many centers use cytology solutions as the sole mode of preparation; however, some clinicians prefer the classical technique of slides prepared at bedside. Whether or not these bedside-prepared slides offer superior diagnostic adequacy over standard cytology solutions has not been examined. Thus, in this study we sought to evaluate the utility of bedside-prepared slides relative to standard solution-based samples.
Materials and Methods
Administration
The study was approved by the Institutional Review Board at Boston Medical Center. The study population consisted of prospectively enrolled patients undergoing thyroid FNA for the evaluation of nodules. Each patient gave written informed consent for participation in the study.
Procedure
We prospectively enrolled 162 subjects. Biopsies were performed by one of three endocrinologists at our medical center. The skin overlying the nodule was sterilized with alcohol. Thyroid aspirates were taken with 1.5-inch needles attached to 10-mL syringes. Needles used were either 21 or 25 gauge.
For each subject, only one needle gauge was used (selected in alternating fashion between patients), but both bedside slides and standard cytology solutions were prepared. Six total needle passes were made: three passes for slides and three for solution. The order of preparation and the needle size used were alternated from subject to subject.
Slides were prepared such that the edge of one slide was used to smear sample across a second slide in the fashion standard for preparing complete blood counts. Slides were prepared at bedside and transferred immediately to a simple ethanol solution. Standard cytology solutions were prepared by flushing collected cells into cytocentrifugation collection fluid (20 mL of Carbowax, a dispersing agent, dissolved in 80 mL of 60% ethanol).
Pathologists blinded to needle size followed the guidelines of the Papanicolaou Society of Cytopathology for adequacy in the interpretation of slides. Observations were made from high-power views and conclusions were drawn after all slides were examined. Specimens were considered insufficient if there was lack of specimen identification, slide breakage, poor smear quality caused by poor fixation, poor staining, poor preservation, or obscuring blood.
Each sample was given a numerical adequacy score of 0 (nondiagnostic, acellular specimen), 1 (nondiagnostic minimal cellular material), 2 (diagnostic with borderline material), or 3 (diagnostic with abundant material). Thus, scores of 0 or 1 were nondiagnostic, whereas scores of 2 or 3 were diagnostic. Each increment of 1 in adequacy score represented an increase in the cellularity of the specimen.
The pathologists used the following categories for the interpretation of the thyroid cytology slides: benign colloid nodule, papillary carcinoma, medullary carcinoma, anaplastic carcinoma, indeterminate, or insufficient cells for diagnosis. Indeterminate was used for micro-follicular cytology.
Statistics
We desired a power of 80% to detect differences between the comparison groups using a two-tailed t-test. Allowing for an α-error of 0.05 and assuming a medium effect size (using Cohen's d of 0.5), a minimum of 64 samples per group were required to attain this 80% power. Data were collected for 162 samples per group, yielding a power of 88.5% under the aforementioned parameters.
We compared the slides and solutions for all subjects, looking specifically at two outcomes: (i) percentage of diagnostic samples and (ii) specimen cellularity. We further analyzed the data stratifying by needle size (21 vs. 25 gauge) for those subjects for whom needle gauge was recorded, looking at the same outcomes.
For the first outcome, percentage of nondiagnostic samples, we compared the groups using Student's t-tests, first for all samples and then broken down by needle gauge. For the second outcome, specimen cellularity, we compared the groups using Chi-square testing. The null hypothesis was that if cellularity were not affected by preparation technique, one technique would be superior to the other as often as the reverse was true. Thus, we used chi-square testing with degrees of freedom of 1.
Results
Diagnostic adequacy
Bedside slides were diagnostic more often than solution-based samples
Scores of 0 or 1 were nondiagnostic, whereas scores of 2 or 3 were diagnostic. Bedside slides were nondiagnostic in 27 of 162 samples (16.7%), whereas solution-based samples were nondiagnostic in 41 of 162 samples (25.3%) (Fig. 1). This difference was statistically significant (p = 0.016).
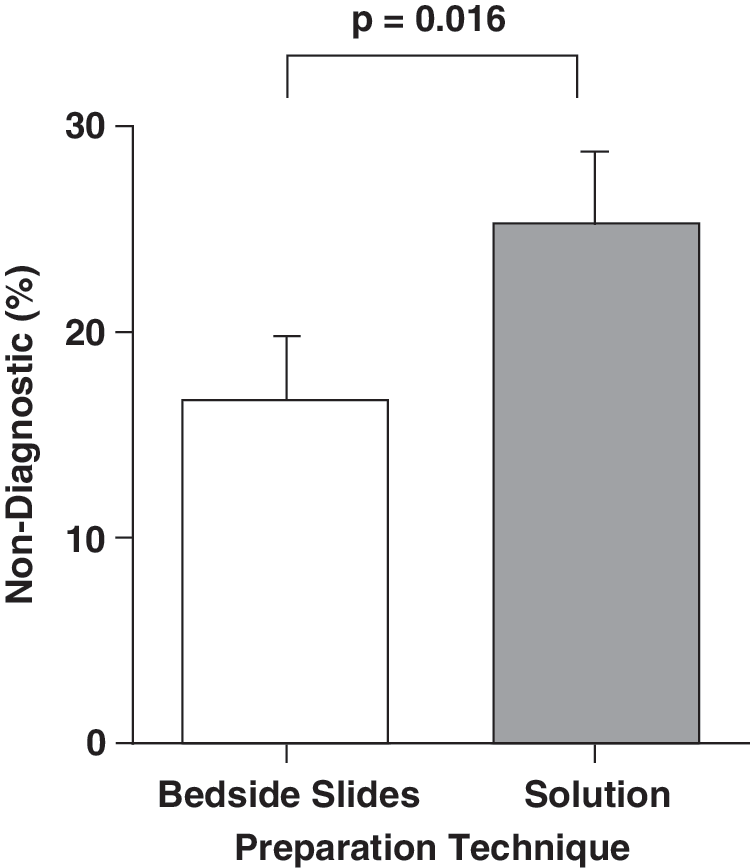
Percentage of nondiagnostic FNA samples for bedside-prepared slides compared to solution-based samples. The white bar shows that 16.7% of bedside slides were nondiagnostic; the gray bar represents the 25.3% of solutions that were nondiagnostic. The error bars represent SD. This difference was significant (p = 0.016). FNA, fine-needle aspiration.
Further, bedside slides were diagnostic in 24 of the 41 cases (58.5%) in which solution-based samples were nondiagnostic, whereas solution-based samples were diagnostic in only 10 of the 27 cases (37.0%) in which bedside slides were nondiagnostic (Chi-squared test, df = 1, two-tailed p-value = 0.016) (Fig. 2).
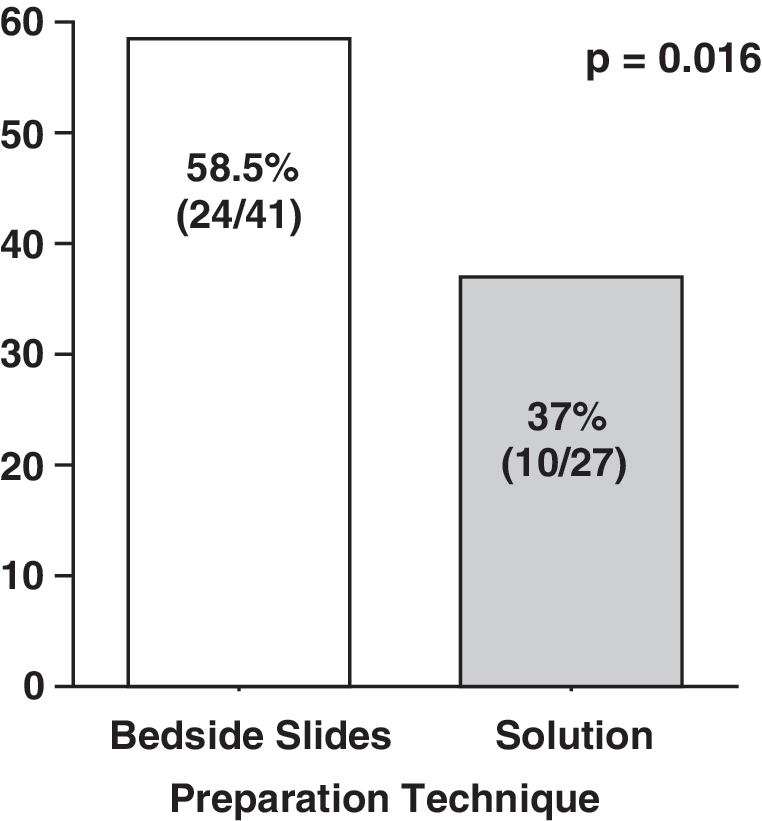
Comparison of how often one technique was diagnostic when the other was nondiagnostic and vice versa. The white column on the left shows that bedside slides were diagnostic in 24 of the 41 cases when solutions were nondiagnostic (58.5%). The gray column on the right indicates that solutions were diagnostic in 10 of the 27 cases when bedside slides were nondiagnostic (37.0%). This difference was significant (p = 0.016).
Impact of needle gauge on diagnostic adequacy
Of the 162 total FNA procedures, needle gauge was recorded in 120 cases. Due to an oversight the needle gauge was not recorded on the remaining 42 cases. Of the cases where needle gauge was recorded, 58 were 21 gauge and the remaining 62 were 25 gauge. This distinction gives four subgroups that could then be compared: bedside slides prepared from 21-gauge FNAs, solution-based samples prepared from 21-gauge FNAs, bedside slides prepared from 25-gauge FNAs, and solution-based samples prepared from 25-gauge FNAs.
We analyzed these groups looking at two distinct questions: (i) Does preparation technique affect diagnostic adequacy for a given needle gauge? (ii) Does needle gauge affect diagnostic adequacy for a given preparation technique?
No difference seen between slides and solution-based samples for 21-gauge FNAs
To answer the first question, we stratified first by needle gauge, and then compared the two techniques within each needle gauge group. For 21-gauge FNAs, bedside slides provided a nondiagnostic specimen in 7 of 58 cases (12.1%) compared with solution-based samples, which provided a nondiagnostic specimen in 8 of 58 cases (13.8%) (Fig. 3A). This difference was not statistically significant (p = 0.71).
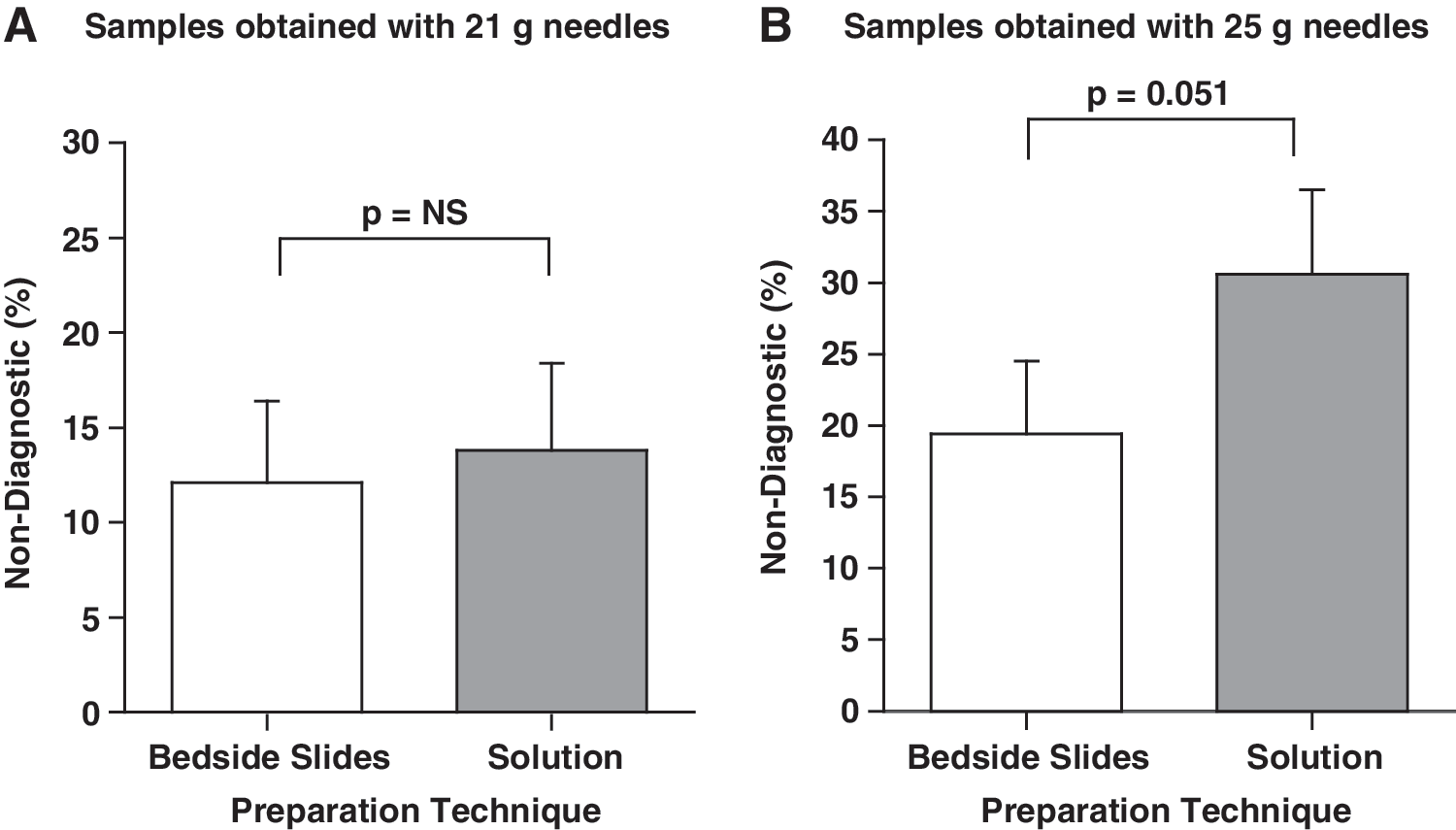
Percentage of nondiagnostic FNA samples for bedside-prepared slides compared to solution-based samples using either
The difference between slides and solution-based samples for 25-gauge FNAs approached statistical significance
For 25-gauge FNAs, bedside slides provided a nondiagnostic specimen in 12 of 62 cases (19.4%), whereas solution-based samples provided a nondiagnostic specimen in 19 of 62 cases (30.7%) (Fig. 3B). This difference approached statistical significance (p = 0.051).
No difference observed between bedside slides prepared from 21-gauge FNAs versus bedside slides prepared from 25-gauge FNAs
To answer the second question, we stratified first by technique, and then compared the two needle gauges for each technique. For the bedside-prepared slides, 21-gauge samples were nondiagnostic in 7 of 58 samples (12.1%), whereas 25-gauge samples were nondiagnostic in 12 of 62 cases (19.4%) (Fig. 4A). This difference was not statistically significant (p = 0.28).
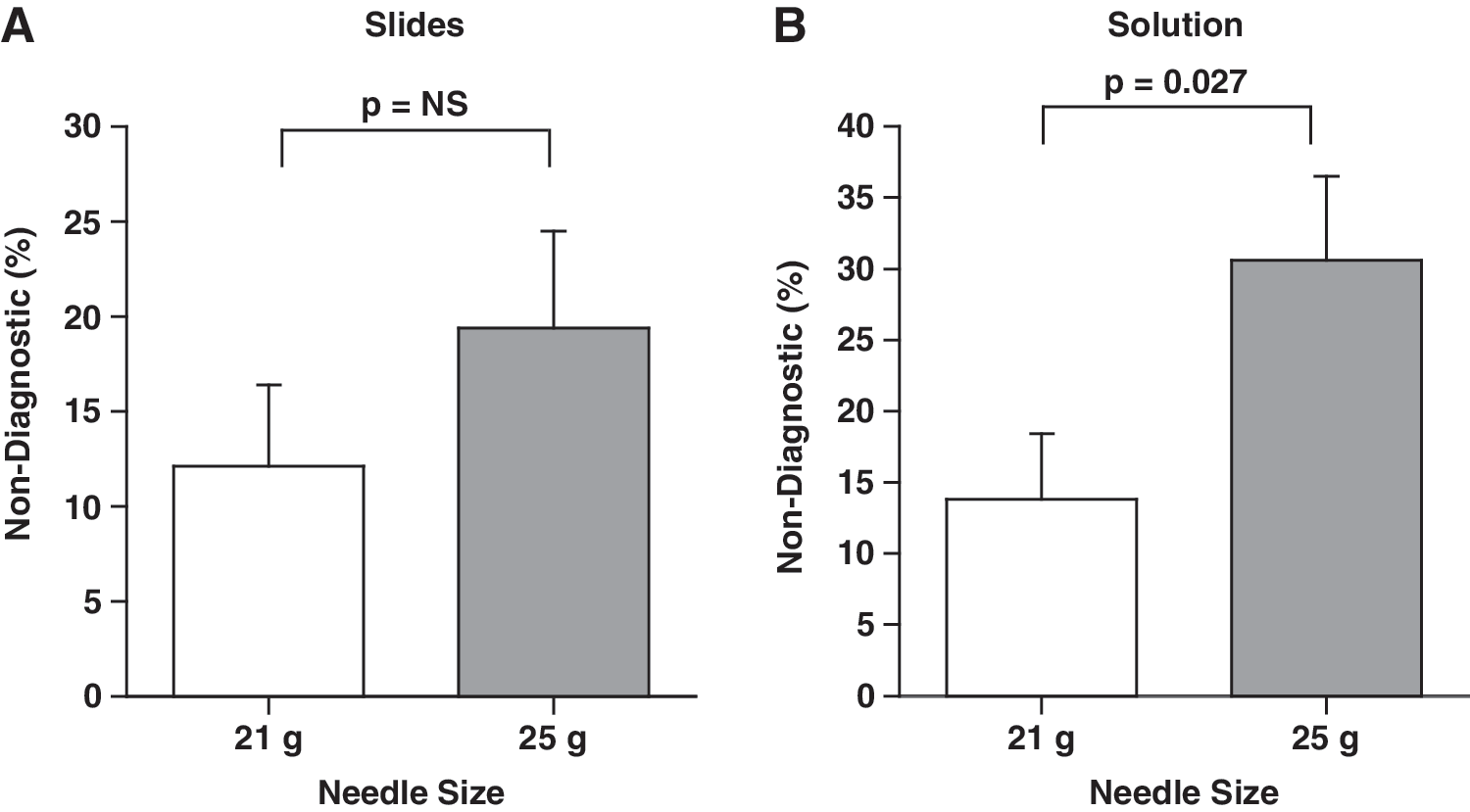
Percentage of nondiagnostic FNA samples for 21-gauge needles compared to 25-gauge needles when preparing either
Solution-based samples prepared from 21-gauge FNAs were more frequently diagnostic than solution-based samples prepared from 25-gauge FNAs
For solution-based samples, 21-gauge FNAs were nondiagnostic in 8 of 58 samples (13.8%), whereas 25-gauge FNAs were nondiagnostic in 19 of 62 cases (30.6%) (Fig. 4B). This difference was statistically significant (p = 0.027).
Specimen cellularity
Bedside-prepared slides provided more cellular specimens than solution-based samples
Bedside-prepared slide provided a more cellular specimen in 64 of 162 cases (39.5%); the solution-based samples provided a more cellular specimen in 29 of 162 cases (17.9%); and equal cellularity was obtained in the remaining 69 of 162 cases (42.6%) (Fig. 5). This result was statistically significant (chi-squared test, df = 1, two-tailed p < 0.01).
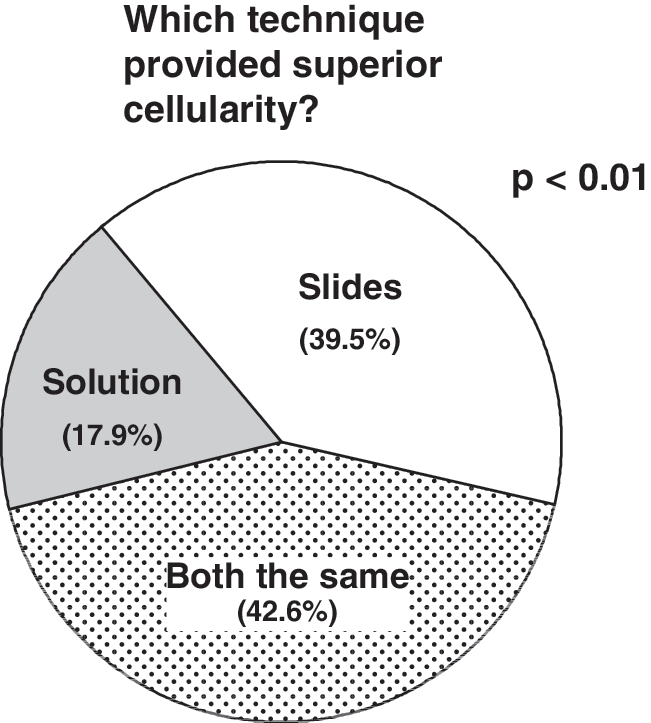
Comparison of specimen cellularity obtained using bedside slides compared to solution-based samples. The pie chart shows the proportion of cases in which cellularity was superior for slides (white), superior for solutions (gray), or equal for both techniques (spotted pattern). Bedside slides provided a more cellular specimen compared to solution-based samples significantly more often (39.5% of cases) than the reverse occurred (17.9% of cases, p < 0.01).
Impact of needle gauge on specimen cellularity
To evaluate whether the superiority of bedside slides over solution-based samples in specimen cellularity was attributable to the size of needle used, these data were also broken down by needle gauge in the 120 cases where this parameter was recorded. The data were analyzed to answer the following questions: (i) Does preparation technique affect specimen cellularity for a given needle gauge? (ii) Does needle gauge affect specimen cellularity for a given preparation technique?
No difference in specimen cellularity observed between bedsides slides and solution-based samples when prepared from 21-gauge needles
For 21-gauge needles, bedside slides provided a more cellular specimen in 16 of 58 cases (27.6%); solution-based samples provided a more cellular specimen in 10 of 58 cases (17.2%); and both techniques provided equally cellular specimens in 32 of 58 cases (55.2%) (Fig. 6A). This result was not statistically significant (Chi-squared test, df = 1, two-tailed p = 0.24).
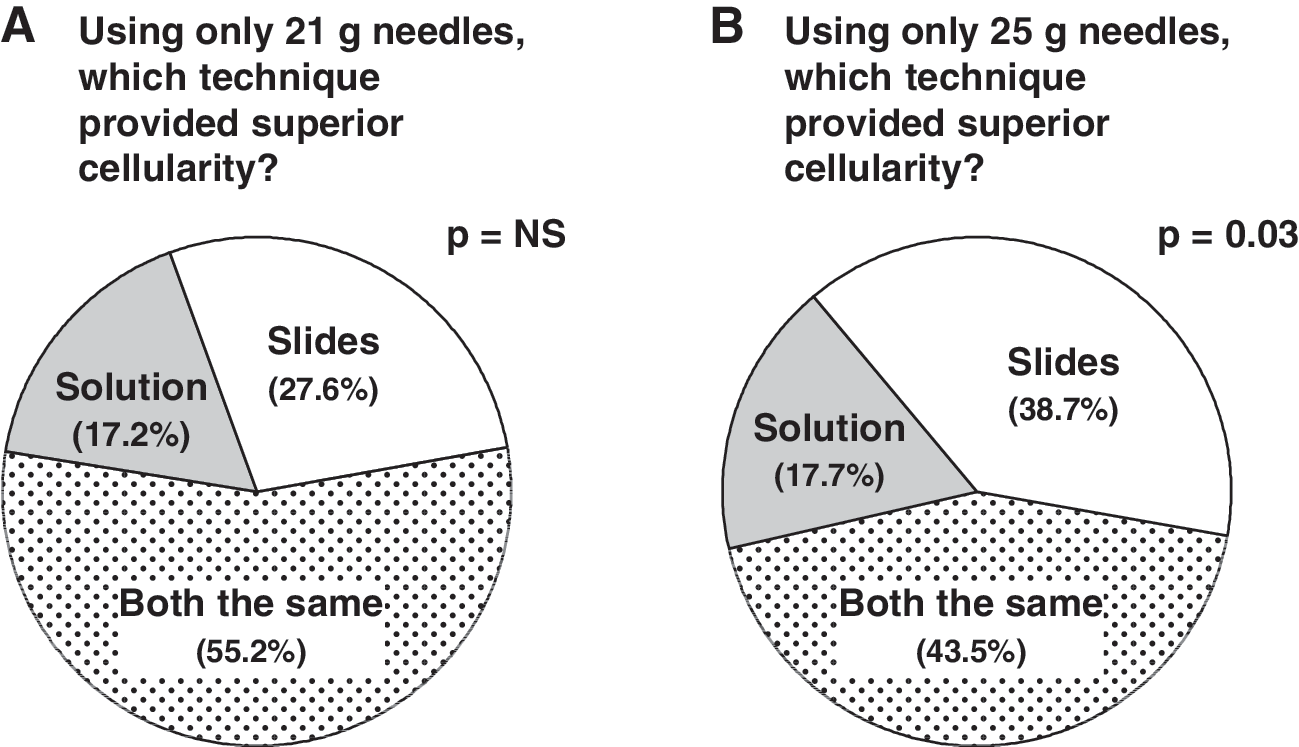
Comparison of specimen cellularity obtained using bedside slides compared to solution-based samples for
Bedside slides provided more cellular specimens than solution-based samples when prepared from 25-gauge needles
For 25-gauge needles, bedside slides provided a more cellular specimen in 24 of 62 cases (38.7%); solution-based samples provided a more cellular specimen in 11 of 62 cases (17.7%); and both techniques provided equally cellular specimens in 27 of 62 cases (43.5%) (Fig. 6B).
This difference was statistically significant (Chi squared test, df = 1, two-tailed p = 0.03)
No difference in specimen cellularity observed for 21-gauge versus 25-gauge needles when using bedsides slides
The same data were also analyzed stratifying first by preparation technique. Bedside slides prepared from 21-gauge FNAs provided an average cellularity of 2.30, whereas bedside slides prepared from 25-gauge FNAs provided an average cellularity of 2.17. This difference in cellularity was not statistically significant (unpaired t-test, p = 0.38).
Trend toward improved specimen cellularity observed for 21-gauge versus 25-gauge needles when using solution-based samples
Similarly, a comparison was done of solution-based samples prepared from 21-gauge FNAs to solution-based samples prepared from 25-gauge FNAs. The 21-gauge samples produced an average cellularity of 2.18, whereas the 25-gauge samples produced an average cellularity of 1.92. Although the difference did not reach statistical significance, the data trended toward increased specimen cellularity for 21-gauge FNAs when preparing solution-based samples (unpaired t-test, p = 0.08).
Discussion
FNA is the standard of care in evaluating thyroid nodules for malignancy. It is a safe, well-tolerated, and cost-effective procedure. Despite its utility, FNA samples are nondiagnostic in ∼20% of cases; modifications that reduce this percentage will be of great value. Variables such as method of specimen preparation and needle gauge may impact specimen cellularity and diagnostic adequacy; these variables were the subject of the current study.
We compared results of thyroid FNAs that were evaluated with two different techniques: first, a standard cytology solution in use at many centers; second, an older, classical method of bedside-prepared slides favored by some providers. Because both slides and solutions were prepared for all subjects, the study groups were identical. Thus, any differences in outcomes for an individual subject are attributable only to preparation technique (bedside slide versus standard solution). Further, any differences in outcomes seen in the overall cohort must be attributable to one of the two variables involved: preparation technique or needle gauge. The latter variable was not noted in all of the subjects, which limited our analysis.
In this study, bedside-prepared slides significantly improved diagnostic adequacy (percentage of samples sufficient for diagnosis) and specimen cellularity over standard solution-based samples. That the superiority of bedside slides was observed in both variables is unsurprising, as increased cellularity would be expected to improve diagnostic yield. In addition, the bedside prepared smears had better preserved architecture. Although the cellularity scale did not directly measure the architecture, the better architecture definitely played a role in the improved diagnostic accuracy. Higher diagnostic yield from FNAs would expedite clinical workups and reduce the need for repeat procedures, which may expose patients to additional anxiety and morbidity. Given their low cost and ease of preparation, we recommend the routine use of bedside-prepared slides in thyroid FNA.
The order of preparation was alternated from patient to patient. That is, slides would be prepared first followed by solutions for one patient, and then solutions would be prepared first followed by slides for the next patient. One might expect that the bleeding caused by prior needle passes would have a more detrimental effect on slides than on solutions. This is because aspirated red blood cells become lysed in solution, which does not occur with immediate fixation on slides. Thus, it is conceivable that the superiority of bedside slides over solutions would be even more pronounced when doing only one preparation technique per patient.
Our results also suggest that combining both techniques would improve both main outcomes compared to either technique alone. Previous studies have shown that increasing the number of needle passes improves diagnostic adequacy (7). Thus, the superiority of the two techniques combined may be due either to an increase in the total number of passes from three to six or to the ability to leverage advantage of each approach in the final diagnosis.
As noted previously, we do not know the needle gauge for 42 of the cases due to an error in data collection. While we anticipate that this oversight would have been equally distributed between the needle gauge groups, it served to decrease our sample size and therefore reduce our power slightly.
No difference in diagnostic adequacy was seen between the bedside slides and solution-based samples for either needle gauge individually. This may have been due to underpowering. It is worth noting, however, that for 25-gauge samples, bedside slides were superior in specimen cellularity over solution-based samples, and their superiority in diagnostic adequacy very nearly achieved statistical significance. We conclude that when a 25-gauge needle is used for FNA, preparing slides at bedside is likely to improve key outcomes.
Aspirates obtained from 21-gauge needles provided a higher rate of diagnostic samples than aspirates obtained from 25-gauge needles when prepared with a standard cytology solution. A trend toward improved specimen cellularity was also observed, again confirming the likely correlation between cellularity and diagnostic adequacy. In contrast, this superiority of 21-gauge needles over 25-gauge needles was not seen with the bedside slides. One explanation for the disparity is that larger bore needles aspirate more cellular material, including more red blood cells, than smaller bore needles. As previously noted, when this aspirate is then flushed into a cytopreservative solution, those red blood cells become lysed, thereby maximizing the benefit of the additional thyroid cells aspirated with a larger needle. Immediate fixing techniques such as bedside slides do not lyse red blood cells, and therefore the benefit of increased cellularity gained from a larger needle is lost.
Finally, one potential concern about use of a larger gauge needle is that it might increase complications such as bleeding. In this study, there were two emergency room visits for pain after FNAs, one from a 21-gauge FNA and the other from a 25-gauge FNA. Neither required intervention.
Conclusion
Bedside-prepared slides offer improved diagnostic adequacy and specimen cellularity over solution-based samples. We recommend their routine use given their low cost and ease of preparation. The difference may be especially important when using 25-gauge needles to perform FNA.
When standard solution-based samples are used as the sole method of preparation, 21-gauge needles provide improved diagnostic adequacy, and may also improve specimen cellularity, over 25-gauge needles.
Footnotes
Disclosure Statement
The authors declare that they have no conflicts of interest to disclose relating to this article.