
Abstract
Background:
Preoperative vocal fold paralysis (VFP) is thought to be rare in patients with benign thyroid disease (BTD). In contrast with cases of malignancy, in which the recurrent laryngeal nerve (RLN) should be severed, in patients with BTD and VFP the RLN can be preserved without threatening patients' lives. This study investigates the clinical features that enable identification of patients who have VFP associated with BTD.
Methods:
Medical records of 187 consecutive patients who underwent thyroid surgery were retrospectively reviewed. The association between preoperative VFP and pathology (benign or malignant), clinical features, and treatment results of patients with BTD and VFP were analyzed.
Results:
Of the 187 patients, 145 patients had BTD and 8 of these cases (5.52%) had preoperative unilateral VFP. The prevalence of BTD with VFP was 4.3% (8/187). The other 42 patients had malignant thyroid disease and 4 of these cases (9.52%) had preoperative unilateral VFP. None of the aforementioned VFP was caused by previous thyroidectomy or surgery to the neck. Although the relative risk of VFP in patients with thyroid malignancy was 1.726 (9.52%/5.52%), there was no significant association between VFP and malignancy. Of the eight patients with BTD, benign fine-needle aspiration cytology or frozen sections, goiter with a diameter larger than 5 cm, cystic changes, and significant radiologic tracheo-esophageal groove compression were the common findings. During thyroidectomy, the RLN was injured but repaired in three patients. Two events occurred in patients who had severe RLN adhesion to the tumor caused by thyroidectomy performed decades ago. Two of the five patients without nerve injury recovered vocal fold function. The overall VFP recovery rate for patients with BTD and VFP was 25% (2/8).
Conclusions:
Preoperative unilateral VFP is not uncommon in thyroid surgery. Obtaining information on laryngeal function is of extreme importance when planning surgery, especially contralateral surgery. Goiter with preoperative VFP is not necessarily an indicator of malignancy. Benign perioperative cytopathologic findings with typical radiographic compression strongly suggest that VFP is caused by BTD. If, during thyroidectomy, the RLN is carefully preserved, recovery of vocal fold function may still be possible.
Introduction
Materials and Methods
From January 2004 to December 2008, 187 consecutive patients underwent thyroid surgery in our otolaryngology-head and neck surgery department for treatment of various thyroid diseases. The medical records of these patients were retrospectively reviewed with regard to patient demographics, clinical presentation, preoperative evaluation of vocal fold motion by fiberoptic laryngoscopy, preoperative imaging findings, surgical procedures, and follow-up records. Results of perioperative pathologic examinations including fine-needle aspiration cytology (FNAC), frozen section, and permanent pathology were also reviewed. The patients were then dichotomized into benign pathology or malignant pathology groups, according to permanent pathologic reports, and into positive or negative groups for preoperative VFP according to fiberoptic laryngoscope findings. The association between preoperative VFP and thyroid malignancy was analyzed using Fisher's exact test. In addition, the clinical features of eight patients with BTD and VFP were assessed. This study was approved by the Institutional Review Board of Taichung Veterans General Hospital.
Results
Table 1 is a cross table of pathologic diagnosis and VFP in the 187 patients who underwent thyroid surgery. Of the 187 patients, 12 patients (6.4%) had unilateral VFP before surgery. Of those 12 cases, 4 patients (33.3%) had malignancy and 8 patients (66.7%) had benign pathologies. No patients with VFP accompanying thyroid malignancy had a history of thyroidectomy or neck surgery that could increase the risk of VFP. Two of eight VFP patients with benign pathology received thyroidectomy decades earlier but their symptoms of husky voice developed just after the recurrence of goiter. Their VFP, therefore, had no relevance to previous surgery. In the rest of the patients who had goiter without VFP, three previously received thyroidectomy. Of the 175 patients without VFP, 38 patients (21.7%) were classified into the malignant pathology group, whereas 137 patients (78.3%) were classified into the benign pathology group. In our series, the prevalence of BTD with VFP was 4.3% (8/187). The relative risk of patients with thyroid malignancy to have VFP was 1.726 (95% confidence interval, range from 0.547 to 5.452), and the relative risk of VFP patients to have malignancy was 1.535 (95% confidence interval, range from 0.657 to 3.585). However, there was no significant association between VFP and thyroid malignancy (p-value = 0.472, Fisher's exact test).
Table 2 summarizes the clinical characteristics of eight patients with BTD and VFP before, during, and after thyroidectomy. Six patients were women and two patients were men (age range from 42 to 81 years and mean age was 61 years). Seven patients complained of husky voice but one patient had normal voice despite having VFP. The duration of symptoms before hospital visits ranged from 1 month to 5 years. All eight patients presented with large goiter. Two patients (patient no. 1 and no. 7) had underwent thyroidectomy for benign disease decades earlier but their symptoms of husky voice developed just after the recurrence of goiter. Their VFP, therefore, had no relevance to previous surgery. These two patients had recurrent bilateral goiters but only right-side VFP. Of the other six patients, three had right-side goiter and three had left-side goiter with ipsilateral VFP. In total, five patients had right VFP and three had left VFP.
F, female; M, male; B, bilateral; R, right; L, left; VFP, vocal fold paralysis; RLN, recurrent laryngeal nerve.
All patients were treated with thyroidectomy, and wherever possible, surgeons tried to preserve the RLN. In two patients with recurrent goiter (patient no. 1 and no. 7), surgeons noted severe adherence of the RLN to the goiter. They opted to partially divide and repair the RLN in one of the cases (patient no. 1). In the other patient (patient no. 7), the surgeon performed reanastomosis of the RLN after transection. Despite immediate repair of the nerves, vocal fold function did not return to normal in the follow-up period in these two patients. In another patient (no. 6), who had a normal voice despite having VFP, a junior surgeon could not identify the RLN, and after completion of thyroidectomy, it was found to have been accidentally transected. The patient's voice quality deteriorated after the surgery. In five of the eight patients with BTD and VFP, surgeons were able to identify and preserve the RLN. We supposed there was no iatrogenic division injury because of the fact that there were no visible cuts or tears on the sheaths of the five preserved nerves. Two patients (patient no. 3 and no. 5) recovered vocal fold function at 3 months and 2 weeks after thyroidectomy, respectively. In this study, the overall recovery rate of vocal fold function after thyroidectomy for patients with BTD and VFP was 25%.
Table 3 summarizes the preoperative imaging analysis findings from all eight patients including computed tomography from seven patients and sonography from one patient. In six patients, the trachea significantly deviated to the contralateral side of the paralyzed vocal fold (Fig. 1). In the two patients with recurrent bilateral goiter after previous thyroidectomy, the bilateral goiter pinched the tracheo-esophageal groove causing tracheo-esophageal separation (Figs. 2 and 3). Previous image features indicated severe compression or stretching of the RLN by the tumor. There was evidence of tumor extension to the clavicle (thoracic inlet) in six of the patients (Fig. 4). The maximal diameters of the tumors ipsilateral to the VFP were all larger than 5 cm. Cystic changes in the goiter presented in seven of eight patients, and no patient had suspected malignant cervical lymph node enlargement.
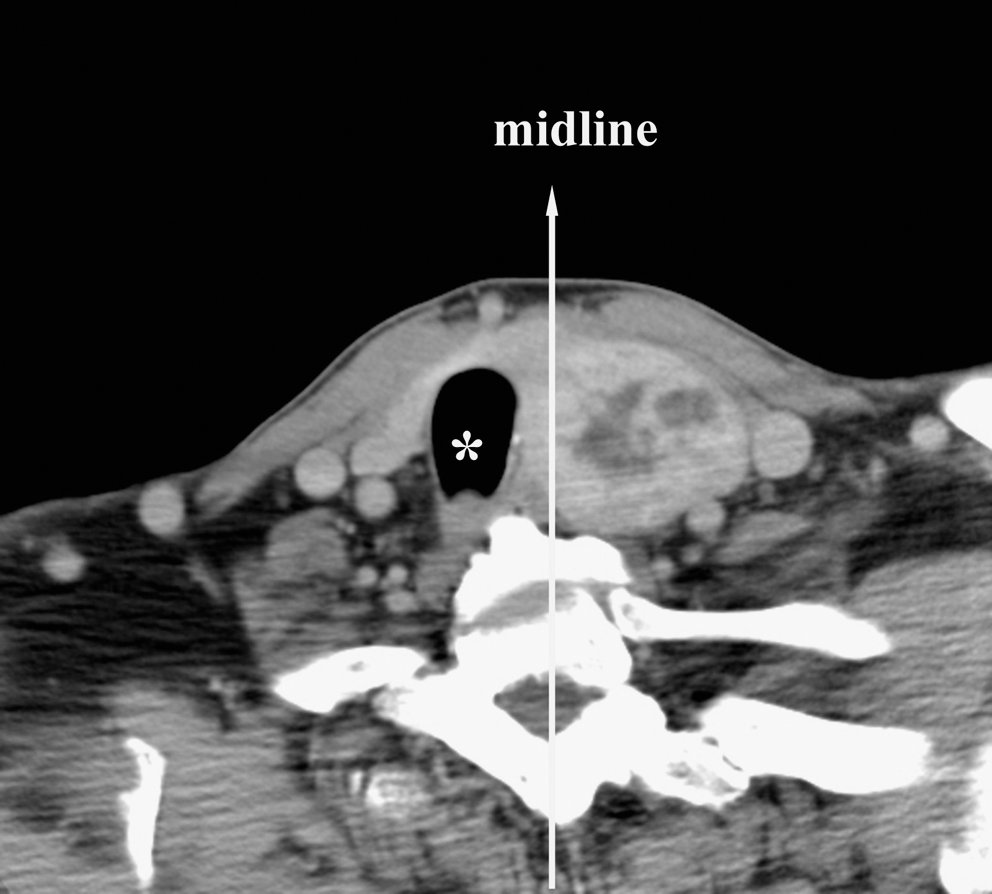
The trachea (asterisk) of patient no. 5 was deviated rightward away from the midline of the neck by left goiter.
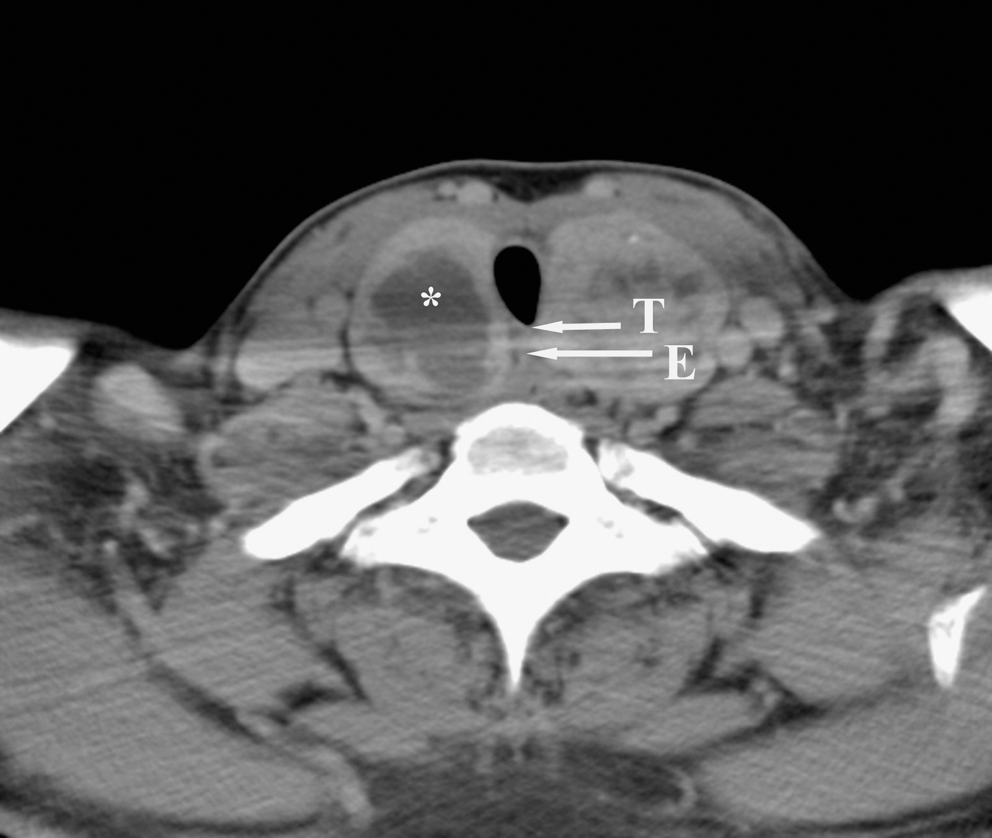
The posterior tracheal wall (short arrow marked with T) and the anterior esophageal wall (long arrow marked with E) of patient no. 1 were separated by tumor extension. Asterisk shows the common feature of cystic change in the right lobe of the thyroid gland.
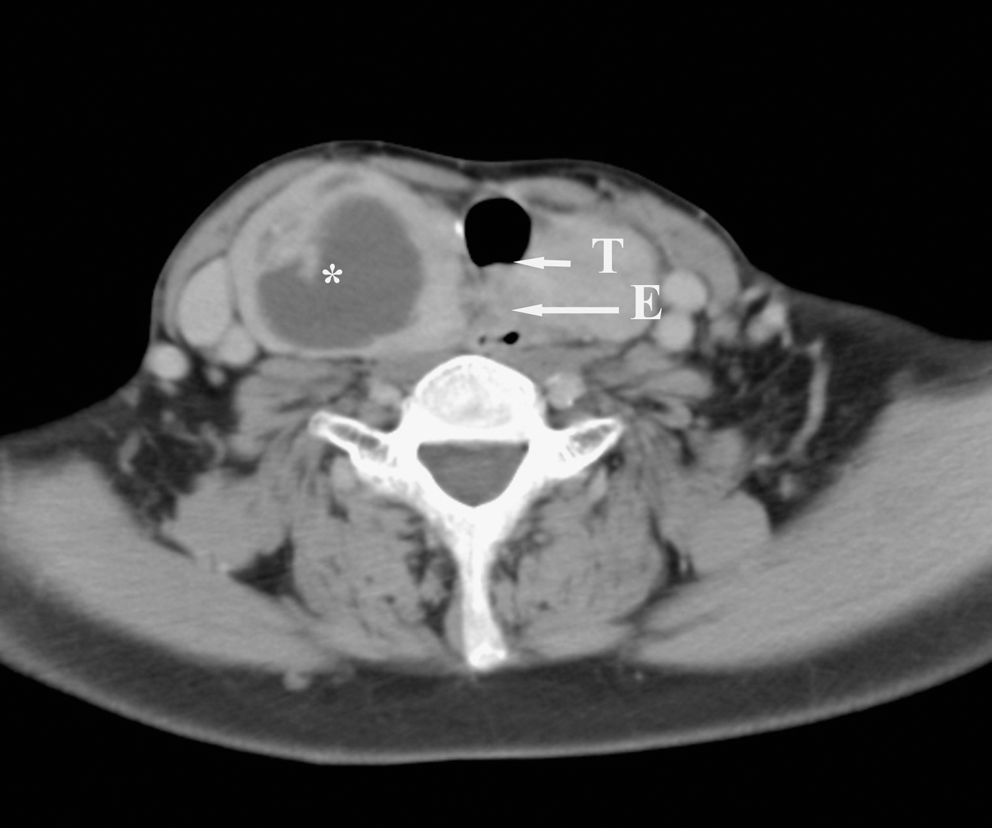
The posterior tracheal wall (short arrow marked with T) and the anterior esophageal wall (long arrow marked with E) of patient no. 7 were separated by tumor extension. Asterisk shows the common feature of cystic change in the right lobe of the thyroid gland.
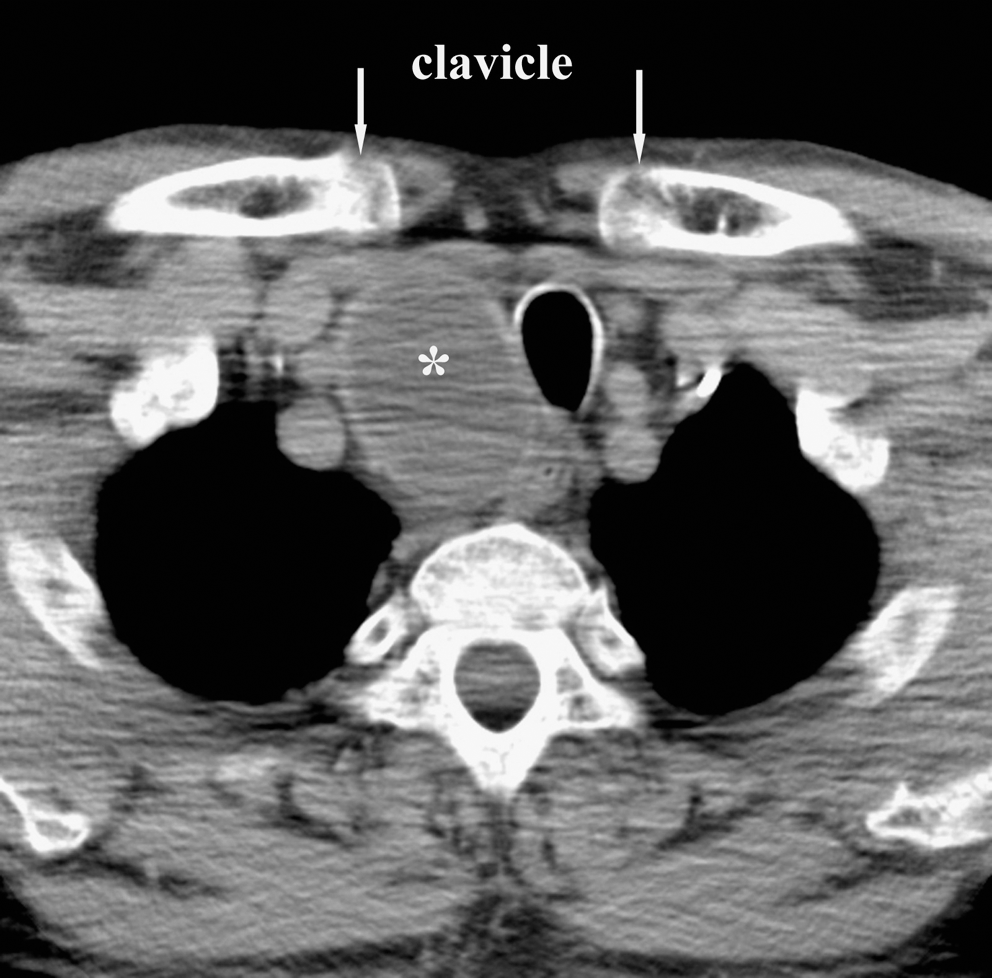
The cystic tumor of patient no. 3 extended to the clavicle (arrows) and into the thoracic inlet. Asterisk shows the common feature of cystic change in the right lobe of the thyroid gland.
CT, computed tomography; Echo, echography; ?, unknown.
FNAC was performed in seven patients with BTD and VFP before thyroidectomy. Six patients had benign results and the results from one patient were inconclusive because of scanty cellularity in the cytology specimen. Tumor specimens from three patients in whom frozen-section analysis was performed had readings of benign goiters in all three cases. The final pathologic reports included five benign goiters, two cases of adenomatous hyperplasia, and one case of Hashimoto's thyroiditis (Table 4).
FNAC, fine-needle aspiration cytology; BG, benign goiter; NA, not available.
Discussion
Vocal fold immobility has multiple etiologies. According to the study by Rosenthal et al. (4), iatrogenic injury during surgery and malignancy, such as lung or esophageal cancer, are the major causes of VFP. However, BTD is not cited as a common etiology of VFP. According to the literature (2,3,5 –10), the prevalence of VFP accompanying BTD varied from 0.69% to 0.96% (Table 5). In comparison, the prevalence in our series was 4.3% (Table 1). Fiberoptic laryngoscopy, which is now a common procedure before thyroidectomy, can detect vocal fold immobility in patients with no or subtle voice symptoms. Randolph (11) also emphasized the importance of routine preoperative laryngeal examination, because voice changes cannot be relied on as a predictor of vocal fold function. For example, one of the eight patients with BTD and VFP had no voice symptoms before thyroidectomy. This may explain the higher prevalence in our study compared with reports that were conducted before fiberoptic laryngoscopy was introduced or popularized. In our series of patients undergoing thyroid surgery, routine laryngoscopy examination revealed that 6.4% (12/187) had preoperative unilateral VFP. Thus, information on preoperative laryngeal function is of extreme importance when planning surgery, especially contralateral surgery. Surgeons must take extreme care when performing contralateral thyroidectomy to ensure preservation of the RLN. Patients also need to understand the potential for permanent tracheotomy if the contralateral RLN is injured during surgery.
BTD, benign thyroid disease.
In previous research, the prevalence of VFP in thyroid cancer widely varied. Raza et al. (1) observed a prevalence of 1.7% (5/300), whereas Chiang et al. (12) determined 9.6% (15/156) prevalence in patients from Taiwan. In the present study, prevalence was 9.5% (4/42). Using fiberoptic laryngoscopy examination, the prevalence of VFP in BTD was 4.3%. According to our findings, VFP does not significantly associate with thyroid cancer (Table 1). This demonstrates that VFP with thyroid tumor is not necessarily indicative of thyroid cancer. Two patients with VFP accompanying BTD were able to recover after thyroidectomy and careful preservation of the RLN. However, if the RLN was accidentally injured, the voice of the preoperatively asymptomatic patient could deteriorate. Although the presence of VFP may suggest malignant disease, it certainly does not prove it. Surgeons should not go into surgery with a preconceived notion of nerve resection of the affected nerve given the potential for benign disease and the potential for vocal cord recovery. It is important to understand the possible features of BTD with accompanying VFP before performing any procedure.
Tables 2 –4 summarize the features of BTD with accompanying VFP observed in this study. Six of the eight patients were older than 60 years, probably because the aging RLN is more vulnerable to compression/stretching. BTD with VFP was more common in female than male adults, but the differences in prevalence between genders need further investigation. One of the patients had no symptom of a husky voice (Table 2). This may be due to a slow-growing goiter in which movement develops in the contralateral vocal fold compensatory to the fold with paralysis. Therefore, absence of voice symptoms does not guarantee that there will be no VFP. To improve the accuracy of diagnosis of VFP, routine preoperative evaluation of vocal fold motion before thyroidectomy is mandatory. The studies by Randolph (11) and Farrag et al. (13) also stressed the importance of preoperative vocal fold examination to appropriately counsel patients on the risks of surgery and to facilitate the planning of surgery.
In this study, goiter was unilateral in six patients and bilateral in two patients. VFP was unilateral in all patients. Worgan et al. (6) reported the cases of two patients with bilateral VFP who both had thyroidectomy decades earlier than the onset of VFP. In the two patients from our study with a history of thyroidectomy, imaging analysis revealed enlarged thyroids, which pinched the tracheo-esophageal groove bilaterally (Figs. 2 and 3). It is possible that RLN decompression may have prevented paralysis of their functional vocal fold. There are other examples of BTD with bilateral VFP. Tsunoda et al. (14) reported a case of Hashimoto's thyroiditis in which vocal fold function returned after thyroidectomy. Krecicki et al. (15) reported a case in which surgery alleviated bilateral VFP in a Graves' disease patient. Previous studies also described cases of VFP contralateral to the goiter. Collazo-Clavell et al. (10) reported two such cases, but it was not clear whether VFP was idiopathic and coincidentally contralateral to the goiter. According to the literature, and from our experiences, VFP is usually unilateral and ipsilateral in BTD. However, as previously described, cases of bilateral VFP do occur. Therefore, we recommend thyroidectomy to aid recovery from VFP and to prevent compression of the contralateral RLN by consequential bilateral VFP.
In previous studies, the rate of RLN recovery ranged from 25% (10) to 100% (9) (Table 5). In the present investigation, the overall recovery rate of RLN function was 25% (Table 2). According to our experience, preservation of the RLN without injury is the prerequsite for vocal fold function recovery. Patients with a history of thyroidectomy usually have severe RLN adhesion that hinders RLN preservation. Thyroidectomy, therefore, might be a poor prognostic factor for recovery of RLN function.
Preoperative radiologic findings usually provide clues about the possible mechanism of VFP. As shown in Table 3, all patients with BTD had at least two of the following image features: tracheal deviation, tracheo-esophageal separation, clavicle extension, and tumor larger than 5 cm in diameter. All of these findings indicated the mechanism of compression or stretching of the RLN and/or its blood supply (5). In addition, rapid tumor growth predisposes the RLN to injury. Hemorrhage into a thyroid cyst (9) or rapid cyst distention due to inflammation could cause sudden compression of the nerve. Imaging analysis revealed that seven patients had cystic changes in the goiter, which might support the aforementioned hypothesis.
Perioperative histopathologic findings can also raise the suspicion of BTD with VFP. In Raza's study (1), cystic lesions as well as benign FNAC findings significantly associated with BTD. These results were similar to our observations (Tables 3 and 4). In patients with undetermined FNAC results, analyzing operative frozen sections facilitated accurate diagnosis. Permanent pathologic reports can confirm a diagnosis of BTD and may help to explain the presence of VFP in some cases. In addition to the mechanism of compression or stretching of the RLN previously mentioned, other possible mechanisms for VFP include thyroiditis, which causes local inflammation followed by edema, thrombosis of the blood supply, or direct involvement of the RLN (Table 4, patient 7) (2,7). Slomka et al. cited perineural fibrosis, calcification, and toxic neuritis as other potential causes of VFP (16). In this study, in the two patients with bilateral thyroid enlargement and thyroidectomy history, previous thyroidectomy might have induced perineural fibrosis and, consequentially, RLN paralysis.
Conclusion
Preoperative unilateral VFP is not uncommon in thyroid surgery. Obtaining information on laryngeal function is of extreme importance when planning surgery, especially contralateral surgery. In patients with thyroid disease, VFP is not necessarily an indicator of malignancy. A huge mass with cystic changes and significant tracheo-esophageal groove compression are the common radiologic features of BTD with VFP. Preoperative FNAC and operative frozen-section analysis can facilitate diagnosis of benign pathology. To increase the likelihood of recovery of vocal fold function, careful preservation of the RLN is mandatory. However, in patients with recurrent goiter and previous thyroidectomy, severe scar adhesion predisposes the RLN to injury and the prognosis for recovery of vocal fold motion is relatively poor.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.