
Abstract
Background:
Pyriform sinus fistulae are the major routes of infection in acute suppurative thyroiditis (AST). There have been only a few reports describing imaging studies in AST. We reviewed our imaging studies in patients with AST to elucidate its features so as to facilitate its diagnosis and treatment.
Methods:
We reviewed ultrasonography (US) examinations, computed tomography (CT) scans, and barium swallow studies performed on 60 patients with the AST who were seen for medical care between 1998 and 2008 and were retrospectively reviewed. All of these patients had pyriform sinus fistulae.
Results:
In the acute inflammatory stage, US showed a hypoechoic lesion spreading in and around the affected thyroid lobe, destruction of the lobe, and abscess formation in the neck. CT scans demonstrated similar features with clearer anatomical involvement and edema in the ipsilateral hypopharynx. These findings allowed easy diagnosis of AST. However, in the early inflammatory stage US showed an unclear hypoechoic area in the affected lobe and CT scans showed a nonspecific low-density area. These findings often led to erroneous diagnoses of subacute thyroiditis. A careful review of the US studies demonstrated that the following findings are characteristic of acute suppurative thyroidits: a perithyroidal hypoechoic space, effacement of the plane between the thyroid and perithyroid tissues, and the hypoechoic lesions being unifocal. The former two are not seen in subacute thyroiditis, and hypoechoic lesions in subacute thyroiditis are usually multiple and often bilateral. In the late inflammatory stage, US and CT scans often showed atrophy and an unclear hypoechoic or low-density area in and around the affected lobe. To detect pyriform sinus fistulae, barium swallow studies are more sensitive than US or CT scans.
Conclusion:
During the acute inflammatory stage of AST, both US and CT scans showed inflammatory processes in and around the affected thyroid lobe, although the CT scans more clearly demonstrate the anatomical locations involved. In the early inflammatory stage, these features may lead to an erroneous diagnosis of subacute thyroiditis. Careful US studies should indicate the correct diagnosis, which can then be proven by a barium swallow study or fine-needle aspiration followed by cytological examination and bacterial culturing.
Introduction
Patients and Methods
Between January 1998 and December 2008, 60 patients with AST due to bacterial infection caused by a pyriform sinus fistula were treated at our hospital. The pyriform sinus fistulae were detected on barium swallow studies in 57 patients, by CT scan findings in 2 patients, and by the observation of pus drainage from the pyriform fossa on endoscopic examination in 1 patient. These 60 patients included 24 males and 36 females with a mean age of 20.6 (range: 2 to 69). Twenty-three were referred to our hospital at or after their first episode of acute inflammation in the anterior neck. Twenty-four patients had experienced two episodes, 4 had experienced three episodes, 2 had experienced four episodes, and 6 had experienced more than five episodes. Of the 60 patients, 44 were referred to our hospital from other hospitals with a diagnosis of AST, 10 were referred with a diagnosis of subacute thyroiditis and were given a prescription of prednisolone, 4 patients had a diagnosis of thyroid tumor, and 1 patient had a diagnosis of infected thyroglossal duct cyst. During the early inflammatory stage, when obvious abscess formation had not yet occurred, eight patients were examined. All eight patients had CT scans, and US was performed in six patients. During the acute inflammatory stage, when abscess formation is obvious, 32 patients were examined. Of these 32 patients, both CT scans and US were performed in 13 patients, CT scans only in 16 patients, and US only in 3 patients. In 29 patients who underwent a CT scan during the acute inflammatory stage, 11 patients were experiencing their first episode of the disease and the other cases (18 patients) had a history of recurrent infectious episodes. During the late inflammatory stage, 57 patients were examined. Of these 57 patients, both CT scans and US were performed in 45 patients, CT scans only in 5 patients, and US only in 7 patients. To identify the fistula during CT scans, some patients were instructed to hold the outer part of a syringe attached to a needle between their lips and to blow into the syringe as if they were inflating a balloon or playing a trumpet (the trumpet maneuver). Barium swallow studies were performed in 27 patients during the early and acute inflammatory stage and in 37 patients during the late inflammatory stage. Some patients underwent repeated examinations. We elucidated the characteristic imaging findings on US, CT, and barium swallow studies during each stage. Two surgeons retrospectively evaluated the images and arrived at a consensus. The present study was approved by the Ethical Committee of Kuma Hospital.
Results
Table 1 summarizes the imaging findings. They are organized according to the stage of inflammation.
CT, computed tomography; US, ultrasound.
Early inflammatory stage
We examined eight patients during the early inflammatory stage. Both US data and CT scan data were available for six patients; CT scans were only available for two patients. They were initially treated at another hospital. US did not show abscess formation in any patient during the early stage. US did show a hypoechoic area, however. There was an obscure border in the affected lobe, a perithyroidal hypoechoic space, and effacement of the plane between the thyroid and perithyroid tissues in 100%, 100%, and 83% of the six patients examined, respectively (Fig. 1a). In the present study, the latter two findings were interpreted as indicating that the inflammation had spread beyond the thyroid capsule. The hypoechoic lesions in the thyroid gland were unifocal in all patients. CT scans showed a nonspecific low-density area in the thyroid lobe, swelling of the thyroid gland, and shifting of the trachea in 100%, 75%, and 63% of the patients examined, respectively (Fig. 1b). These CT scan findings were not necessarily suggestive of suppurative thyroiditis. However, the CT scans also demonstrated edema of the ipsilateral hypopharynx in 75% of the patients examined, which may be specific to thyroiditis caused by a pyriform sinus fistula. There were no signs indicating abscess formation or thyroid shifting combined with abscess formation in any patient. During the early inflammatory stage, US-guided puncture of the affected thyroid lobe was performed in four of eight patients to examine cytology and perform bacterial culture, resulting in a diagnosis of AST.

A 24-year-old woman with AST.
Acute inflammatory stage
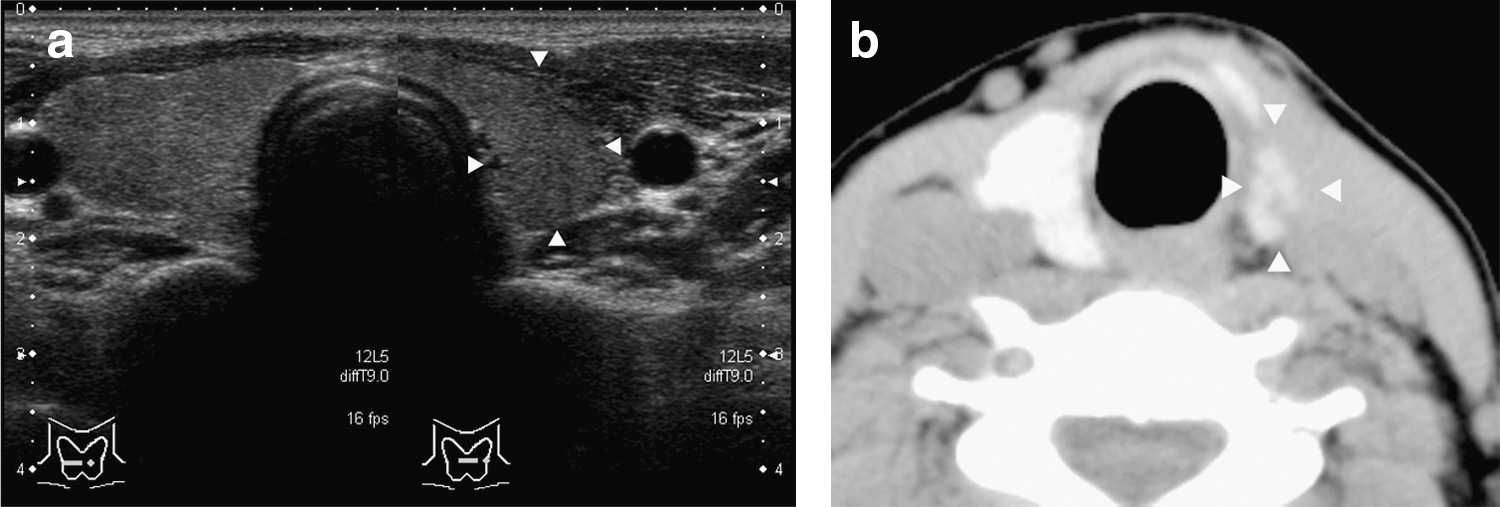
We examined 32 patients during the acute inflammatory stage. Both US data and CT scan data were available for 13 patients, CT scans only for 16 patients, and US only for 3 patients. US showed abscess formation in and/or around the affected thyroid lobe in most of the patients (Fig. 2a). However, whether the abscess occupied mainly the affected lobe or the adjacent structures could not be accurately determined. CT scans demonstrated edema of the ipsilateral hypopharynx, abscess formation, a low-density area in the thyroid lobe, swelling of the thyroid gland, thyroid shifting due to the abscess, and shifting of the trachea in 83%, 97%, 76%, 38%, 41%, and 55% of the patients, respectively (Table 1). The CT scans demonstrated the anatomical location and spread of the inflammation more clearly than the US examinations. Air pockets, air-fluid pockets, and barium density were seen in the abscesses of some patients.
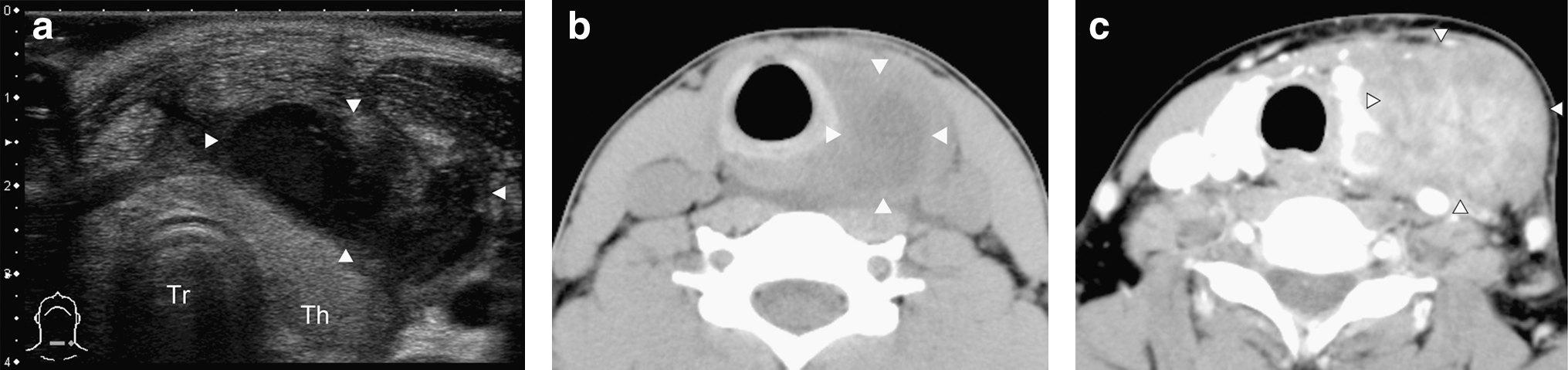
There were several differences between the CT scan findings of primary cases and those of recurrent cases (Table 2). A deformity in the affected lobe and swelling of the affected lobe, which were considered to be an indication of intraglandular abscesses (Fig. 2b), were detected in 91% and 73% of the 11 primary cases, respectively, that is, more frequently than in the recurrent cases. However, dislocation of the affected lobe by the perithyroid abscess (Fig. 2c) was detected in 56% of the 18 recurrent cases, which was more frequent than that in the primary cases.
Late inflammatory stage
We examined 57 patients during the late inflammatory stage. Most of these 57 patients were followed after treatment of the acute inflammation in our hospital, whereas the others were referred to us after entering the late inflammatory stage of the disease. Both US data and CT scan data were available for 45 patients, CT scans only for 5 patients, and US only for 7 patients. US images obtained during the late inflammatory stage demonstrated deformity of the thyroid gland, atrophy of the affected lobe, air pockets in the thyroid gland, and inflammation or scarring of the perithyroid tissue in 71%, 54%, 13%, and 44% of the patients examined, respectively. CT scans taken during the late inflammatory stage showed deformity of the thyroid gland, atrophy in the affected lobe, and inflammation or scarring of the perithyroid tissue in 76%, 60%, and 70% of the patients examined, respectively. US and CT scans performed during the late inflammatory stage showed asymmetric thyroid lobes, due to the atrophy of the affected left lobe (Fig. 3a, b).
Detection of pyriform sinus fistulae
Barium swallow studies showed fistulae originating from the apex of the pyriform recess in most patients. Figure 4b shows a typical case, in which the fistula extended caudally, showed a short narrowing (arrow), and then turned ventrally. In 7 of 27 patients during the early or acute inflammatory stage and 21 of 37 patients during the late inflammatory stage, stenosis of the fistula was detected before it had reached the abscess cavity, which might indicate the crico-thyroid joint (Fig. 4b). The ability of barium swallow studies to detect pyriform sinus fistulae varied slightly with the stage of inflammation. During the early or acute inflammatory stage, fistulae were demonstrated in 24 of 27 patients (89%) examined, whereas during the late inflammatory stage, fistulae were seen in 36 of 37 patients (97%) examined. However, CT scans performed under the trumpet maneuver demonstrated fistulae containing air pockets in 2 of 10 patients (20%) during the acute inflammatory stage and 25 of 46 patients (54%) during the late inflammatory stage, respectively (Fig. 4c, d). In some cases, there was no detectable fistula during the acute inflammatory stage, but fistula was detected upon re-examination during the late inflammatory stage (Fig. 4a, b).
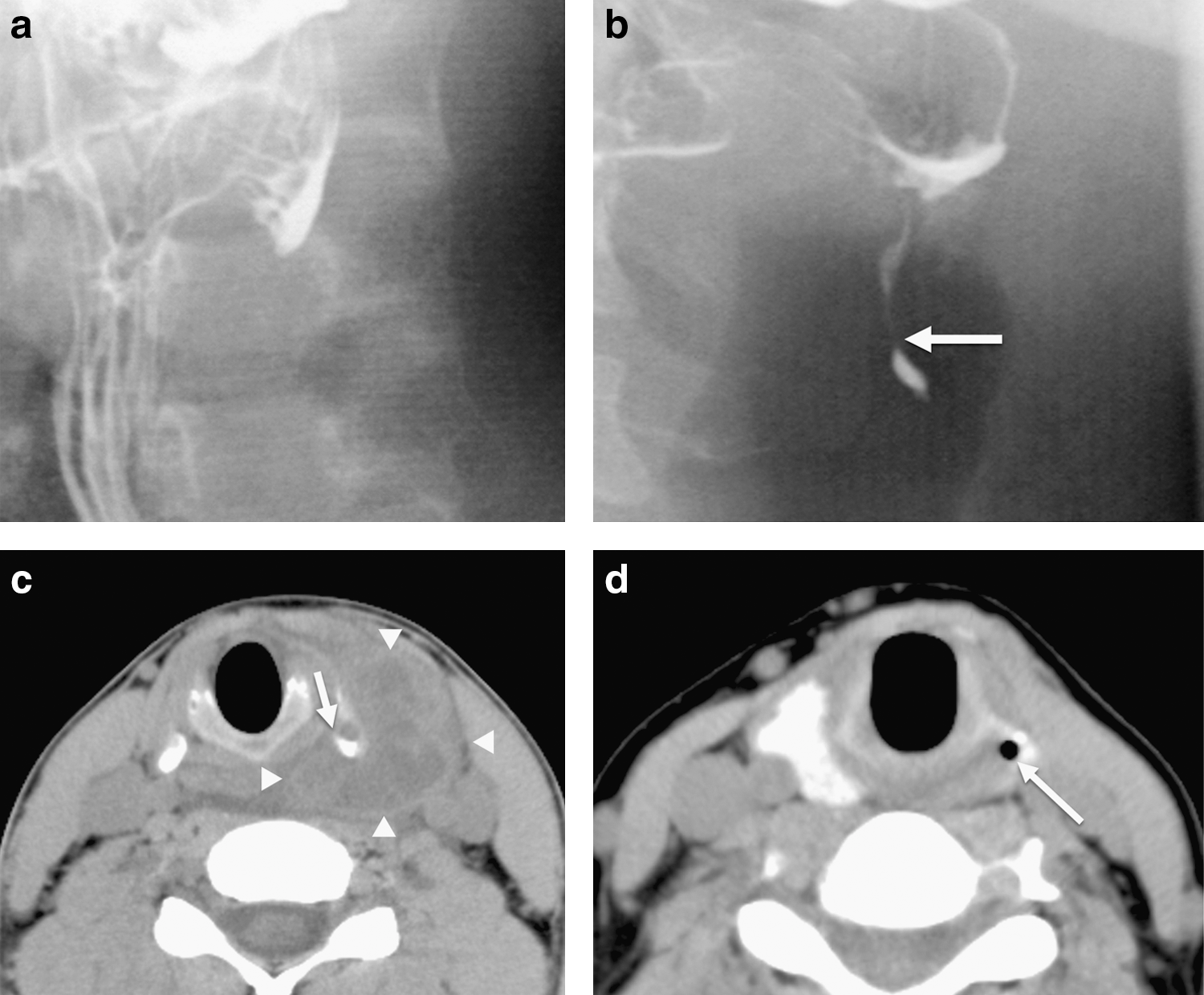
A 31-year-old woman:
Treatment of pyriform sinus fistulae
Thirty-two of 60 patients underwent fistulectomy with or without partial lobectomy of the thyroid. None of the 32 surgically treated patients developed inflammatory recurrence during follow-up. Eighteen patients were treated with chemocauterization of the internal opening of the piriform sinus fistula using trichloroacetic acid. One of the 18 patients treated with chemocauterization developed inflammatory recurrence and was treated again, achieving closure of the internal opening of the fistula. None of the others developed recurrence. The remaining 10 patients are waiting for chemocauterization or undergoing simple follow-up.
Discussion
Pyriform sinus fistulae have been reported as the major route of infection in AST (1). The typical symptoms include a painful anterior neck swelling and fever with an abrupt onset or following an upper respiratory infection. The overlaying skin may be erythematous and edematous, and palpable fluctuation indicates abscess formation. Recurrence is common. Barium swallow studies are useful for detecting such fistulae (2). We previously reported that CT scans obtained under the trumpet maneuver and using air as a contrast medium were able to detect pyriform sinus fistulae and clarify the anatomical path of the fistula, although the success rate of fistula detection was inferior to that of barium swallow studies (3). Bar-Ziv et al. (4), Park et al. (5), and Gan et al. (6) reported imaging studies of AST involving a small number of patients. However, these reports described typical features seen during the acute inflammatory stage, and none of the reports described the early inflammatory stage of the disease. In the early inflammatory stages of the disease, the symptoms include nonspecific inflammation of the anterior neck or thyroid, and it is very difficult to diagnose AST.
In the present study, we divided the timing of examination into three stages, the early inflammatory stage, the acute inflammatory stage, and the late inflammatory stage, to understand the clinical process of inflammation and elucidate the characteristic findings of each stage. We separated the early inflammatory stage from the acute inflammatory stage because the imaging features in the early inflammatory stage are subtler and more important to facilitate early diagnosis and appropriate treatment than those of the acute inflammatory stage. The imaging findings on CT scan obtained shortly after the onset of inflammation were a nonspecific low-density area and slight lobular swelling. Unfortunately, the symptoms detected are not specific to the condition, such as fever, anterior neck discomfort, and sore throat. As it is difficult to distinguish from subacute thyroiditis (7), 7 of 60 patients with AST reviewed in this study had been referred to us under an erroneous diagnosis of subacute thyroiditis and had been prescribed prednisolone. Miyauchi pointed out that the differential diagnosis can be difficult during the early stage of inflammation, especially if it is the first episode and the inflammation is mainly located within the thyroid lobe (8). Makino et al. described the clinical characteristics of AST due to a pyriform sinus fistula as occasional swelling in the neck that is sometimes misdiagnosed as subacute thyroiditis (9). Taking these comments into consideration, it is important to closely examine patients who are difficult to distinguish from subacute thyroiditis, and if necessary to administer antibiotics and drain the abscess surgically. To distinguish AST from other disorders, US images should be examined carefully, as this modality is more capable of diagnosing AST during the early stages of the disease than other imaging modalities. US can demonstrate the collection of small amounts of fluid around the affected thyroid lobe, a small heterogeneous low-density area in the thyroid gland, and whether hypoechoic lesions are unifocal, which are characteristic findings in patients with AST during the early stages of the disease. If necessary, US-guided aspiration of the lesion can be performed to examine the lesion's cytology and allow bacterial culture to be performed or to drain an abscess. In addition, as steroids (which aggravate AST) are often used for the treatment of subacute thyroiditis, caution should be taken to distinguish between these two disorders.
CT scans taken during the acute inflammatory stage demonstrated abscess formation within and around the thyroid gland, destruction of the affected thyroid lobe, swelling of the affected lobe, thyroid shifting due to the abscess, and displacement of the trachea. Although Park et al. and Gan et al. had already reported similar findings, the present study demonstrated how often these findings occurred. Moreover, we demonstrated that the frequency of these findings differs between primary cases and recurrent cases. In primary cases, involvement of the thyroid was often obvious, whereas in recurrent cases, the inflammatory process tended to localize around the thyroid, probably due to fibrosis and scarring from previous episodes. However, none of the previous reports have described this phenomenon.
Barium swallow studies are very sensitive for detecting pyriform sinus fistulae. Concerning the course of the fistula, Takai et al. first reported that the fistula typically ran anterior-inferiorly and then anteriorly along the thyroid (10). In the present study, we found that the fistula often demonstrated a narrow segment around the crico-thyroid joint. From the findings during surgery, we believe that the narrow segment indicates the portion passing into the laryngeal space behind the thyroid lobe. The narrow segment might make the drainage of pus from the pharynx difficult, leading to abscess formation, when inflammation occurs at the peripheral site of the fistula.
Conclusion
During the acute inflammatory stage of AST, both US and CT scans showed the occurrence of inflammatory processes in and around the affected thyroid lobe. The diagnosis of AST can be confirmed by barium swallow studies, which is the most sensitive method of diagnosing the disorder during the acute inflammatory stage as well as during the late inflammatory stage. However, during the early stage, features on US and CT scans may lead to an erroneous diagnosis of subacute thyroiditis, resulting in the prescription of prednisolone, which will have an adverse impact. Therefore, careful US studies should be performed to detect characteristic findings during the early stage. If suspected, barium swallow study or fine-needle aspiration combined with a cytological examination and bacterial culturing might confirm the correct diagnosis of AST.
Footnotes
Disclosure Statement
The authors declare that there are no competing financial interests in relation to this article.