
Abstract
Background:
A “taller-than-wide” shape is associated with thyroid malignancy, but taller-than-wide in which plane is most accurate is unclear. We determined in which ultrasonography (US) plane a taller-than-wide shape is most predictive of malignancy.
Methods:
A total of 471 thyroid nodules from 435 patients were studied. The final diagnosis was based on histopathology in 145 nodules in 120 patients, and cytology in the remaining patients. A taller-than-wide shape was defined as a ratio of ≥1, calculated by dividing the anteroposterior diameter by the transverse diameter. Three criteria were formulated as follows: criterion 1, a taller-than-wide in any plane as a suspicious feature; criterion 2, that in the transverse plane; criterion 3, that in the longitudinal plane. The sensitivity, specificity, positive predictive value, negative predictive value, and area under the receiver operating characteristic curve (Az) were compared among the three criteria.
Result:
Of the 471 lesions, 125 (26.5%) were classified as malignant, and 346 (73.5%) were classified as benign. Criterion 1 showed high sensitivity (68%) and negative predictive value (87.7%), whereas criteria 2 and 3 showed high specificity (83.5% and 94.5%, respectively). The Az vale of criterion 1 was significantly higher than criteria 2 and 3 (p values = 0.0061 and 0.0362, respectively).
Conclusions:
A taller-than-wide shape was a useful US feature for predicting thyroid malignancy. Criterion 1, a taller-than-wide shape in either transverse or longitudinal plane, was most accurate and sensitive for predicting thyroid malignancy among the three criteria.
Introduction
A taller-than-wide shape on two dimensional US refers to a ratio of equal to or greater than 1 as calculated by dividing the anteroposterior diameter by the transverse diameter of the nodule at 90 degrees from the anteroposterior diameter as visualized in the plane. This means that two values for a taller-than-wide shape ratio can be calculated: one for US performed in the transverse (horizontal) plane, and one for US performed in the longitudinal (sagittal) plane. In some studies, a taller-than-wide shape is conferred on a thyroid nodule in either the transverse or longitudinal plane (7,9,10). In other studies, there is no description of whether US was performed in the transverse or longitudinal plane to determine whether the thyroid nodule was a taller-than-wide shape or not (1,4,5). In the revised 2009 management guidelines of the American Thyroid Association (ATA), a taller-than-wide shape is defined in the transverse dimension (14).
Therefore, we have investigated in which US plane a taller-than-wide shape most accurately predicts thyroid malignancy.
Materials and Methods
The institutional review board approved this retrospective observational study and required neither patient approval nor informed consent for the review of their images and records. However, informed consent for the US-guided fine-needle aspiration biopsy (US-FNA) was obtained from all patients before each biopsy.
Study population
This retrospective observational study was performed at Severance Hospital, a referral center in Seoul, Korea, in April 2008. There were a total of 561 thyroid nodules in 555 patients who had consecutive US and US-FNA during the study period. Ninety nodules were excluded from the study, because they did not undergo surgery or follow-up US-FNA after nondiagnostic cytology results. A total of 471 nodules in 435 patients were included in the study. The mean age of the patients in the study was 50.9 years (range, 15–82 years). There were 370 women (mean age, 50.4 years; range, 15–82 years) and 65 men (mean age, 52.3 years; range, 31–73 years). Of the 435 patients, 400 underwent US-FNA for one thyroid nodule, 34 underwent US-FNA for two nodules, and 1 underwent US-FNA for three nodules.
Among the 471 nodules in the study, 339 (72%) had benign cytology results, 98 (20.8%) had malignant cytology results, 20 (4.2%) were suspicious for papillary thyroid carcinoma (PTC), 1 (4.2%) had indeterminate cytology results, and 13 (2.8%) had nondiagnostic cytology results. Thyroid surgery is performed for patients with cytology results of malignancy, suspicious for PTC, and indeterminate. Total thyroidectomy was performed for 91 patients in 116 nodules, and hemithyroidectomy was performed for 29 patients in 29 patients. The final diagnosis of whether the thyroid nodule was malignant or benign was made by histopathology for the 145 nodules in 120 patients. There were 326 nodules in 315 patients in the study that underwent US-FNA only without surgery. In them, the diagnosis of whether they were malignant or benign was made by cytology.
US examination
All gray-scale US examinations were performed using an iU22 5- to 12-MHz linear probe (Philips Medical Systems, Bothell, WA) and an Acuson Sequoia 8- to 15-MHz linear probe (Siemens Medical Solutions, Mountain View, CA). When using the iU22, compound imaging was performed in all patients. US examinations were performed by one of six board-certified radiologists with 1–14 years of experience in thyroid imaging.
US features of thyroid nodules that underwent US-FNA were classified according to the internal component, echogenicity, margin, calcifications, shape, and final assessment. Images of biopsied nodules were obtained with one image in the transverse plane and one image in the longitudinal plane, with one set of images with electronic calipers and one set of images without electronic calipers. US features suspicious for malignancy were classified using our previously published criteria: marked hypoechogenicity, microlobulated or irregular margins, microcalcifications, and a taller-than-wide shape (7). Final assessments were classified as either suspicious or probably benign. When thyroid nodules showed one or more of the suspicious malignant US features, they were classified as suspicious. When the thyroid nodules showed none of the suspicious features, they were classified as probably benign.
Ultrasound-guided fine-needle aspiration biopsy
The same radiologists who performed the US examinations performed the US-FNAs. US-FNAs were performed on either the thyroid nodules assessed as being suspicious on US or the largest of thyroid nodules assessed as being probably benign. US-FNA was not performed on entirely cystic nodules. US-FNA was performed with a 23-gauge needle attached to a 2 mL disposable plastic syringe using a free-hand technique. Each lesion was aspirated at least twice. Aspirated material was expelled on a glass slide and immediately placed in 95% alcohol for Papanicolaou staining. A small portion of the aspirated material was rinsed with saline and processed for cell block. The cytopathologist was not on site during the aspiration procedure. Additional special staining was performed according to the requirements of the cytopathologists.
Retrospective review of images and statistical analysis
For this study, one radiologist (M.H.J.) with 7 years of experience in thyroid imaging retrospectively reviewed the US examinations with digitized static images on the 5,000-pixel monochrome liquid crystal display monitor (ME1i2-BC; Totoku, Electric Co., Tokyo, Japan) of a picture archiving and communicating system. The US examinations of thyroid nodules were routinely performed in both the transverse and longitudinal planes. A taller-than-wide shape was defined as a ratio of the anteroposterior diameter to the transverse diameter of ≥1 (Fig. 1).
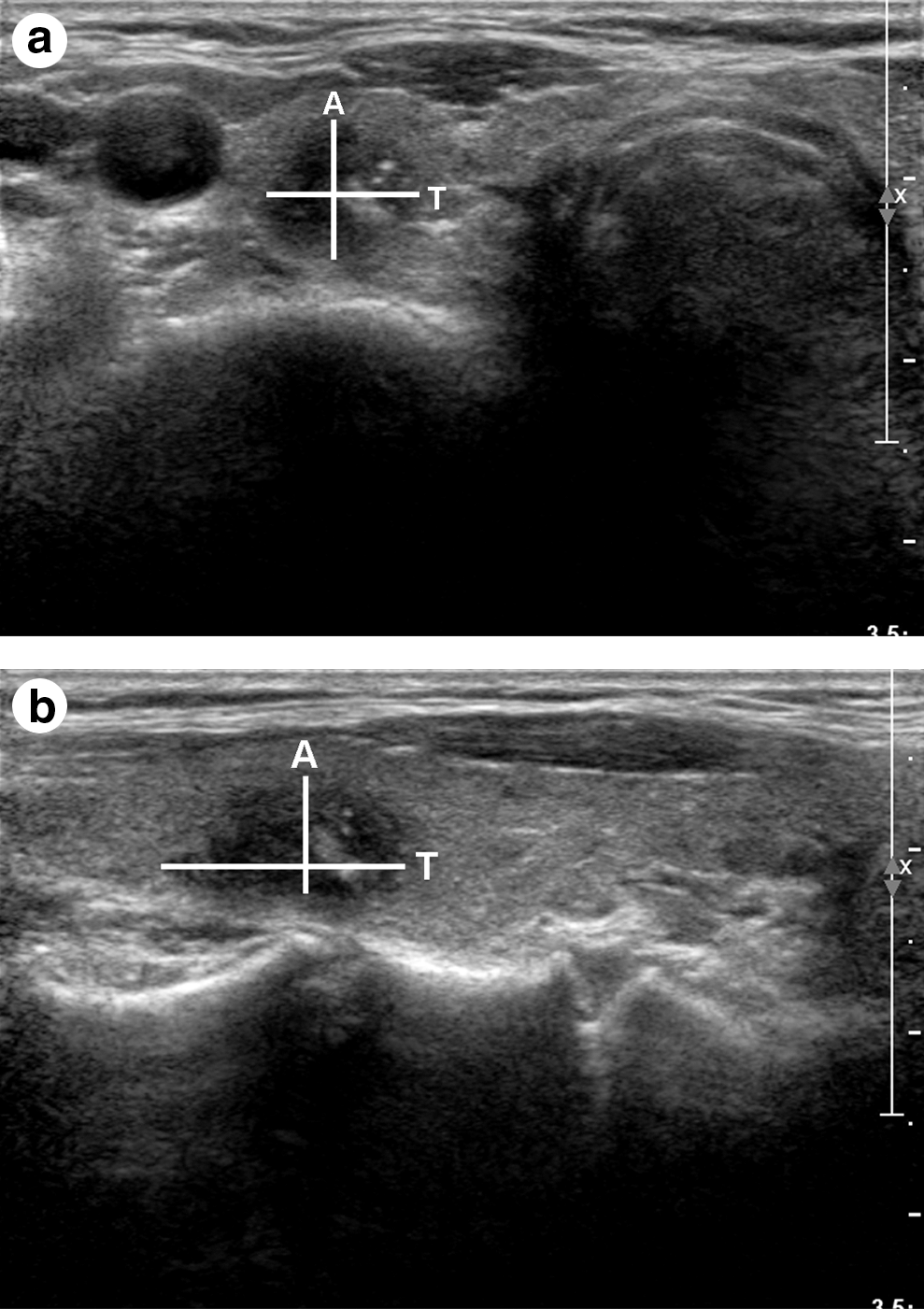
Transverse and anteroposterior diameters of thyroid nodules on the
Three criteria were designated relating to a taller-than-wide shape in transverse and longitudinal planes as follows: criterion 1, a taller-than-wide shape in either transverse or longitudinal plane; criterion 2, a taller-than-wide shape in the transverse plane but not the longitudinal plane; and criterion 3, a taller-than-wide shape in the longitudinal plane but not the transverse plane.
The final diagnosis to determine whether a thyroid nodule was benign or malignant was based on cytology and histopathologic reports. Of the 471 nodules in 435 patients in the study, the final diagnosis was based on histopathology in 145 nodules in 120 patients and on cytology in 326 nodules in 315 patients. In 326 nodules in 315 patients in whom the final diagnosis was based on cytology, the cytology readings were benign in 321 nodules in 310 patients and PTC in 5 nodules in 5 patients. Benign cytology included adenomatous hyperplasia in 229 nodules in 288 patients and lymphocytic thyroiditis in 22 nodules in 22 patients.
An independent two-sample t-test was used to compare patient age and nodule size on US between malignant and benign lesions. Associations between criteria 1, 2, and 3 and malignancy were calculated using a chi-square test. Receiver operating characteristic (ROC) curve analysis was also used to compare diagnostic performance. The diagnostic performance of each of the three criteria were reported as sensitivity, specificity, positive predictive value, negative predictive value, and area under the ROC curve (Az) with 95% confidence intervals. Statistical significance was determined as a p-value less than 0.05. Statistical analyses were performed using SAS statistical software (SAS system for Windows, version 9.1.3; SAS institute, Cary, NC).
Results
Of 471 nodules, 125 (26.5%) were malignant and 346 (73.5%) were benign. The age of patients was not significantly different in those having malignant and benign lesions (p = 0.563) (Table 1). The mean size of malignant nodules was significantly smaller than that of benign nodules (p < 0.0001).
Criterion 1: A taller-than-wide in any transverse or longitudinal plane.
Criterion 2: A taller-than-wide in the transverse (horizontal) plane.
Criterion 3: A taller-than-wide in the longitudinal (sagittal) plane.
Malignancy was diagnosed by histopathology (n = 120) or cytology (n = 5).
There were 147 nodules that met criterion 1, 129 nodules that met criterion 2, and 76 nodules that met criterion 3. Nodules that met any of the three criteria were more frequent among malignant than benign nodules (p < 0.0001) (Table 1) (Figs. 2 and 3). The meeting of criterion 1 had a high sensitivity (68%) and negative predictive value (87.7%) for predicting malignancy. The meeting of either criterion 2 or 3 had a high specificity for predicting malignancy (83.5% and 94.5%, respectively) (Table 2). On the ROC curve analysis, the Az values for meeting criteria 1, 2, and 3 were 0.7504, 0.7096, and 0.6925, respectively. The Az value for meeting criterion 1 was significantly higher than those values for meeting criteria 2 and 3 (p = 0.0061 and 0.0362, respectively). There were 40 malignancies that did not meet criterion 1 (32%, 40 of 125 malignancies), 52 malignancies that did not meet criterion 2 (41.6%, 52 of 125), and 70 malignancies that did not meet criterion 3 (56%, 70 of 125).

A 49-year-old woman underwent a routine evaluation. An approximately 12 mm papillary thyroid carcinoma in the left thyroid gland showed
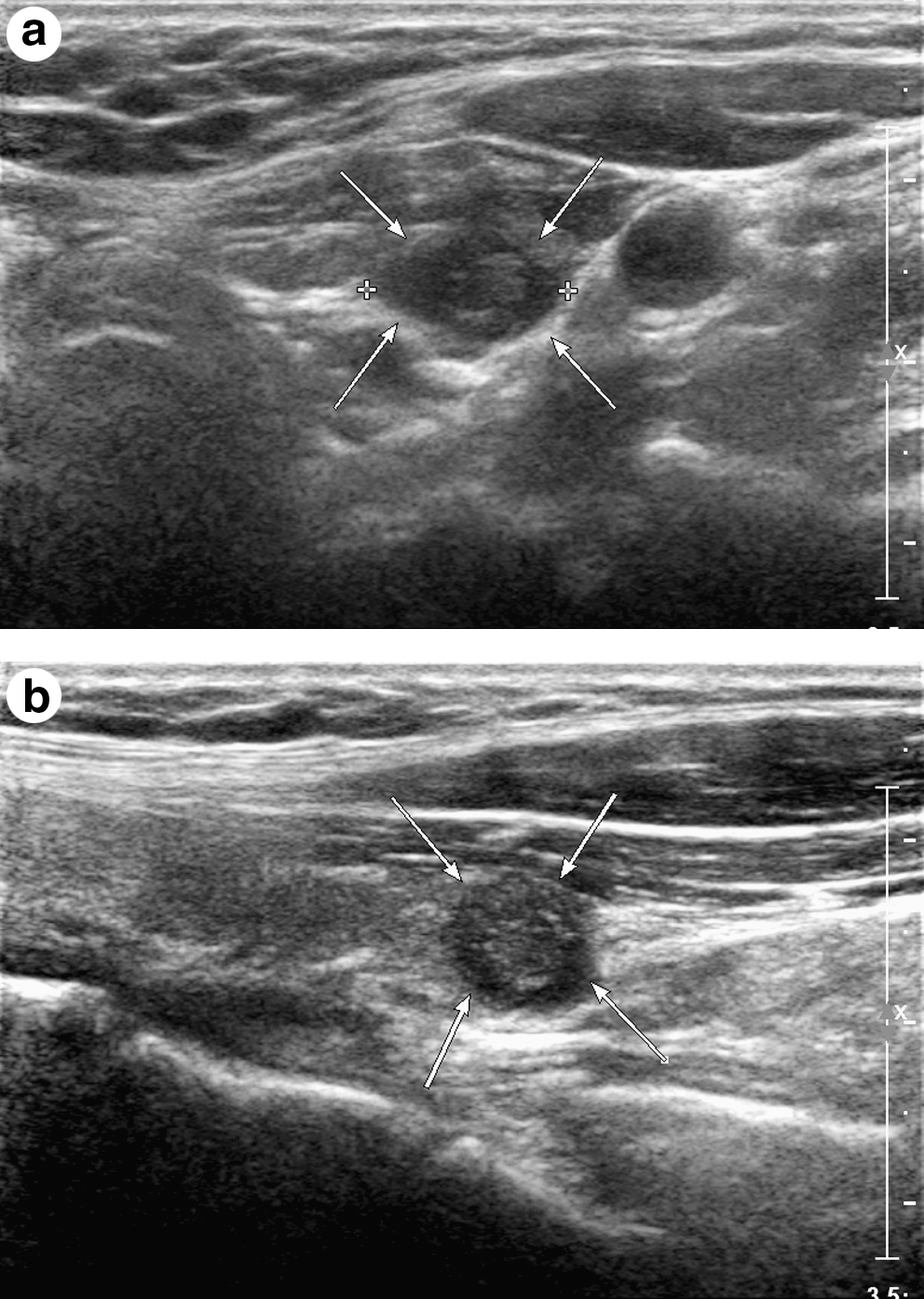
A 49-year-old woman underwent a routine evaluation. An approximately 11 mm papillary thyroid carcinoma in the left thyroid gland showed
Criterion 1: a taller-than-wide in any transverse or longitudinal plane as a suspicious feature.
Criterion 2: a taller-than-wide in the transverse plane as a suspicious feature.
Criterion 3: a taller-than-wide in the longitudinal plane as a suspicious feature.
p-Value was from ROC comparison with criterion 1.
Az, area under the ROC curve; NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic.
Discussion
Out of multiple suspicious US features, such as microcalcifications, hypoechogenicity, irregular margin or no halo, solidness, and a taller-than-wide shape (1 –7,9 –13), a taller-than-wide shape can be used independently to differentiate malignant from benign nodules (1,4,5,7,9,10). In some studies, a taller-than-wide shape is the best predictor for malignancy (5), and the use of a taller-than-wide shape accompanied by at least two additional suspicious malignant US features may represent the best compromise between false-negatives and cost-benefit considerations (4). In a number of studies, the range of sensitivity, specificity, positive predictive value, and negative predictive value of a taller-than-wide shape were 32.7%–83.6%, 60%–92.5%, 8.3%–77.4%, and 67.4%–98%, respectively (4,5,7,10).
To provide high-quality US examinations, the American Institute of Ultrasound in Medicine (AIUM) published guidelines for the performance of US examinations of the thyroid and parathyroid (American Institute of Ultrasound in Medicine 2003) (15). According to the AIUM guidelines, the thyroid gland should be imaged and recorded in at least 2 projections, transverse and longitudinal planes, and suspicious US features are usually assessed in both planes (15). A taller-than-wide shape is defined as being present on any plane in a few studies (7,9,10), and the transverse or longitudinal plane is not described in other studies (1,4,5). However, according to the ATA guidelines, a taller-than-wide shape is defined as “a shape taller than the width measured in the transverse dimension” (14). Therefore, we have investigated in which US plane a taller-than-wide shape most accurately predicts thyroid malignancy.
The range of sensitivity, specificity, positive predictive value, and negative predictive value of our three criteria were comparable to previous studies (sensitivity of 41.6%–68%, specificity of 82.1%–96.2%, positive predictive value of 56.2%–57.8%, and negative predictive value of 82.4%–87.7%) (4,5,7,10). The Az value of criterion 1 was 0.7504, significantly higher than the Az values of criteria 2 and 3, 0.7096 and 0.6925, respectively (p = 0.006 and 0.036). Meeting criterion 1 had the highest Az value and the least false negatives among the three criteria. Meeting criterion 1 was associated with only 32% (40/125) false negatives, whereas meeting criteria 2 and 3 was associated with 41.6% (52/125) and 56% (70/125) false negatives, respectively. Therefore, meeting criterion 1 was the most accurate for predicting thyroid malignancy.
The mechanism by which malignant thyroid nodules grow across normal tissue planes has not been defined. However, a recent study by Yoon et al. supported the conclusion that a taller-than-wide shape in malignant thyroid nodules and a wider-than-tall shape in benign nodules are related to the ability of the probe to compress the thyroid nodule during the US examination (16). Since the benign nodules and cystic nodules are softer and infiltrate less into the surrounding tissue, benign nodules, especially those located in the anterior portion of the thyroid, are more easily compressed than malignant nodules (16). Therefore, a taller-than-wide shape appears to be lost during the US examination of benign nodules (16). The most common malignancy of the thyroid gland is PTC. Dense fibrosis is seen in 56%–89% of PTCs (17 –19). Dense fibrosis in a PTC may be the main cause of decreased compressibility when compared with benign nodules, which results in a taller-than-wide shape.
Our study had several limitations. First, the reference standard in our study was cytology with the exception of the 144 nodules that underwent surgery. Thyroid nodules with malignant and benign cytologic results without surgery were included, and there is the possibility of false-negative and false-positive cytologic results. Second, the diagnosis of thyroid nodules and recommendation for US-FNA is usually based on the combination of suspicious features of marked hypoechogenicity, microlobulated or irregular margins, microcalcifications, and a taller-than-wide shape. Given that only a taller-than-wide shape was considered in this study, bias may exist.
In conclusion, a taller-than-wide shape on US was a useful US feature for predicting thyroid malignancy. A taller-than-wide shape on US in either the transverse or longitudinal plane (criterion 1) was the most sensitive and accurate for predicting malignancy among three criteria, so it seems important to evaluate this finding by both transverse and longitudinal US.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.