
Abstract
Background:
Interpreting I-131 whole-body scans (WBSs) after thyroidectomy for thyroid cancer is not simple. There are scans in which interpretation is speculative because of cryptic findings (CF). Complexity is added in scans that are done a week after an ablative or therapeutic dose of I-131 because not only is I-131-labeled thyroxine (T4) distributed throughout the body, but inorganic I-131 that is derived from the de-iodination of T4 may be also detected. We present our observations regarding the analysis of CF on WBS using I-131 single-photon emission computed tomography (SPECT) in fusion with noncontrast computed tomography (CT), referred to here and elsewhere as I-131 SPECT/CT.
Methods:
Forty of 184 WBSs in 38 thyroidectomized thyroid cancer patients were followed up with I-131 SPECT/CTs. The SPECT/CT images were acquired after a tracer dose of I-131 (n=82) or a week after an ablative or therapeutic dose of I-131 (n=102).
Results:
Among 184 WBSs, 40 (22%) had CF. In 35 patients the WBS was negative for metastatic disease except for the CF and 5 patients had evidence of thyroid cancer in addition to the CF. There were 49 CF in the planar scans that were localized by SPECT/CT. These were characterized as physiological uptake in gingiva, thymus, gall bladder, menstrual blood, uterine fibroid, recto-sigmoid, colon, and bladder. Also observed was uptake in sites that represented nonthyroidal pathology including dental abscess, hiatal hernia, renal cyst, and struma ovarii. SPECT/CT suggested that 10 of the CF were actually of thyroid origin. In 40 SPECT/CT scans, the images contributed to interpreting the scan. In 15 of 40 patients the SPECT/CT analysis of WBS was performed with tracer doses of I-131 and was important for determining whether to administer ablative I-131 treatment. In another 25 patients, in whom SPECT/CT was performed after ablative or therapeutic doses of 131-I, information regarding the characterization of CF by SPECT/CT was useful in determining if thyroid cancer metastases or thyroid remnants were present.
Conclusions:
I-131 SPECT/CT is a useful tool to characterize atypical or CF on WBS by differentiating thyroid remnant or cancer from physiologic activity or nonthyroid pathology. In the past, uptake on a WBS that was not explicable as physiologic activity was identified as putative or possible thyroid cancer and generally was treated with I-131. Now, by identifying activity in some possible cancer sites as not thyroid cancer, SPECT/CT can reduce inappropriate treatment with I-131. SPECT/CT of WBS performed after ablative doses of 131-I is useful in determining the nature of CF and therefore likely providing prognostic information.
Introduction
The utility of a planar WBS derives from the unique ability of postoperative benign thyroid tissue remnants and cervical or distant metastatic foci of differentiated thyroid cancer to concentrate and organify iodide (I−) and to store it as thyroxine (T4). A WBS also identifies as landmarks I-131 I− or I-131-labeled T4 in the circulation, and is thus helpful to orient interpretation of the images. Yet, regions that are rich in blood such as the lungs, heart, and inflamed hypervascular sites may provide a source of confusion between the normal and the pathologic.
There are nonthyroid organs that concentrate iodide but do not synthesize T4 from the I-131 I−. These organs comprise the salivary glands, stomach, kidneys, breasts, sweat glands, hair follicles, choroid plexus, and the thymus.
They and their I-131-containing secretory/excretory products in saliva, sweat, milk, urine, and stool, are imaged on I-131 WBS. Radioactive urine and saliva are usually detected in their physiologic anatomic sites but also may be the source of artifactual contamination on the skin, clothes, and hair. Anomalous thyroid tissue like thyroglossal duct, substernal thyroid, and struma ovarii may also be detected.
The different dynamics of I-131 I− and I-131-labled T4 and the effects of a euthyroid or hypothyroid metabolic state impact on the appearance of a WBS in ways that is often stereotypical but at times unexpected. The residence of radioactivity in the extrathyroid sites is usually of relatively short duration. These organs remove iodide from blood independent of thyrotropin (TSH) stimulation in direct proportion to its concentration in the blood. Since 90% of renal iodide clearance from the blood is accomplished within 24 hours in a euthyroid individual and within several days in hypothyroid patients, radioiodine in the blood-pool and the extrathyroid concentrating sites are imaged decreasingly with the passage of a few days. When there is no thyroid tissue, the blood pool of the head and neck, parotid and submandibular salivary glands, oral cavity containing 131 I−-labeled saliva, and the nasal/sinus mucosa are apparent. At 48 hours, if rTSH was used to secure TSH elevation, the nontumor sites of activity generally will have decreased considerably. In contrast, if hormone withdrawal and hypothyroidism are employed, these sites will be quite apparent at 48 hours. The rest of the WBS is done usually at or after 48 hours to take advantage of loss of background, which enhances the signal-to-noise ratio. The activity of 131 I− may still be seen in the systemic circulation, the stomach, the urinary bladder, and variably the gastrointestinal tract. Activity in the sites diminishes in the ensuing day in euthyroid patients but may persist for several days in the hypothyroid state or when there is renal failure.
When there are benign and/or malignant thyroid cells and TSH is elevated, the 131 I− is usually converted to T4, which has a longer effective half-life in the body than 131 I−. The newly produced I-131-labeled T4 will be present as well as the 131 I− and will behave as described above. In addition, I-131-labeled T4 will be secreted into the blood and cleared from the blood, notably by the liver where it is glucuronidated, secreted via the bile ducts, and reabsorbed from the intestine to the blood, which is called the enterohepatic circulation of T4. Thus, the liver may be imaged on a WBS if there is functioning thyroid tissue but only after formation of thyroid hormone has occurred. In the absence of normal thyroid tissue, observation of the liver implies functioning thyroid cancer (see Patient #1, Appendix). A portion of this I-131-labeled T4 is not absorbed into the blood, is excreted in the stool, and may confound interpretation of a WBS by bowel activity, particularly the recto-sigmoid colon. If a thyroid remnant or even T4 producing thyroid cancer is present, the extrathyroid organs may be normally imaged even after a week or more. We and others ascribe this phenomenon to a second phase of inorganic I-131 I− in the circulation that derives from the deiodination of I-131-labeled T4 produced by a thyroid remnant or cancer. Imaging of the liver is common after diagnostic I-131 WBS and post-I-131 WBS. Although this does not correlate well with measures of thyroid tissue mass in thyroid cancer patients (1) we generally interpret hepatic uptake of I-131 that occurs 3 or more days after a WBS as evidence for residual thyroid tissue, either benign or malignant.
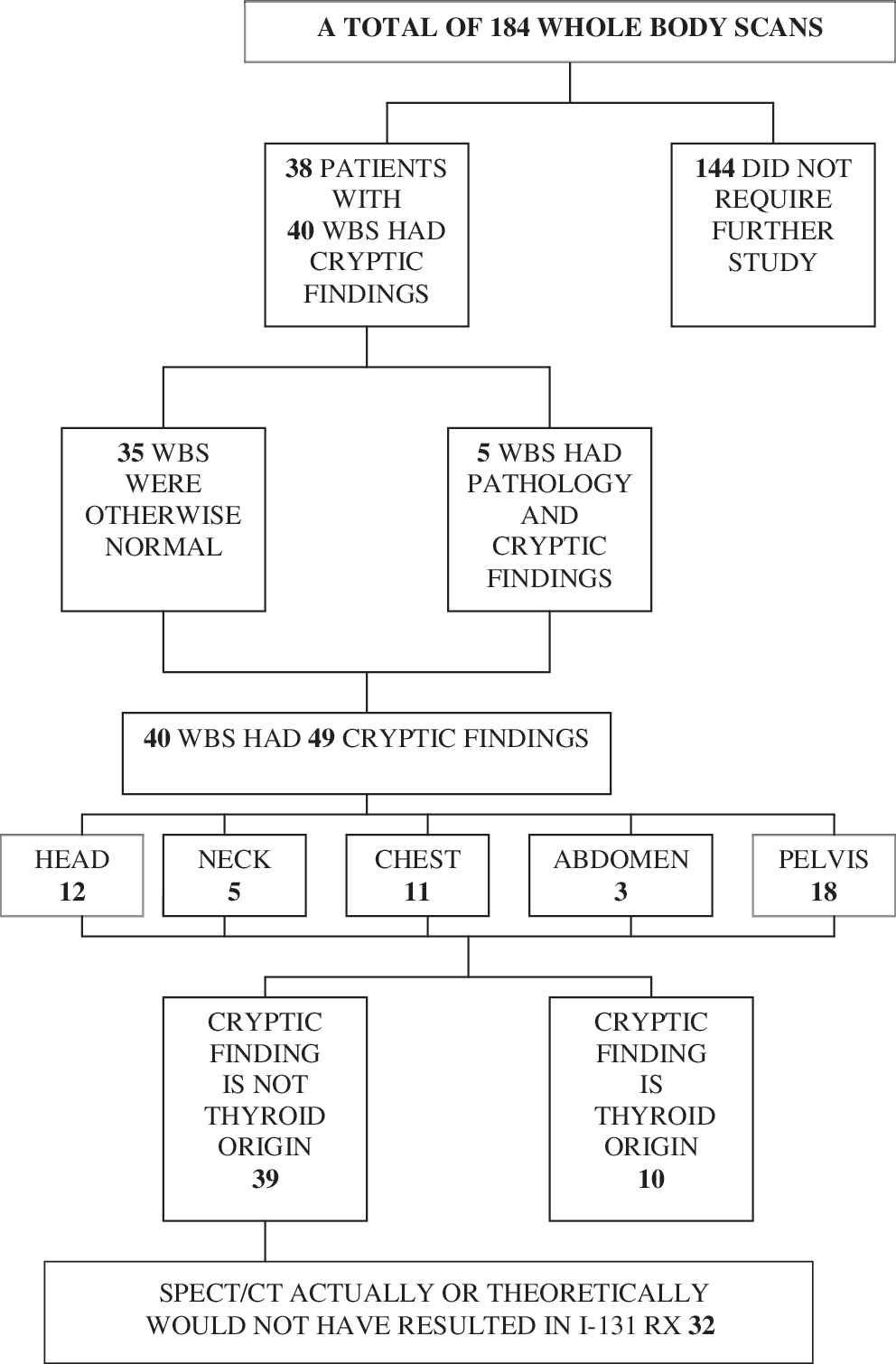
Flow diagram illustrating the frequency and location of cryptic findings on I-131 whole-body scan (WBS) that were further evaluated by SPECT/CT.
Several other factors often contribute to uncertainty in the interpretation of WBS. In the chest, bewildering radioactivity may be attributable to I-131 in the esophagus due to swallowed saliva, the cardiac blood pool, the thymus, and I-131 in the breasts. Breast activity is seen mainly during lactation but also occurs in the nonlactating state, when it may be unexpected, and the images may be asymmetrical. The image of the breasts may mimic pulmonary metastatic lesions unless proper imaging maneuvers that separate lung and breast are made. In the pelvic region confusion may be generated by radioactive urine in the bladder; isotope in the female reproductive organ blood, which has been poorly described in the literature, in struma ovarii, and in the stool.
Technologic innovations have enhanced the information derived from WBS. I-131 single-photon emission computed tomography (SPECT) improves localization of functional data from a WBS. X-ray noncontrast computed tomography (CT) reveals precise anatomic detail but does not detect radioactive emission. Computer-assisted fusion of the two types of images (SPECT/CT) combines thyroid functional images with anatomic images and thus has been reported to be feasible and to have a positive impact that can improve interpretation of a WBS (2 –14) by correctly assigning an organ, lymph node, or blood pool to a focus of I-131 activity.
We have investigated if sequentially acquired SPECT/CT images from a single scanner can offer novel physiologic-anatomic insight to improve the interpretation of a WBS with CF and provide therapeutic advantage after a thyroidectomy for thyroid cancer.
Materials and Methods
This was a Health Insurance Portability and Accountability Act (HIPAA)–compliant, New York University (NYU) Institutional Review Board (IRB)–approved study.
Patients
We performed a retrospective image analysis of our database of 184 thyroid cancer patients who underwent WBS from January 2008 to August 2009. Their endocrinologists had ordered the examination as a part of regular endocrine management after a total thyroidectomy had been performed for differentiated thyroid cancer.
TSH elevation was obtained either by withdrawing thyroid hormone or by administering recombinant TSH (rTSH, Thyrogen®). In all patients TSH was over 40 mIU/mL. When T4 withdrawal was employed, TSH and thyroglobulin (Tg) were assayed before isotope administration, and when rTSH was used, TSH and Tg were assayed on days 3 and 5, of the standard protocol. The patients were not pregnant or nursing. Radiation safety precautions were utilized. The patients had been consuming a low iodine diet and refrained from sources of iodine contamination such as radiographic contrast agents, or dietary supplements. Iodine deprivation was confirmed by assessing 24-hour urinary iodine excretion when there was any doubt of contamination, based on history. The patients were instructed to cleanse the bowel and to urinate before a WBS.
The endocrinologist managing each patient ordered ultrasonography of the neck, regional CT (without contrast), MRI, PET, or other diagnostic procedures, as clinically indicated. The results of these tests were correlated with our findings if clinically appropriate.
Imaging technique
Scans were performed either after a 2 mCi or less (range: 1.45–2.0; mean: 1.88) diagnostic (tracer) dose of I-131 or after an ablative or a therapeutic dose of 50–248 mCi (mean 135.6) I-131. I-123 was not employed in this investigation.
Technique of planar WBS
The WBS images were acquired using either a Siemens Ecam or Symbia dual-head system. Whole-body acquisition was performed using a 256×1024 matrix size, zoom of 1.0, a scan speed of 5 cm/min, and a total scan length of 200 cm. Static images were acquired for 10 minutes with a 256×256 matrix size and a zoom of 1.0. High-energy collimators were employed in both studies and the detector configuration was 180°.
The WBS was done from the top of the head to the toes. The arms were imaged. Spot views were obtained as requested by the nuclear medicine physician. The scan and/or spot views were repeated when needed after bowel preparation, or urination when needed to cleanse the colon of feces, or void the bladder of urine, respectively. Contamination of the surface of the body was removed by showering. When there was a linear focus of radioactivity in the lower part of the neck or the upper part of the mediastinum, particularly if it was located just to the left of the midline, the patient was given a drink of water and subsequently asked not to swallow for the duration of a regional scintiscan to exclude retained I-131-saliva in the esophagus. When there was radioactivity in the chest that corresponded to the breast regions, a scan of the chest was performed in both lateral projections with the patient leaning forward at a 45° angle.
One of three experienced nuclear medicine physicians (K.F., S.T., and M.B.) initially interpreted the planar WBS images as part of routine clinical care. A report was issued when there was confidence in the assessment of the localization of the isotope. Then, management by the endocrinologist proceeded without additional nuclear imaging. When focal iodine localization was anatomically ambiguous or atypical on a planar WBS, the foci in question were classified “cryptic” and an I-131 SPECT/CT was performed on the same or next day. For the retrospective study, all three authors together reviewed the original planar images obtained in all patients who underwent SPECT/CT and recorded the location and number of cryptic foci. There was no disagreement among them.
I-131 SPECT/CT images
SPECT/CT images were acquired using a Siemens Symbia T6 SPECT/CT scanner consisting of a traditional dual-head gamma camera coupled to a 6 slice helical CT scanner. CT images were acquired using a 6×5 mm CT detector configuration and Siemens Care Dose 4D dose modulation. Images were reconstructed using a 5 mm slice thickness and 2.5 mm slice interval. SPECT images were acquired using a 360 degree rotation, 128 stops, 128×128 matrix size, and 40 seconds per frame, and were generated using iterative reconstruction and CT attenuation correction. For low count studies, Siemens eSoft processing software was used to multiply the raw planar tomographic images by a factor of 2x–4x before reconstruction. SPECT/CT images were interpreted in a joint reading session conducted by the authors (K.F., S.T., and M.B.). There were no disagreements regarding interpretation.
Results
A schematic of the data are shown in Figure 1. A total of 184 WBS were performed, 144 of which (78%) did not require further study. Eighty-two of the 184 patients had the scan shortly after thyroidectomy. Forty-two of them were prepared for the scan by withdrawing suppressive therapy (withdrawal) and therefore were hypothyroid. Forty were prepared with rTSH, in whom levo-T4 was continued; these patients were euthyroid. One hundred two patients had the WBS 1 week after therapeutic I-131 (after either ablative therapy, which is I-131 that is designed to destroy a remnant of thyroid tissue in the thyroidectomy bed or the thyroglossal duct, or after treatment of recurrent local or metastatic thyroid cancer).
Thirty-eight patients had 40 I-131 SPECT/CT scans because there were CF on the tracer planar I-131 WBS. Of these 40 I-131 SPECT/CT scans, 15 were performed after a diagnostic dose of I-131 (2 mCi or less), and 25 were performed after ablative or therapeutic doses of I-131 50–248 mCi (mean 135.6). The Appendix is a sequential list of these patients in the chronological order in which they presented to our laboratory for WBS, except when several scans were done on the same person, the studies are grouped together. Generally, each patient had a SPECT/CT of a single anatomic region but two patients had SPECT/CTs, of two separate anatomic regions. Thirty-five of the 40 problematic WBS were otherwise without abnormality and 5 had thyroid cancer metastases as well as additional radioactive foci that were difficult to diagnose and thus were classified as cryptic. There were 44 CF in total among the 35 scans that had only CF. The cryptic radioiodine foci on WBS were located outside of the regions that normally accumulate inorganic I-131 iodide (I−), the liver that accumulates I-131-labeled T4, or outside the time frame in which those materials would be reasonably expected, as will be discussed below and summarized in Table 1. There were 49 such instances on the WBS in the 40 SPECT/CTs. Twelve were in the head, 5 in the neck, 11 in the chest, 3 in the abdomen, and 18 in the pelvis. Several WBSs had more than 1 cryptic area. In addition, there were artifacts on the WBS due to radioactive saliva or urine that were easily identified without SPECT/CT. Two of these did require SPECT/CT examination to identify that their location was on the surface of the skin or hair.
Struma ovarii: Histologically benign-looking struma ovarii with seeding of abdominal wall with histologically benign-looking multiple thyroid nodules.
Rx, therapy; IUD, intrauterine device.
Among the 49 cryptic foci, 39 (80%) were attributable by SPECT/CT as not thyroid cancer because their I-131 activity fused to visually identifiable normal anatomic sites and/or physiologic functions. More objective, independent correlation was not possible. The remaining 10 foci of radioactivity are listed in Table 1 and the Appendix as thyroid tissue, including thyroglossal or thyroid bed, lymphadenopathy, substernal ectopic thyroid tissue, thyroid cancer metastases to bone, or struma ovarii. There were 32 patients in whom the SPECT/CT provided useful clinical information. In 8 of the 32 patients, treatment with I-131 had been considered based on the planar WBS, but the therapy was not administered because of the result of a SPECT/CT. In 24 of the 32 patients, I-131 ablation or treatment had been ordered by the clinician and administered because there were functioning remnants, metastatic disease, or Tg elevation. In them, a planar WBS seven or more days after the therapy revealed that the cryptic site was not thyroid cancer.
TSH-stimulated Tg levels (secured by either withdrawal of suppressive therapy or rTSH administration) were available in 34 patients who had CF on WBS and had SPECT/CT. Seven were associated with elevated anti-Tg antibody titers and were therefore excluded from further analysis. Among the remaining 27, Tg was elevated in 11 patients, all of whom had additional abnormal I-131 foci on the planar WBS that were highly suggestive of metastatic disease. The SPECT/CT revealed that the cryptic focus in one patient was a thyroid metastasis to a lymph node (#2, Appendix) and a substernal thyroid deposit in the other (#14, Appendix). In the remaining patients the cryptic foci were not related to the presence of thyroid tissue as judged by analyzing and correlating the anatomic information derived from the CT and the I-131 localization on the SPECT images. Tg was not elevated in 16 patients who had CF on planar WBS. In 15 the SPECT/CT revealed nonthyroid localization, and in 1 patient there was focal uptake of I-131 in the right maxilla that we strongly suspect as a thyroid metastasis because the WBS demonstrated liver activity and was otherwise not suspicious except for the maxillary focus (#1, Appendix). Figures 2 –5 demonstrate situations in which equivocal planar WBS scan findings were determined to be benign on SPECT/CT.
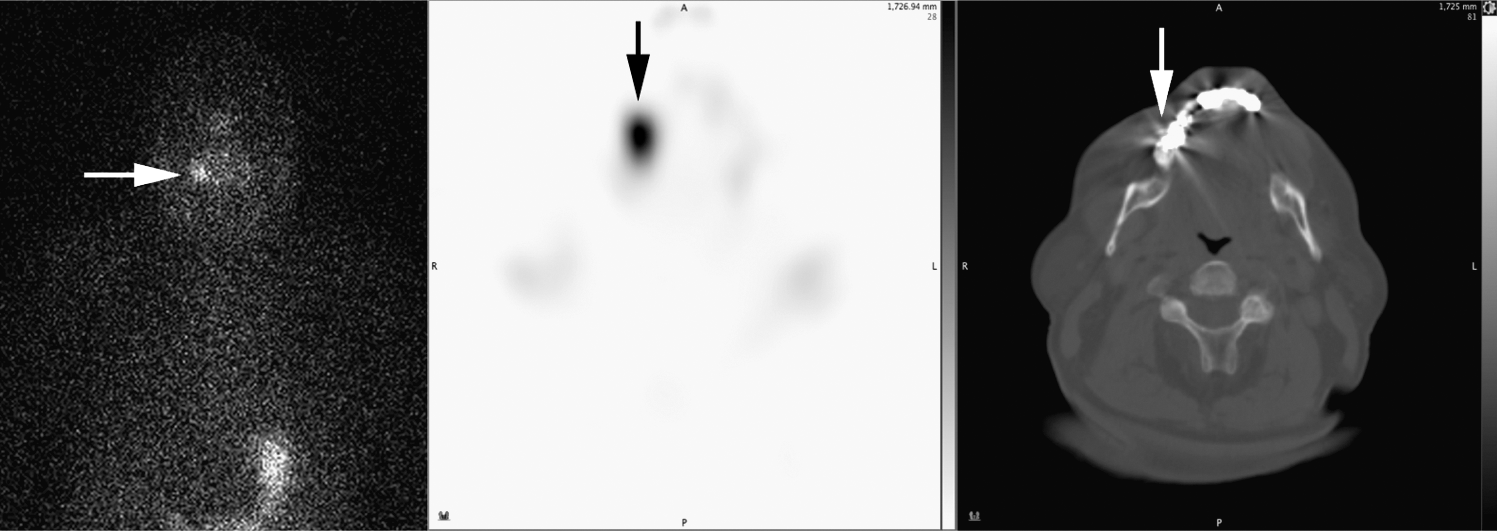
Seventy-year-old man (Patient #18) with a history of papillary thyroid cancer treated with surgery and ablation. The patient presented with a serum Tg of 70 ng/mL. Pretreatment WBS was negative and the patient received 200 mCi I-131 as empiric therapy. Post-treatment planar WBS demonstrated equivocal right facial activity (horizontal arrow) that on SPECT/CT (vertical arrows) was noted to correspond to a site of dental inflammation. SPECT, single-photon emission computed tomography; CT, computed tomography; Tg, thyroglobulin.
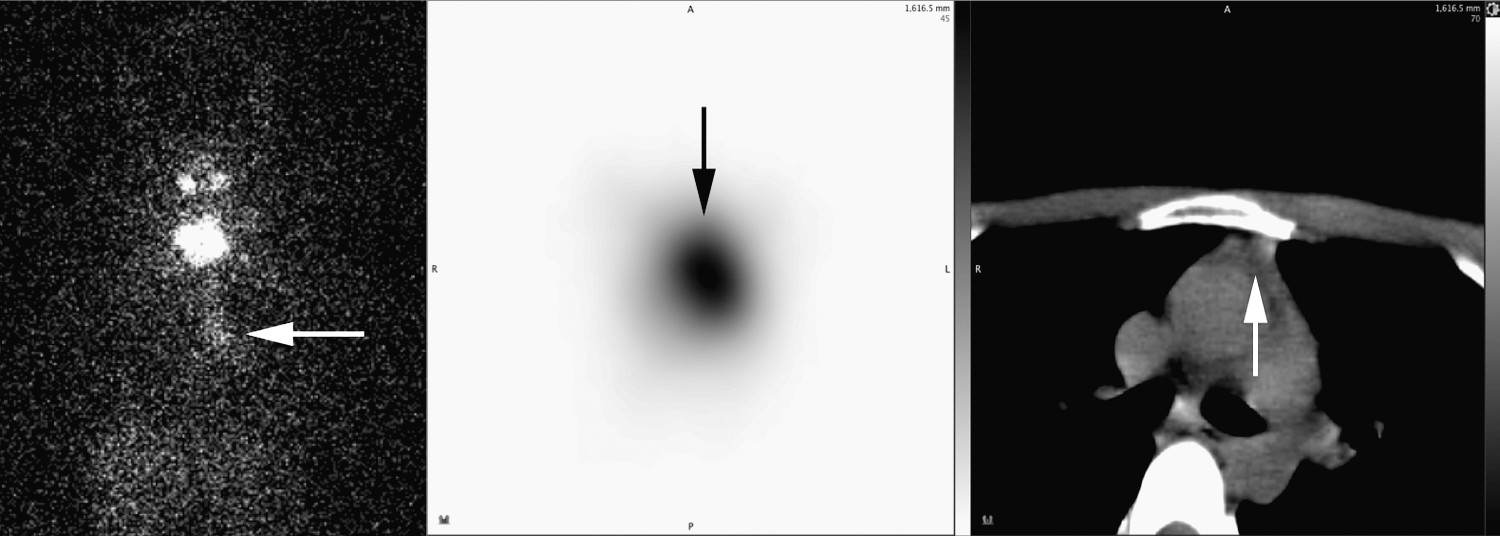
Thirty-three-year-old woman (Patient #38) with a history of papillary thyroid cancer treated with surgery and then ablation with 50 mCi of I-131. The patient presented with a serum Tg level of 0.1 ng/mL and was anti-Tg antibody positive. A follow-up withdrawal WBS demonstrated residual activity in the thyroid bed and the patient received an additional 100 mCi of I-131. Post-treatment planar imaging demonstrated equivocal chest activity (horizontal arrow) that on SPECT/CT (vertical arrows) was confirmed to represent normal thymus tissue.
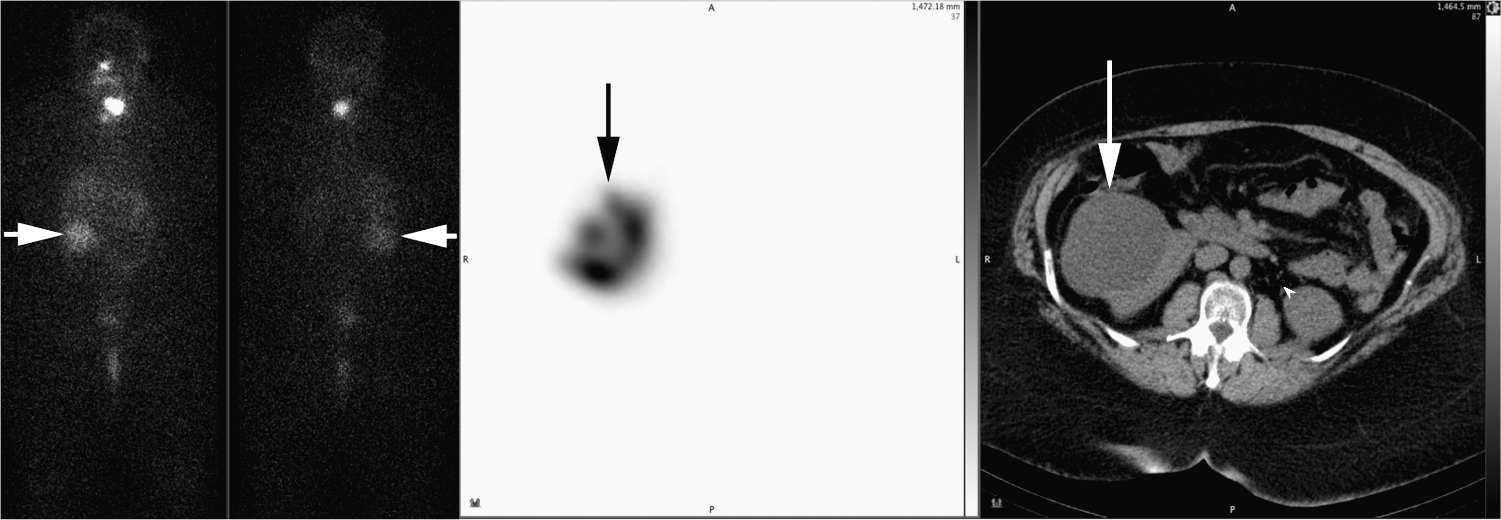
Sixty-three-year-old woman (Patient #10) with a history of papillary thyroid cancer treated with surgery and then ablation with 100 mCi of I-131. Post-treatment WBS demonstrates equivocal right upper quadrant activity (horizontal arrows) that on SPECT/CT (vertical arrows) was confirmed to represent I-131 accumulation within a benign renal cyst.
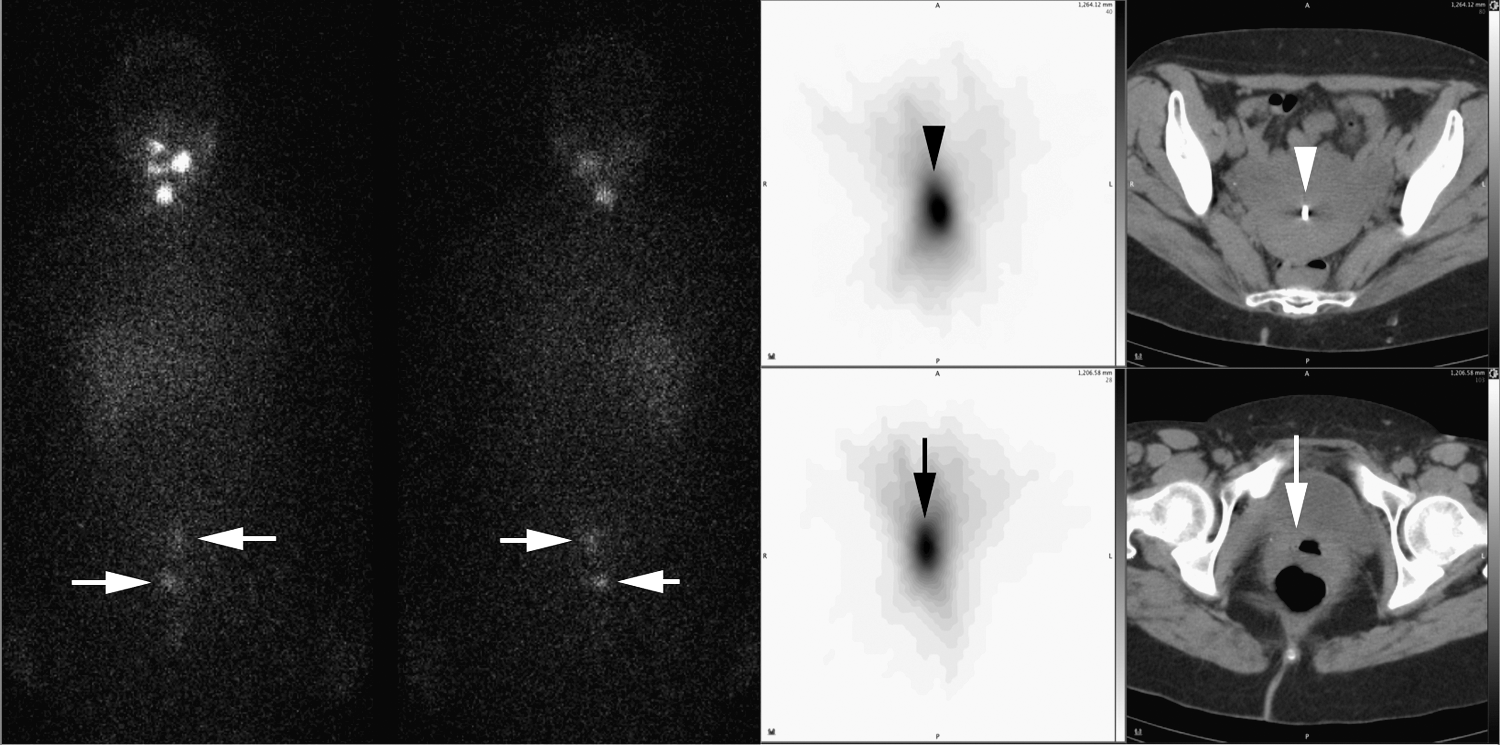
Forty-one-year-old woman (Patient #24) with a history of papillary thyroid cancer treated with surgery and then treatment with 150 mCi of I-131. Post-treatment WBS demonstrates two equivocal foci in the pelvis (horizontal arrows) that on SPECT/CT was confirmed to represent accumulation of I-131 in the uterine cavity associated with an intrauterine device (vertical arrowheads) and at the cervix (vertical arrows).
Discussion
A WBS is an essential component of the postoperative diagnosis of patients with well-differentiated thyroid cancer, periodic assessment for cancer recurrence, and selection for treatment with I-131. Nevertheless, it is controversial if a WBS is needed before an ablative dose of I-131 is administered because a planar scan 7 days after treatment is more sensitive and it avoids the risk of preablation stunning (15 –17).
We performed WBS in patients with thyroid cancer who had as near a total thyroidectomy as is surgically possible. The patients were prescribed and complied with a low iodine diet, and the serum TSH was appropriately elevated to permit stimulation of the iodine symporter and the metabolic steps that lead to T4 production by responsive thyroid tissue. Sensitive, state-of-the-art equipment was employed and the images that were acquired were technically excellent. The readers were highly practiced nuclear imaging specialists (one of whom is also an endocrinologist) who correlated the images with anatomic landmarks, possessed a detailed understanding of thyroid metabolism and extrathyroid iodine concentrating sites, and had many years of experience with these scans (18 –28). The planar WBS were usually interpreted directly and further analysis was not required. However, even when all of the requirements had been met, there were scans in which interpretation was speculative because of CF that generated uncertainty as to whether they represented nontumor activity or thyroid cancer. As a result, tumor stage and the need for treatment with I-131 were in doubt.
We have presented our experience with SPECT/CT scanning in thyroid cancer patients in whom the images were acquired because of cryptic observations on planar WBS. Our study explored the utility of SPECT/CT images to identify more accurately the location and nature of CF and the subsequent effect on the decision for or against I-131 therapy.
There are scattered reports and articles that suggest that image fusion technology may enhance proper interpretation of scan images in thyroid cancer patients (20,23 –25,29 –37). Further, there is emerging literature that demonstrates that SPECT/CT may reveal equivocal findings on planar WBS as thyroid cancer (8).
Planar WBS
Interpretation of I-131 tracer or post-therapy WBS was achieved in standard fashion in 144 of the 184 (78%) WBS. Of these 184 scans, 82 were tracer scans and 102 were done after therapeutic quantities of I-131 had been given. Additional elucidation of the location of the normal or pathologic foci was not deemed necessary in these patients by a consensus of experienced observers. When foci or regions of radioactivity did not achieve consensus interpretation, the problematic findings were called cryptic. In these patients SPECT/CT was performed to assess which of them was likely metastatic thyroid cancer.
I-131 SPECT/CT
I-131 SPECT/CT scans further defined the anatomic location and nature of the cryptic sites. There was no significant difference between the success of interpreting a tracer (2 mCi) or a post-therapy examination, a finding that is in agreement with preliminary reports describing the feasibility of I-131 SPECT/CT with low doses of I-131 ranging from 1 to 4 mCi (2,10). Of note, in our study a struma ovarii tumor was detected with a 1.5 mCi tracer dose. All SPECT/CT scans contributed to interpretation of the WBS and thus, to patient management. Examples where SPECT/CT improved identifying the location of the isotope include (A) I-131 in the blood pool on 48 hour pretreatment images consisting of inorganic I− derived from the original tracer administration; (B) organic I-131-labeled T4 in the circulation; (C) I-131 in the form of inorganic I− in the circulation on 1-week post-treatment images that is derived from the de-iodination of radio-labeled T4; (D) physiologic sites such as salivary glands, saliva, thymus, gall bladder, stool in recto-sigmoid colon, or bladder; (E) nonthyroid situations like dental disease, menstrual blood, uterine fibroids, kidney cyst, and struma ovarii; and (F) thyroid cancer.
Distribution and nature of CF
We have observed that SPECT/CT frequently resolved a diagnostic dilemma posed by CF on planar WBS, increased diagnostic specificity and accuracy, localized ambiguous activity, identified atypical physiologic activity, revealed nonthyroid pathology, and excluded or confirmed metastatic disease.
The cryptic activity in the head correlated with dental and/or periodontal disease in most patients (Fig. 1). Once we recognized the frequent occurrence and the significance of spotty bright oral areas as gingivitis or dental disease, the interpreters were more secure in not attributing such instances to possible thyroid pathology. With experience, the need to do SPECT/CT for focally prominent regions in the oral cavity reduced. However, cautious interpretation was warranted. In one patient who had a dental abscess there was also a probable thyroid cancer metastasis in the maxillary bone. We initially concluded that this activity in right maxilla as seen on SPECT/CT was probably thyroid cancer because she had a complete thyroidectomy for papillary thyroid cancer and had no thyroid bed remnant, the WBS showed no other focus of suspicious activity, and the WBS visualized the liver, which is highly likely indicative of T4 production by thyroid cancer somewhere, as discussed above. The dental focus was finally excluded as thyroid cancer because a biopsy of the tissue in the tooth socket after the abscess had been drained did not reveal thyroid tissue. In contrast, in one patient with dental pathology, Patient 3, the cryptic uptake in the projection of the left mandible was identified as contamination of the skin by saliva.
The cryptic activity in the neck was adenopathy in one patient and in others was related to the thyroid bed or thyroglossal duct.
In the chest, SPECT/CT identified cryptic activity as noncancer: I-131 in the blood pool, thymus, hiatus hernia, or cancer. In one patient there was a thyroid metastasis to an axillary lymph node in a patient who had prior resection of a rib due to thyroid cancer metastases.
Abdominal cryptic activity on planar WBS outside of the usual distribution of bowel or liver was suspected as thyroid cancer and I-131 therapy was considered until SPECT/CT demonstrated I-131 in a right renal cyst in one patient (Fig. 4), and physiologic blood-pool activity in another. Needless treatment with I-131 was avoided in both patients.
Eighteen of the 48 cryptic foci (37%) occurred in the pelvis and usually occurred in women. This preponderance in the pelvis is due to the complexity of compartments and chemical forms of I-131 in that region, especially in women. There is I− in urine and in the circulation and menstrual blood and T4 in stool within the bowel and T4 in metastases or rarely in struma ovarii. The relative frequency of menstrual bleeding in our series is attributable to selection bias. Women in the reproductive age group were instructed to schedule their WBS as soon as a menstrual period began to avoid the possibility of pregnancy. In these patients the planar WBS depicted cryptic activity in the anterior/posterior projection of the urinary bladder (after voiding) that was either better seen on the posterior than the anterior view of the pelvis (taken simultaneously) or extended outside of the expected confines of the bladder. SPECT/CT elucidated uterine uptake during menstruation in 5 patients (Fig. 4). We did not assess how often menstruation takes place without demonstrable uterine activity on SPECT/CT. One of the menstruating women had an intrauterine device (IUD) and a bright spot of isotope uptake fused to the image of the IUD on the CT (Fig. 5). A small bright focus within the body of the uterus was observed in 2 patients on SPECT/CT and that correlated with the presence of vascular fibroids. We did not investigate the frequency or sensitivity of detecting fibroids or their vascularity. In 2 patients focal activity was found in the adenexal regions on SPECT/CT. One of these had struma ovarii that was treated surgically and one a para-ovarian cyst that is under gynecologic observation. Finally, a pelvic focus that was better seen on the posterior image than the anterior on planar WBS was demonstrated on SPECT/CT in Patient #4 as a small sacroiliac metastasis from thyroid cancer (elevated stimulated Tg and lesion confirmed on a dedicated CT and other imaging). She was treated with I-131. WBS and SPECT/CT a year later showed no regional uptake and a nonelevated stimulated Tg level. We suggest that a GYN, especially menstrual history, is essential for proper interpretation of a WBS and may reduce the indication for a SPECT/CT.
Our observations also suggest that the serum Tg level may be an imperfect predictor of the significance of a cryptic focus on a WBS. SPECT/CT revealed that in two of 11 patients with elevated stimulated Tg, the cryptic foci were thyroid cancer. In contrast, in 1 of 16 patients without Tg elevation the cryptic focus was thyroid cancer.
We speculate that since our investigation with SPECT/CT has revealed that CF on a planar WBS are often attributable to dental disease, gingival inflammation, or menstruation, there will be fewer confusing findings and a less frequent need for additional testing or treatment with radioactive iodine.
Our observations impact on the selection of post-thyroidectomy thyroid cancer patients for treatment with I-131. I-131 generally is administered in either of two settings (8,18 –28,38). The first type of therapy is ablation of thyroid tissue that remains in the neck after a thyroidectomy has been performed. There is controversy regarding whether or not a preablation tracer WBS is required or if only a WBS a week after ablation is more appropriate because of greater sensitivity and avoidance of stunning (15 –17). The second type of therapy is treatment of metastatic thyroid cancer or local recurrence of disease. A WBS is done a week after a therapeutic dose of I-131 has been administered to see if the putative cancer focus from the tracer WBS accumulated the therapy dose and also to see if additional iodine-avid sites (cancers), that escaped detection by the tracer, are visualized by the therapy dose. Patients with foci of I-131 uptake on planar WBS images may be judged as suffering putative thyroid cancer and thus are eligible for I-131 therapy (38).
As discussed earlier, either a tracer or a post-therapy WBS may reveal a focus that is not easily or reliably explicable, in other words, cryptic and is or could be thyroid cancer. There are no data on how many patients with CF have been selected for a therapeutic dose of I-131 under the supposition that cancer cannot be excluded. Since I-131 therapy is not without risk, a subject recently reviewed (39), it would be well to avoid or reduce needless radiation exposure, which might be achievable by reducing CF, facilitated by SPECT/CT.
In our series, 32 of 49 cryptic foci were demonstrated by SPECT/CT not to represent thyroid cancer and did not or would not have required treatment with I-131 based on the results of a planar WBS alone. Eight of them were observed on tracer WBS and SPECT/CT and thus influenced therapy by avoiding a recommendation to the clinician for treatment with I-131. Twenty-four were in WBSs and SPECT/CTs that were done after ablation or therapy had been given and thus advice against I-131 administration in these patients was theoretical but supports the concept that SPECT/CT can reduce needless therapy.
CF were more often seen on post-therapy scans than on pretherapy scans, which we attribute to the differences the quantity of administered I-131. We doubt that this factor could have potentially affected management. As is current practice, many of our patients had a WBS 1 week after ablation without a prior WBS. We cannot predict precisely how often a negative preablation WBS would have influenced a clinician's therapeutic decision.
There were some limitations to our study. Random selection of patients and appropriate controls for SPECT/CT in all study patients who had a WBS were not done to avoid nonrequired, additional radiation exposure to the patients from the CT and added expense. These are acknowledged, unavoidable inadequacies of this investigation. Of note, quality control testing at our institution revealed that the CT portion of a SPECT/CT of the abdomen/pelvis results in a total effective dose of 4.9 mSv (40) (data not shown), which is roughly equivalent to double the amount of yearly exposure patients receive from background radiation. For comparison, the total body radiation dose from 2 mCi of I-131 is 14.4 mSv and for 100 mCi it is 720 mSv. Although not inconsequential, the dose imparted by CT is relatively little compared to the dose generated by the I-131 exposure. Clinicians need to balance the benefits of SPECT/CT against the potential risks of added radiation on a patient-by-patient basis, particularly in younger patients.
The main technical limitation is misalignment (misregistration) of the SPECT and CT images that may result in erroneous anatomical localization of radioiodine. To avoid this type of artifact, we have been attentive to standardization, quality control, constant awareness of the need to superimpose known physiological and anatomic features on both types of images, the potential for patient movement, and the effects of respiratory and bowel motion. A second technical issue is that SPECT may not demonstrate a focus that was observed on the planar images because the radioactivity may have become too low due to decay or excretion. This limitation was reduced for all CF identified in this study by mathematically multiplying the raw planar SPECT images by a factor of 2x–4x before reconstruction of the dataset. This technique generated sufficient count density such that iterative reconstruction techniques were able to function properly and identify the origin of cryptic foci. Without this multiplication step, many lesions would have remained invisible above the noise floor. Despite our success with this maneuver, increasingly broad application of I-131 SPECT/CT will probably not resolve every single cryptic focus.
Another consideration possibly impacting the accuracy of I-131 SPECT/CT is the level of circulating nonradioactive iodine in the patient before administration of I-131. We did not routinely measure 24-hour urinary excretion of iodine. Although some laboratories routinely perform this test, we (many others do as well) rely on a thorough history to exclude a likelihood of iodine contamination and employ medical judgment to decide when an actual urinary measurement is necessary. We prefer this protocol because of the difficulty inherent in the test and patient's resistance to collect a full specimen. We acknowledge the limitations posed by our decision.
Finally, the relatively small number of patients involved in this study limits our assessment of the potential impact on patient management in larger populations.
Our data suggest that SPECT/CT is able to resolve CF in the vast majority of patients undergoing planar WBS. However, as this technology gains more widespread use it is expected that SPECT/CT will not resolve every single CF in all patients. Other modalities to consider may include ultrasound, MRI, and CT depending on the anatomical location of the CF. Patients with elevated serum Tg levels and CF on WBS that are not resolved by SPECT/CT may benefit from FDG PET/CT scanning which has been demonstrated to be useful in this clinical scenario (41 –45). Further, I-124 PET/CT with its superior image quality compared to I-131 is a promising new methodology for detecting small, iodine-avid metastases with precise anatomical localization (46 –48). Although not currently available for widespread use in the United States, the relatively long half-life and excellent sensitivity of this tracer suggest a promising future for this agent as an adjunct or possibly a replacement for I-131 imaging.
In summary, our results demonstrate that I-131 SPECT/CT was needed in 22% of WBSs, provided important diagnostic information that was previously not available, and helped limit superfluous therapy with I-131 in patients with thyroid cancer. The suspect CF on a pretherapy planar WBS might have inappropriately triggered therapy with I-131 had the I-131 SPECT/CT not correctly identified it as not representing thyroid cancer. SPECT/CT is feasible with 2 mCi I-131 and also in the post-treatment setting. It can accurately characterize cryptic I-131 on planar WBS to confirm physiologic activity, identify metastatic disease, and identify nonthyroid pathology in all parts of the body. The noteworthy applications of SPECT/CT are several. In the head it correctly categorizes oral activity secondary to dental infection and gingivitis in distinction to salivary glands and saliva. It can corroborate an unusual metastasis to the head that may be obscured by adjacent physiologic activity. In the chest it correctly identifies physiologic blood pool activity, fibroglandular breast tissue uptake, thymus, lymphadenopathy, lung, or bone pathology. In the abdomen it can identify unusual renal or gastrointestinal pathology that may mimic a thyroid lesion. In the pelvis it is very helpful in distinguishing menstruation, uterine fibroid, other gynecologic lesions, physiologic urine in bladder, stool in the recto-sigmoid colon, and other nonthyroid, or thyroid pathology.
We anticipate that since our investigation with SPECT/CT has demonstrated the manifestations of dental, gingival, and menstrual foci on a planar WBS, there will be fewer confusing findings and less frequent need for additional testing.
Footnotes
Acknowledgments
We appreciate Dr. Elizabeth Sedlis' participation in this investigation while she was on elective in Endocrinology as a student at the NYU School of Medicine. The authors also recognize and appreciate the expert technical assistance rendered by Mrs. Evelyn Millan.
Disclosure Statement
The authors declare that no competing financial interests exist.
| Patient no. | ||||||
|---|---|---|---|---|---|---|
| Sex/age, type of Ca | Stim Tg (ng/mL) | Type of WBS | Cryptic finding on WBS | Clinical dilemma posed by WBS: what does WBS finding mean? | SPECT/CT result | Clinical decision based on SPECT/CT |
| #1 F/54, Pap | 0.2 Ab neg | Wdrl Post-Rx | Focal activity in the oral cavity and just above that on right side. | Physiol, met, or inflam in maxilla? WBS revealed no other abnormal site but the liver was imaged | Dental disease & lesion in right maxilla | No additional thyroid cancer; observe after I-131 Rx |
| #2 M/50, Pap | 26.6 Ab neg | Post-Rx | Is there a submandibular node? | Parotid activity alone or parotid+node? | Adenopathy | Observe after I-131 Rx |
| #3 M/57, Pap | <0.2 Ab neg | TGN tracer | Question of activity in upper mediastinum | Mediastinal disease? | No disease in mediastinum: blood pool |
|
| #4 F/77, Pap | 7.6 Ab neg | Wdrl tracer | Focal pelvic activity | Back pain; is there a sacral met? | Not done: Before SPECT/CT was available | Advised treatment with I-131 |
| #4A F/77, Pap | — | Post-Rx | Cryptic focal pelvic activity | Back pain. Is there a sacral met? | Small focus right ilium | Observe after I-131 Rx |
| #4B F/78, Pap | 1.1 Ab neg | TGN tracer | None 13 months after I-131 therapy | Is focus Right Ilium still present? | Small focus right ilium is no longer seen | Continue to observe; |
| #5 M/66, Pap | 0.3 Ab pos | TGN tracer | Location of cryptic foci in neck | Are post-operative foci residual tissue or mets? | Foci are in thyroid/thyroglossal region. | SPECT/CT did not help in clinical decision |
| #6 F/43, Pap | 5.1 Ab neg | Wdrl tracer | Focal left pelvic activity | Sacral met, bowel, or soft tissue met? | Uterine cavity; menstruating |
|
| #7 F/46, Pap | NA | Post-Rx | Focal pelvic activity | Sacral met, bowel, or soft tissue met? | Activity is in bowel | No additional thyroid cancer; observe after I-131 Rx; |
| #8 M/40, Pap | 1.0 Ab neg | TGN tracer | Activity in upper abdomen | Bowel or met? | Activity is in bowel |
|
| #9 F/28, Pap | NA | Post-Rx | Focal pelvic activity | Uterine, bladder, or met? | Uterine activity | No additional thyroid cancer; observe after I-131 Rx; |
| #10 F/63, Pap | 1.0 Ab neg | After ablation | Right upper quadrant abdomen | Liver met, kidney met, or bowel activity? | Right renal cyst | No additional thyroid cancer; observe after I-131 ablation; |
| #11 F/46, Pap | 0.2 Ab neg | Post-Rx | Pelvic activity | Pelvic met, sacral met, or uterine? | Uterine cavity; menstruating | No additional thyroid cancer; observe after I-131 Rx; |
| #12 M/58, Hurt | 385.2 Ab neg | Prior metastatic Ca Rxd I-131 |
Pelvic activity | Prior extensive metastases in neck and bones unusually large bladder or pelvis metastasis? | Treatment with I-131 management in progress; |
|
| 25.5 Ab neg | Wdrl tracer | Large neurogenic bladder | ||||
| #13 M/37, Pap | 0.8 Ab neg | After ablation | A. Ill defined conglomerate of activity in neck in thyroid region |
Physiologic vs. metastasis? | A. Thyroid bed activity |
No additional thyroid cancer; observe after I-131 ablation; |
| #14 M/45, Pap | 5.6 Ab neg | Wdrl tracer | Superior mediastinal activity | Nature of superior mediastinal activity? | Substernal ectopic thyroid tissue | Advised treatment with I-131 |
| #15 F/37, Hurt | 152.8 Ab neg | Post-Rx | Mediastinal activity | Nature of mediastinal activity? | Activity in cardiac blood pool | No additional thyroid cancer; Observe after I-131 Rx; |
| #16 F/40, Pap | <0.1 Ab pos | Wdrl WBS | Wdrl WBS showed pelvic activity, met not excluded; clinician ordered I-131 therapy | Not done: Before SPECT/CT was available | Treated with I-131 to ablate thyroid remnant and to try to destroy ectopic pelvic activity | |
| Post-Rx | Post-therapy WBS also showed suspicious pelvic activity | Not done: Before SPECT/CT was available | ||||
| #16A F/41, Pap | Wdrl tracer | 1 year after therapy there was again pelvic activity | Nature of pelvic activity? | Pelvic activity is left struma ovarii |
|
|
| #17 F/51, Pap | <0.2 Ab pos | After ablation | Spotty activity in mouth region | Nature of oral activity? | Oral activity is dental/gingivitis | No additional thyroid cancer; observe after I-131 ablation; |
| #18 M/70, Pap | 70.7 Ab neg | Post-Rx | Focal activity in right side of mouth region | Nature of oral activity? | Oral activity is dental | Has thyroglobulin pos & scan neg disease; no additional thyroid cancer; observe after I-131 Rx; |
| #19 F/47, Pap | <0.1 Ab neg | Post-Rx |
Suspicion of increased activity in chest | Nature of chest activity? | Nothing abnormal: blood pool | No additional thyroid cancer; observe after I-131 Rx; |
| #20 F/56, Pap | 78.8 Ab pos | After ablation | Suspicion of increased activity in chest | Nature of chest activity? | Nothing abnormal: blood pool | No additional thyroid cancer; observe after I-131 ablation; |
| #21 F/62, Pap | 4.3 Ab neg | After ablation | Right paramedian pelvic activity | Nature of pelvic activity? | Uterine | No additional thyroid cancer; observe after I-131 ablation; |
| #22 F/58, Pap | <0.2 Ab neg | Wdrl tracer | Right paramedian pelvic activity | Nature of pelvic activity? | Rectosigmoid |
|
| #23 F/43, After surg for struma ovarii, prob malig a | NA | Tracer | Focal pelvic activity | Nature of pelvic activity? | Foci anterior to bladder and lower mid-abdomen | Thyroidectomy followed by I-131 therapy, declined by patient |
| #24 F/41, Pap | <0.2 Ab pos | Post-Rx | Focal pelvic activity | Nature of pelvic activity? | Uterine cavity, menstruating; activity also fused with CT showing IUD in uterine cervix | No additional thyroid cancer; observe after I-131 Rx; |
| #25 M/39, Pap | 0.5 Ab neg | Post-Rx | Right upper quadrant abdomen focus | Nature of right upper quadrant abd focus? | Gall bladder | No additional thyroid cancer; observe after I-131 Rx; |
| #26 M/46, Pap | NA | Post-Rx | Confusing foci in anterior neck | Nature of foci in anterior neck? | Activity in thyroid bed | No additional thyroid cancer; observe after I-131 Rx; |
| #27 F/41, Pap | <0.1 Ab neg | TGN tracer | Confusing diffuse activity chest | Nature of diffuse activity chest? | Contamination of skin & activity in blood pool |
|
| #28 F/40, Pap | <0.1 Ab neg | TGN tracer | Focal pelvic activity | Nature of pelvic activity? | Rectum |
|
| #29 M/87, Pap | NA | After ablation | Focal activity in mouth region | Nature of focal activity in mouth region? | Dental/gingivitis | No additional thyroid cancer. Observe after I-131 ablation; |
| #30 F/83, Pap | <0.1 Ab neg | TGN tracer | Focal activity in lower thorax, left, paramedial | Nature of focal activity in lower thorax, left, paramedical? | Hiatus hernia |
|
| #31 M/53, Pap |
|
Post-Rx | Activity along left aspect of mandible | Nature of activity along left aspect of mandible? | Contamination of skin | No additional thyroid cancer. Observe after I-131 Rx; |
| #32 F/52, Follic | NA | Post-Rx | A. Focal activity in mouth region. |
A. Nature of focal activity in mouth region? |
A. Dental |
A. No additional thyroid cancer; observe after I-131 Rx; |
| #33 M/33, Pap | 0.2 Ab neg | Post-Rx | Activity right superior mediastinum | Nature of cryptic activity right superior mediastinum? | Nothing abnormal; blood pool | No additional thyroid cancer; observe after I-131 Rx; |
| #34 F/22, Pap | 5.0 Ab neg | After ablation | Activity superior mediastinum | Nature of cryptic activity superior mediastinum? | Nothing abnormal: blood pool | No additional thyroid cancer; observe after I-131 Rx; |
| #35 F/42, Pap | 0.2 Ab neg | After ablation | Focal pelvic activity | Nature of focal pelvic activity | Uterine, menstruating & right adenexal cyst | No additional thyroid cancer; observe after I-131 ablation; |
| #36 F/38, Pap | 7.2 Ab pos | After ablation | A. Focal activity in mouth region |
A. Nature of focal activity in mouth region? |
A. Dental |
No additional thyroid cancer; observe after I-131 ablation; |
| #37 F/67, Follic | <0.1 Ab neg | TGN tracer | Focal activity to right of midline above mouth | Nature of focal activity to right of midline above mouth? | Asymmetrical nasal activity |
|
| #38 F/33, Pap | 0.1 Ab pos | After ablation | Activity in mediastinum | Nature of focal activity in mediastinum? | Thymus | No additional thyroid cancer; Observe after I-131 ablation; |
Note: Decision for ablation or therapy was made by clinician before result of SPECT/CT was available.
Struma ovarii: Histologically benign-looking struma ovarii with seeding of abdominal wall with histologically benign-looking multiple thyroid nodules.
CT, computed tomography; SPECT, single-photon emission computed tomography; Pap, papillary; Hurt, Hurthle cell thyroid cancer; follic, follicular thyroid cancer; FPap, follicular varient of papillary thyroid cancer; Wdrl, withdrawal preparation; TGN, thyrogen preparation; post-Rx, scan after therapy; tracer, diagnostic or tracer scan; Physiol, physiologic activity; met, metastasis; inflam, inflammation; act, activity; Ab neg, antithyroglobulin antibody is negative; Ab pos, antithyroglobulin antibody is positive; IUD, intrauterine device; NA, not available.