
Abstract
Background:
Thyroid nodules are relatively common (7% of the population) but are malignant in only 5%–10% of cases. Fine-needle aspiration (FNA) to detect cancer can have >90% sensitivity but only 50%–65% specificity because of false-positive results, which necessitates surgical controls. We aimed to assess the diagnostic accuracy of immunocytochemistry (ICC) of thyroid FNA to improve its sensitivity and specificity.
Methods:
We prospectively collected 2038 thyroid FNAs, of which 1397 were FNA biopsies with liquid-based cytology (Thin-Prep-Hologic®). ICC with cytokeratin 19 and HBME1 antibodies (Dako®A/S) was used for all malignant cases and cases of atypical cells of undetermined significance (AUS), follicular neoplasm (FN), and nodules suspicious for malignancy-papillary thyroid carcinoma (SM-PTC) as well as some benign cases (abnormal features on radiography or benign on secondary FNA). ICC results were defined as “non-contributory,” “favoring benign,” “favoring malignant,” or “indeterminate.” Results for 150 cases were compared with histological controls for diagnostic accuracy.
Results:
Of these 150 cases ICC was helpful for benign or malignant triage of 48 cases of AUS, FN, and SM-PTC (42% of these lesions). Six (4%) ICC results were false positive (favoring malignant with benign histology) but none were false negative (favoring benign with malignant histology). Results for indeterminate cytological cases favored malignant or benign disease with sensitivity, specificity, and negative and positive predictive values of 100%, 85.2%, 100%, and 86.2%, respectively.
Conclusions:
ICC of thyroid FNAs with cytokeratin 19 and HBME1 antibodies can reduce the false-positive and false-negative results of single morphological analyses. It can increase the sensitivity and specificity of diagnosis, thus improving diagnostic accuracy and reducing the need for surgical controls.
Introduction
Nevertheless, thyroid FNA has low specificity—usually 50%–65%—which leads to many unnecessary surgical procedures. Only 20%–30% of all “indeterminate cases” were found malignant on histology, with again high variability in assessment of risk of malignancy, from 6.8% and 44%, depending on the terminology used (12,13).
This situation leads to another issue concerning the terminology cytopathologists use in reports of thyroid FNA. Until recently, no well-accepted international terminology existed, with no standards for describing thyroid FNA specimens (14). Several published classification schemes were based on personal or institutional experiences or were proposed by scientific groups, including the Papanicolaou Society (15), the American Thyroid Association (16,17), the American Association of Clinical Endocrinologists (18,19), and the British Thyroid Association (20). Various terms have been used in these five- to eight-tiered classifications. Therefore, comparing the results of the published series and obtaining results for homogeneous categories of lesions, as well as determining well-defined clinical management for categories, are difficult. The National Cancer Institute State of the Science conference on thyroid FNA (Bethesda, October 2007) led to the Bethesda Terminology (21), published in 2009 (22), a common terminology based on well-described cytological criteria that are related to a risk percentage of cancer and accompanied by management recommendations. Now the “indeterminate cases” are shared among three categories: (i) follicular lesions of undetermined significance or atypia of undetermined significance (AUS), (ii) FNs and FNs/Hürthle-cell type (Hürthle-cell neoplasms), and (iii) SM (specify lesion). The associated risk of cancer is 5%–15%, 15%–30%, and 60%–75%, respectively, and a standardized follow-up is proposed.
Nevertheless, how to detect malignant cases in these three categories has not been yet determined. Most of the nodules of the three “indeterminate categories” (AUS, FNs, and SM) would be found benign by systematic surgical controls. Therefore, additional diagnostic criteria are needed to increase the accuracy of thyroid FNA. However, the National Cancer Institute conference session on ancillary techniques produced no recommendations for these cases (23). Potential problems were the few data available for immunohistochemistry (IHC) in large cohort studies and the variable methods used to obtain cytological specimens (i.e., liquid medium, air-dried smears) and for immunocytochemistry (ICC). Conclusions from the conference were “that IHC/ICC may be considered for some suspected malignancy and for some specific diagnoses (e.g., thyroid nodule versus parathyroid nodule), but that there was insufficient evidence for a specific recommendation for the indeterminate/suspicious FNAs.” Moreover, most of the articles describing ICC of cytological material described use of a single antibody (24 –28); even a panel of antibodies has been recommended, because “individual thyroid tumors may not express some markers” (29).
Therefore, we aimed to perform a prospective study of ICC based on the Bethesda terminology using several antibodies with available histological control to assess the accuracy of ICC with thyroid FNA in indeterminate cases.
Materials and Methods
We collected information on 2038 thyroid FNAs performed from May 2007 to June 2010 in our department, of which 1397 were FNA biopsies with liquid-based cytology (LBC) (Thin-Prep-Hologic®). For case reports from September 2008 onward, the Bethesda terminology was used; those from 2007 to September 2008 were transcribed from the previous institutional terminology (five-tiered classification) to the Bethesda terminology. All malignant cases, as well as all cases of AUS, FN, and SM-papillary thyroid carcinoma (SM-PTC) found on LBC underwent ICC, as did some cases of benign lesions (nodules with abnormal radiological features—recent or rapid increase in size, microcalcifications, central vascularization—or benign lesions on secondary FNA after a previous AUS). For 150 cases, results of ICC with two antibodies combined, cytokeratin 19 (CK19, Novocastra® distributed as Menarini®; dilution 1:100) and HBME1 (Dako® A/S, dilution 1:50), were compared with histological controls. For LBC, one superfrost slide was prepared for each case following the guidelines of the manufacturer and analyzed after Papanicolaou staining. For ICC, two additional slides were prepared the same day or the day before ICC and then preserved at 4°C. An automated technique was used (Ventana BMK®). Detection was by use of avidin–biotin complex with diaminobenzidine (DAB) chromogen, without epitope retrieval. Positive control was represented by typical papillary carcinoma and negative control by histiocytes and lymphocytes present in most of the thyroid nodules.
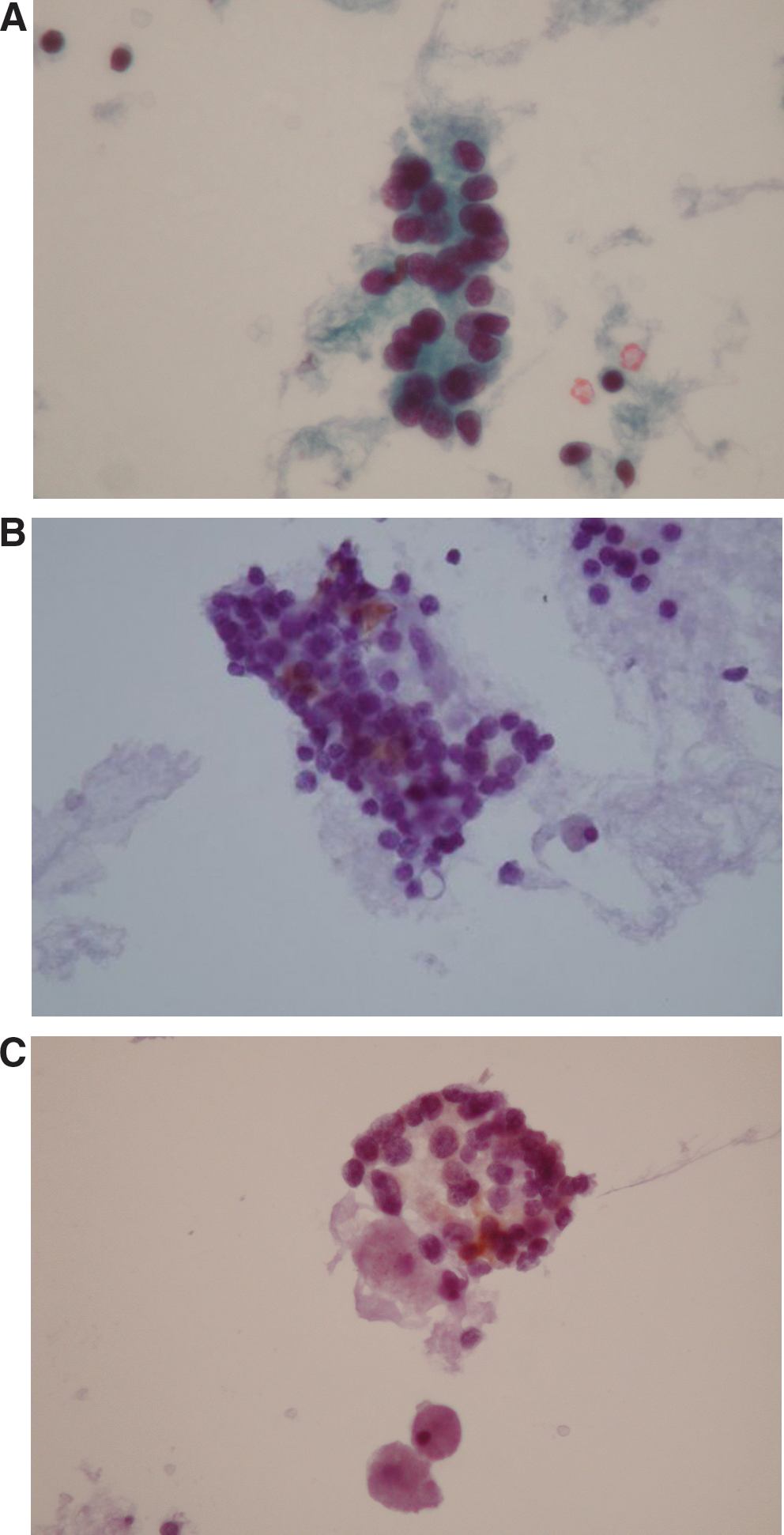
ICC results were divided into four categories: (i) noncontributory (<5 remaining sheets of follicular cells), (ii) favoring benign (<30% positive cells for both antibodies) (Fig. 1), (iii) favoring malignant (>70% positive cells for both antibodies) (Fig. 2), and (iv) indeterminate (30%–70% positive cells for both antibodies or results for both antibodies not falling into the previous categories).

All these technical criteria had been previously tested and validated on FNA samples of surgically removed thyroid nodules. ICC results from the cytological material were compared with IHC results from histological specimens to assess reproducibility. The four ICC category cutoffs were established with available histological diagnoses (unpublished series of 50 cases). CK19 and HBME1 were chosen because of their technical reproducibility. A panel of three antibodies would have been a more satisfying option but routinely obtaining three additional slides in a thyroid FNA is not totally realistic, especially for this “AUS category,” including some nodules for which this diagnosis is proposed because of few cellular abnormalities and often not enough cellular material. Two additional slides are mainly obtained. We therefore have very few noncontributory cases.
SM for medullary carcinoma, lymphoma, metastases and Hürthle-cell neoplasms were excluded from this study, the former because antibodies other than those studied in this report were used for diagnosis (e.g., calcitonin, CEA, CD45, CK7, CK20), the latter because no immunohistochemical profile could be found in our validation study or in the literature to distinguish benign and malignant cases.
Results
ICC was performed for 350 of 1397 FNABs/LBC: 26 samples (1.8%) showed malignant nodules, 93 (6.7%) SM-PTC, 38 (2.7%) FNs, 114 (8.2%) AUS, and 79 (5.7%) benign lesions (nodules with abnormal features on radiography or with secondary FNA) (Table 1).
NC, noncontributory; AUS, atypical cells of undetermined significance; FN, follicular neoplasm; SM-PTC, suspicious malignant-papillary thyroid carcinoma.
In total, surgery was performed for 150 patients. For 25 cytologically malignant nodules found malignant on histology, ICC was malignant for 15 (62.5%) and was indeterminate for 10; 23 cases of AUS, FN, and SM-PTC were benign on histology and ICC; 25 cases of AUS, FN, and SM-PTC were malignant on ICC and histology; 4 cases of AUS (1), FN (2), and SM (1) were benign on histology and malignant on ICC; 3 benign nodules were malignant on ICC; 2 were found benign on histology and the third malignant; 5 nodules were benign on ICC and histology. For 56 cases of benign, AUS, FN, and SM-PCT (38%), ICC results were indeterminate; 33 cases were benign and 23 malignant on histology; for 9 cases (6%), ICC results were noncontributory (Table 2). Four of them were malignant on histology.
ICC was helpful for benign or malignant triage of 48 cases of AUS, FN, and SM-PTC (42% of these types of lesions). We found six (4%) false-positive ICC results (favoring malignant on ICC with benign histology results) but no false-negative ICC results (none favoring benign with malignant histology results). Therefore, concerning the “indeterminate lesions” (i.e., cases of AUS, FN, and SM-PTC), the sensitivity, specificity, and negative and positive predictive values were 100%, 85.2%, 100%, and 86.2%, respectively, for ICC favoring malignant and benign. The results were similar if we included all cases examined by ICC (i.e., benign and malignant cases): 100%, 82.3%, 100%, and 87.2%. The number of cases of indeterminate ICC results is substantial (38%) and concerns all categories. This finding underlines the so-called “grey zone” of abnormal thyroid nodules.
Discussion
Thyroid FNA is often considered a screening test (11). Therefore, its sensitivity is usually higher than 90% but its specificity is low—50%–65%—which leads to numerous unnecessary surgical procedures. Even recent studies have not produced more accurate results (30,31), especially in terms of specificity. So, the best diagnostic endpoint seems to be with morphology alone. In a previous personal study published in 2003 concerning 80 cases of thyroid FNAs performed on LBC (Thin-Prep-Hologic), with a systematic histological control as well, specificity and sensitivity were 60% and 81%, respectively (32). In this series, ICC with the combination of two antibody markers showed 100% negative predictive value, which increased the FNA accuracy for cancer detection, and the 85% specificity reduced the number of false-positive cases.
Histology is the “gold standard” diagnostic test. However, benign and malignant tumors, especially follicular lesions, can show morphologic similarities on routine hematoxylin and eosin–stained slides, which results in poor interobserver reproducibility (11,33). Thus, some authors studied the expression of several proteins to improve diagnoses. Most of them, with quite large series, recommended a panel of antibodies combined, “because individual thyroid tumors may not express some markers” (29). Several immunohistochemical markers used together may be helpful in the diagnosis of follicular-derived lesions of the thyroid. CK19, HBME1, galectin-3, and fibronectin-1 are the antibodies most often studied (34 –37), but they are not exclusive.
Because IHC can improve diagnostic accuracy in difficult histological cases, ICC could also be helpful in indeterminate cytological cases. The new technologies have the advantages of optimal cell preservation and available residual material and thus the opportunity to apply some ancillary techniques such as ICC. ICC is easily performed on cell-block preparations, because the reactivity does not differ from that with histology and IHC, but the technique also seems to be controversial, essentially because of the low cellularity of the specimens (38,39). A liquid medium may be used after validated protocols, because the reactivity of the antibodies may differ (40,41). We aimed to improve the diagnostic accuracy of thyroid FNA and especially increase the specificity of our previous published results with conventional techniques and LBC (32,42).
Because we had already used the liquid medium technique in our department, we chose ICC with LBC and validated the technique.
Few published series have described the use of ICC with multiple antibodies for thyroid FNA. A study of 49 cases with histological control and three antibodies (RET-oncogen, galectin-3, HBME1) on LBC material showed encouraging results, with 100% sensitivity and 76.4% specificity (43). Another series of 20 FNAs performed on cell blocks with histological control showed 100% specificity and sensitivity with the same antibodies we used (CK19, HBME1) (44). A third, recently published series of 44 thyroid papillary carcinomas examined on ThinPrep® material (45) involved four antibodies with high expression: 92.7%, 89.1%, 78.3%, and 86.7% for CK19, galectin-3, HBME1, and CD44, respectively. Our results for 150 controlled cases agree with these findings.
For ICC, cutoff values vary among series (43 –45). We chose the cutoff levels of 30% and 70% to avoid risk of overlap and therefore no reproducibility for the categories “favoring benign” or “favoring malignant” between the different cytopathologists responsible for the diagnoses. We chose a low level of 30%, because many benign follicular nodules or adenomas show some positive cells with the two markers we used on histology and because a lower level could induce more false-positive results. We chose a high level of 70%, because such a high number of positive cells with the two antibodies combined is largely observed in cases of malignancy. A high number of positive cells for only one antibody, especially with CK19, may be observed in benign lesions such as lymphocytic thyroiditis and therefore was not taken into account (33).
Detection of molecular markers such as BRAF mutation or RET/PTC rearrangements could be a further option, because the V600E BRAF mutation and the RET oncogen seem to be highly specific for papillary carcinomas. Nevertheless, although papillary carcinomas represent the most frequent thyroid carcinoma, difficult diagnoses more often occur for other carcinomas or malignant tumors, especially follicular carcinoma. Further, although these markers are specific, they are less sensitive, and the processing protocols usually are not available in routine practice (46 –49). ICC with a panel of two antibodies considered as markers of malignancy in general and not a specific type of cancer seems to be more relevant for clinical practice.
Conclusions
The high negative predictive value of ICC used with thyroid FNA could be a strong argument for its use in cases of AUS and FN and perhaps SM-PTC nodules to avoid unnecessary surgery and to suggest clinical and radiologic follow-up. Further analyses are required, but considering these preliminary results, ICC of thyroid FNAs could be recommended as a diagnostic aid and could lead to follow-up and more suitable therapeutic decisions for cases of the three Bethesda categories when the benign or malignant characterization is not confirmed on cytology alone.
Footnotes
Acknowledgments
The authors thank Beatrice Peraton and Isabelle Lévêque for their great technical contributions.
Disclosure Statement
The authors declare that no conflicts of interest and no commercial or financial interests exist.