
Abstract
Background:
Positron emission tomography/computed tomography (PET/CT) scan has a role in the surveillance of patients with a history of thyroid carcinoma. Its efficacy after remnant ablation as far as detecting persistent or recurrent thyroid carcinoma before other surveillance methods is not known, however. In intermediate-to-high risk thyroid carcinoma patients we studied whether PET/CT scan, performed 6–12 months after the first remnant ablation, could provide more information than ultrasonography (US) and thyrotropin-stimulated serum thyroglobulin (Tg) determination with diagnostic whole-body scan (DxWBS).
Methods:
We studied 71 subjects with differentiated thyroid cancer (DTC) who were intermediate-to-high risk for persistent/recurrent disease and who had received PET/CT scan, US, and DxWBS simultaneously with stimulated Tg levels 6–12 months after remnant ablation. To evaluate the diagnostic efficacy of PET/CT scan, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy were calculated.
Results:
Ten subjects (14%) had persistent/recurrent disease detected 6–12 months after remnant ablation. Persistence/recurrence was detected in nine (12.7%) of these patients by conventional methods, including US and DxWBS, along with stimulated Tg levels. The remaining case was detected solely by a PET/CT scan, which showed a mediastinal prevascular lesion; this was confirmed by a therapeutic WBS after additional radioiodine therapy. Among the six patients whose PET/CT scan showed positive results, five had persistent/recurrent disease. The sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of PET/CT scan for detecting persistent/recurrent thyroid carcinoma were 50%, 98.4%, 83.3%, 92.3%, and 91.5%, respectively.
Conclusion:
In intermediate-to-high risk patients with DTC seen 6–12 months after their first remnant ablation, there is almost no complementary role for adding a PET/CT scan to conventional follow-up methods, an US and a DxWBS simultaneously with stimulated Tg levels.
Introduction
[18F]-fluorodeoxy-D-glucose ([18F]-FDG) positron emission tomography and computed tomography (PET/CT) scan, which relies on an abnormal glucose metabolism of malignant cells, is widely used in both diagnosis and surveillance of many types of tumors. In several cancers, it has also provided prognostic information (9 –11). As for DTC, when patients who have undergone a total thyroidectomy and remnant ablation have a negative 131I WBS with detectable Tg levels during their surveillance, a PET/CT scan has an important role in localizing the disease (12,13). The role of PET/CT scan has expanded to initial staging, a prognostic tool, and an evaluation of the post-treatment responses in a subset of patients with aggressive thyroid cancer (8).
Little is known as to whether a PET/CT scan along with US and diagnostic WBS (DxWBS) could contribute to the early detection of persistent/recurrence disease occurring 6–12 months after RAI ablation. Whether there are additional advantages of PET/CT scan over US, DxWBS, or TSH-stimulated Tg during the initial follow-up is also unclear.
The aim of this study was to investigate, in DTC patients who are at intermediate-to-high risk for recurrence, whether a PET/CT scan, performed 6–12 months (the first follow-up) after remnant ablation, could provide additional information to compliment the conventional methods of US and TSH-stimulated Tg with DxWBS.
Materials and Methods
Patients
Among the 581 subjects who received PET/CT scan for DTC between January 2006 and October 2010 we excluded, 411 patients who had a PET/CT scan more than 1 year after the first remnant ablation, an additional 64 patients who had an interval of more than 1 month between their US, WBS, and PET/CT scans, and a further 9 patients who had surgery or PET/CT scan in another institution. In addition we excluded 26 patients with low-risk of persistent/recurrent disease. Based on recent ATA guidelines (8), low-risk patients were defined as those patients with no local or distant metastases, complete resection of all macroscopic tumor, no tumor invasion of locoregional tissues or structures, and lack of aggressive histology or vascular invasion. In addition, they were low risk if after RAI there was no 131I uptake outside the thyroid bed on the first posttreatment whole-body RAI scan. This left 71 patients with intermediate-to-high risk for recurrence, all of whom had high dose (3700 MBq [100 mCi] or 5550 MBq [150 mCi]) RAI ablation, in the study.
Methods
DxWBS and Tg measurement
DxWBS 6–12 months after remnant ablation was performed according to our institutional protocols, which consist of withdrawal of thyroid hormone (thyroxine [T4]), replacement of triiodothyronine for 2 weeks, and low iodine diet for at least 2 weeks before the studies (14). Seven patients had recombinant human TSH (rhTSH) stimulation for WBS instead of T4 withdrawal. The DxWBS results were interpreted visually by agreement between two experienced nuclear medicine physicians.
Serum Tg levels were measured by an immunoradiometric assay (IRMA) kit (CIS Bio International, Cedex, France); functional sensitivity was 0.7 ng/mL. Levels of serum TSH were measured by an IRMA kit (Beckman Coulter, Prague, Czeh Republic) with a detection limit of 0.025 mIU/L.
[18F]-FDG PET/CT scan
All patients fasted for at least 6 hours before the PET/CT study. [18F]-FDG was injected intravenously (3700–5550 MBq) and scanning began 60 minutes later. None of the patients had blood glucose levels >130 mg dL–1 before the injection. No intravenous contrast agent was administered. Studies were acquired on three combined PET/CT inline systems, Biograph Duo or Biograph Truepoint (Siemens Medical Solutions, Knoxville, TN). The acquisition time was 2–3 minutes per bed position. All patients were in a supine position with their arms raised. The CT scan was begun at the orbitomeatal line and progressed to the upper thigh (130 kVp, 80 mA, and 5-mm slice thickness; 120 kVp, 80 mA, and 5-mm slice thickness; 120 kVp, 70–100 mA, and 5-mm slice thickness). PET scan was followed immediately over the same body region. The axial spatial resolution was 6.5 mm or 4.5 mm or 4.2 mm at the center of the field of view.
Determination of disease status
PET/CT scan findings were reviewed by two experienced nuclear medicine physicians. All PET/CT scan and US image findings were defined as negative or positive. If there were no FDG uptake lesions, or no identifiable lesions in CT scans, they were defined as negative in PET/CT scans. Diffuse or symmetric FDG uptake lesions with no identifiable lesions in CT scans were regarded as negative findings. Diffuse FDG uptake refers to FDG activity that is increased but does not have a clear-cut margin from the background FDG activity. In contrast, focal discrete FDG uptake with a lesion detected by matched CT scans was defined as positive. The US readings of lymph nodes were considered positive if there were findings suspicious of malignancy, such as cystic appearance, hyperechoic punctuations, loss of hilum, and peripheral vascularization (15). Otherwise, the USs were read as negative.
Clinically persistent or recurrent disease was defined as follows: (i) lesions confirmed by cytology or pathology, (ii) stimulated Tg levels >10 ng/mL regardless of imaging studies, or (iii) detectable stimulated Tg levels (>2 ng/mL) with any evidence of imaging studies suggesting malignant lesion. Criterion (ii) was only applied after adequate evaluation of multiple imaging modalities such as US, WBS, PET/CT scan, or chest CT. According to the ATA guidelines (8), patients of this category could be candidates for empirical RAI ablation therapy. In the context of change in the management of patients, we also defined the patient with Tg >10 ng/mL as being a persistent or recurrent case.
Data analyses
To evaluate the diagnostic efficacy of PET/CT scan, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy were calculated. We also analyzed the data of each patient with persistent or recurrent disease, focusing on the results of PET/CT scan, US findings, and DxWBS with stimulated Tg levels. The protocol of this study was approved by Institutional Review Board of Seoul St. Mary's Hospital, The Catholic University of Korea.
Results
Baseline characteristics of study subjects
The baseline characteristics of study subjects are shown in Table 1. Most patients in stage I disease were relatively young (<45 years of age). Among the three patients who had levels of anti-Tg antibody that were higher than upper normal values, one patient had a suspicious lesion revealed by PET/CT scan and US, which was confirmed to be persistent/recurrent by fine needle aspiration (FNA) cytology. Ten subjects of 71 (14.0%) had persistent/recurrent diseases detected 6–12 months after the first RAI ablation (Table 2). Four patients (cases 1, 3, 4, and 5) were confirmed by cytology or pathology, five patients (cases 2, 6, 7, 8, and 10) by evidence of DxWBS images along with increased Tg levels, and one patient (case 9) by elevated and rising Tg levels (18.12 ng/mL). In the latter patient, posttherapeutic WBS revealed suspicious uptake in the thyroid bed. Further treatment of these 10 patients with persistent/recurrent disease involved surgery (2 patients; cases 1 and 3), radiofrequency ablation (1 patient; case 5), and repeated RAI therapy (7 patients). Representative cases are shown in Figure 1 (case 5) and Figure 2 (case 10).
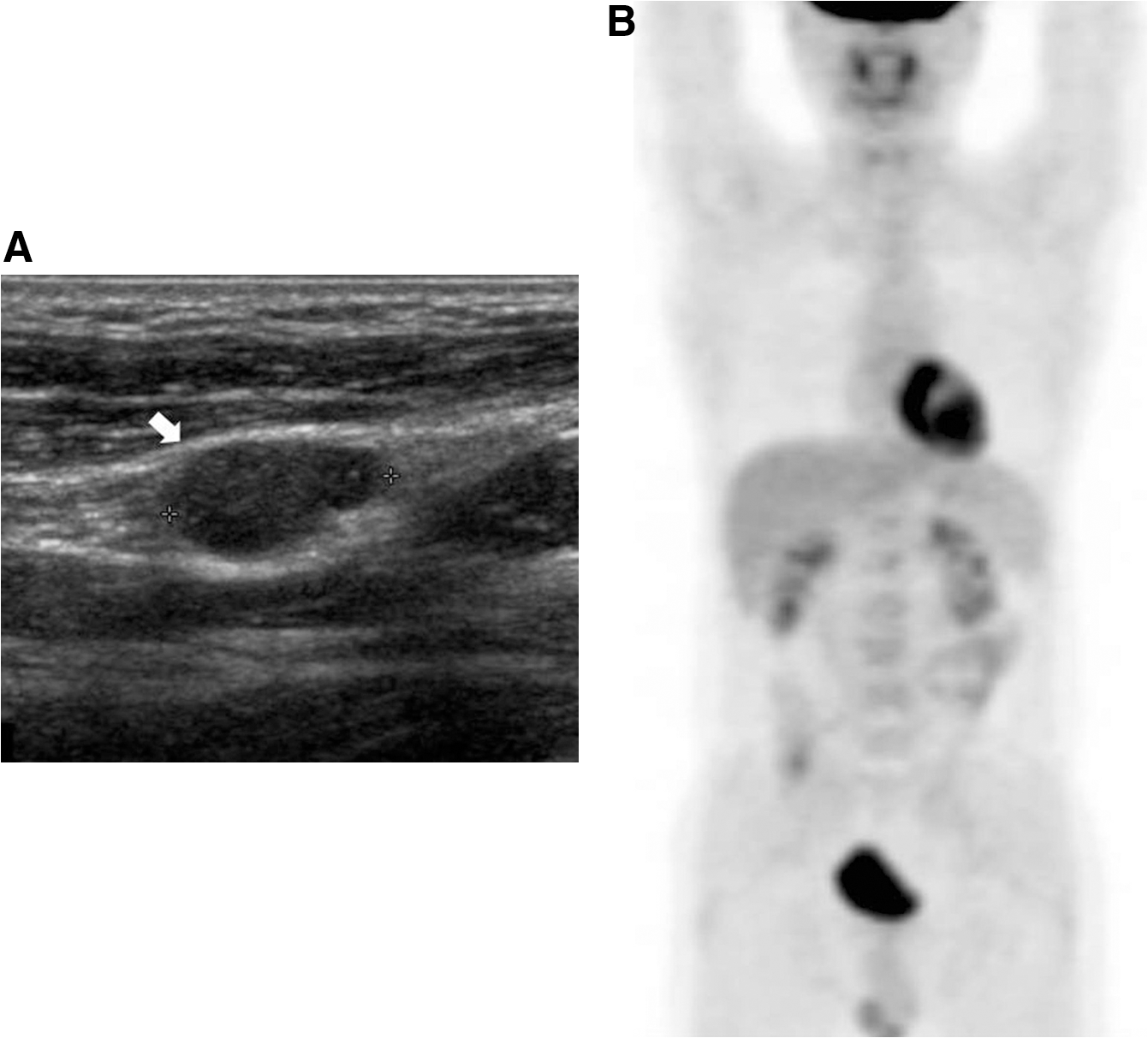
A persistent/recurrent case with negative result in the PET/CT scan (case 5).

A persistent/recurrent case with positive result only in the PET/CT scan (case 10).
AJCC stage based on sixth edition (2002).
TNM, Tumor, Node, Metastasis.
WBS, whole-body scan; T4, thyroxine; LN, lymph node metastasis; rhTSH, recombinant human TSH; AJCC, American Joint Commitee on Cancer.
The PET/CT scans were performed during the periods of T4 withdrawal.
The cutoff value of anti-Tg antibody positivity is 70 IU/mL.
PET/CT, positron emission tomography/computed tomography; Tg, thyroglobulin; F, female; M, male; P, positive; N, negative; Y, yes; N, no; N/A, not available.
Conventional methods at 6–12 months after the first RAI ablation
Nine of 10 patients (cases 1–9) had persistent/recurrent disease 6–12 months after the first RAI ablation as detected by conventional methods, including US and DxWBS, along with stimulated Tg levels (Table 2). One patient (case 10) was noted to have persistent/recurrent disease only by PET/CT scan criteria. Of the 71 subjects in the study, DxWBS revealed lesions suspicious for persistence/recurrence in 14 subjects (19.7%). Among them, the results for five patients (cases 2 and 5–8) met the criteria of persistent/recurrent disease. The remaining nine patients who were positive for DxWBS did not meet the criteria; their US and PET/CT scan results were negative. Positive readings in US were found in seven patients; four of these patients (cases 1, 3, 4, and 5) had persistent/recurrent disease proven by FNA cytology.
PET/CT scan at 6–12 months after the first RAI ablation
PET/CT scan was able to detect half of the 10 persistent/recurrent cases, most of which were also detected by conventional methods (Table 2). Sixty-four patients (90.1%) had PET/CT scan with TSH stimulation (either T4 withdrawal or rhTSH injection) and seven (9.9%) had this without TSH stimulation. Nine among 64 patients who had TSH-stimulated PET/CT scan had persistent/recurrent disease, and PET/CT scan was able to reveal the disease in 5 patients. Only one patient among seven patients who had PET/CT scan without TSH stimulation had persistent/recurrent disease; this was not detected by PET/CT scanning. PET/CT scans were performed before DxWBS in 56 cases (78.9%) and after DxWBS in 15 cases (21.1%). One of 56 patients who had a PET/CT scan before DxWBS and 5 of 15 patients after DxWBS had positive results for their PET/CT scans. Among six patients whose PET/CT scan was positive (Table 3), five had persistent/recurrent diseases. These patients received a PET/CT scan within a month after DxWBS. Four out of five cases with persistent/recurrent disease also had positive results in US or DxWBS with stimulated Tg levels, but only one patient (case 10; Fig. 2) had negative results by the conventional methods. The value of stimulated Tg in this patient was near 10 ng/mL (9.78 ng/mL), and an iodine uptake lesion was identified in posttherapeutic WBS after the second RAI therapy (5550 MBq [150 mCi]). One patient, who was defined as free from the disease despite positive results for the PET/CT scan (Table 3), had negative US findings, undetectable stimulated Tg levels (0.19 ng/mL), and no detectable anti-Tg antibody. PET/CT scans were negative in the other five patients with persistent/recurrent disease (Table 3). In these five patients, PET/CT scans were performed before DxWBS; two subjects were on TSH stimulation, with there being <1 week between the PET/CT scan and DxWBS. The sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of PET/CT scan for detecting recurrent/persistent thyroid carcinoma were 50%, 98.4%, 83.3%, 92.3%, and 91.5%, respectively.
Description of each recurrent or persistent case
Persistent/recurrent lesions in case 1, ranging in size from 7 to 20 mm, were located in the left cervical lymph node levels II and IV, and the thyroid bed. Most lesions were detected by US and displayed FDG uptake in the PET/CT scan, suggesting malignancy. In case 2, a metastatic lesion was detected in the retrotracheal region by PET/CT scan, and DxWBS was also positive with a stimulated Tg level of 7.89 ng/mL. In case 3, lesions (7–12 mm in size) in the right cervical lymph node levels III and IV were detected by US and PET/CT scan, but one 13-mm-diameter lesion in the left cervical lymph node level II was detected only by US. A 9-mm lesion was present in case 4 and was located on the right thyroid bed. It was detected by both US and PET/CT scan (maximum standardized uptake value [SUVmax]=2.1). A suspicious malignant lesion (13 mm) in the cervical lymph node level II was detected by US in case 5 (Fig. 1). However, there was no identifiable lesion in the PET/CT scan. There was no lesion detected by either US or PET/CT scan in cases 6–9. A lesion in case 10 (Fig. 2), located in the left mediastinal prevascular space, was detected only by PET/CT scan (SUVmax=3.5). However, this lesion displayed radioiodine uptake in a posttherapeutic WBS.
Discussion
Recently, there has been increasing interest in use of the PET/CT scan in the diagnosis or surveillance of thyroid cancer (8). Our study focused on the role of PET/CT scan in the early period of follow-up, especially within 6–12 months after remnant ablation therapy, because the evaluation of disease status at this time is very important for predicting prognosis (16). In patients with low risk for recurrence, US and stimulated Tg have been accepted as routine surveillance tools at 6–12 months after first RAI ablation therapy but a DxWBS has not. Therefore, we restricted our study population to those who were intermediate-to-high risk for persistent/recurrent disease as hypothetically they might benefit from more intense workup in addition to US and DxWBS with stimulated Tg. We expected that PET/CT scan at 6–12 months after first RAI ablation, which requires little preparation, might have a role in early detection of disease. Our results, however, did not provide evidence for a complementary role of preemptive PET/CT scan as an adjunct to DxWBS or US in intermediate-to-high risk DTC patients, with the likely exception of a very limited number of patients.
In the ATA revised guidelines for thyroid cancer management (8), it is recommended that patients who are intermediate-to-high risk for recurrence of their thyroid cancer have US and suppressed Tg, and then stimulated Tg with DxWBS for surveillance 6–12 months after remnant ablation. The US is highly sensitive in detecting recurrent thyroid cancer (17), especially in the follow-up of low-risk patients (18). However, as US examination is an operator-dependent, one-time performance, raising the possibility that suspicious lesion may be missed. DxWBS is challenging as it requires thyroid hormone withdrawal and a low iodine diet.
PET/CT scan in thyroid cancer is typically used in thyroid cancer patients with negative DxWBS but detectable Tg levels (19). In this group it has excellent sensitivity (88.6%) and specificity (89.3%) (20), especially in patients with Tg levels exceeding 10 ng/mL (21). In addition to localizing disease, PET/CT scan has prognostic value for recurrent disease (22). Furthermore, preoperative PET/CT scans can be of significant diagnostic value in conjunction with US (23). Even in cases of papillary thyroid microcarcinoma, the presence of FDG uptake in the lesion on PET/CT scan has been thought to be useful for initial risk stratification (24).
Postoperative PET/CT scan before remnant ablation therapy has been considered to be superior to diagnostic or therapeutic WBS in detecting lesions outside of the thyroid bed, and correlate with the stage of disease or long-term outcome (25). In contrast to this study, another study reported that PET/CT scan did not provide more information than US or neck CT scan did in the initial evaluation of lymph node status (26). Thus, except for the use of PET/CT scan in patients with increased TSH-stimulated Tg levels without visible lesions in their diagnostic or therapeutic WBS, the exact role or proper timing of PET/CT scan is still debatable.
Several studies evaluated the diagnostic efficacy of PET/CT scan for follow-up of thyroid cancer patients. In one study, in which PET/CT scan was performed early in follow-up (median 18 months, range 12–30 months) in 61 patients suspected of recurrent disease, improved diagnostic accuracy was evident (27). Another study reported that PET/CT scan performed in patients with high risk for recurrence was useful to detect residual lymph node metastasis immediately after remnant ablation (28). In a recent meta-analysis study (29), PET/CT scan was suggested as a useful tool for surveillance of papillary thyroid carcinoma. However, no study has examined the diagnostic efficacy of PET/CT scan 6–12 months after the first remnant ablation. Furthermore, only one study (30), which lacked risk stratification of patients and had a small number of patients (n=12), has so far directly compared the diagnostic efficacy of PET/CT scan to that of conventional methods such as US, stimulated Tg levels, and DxWBS.
In our study, PET/CT scan detected only half of the persistent/recurrent cases. Furthermore, all cases, except one (case 10), in which the lesion was detected only by PET/CT scans, could also be diagnosed as being persistent/recurrent disease by conventional methods. All persistent/recurrent cases, except one (case 1) who had high levels of anti-Tg antibody, had increased TSH-stimulated Tg levels (>5 ng/mL). This finding is concordant with previous studies showing that the efficacy of PET/CT scan in detecting recurrent disease is high with increased Tg levels (23,31). There was one exceptional case (case 1) in whom serum Tg was undetectable and the anti-Tg antibody test was positive. In this regard it should be noted that there was a recent report that a PET/CT scan could be useful for detecting thyroid cancer in patients with positive anti-Tg antibody tests (32).
Regarding the apparently low diagnostic accuracy of PET/CT scan, it should be noted that in the five false negative cases by PET/CT scans there were three patients (cases 6, 7, and 8) who had moderately increased stimulated Tg levels (<10 ng/mL) but negative results by US and iodine uptakes confined to thyroid bed in the DxWBS. When faint iodine uptake is confined to thyroid bed, it may be clinically insignificant (33). Furthermore, as shown previously (34), there is a possibility that three aforementioned cases were not true persistent or recurrent cases. Therefore, the diagnostic accuracy of PET/CT scan might be underestimated.
The proper timing should be considered if both PET/CT scans and DxWBS are performed, specifically with respect to the contrasting stimulating role of TSH stimulation, and stunning effect of 131I, on [18F]-FDG uptake. When a PET/CT scan was taken before DxWBS, especially more than 2 weeks earlier, the lack of TSH stimulation, which can raise the detection rate of the disease by PET/CT scan (35), might impact on the results of PET/CT scan. In contrast, when a PET/CT is taken after DxWBS, radiation by 131I could have stunning effects on the PET/CT scan (36 –38). Nonetheless, although the PET/CT scans that were performed before DxWBS could not detect the five persistent/recurrent cases, these patients had adequate TSH stimulation by T4 withdrawal. Three of the subjects had their DxWBSs within a week after PET/CT scans. The remaining two patients had their PET/CT scan at least 2 weeks prior to DxWBS. The five persistent/recurrent cases, detected by PET/CT scans, were performed after DxWBS. Thus, we cannot make any conclusions regarding the proper timing of a PET/CT scan and DxWBS. However, this study suggests that stunning by 131I is clinically insignificant when PET/CT scans are performed after DxWBS in the time frames we used.
One major limitation of our study is the possibility of selection bias. As the study was retrospective, two kinds of intermediate-to-high risk patients might have been excluded from our study. One is a group of intermediate-to-high risk patients who were noted to have recurrent diseases before the use of PET/CT scans. The other is patients who had no evidence of disease based on conventional methods and did not have PET/CT scans. Assuming that all patients in the former group were included in the study, several FDG-avid lesions might exist in PET/CT scans. Nonetheless, the routine use of PET/CT scan could not be justified because conventional methods would be sufficient for detection of disease in this group. In contrast, exclusion of the latter group may cause underestimation of the efficacy of PET/CT scans as an early follow-up tool because PET/CT scan, if done, might detect some recurrent lesions. However, the recurrence rates according to revised ATA (initial) risk stratification during follow-up for a median 7 years were reported as 21% in intermediate-risk group and 68% in high-risk group (39) and more than half of the recurrences had developed within the first 2 years (40). Therefore, the recurrence rate of our study, 14% (9.2% [6/65] in intermediate-risk and 66% [4/6] in high-risk patients) for a 2-year follow-up, would not be unexpected.
Our study suggests that a PET/CT scan 6–12 months after initial remnant ablation therapy is not useful for the earlier detection of recurrent diseases. This is contrary to our hope that a PET/CT scan, even though less cost effective, may be able to detect a recurrent disease earlier and prevent the need for a strenuous course of thyroid hormone withdrawal or a high-cost rhTSH use in intermediate-to-high risk patients. The lack of a complementary role of PET/CT scan might be caused by the characteristics of persistent or recurrent lesions in early follow-up periods. As every PET/CT scan was performed early during follow-up, recurrent diseases might be too small. As previously reported, PET/CT scan is not suitable for detecting small-sized lymph node lesions, because FDG uptake in itself depends on the size of the lesions (41). Since the usefulness of single-photon emission computed tomography (SPECT)/CT images for 131I was proved in several studies (42 –44), 131I SPECT/CT could be suggested as a complementary tool to conventional methods instead of PET/CT scan. However, PET/CT scan can still be helpful in detecting disease in some cases. As proven in case 10, a PET/CT scan is a very reliable method to identify lesions in the setting of negative WBS and detectable Tg levels. In fact, the location of the lesion in the mediastinal prevascular area typically precludes detection by US. The patient with anti-Tg antibody (case 1) would have benefited from a PET/CT scan for surveillance early in the follow-up period. In addition, the approach may have prognostic value (22,45), which would require a longer follow-up to prove.
In conclusion, PET/CT scan 6–12 months after the initial RAI ablation does not provide more information regarding persistent/recurrent disease than conventional diagnostic tools such as DxWBS or US, except in very limited cases. Consistent with ATA guidelines (8), it seems reasonable to perform PET/CT scan only when there is no identifiable lesion detected by conventional methods despite of the presence of serum Tg values of >5–10 ng/mL.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.