
Abstract
Background:
Salivary dysfunction is the most common side effect associated with 131I therapy in patients with differentiated thyroid cancer. The purpose of this study was to evaluate the effect of parotid gland (PG) massage on radioisotope accumulation in the salivary gland.
Methods:
Sixty patients were included in this study. Using Tc-99m pertechnetate, two salivary scans were performed in all patients. In 30 patients, PG massage was performed between the two salivary gland scans, whereas in the other 30 patients no massage was performed between the two scans. Total counts of both PGs and accumulation ratios were calculated.
Results:
In the patients who received massage, no difference was observed between the mean PG counts of first and second images (8556.9±3333.4 count vs. 8598.3±3341.3 count, p=0.39). In the patients who did not receive massage, the mean PG count on second images was significantly higher than that on first images (8581.2±3618.0 count vs. 9096.4±3654.0 count, p<0.01). Mean accumulation ratio in the patients who received massage was significantly lower than in the patients who did not receive massage (0.5%±3.3% vs. 6.8%±3.8%, p<0.01). Further, among the patients who received massage there was a higher percentage of patients with a negative accumulation ratio than among the patients who did not receive massage (43.3% vs. 0%, p<0.01).
Conclusions:
PG massage can reduce Tc-99m pertechnetate accumulation in the PG, and thus, should be helpful to prevent salivary damage associated with 131I therapy.
Introduction
Of the salivary glands, the parotid gland (PG) most frequently produces symptoms after 131I therapy, and is known to be more radiosensitive than the submandibular salivary gland (10). External massage of the PG is presumed to be helpful in preventing parotid dysfunction after 131I therapy (3,11 –13), because it is believed to “milk out” accumulated 131I into the oral cavity, and thus, reduce radiation risks. However, no evidence has been presented that the massage of the PG actually reduces radioisotope accumulation in the PG. Therefore, the purpose of this study was to evaluate the effect of PG massage on radioisotope accumulation in the glands using Tc-99m pertechnetate salivary gland scans.
Methods
Patient population
Sixty patients (58 women and 2 men) who visited our nuclear medicine department for a thyroid scan were included in this prospective randomized study. Their ages ranged from 17 to 65 years (mean age 46.6±10.8 years). In 37 patients the diagnosis was hyperthyroidism; the other 23 patients had a normal thyroid function based on thyroid function tests and thyroid scan results. Using Tc-99m pertechnetate, two salivary scans were performed after a thyroid scan on all 60 patients. The study design was approved by the institutional review board of Kyungpook National University Hospital and informed consent was obtained.
Thirty patients were randomly chosen to receive a PG massage between two salivary gland scans; in the other 30 patients no massage was performed between scans. According to the thyroid function, patients were classified into four groups. In the patients who received massage, 18 patients with hyperthyroidism were classified as group Hyper-Mas and 12 patients with normal thyroid function were classified as group Euthy-Mas. In the patients who did not receive massage, 19 patients with hyperthyroidism were classified as group Hyper-noMas and 11 patients with normal thyroid function were classified as group Euthy-noMas. Patients with a previous history of a salivary gland disorder, diabetes, or collagen tissue disease, and patients that had previously undergone 131I therapy or external irradiation to the neck were excluded.
Data acquisition
Salivary gland images were acquired using a dual-head gamma camera (Infinia II; GE Healthcare, Milwaukee, WI) equipped with a low-energy, high-resolution collimator. Patients were placed supine in Water's position. Detectors were positioned to cover the region of head and neck. Initially, an anterior static image (2 minutes) was acquired 50 minutes after injecting 185 MBq (5 mCi) of Tc-99m pertechnetate. After one minute with or without PG massage, a second anterior static image (2 minutes) was acquired. Images were digitally recorded in a 128×128 matrix. The energy window around the 140-keV photopeak of Tc-99m was 15%.
PG massage
After obtaining the first salivary gland image, patients in the groups who received massage (the massage groups) received a PG massage in a sitting position by a physician. The physician performed bilateral PG massages from posterior to anterior along the parotid duct using both palms. During this massage, patients tightened their jaw muscles and contracted their masticator muscles to provide PG support. PG massage was performed 20 times over one minute. The method of PG massage is illustrated in Fig. 1 (3).
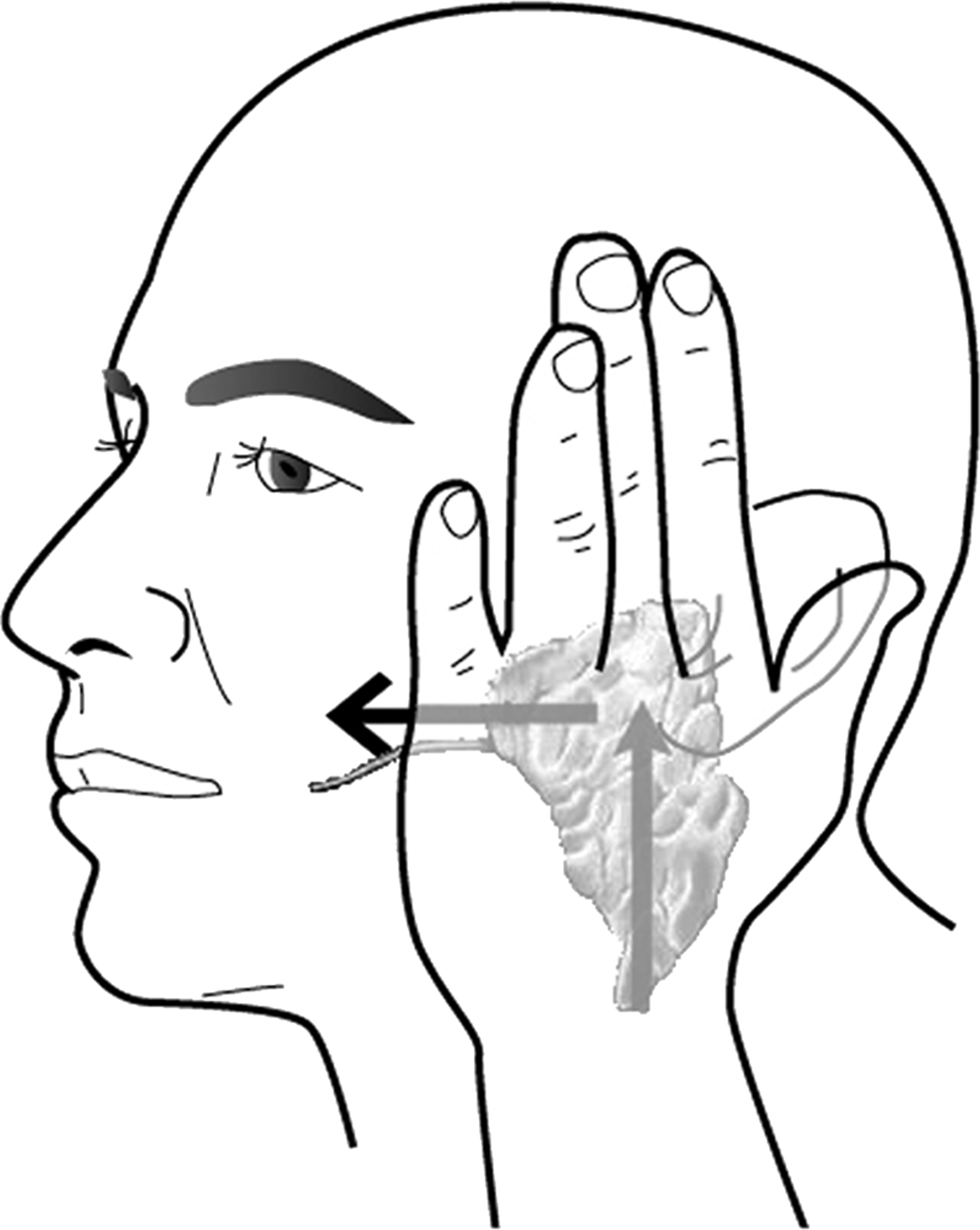
Sketch demonstrating the parotid gland (PG) massage method used (3).
Quantification of Tc-99m pertechnetate uptake in PGs
Regions of interest (ROI) over both PGs were manually drawn on first and second scans, and total counts for 2 minutes in ROIs were recorded (Fig. 2). Accumulation ratios were calculated using the total counts of PGs in first and second salivary gland images using:
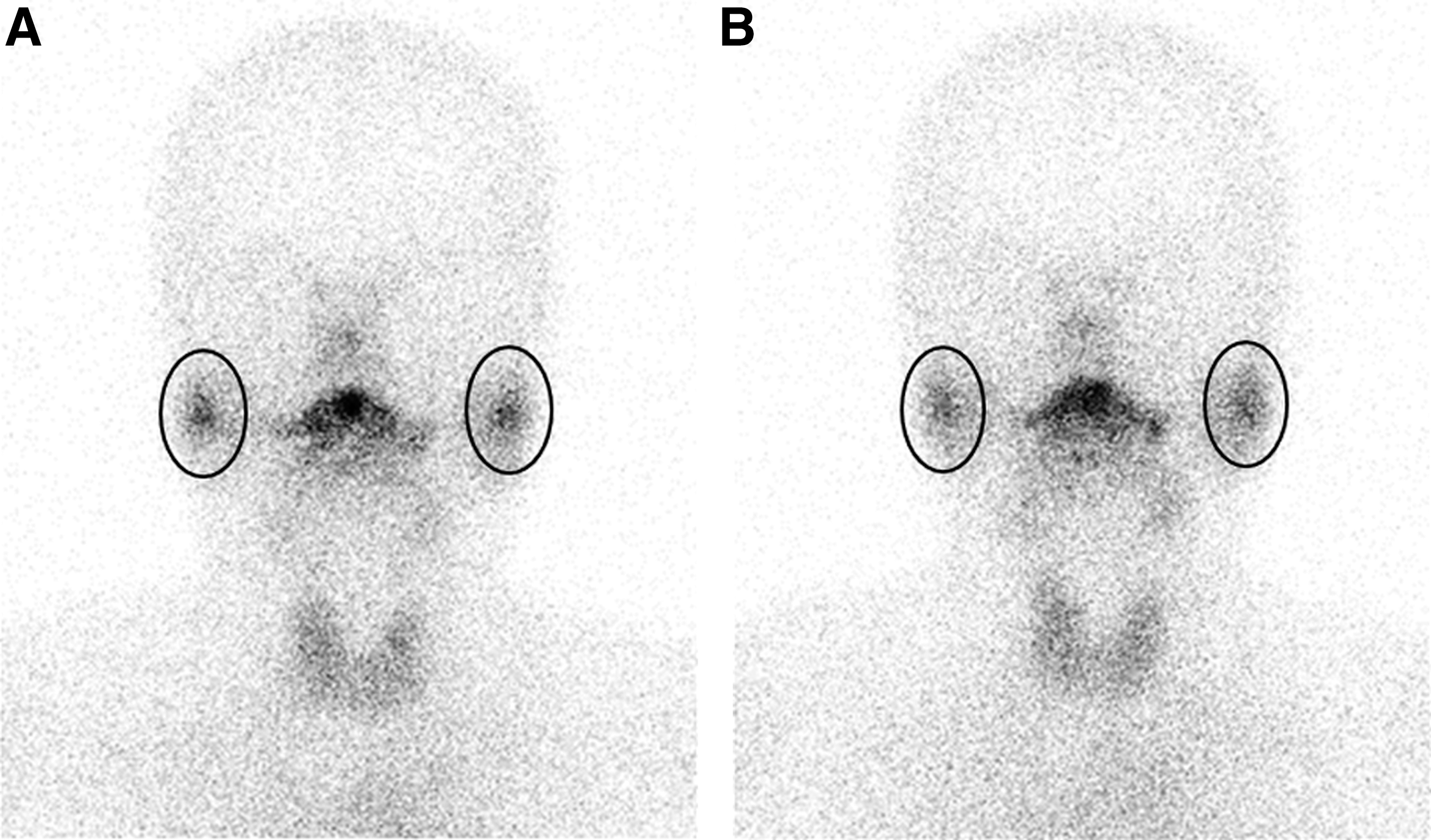
Regions of interest (ROI) were drawn manually over both PGs on first
Statistical analysis
PG counts and accumulation ratios are expressed as mean±SD. The independent two sample t-test was used to analyze differences between PG counts and accumulation ratios in the massage groups and the groups who did not receive massage (the no massage groups). The paired sample t-test was used to compare PG counts of first and second salivary gland images. Fisher's exact test was used to compare the number of patients with a negative accumulation ratio in each group. p-Values of <0.05 were considered significant.
Results
Comparison between the massage groups and the no massage groups
No patient experienced any side effect related to massage, including salivary gland pain. Results of comparisons of PG counts and accumulation ratios in the massage groups (group Hyper-Mas and group Euthy-Mas) and no massage groups (group Hyper-noMas and group Euthy-noMas) are summarized in Table 1. In the massage groups, no difference was observed between the mean PG counts of first and second images (8556.9±3333.4 count vs. 8598.3±3341.3 count, p=0.39). However, in the groups that did not receive parotid massage, the mean PG count on second images was significantly higher than that on first images (8581.2±3618.0 count vs. 9096.4±3654.0 count, p<0.01).
Massage groups: group Hyper-Mas and group Euthy-Mas.
No massage groups: group Hyper-noMas and group Euthy-noMas.
PG, parotid gland.
Mean accumulation ratio in the massage groups was significantly lower than that in the no massage groups (0.5%±3.3% vs. 6.8%±3.8%, p<0.01) (Fig. 3). Further, the massage groups had a higher percentage of patients with a negative accumulation ratio than the no massage groups (43.3% vs. 0%, p<0.01). Interestingly, patients in the massage groups with negative accumulation ratio tended to be younger than patients with a positive accumulation ratio (45.5±12.9 years vs. 51.1±10.0 years, p=0.09), and in the groups that did not receive massage, younger patients (≤41 years old) tended to have a higher accumulation ratio than older patients (7.8%±4.1% vs. 6.0%±3.3%, p=0.11).

Box plots of accumulation ratio in each group. Mean accumulation ratio in the massage groups was significantly lower than that in the no massage groups
Mean PG counts in first salivary gland images in the massage and no massage groups were almost identical (8556.9±3333.4 count vs. 8581.2±3618.0 count, p=0.979), and although mean PG count in second images in the massage groups was lower than in the no massage groups, the difference was not significant (8598.3±3341.3 count vs. 9096.4±3654.0 count, p=0.584).
Mean PG counts in patients with hyperthyroidism were lower than those in patients with normal thyroid function on both first and second images, but this was not statistically significant (8105.5±3076.8 count vs. 9314.8±3933.1 count, p=0.189 and 8422.7±3143.8 count vs. 9530.4±3939.7 count, p=0.234). No significant difference of accumulation ratio was found between patients with hyperthyroidism and normal thyroid function (4.1%±4.9% vs. 2.9%±4.5%, p=0.343).
Comparison between the four groups (Hyper-Mas, Euthy-Mas, Hyper-noMas, Euthy-noMas)
Results of comparisons of PG counts and accumulation ratios in the four study groups are summarized in Tables 2 and 3. In group Hyper-Mas and group Euthy-Mas, no differences were observed between the mean PG counts of first and second images (7563.7±2962.4 count vs. 7615.0±3010.0 count, p=0.3 and 10046.7±3420.0 count vs. 10073.3±3387.6 count, p=0.789). However, in group Hyper-noMas and group Euthy-noMas, the mean PG count on second images was significantly higher than that on first images (8618.7±3173.8 count vs. 9188.0±3152.8 count, p<0.01 and 8516.4±4452.2 count vs. 8938.2±4559.0 count, p<0.01). There was no significant difference of mean PG counts between group Hyper-Mas and group Hyper-noMas on first salivary gland images (7563.7±2962.4 count vs. 8618.7±3173.8 count, p=0.891), and between group Euthy-Mas and group Euthy-noMas (10046.7±3420.0 count vs. 8516.4±4452.2 count, p=0.879). On second salivary gland images, mean PG counts were not significantly different between group Hyper-Mas and group Hyper-noMas (7615.0±3010.0 count vs. 9188.0±3152.8 count, p=0.781), and between group Euthy-Mas and group Euthy-noMas (10073.3±3387.6 count vs. 8938.2±4559.0 count, p=0.801).
Mean accumulation ratio in group Hyper-Mas was significantly lower than that in group Hyper-noMas (0.7%±3.2% vs. 7.4%±3.8%, p<0.01) and mean accumulation ratio in group Euthy-Mas was significantly lower than that in group Euthy-noMas (0.4%±3.6% vs. 5.8%±3.7%, p=0.002) (Fig. 3B, C).
Discussion
In general, higher levels of 131I accumulation in salivary glands are associated with a greater risk of gland dysfunction (14 –16). Thus, increasing the elimination of 131I from salivary glands, or preventing its uptake by glands provides a strategy for limiting the toxicity. The present study shows for the first time that PG massage significantly decreases Tc-99m pertechnetate accumulation in the PG.
131I is used to treat thyroid cancer, and is taken up by salivary glands and by thyroid tissues because both express NIS (2,3). As a result, the β-radiation emitted by 131I damages the salivary glands, which are highly radiosensitive (17). In fact, radiation sialadenitis and xerostomia are the most frequent complications of high-dose 131I therapy in thyroid cancer (3,4,18). Further, salivary gland injury can be observed even when the administered 131I level is relatively low (4,19). Recent reviews of adverse effects of 131I therapy on salivary glands cite incidences of acute sialadenitis from 24% to 67% and of chronic sialadenitis from 11% to 43% (3 –5,19). Clinically relevant xerostomia is characterized by a dry mouth, swallowing difficulties, and a loss of a sense of taste, and markedly impairs quality of life after 131I therapy (19 –21). Thus, the prevention of salivary gland dysfunction by 131I is clinically important and methods to prevent this dysfunction are urgently required.
Efforts to reduce radiation exposure of the salivary glands include hydration, salivary stimulation with sialagogues, and salivary gland massage. Salivary stimulation with secretagogues or sialagogues, such as, pharmacologic agents (like pilocarpine and cevimeline), sour candies, gum, lemon drops, juices, and candies, have long been recommended to promote the excretion of 131I from the salivary glands despite the fact that they have never been subjected to a randomized clinical trial (7,8,19,22,23). In a blinded trial, oral sour stimulation using vitamin C was found to have a minimal effect on salivary 131I accumulation (8). Nakada et al. found that salivary gland accumulations of 131I were elevated in patients given lemon candies within 1 hour of 131I therapy compared with patients given candies 24 hours after starting the same therapy (7). They hypothesized that lemon candy can stimulate salivary blood flow and enhance tracer uptake, and thus, could increase rates of sialadenitis and xerostomia. Intravenous amifostine (an oxygen radical scavenger) given with dexamethasone and ascorbic acid has been reported to be better than placebo for reducing early and late xerostomia, but the need for intravenous administration, cost, and the unknown effect of this treatment on tumor 131I uptake have limited its use in practice (18,19,22).
PG massage might provide a straightforward means of reducing radioisotope accumulation. It physically “milks out” radioisotope into the oral cavity and does not stimulate salivary blood flow or increase radioisotope accumulation in the gland. In our study, the effect of PG massage on radioisotope excretion was found to be significant even though not very effective. It may be related to the massage mainly expel the radioisotope located in the salivary duct. The most common first symptom induced by 131I induced salivary dysfunction is obstructive nature consisting swelling and pain related to salivary retention. 131I induced radiation injury to the salivary duct might narrow the lumen of the duct and accelerate the salivary gland dysfunction (17,20). PG massage could more efficiently reduce radiation burden to the duct and more effectively prevent the injury.
In the present study, Tc-99m pertechnetate scan was used to evaluate the effect of PG massage instead of 131I scan. Salivary glands accumulate iodide and other negatively charged ions like Tc-99m pertechnetate, because cells of salivary acini and ductal lumen express NIS (24,25). 131I is orally administered for thyroid ablation or thyroid cancer treatment, therefore it is slowly accumulated in the salivary glands (3,26). Tc-99m pertechnetate was intravenously administered and its accumulation to the salivary gland was faster than orally administered 131I. However, Tc-99m pertechnetate scans can be used to predict the effect of PG massage on the salivary accumulation and excretion of 131I, because the pharmacokinetics of Tc-99m pertechnetate is known to be similar to 131I (24 –27). The plan in all subjects was that they were to have thyroid scan with Tc-99m pertechnetate and, therefore, they did not received an additional radiation burden for study purposes. In contrast to a study using 131I, only a negligible radiation dose was delivered to the researchers who were involved in this study.
Salivary gland scans can also provide quantitative data, such as, salivary gland counts and accumulation ratios, which reflect amount of accumulated radioisotope and its kinetics in the glands (14,28). Previous studies using salivary gland scan demonstrated that PG counts gradually increase and plateau without any procedure after radiotracer injection (25,28,29). In the present study, as in previous reports, PG counts significantly increased when no procedure was used between first and second scans, however, the counts were not increased after the parotid massage. Further, mean accumulation ratio was significantly lower in the massage groups than in the no massage groups. In addition, all 30 patients in the no massage groups had a higher parotid count in second than in first scans, but 43.3% of patients in the massage groups had a lower parotid count in second scans. These results demonstrate that PG massage can effectively expel radioisotope into the oral cavity in a subgroup of patients, and consequently reduce radiation exposure of the PG and its duct. It was interesting to find that younger patients tended to respond to massage better than older patients. On the other hand, in the no massage groups, younger patients tended to retain more Tc-99m pertechnetate than older patients at second scans. These results encourage us to suggest that PG massage might be more effective at reducing radiation injury to the gland in young patients. In addition, repeat massages could easily be performed at minimal cost and would further reduce the risk of side effects after the 131I therapy.
Tc-99m pertechnetate in patients with hyperthyroidism could accumulate to the salivary gland less than in patients with normal thyroid function, because thyroid uptake in patients with hyperthyroidism is higher than that in patients with normal thyroid function (30,31). In the present study, the study population included patients with hyperthyroidism and normal thyroid function and patients were classified into four groups according to the thyroid function. Mean PG counts of first images were not different from those of second images in group Hyper-Mas and group Euthy-Mas, but significantly different in group Hyper-noMas and group Euthy-noMas. Mean accumulation ratios in group Hyper-Mas and group Euthy-Mas were significantly lower than those in group Hyper-noMas and group Euthy-noMas, respectively. These results are consistent with results of comparison between massage and no massage groups. Further, these results indicate that PG massage can effectively reduce salivary accumulating radioisotope in the PG not only in patients with normal thyroid function but also in patients with hyperthyroidism.
Our study has some limitations. First, dynamic images were not acquired due to technical difficulties of acquiring data during PG massage, and time-activity curves were not evaluated. Second, the effect of PG massage on the accumulation of Tc-99m pertechnetate might differ from its effect on the accumulation of 131I. Future studies using 131I salivary gland scans are needed to confirm the effect of PG massage on the accumulation of 131I.
Conclusions
The results of the present study suggest that PG massage can expel Tc-99m pertechnetate from the PG and reduce radioisotope accumulation in the gland, and that this is probably more efficient in younger patients. Parotid massage should be helpful in protecting the PGs from radiation damage associated with 131I therapy.
Footnotes
Acknowledgments
This research was financially supported by the Ministry of Knowledge Economy (MKE), Korea Institute for Advancement of Technology (KIAT) and Daegyeong Leading Industry Office through the Leading Industry Development for Economic Region and Nuclear Research & Development Program of National Research Foundation of Korea (NRF) funded by Ministry of Education, Science & Technology (MEST; grant code: 2010-0017515) and the grant (A102132) of the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea.
Disclosure Statement
The authors declare that no competing financial interests exist.