
Abstract
Background:
In patients with differentiated thyroid carcinoma considered to be free of the disease after initial therapy, the appropriate timing or necessity of subsequent stimulated thyroglobulin (Tg) testing is uncertain. The objective of this study was to determine the value of a repeat stimulated Tg in patients considered to be free of disease 6–12 months after thyroid ablation, and also who continued to have serum Tg <1 ng/mL while on thyrotropin suppressive doses of thyroxine (T4) (Tg/T4), negative anti-Tg antibodies (TgAb), and a normal clinical examination 5 years after their initial therapy.
Methods:
The study participants were 203 patients who had total thyroidectomy followed by ablation with 131I, who were considered to be free of disease 6–12 months after ablation (stimulated Tg <2 ng/mL in the absence of TgAb and negative diagnostic whole-body scanning), who had no recurrence, and who continued to have serum Tg/T4 of <1 ng/mL, negative TgAb and a normal clinical examination 5 years after initial therapy. These patients were evaluated with repeat stimulated Tg testing after 4 weeks of T4 withdrawal.
Results:
Repeat stimulated Tg values after 5 years were <2 ng/mL in 192 (94.6%) patients of whom 188 were <1 ng/mL. Subsequent follow-up after a mean of 102 months did not detect new cases of tumor recurrence in this subgroup. Eleven patients (5.4%) had stimulated Tg levels of >2 ng/mL. Neck ultrasonography (US) revealed metastases in three and other imaging methods detected metastases in five patients with negative US. In the other three patients, no metastases were detected initially or during follow-up. Gender, age, and tumor stage were not predictors of recurrence or elevated Tg upon repeat testing after 5 years.
Conclusions:
The present results favor repeating stimulated Tg 5 years after ablation in patients who were initially considered to be free of disease and who continued to have Tg/T4 values of <1 ng/mL and negative TgAb tests. A negative predictive value of 100% was obtained for patients who continued to have low stimulated Tg values.
Introduction
In this respect, the Latin American Thyroid Society (LATS) states that “the frequency for subsequent stimulated testing is not clearly established for patients found to be free from the disease” (1), the European Thyroid Association (ETA) states “whether control of Tg following rhTSH stimulation may be useful at 3–5 years requires confirmation” (2), and the American Thyroid Association (ATA) states that “the timing or necessity of subsequent stimulated testing is uncertain for those found to be free of disease” (3).
In view of this controversy and lack of definitive recommendations, the objective of this study was to determine the value of repeat stimulated Tg testing in patients considered to be free of disease 6–12 months after ablation, who continue to have Tg/T4 values of <1 ng/mL, negative TgAb, and normal clinical examination 5 years after initial therapy.
Materials and Methods
Subjects eligible to participate in the study were patients with papillary thyroid carcinoma who have been treated with total thyroidectomy, with apparent complete tumor resection, followed by ablation with 1.1–5.5 GBq 131I. In addition, their post-therapy whole-body scanning (RxWBS) showed no distant metastases and they were considered to be free of disease 6–12 months after ablation based on stimulated Tg values of <2 ng/mL in the absence of TgAb and negative DxWBS studies. Five years after their initial therapy they were not considered to have recurrence, and their Tg/T4 values were <1 ng/mL, their TgAb test were negative, and the clinical examination was normal (Fig. 1). Patients without indication for ablation [with microcarcinoma restricted to the thyroid (1 –3,11,12)] were excluded. The study was approved and reviewed by the Research Ethics Committee of our institution.
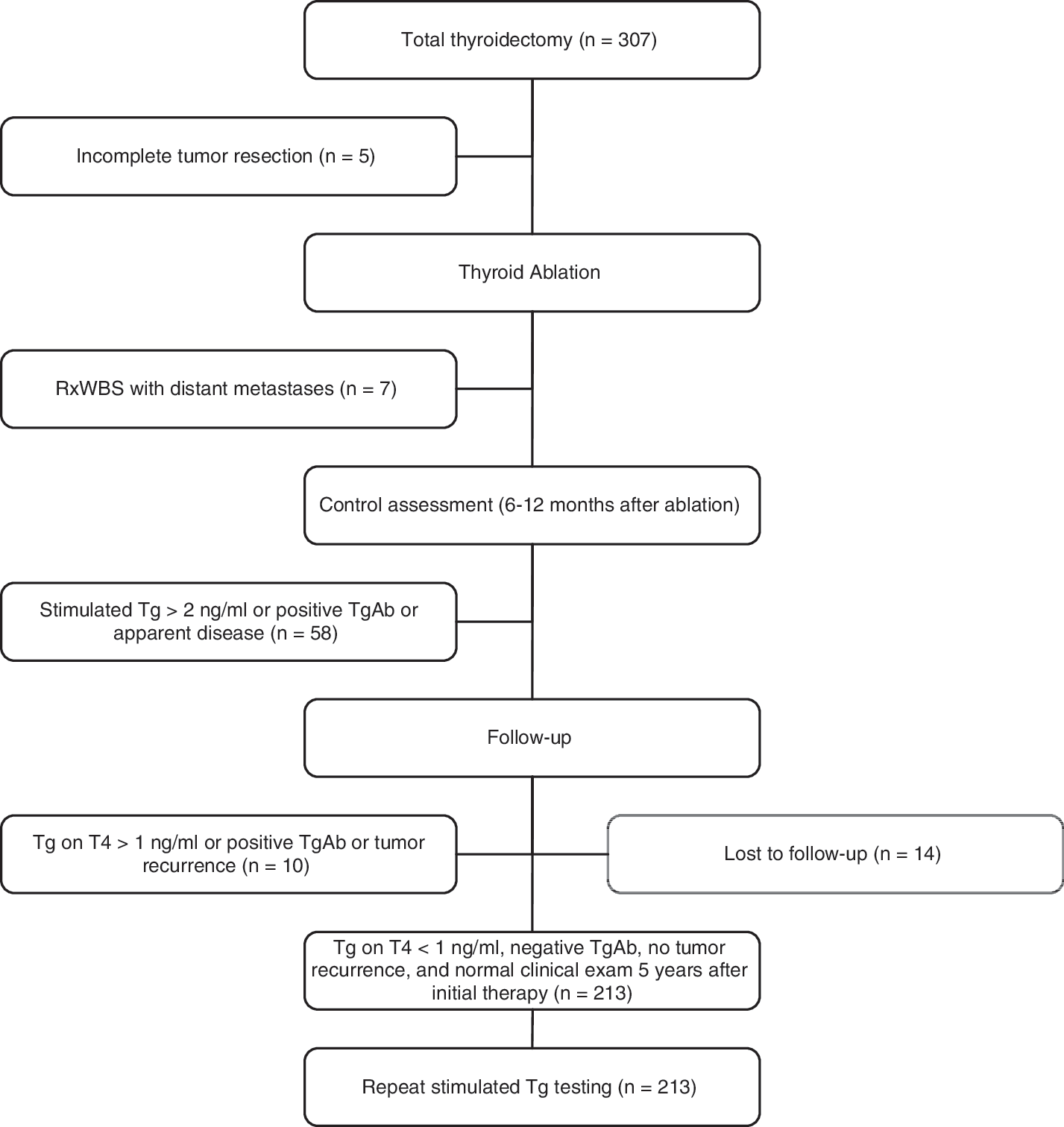
Patients excluded from the entire cohort. RxWBS, post-therapy whole-body scanning; Tg, thyroglobulin; TgAb, anti-Tg antibodies.
At our institution, until 2002, these patients were routinely submitted to repeat stimulated Tg testing for the confirmation of cure. The group included 167 women and 36 men with age ranging from 9 to 81 years (median of 49 years), with initial stage [American Joint Committee on Cancer/tumor-node-metastasis (AJCC/TNM) (3)] I, II, III, and IVA in 85, 21, 60, and 37 patients, respectively.
When the second stimulated Tg continued to be <2 ng/mL, neck US, Tg, and TgAb measurement were repeated annually during L-T4 therapy. When the second stimulated Tg converted to levels >2 ng/mL, neck US, cervical, mediastinum, and chest computed tomography (CT), and a 99mTc-methoxy isobutyl isonitrile (MIBI) scan were obtained from all patients. In the case of patients without apparent disease and stimulated Tg >10 ng/mL, an empirical activity of 131I (3.7 GBq) was administered and RxWBS was performed.
US was performed with a linear multifrequency 10-MHz transducer and all suspected lesions apparent on the scan (13,14) were evaluated by US-guided fine-needle aspiration biopsy. CT was performed on 5- to 10-mm thick sequential sections. 99mTc-MIBI scans were performed during T4 therapy using a tracer dose of 720–925 MBq and whole-body images were obtained during the early (20 minutes) and late period (6 hours). Whole-body scanning was performed with a tracer (185 MBq, DxWBS) or therapeutic (1.1–5.5 GBq, RxWBS) activity of 131I after L-T4 withdrawal for 4 weeks and administration of a low-iodine diet during the 10 days preceding the test. Anterior and posterior whole-body images were obtained 3 (DxWBS) or 7 (RxWBS) days after iodine administration.
Tg was measured by a radioimmunometric assay (ELSA-hTG; CIS Bio International) with a functional sensitivity of 1 ng/mL. TgAb were determined by chemiluminescent assay (Nichols Institute Diagnostics [detection limit of 1 IU/mL and reference value of up to 2 IU/mL]). L-T4 was withdrawn for 4 weeks before obtaining stimulated Tg.
Multivariate Cox regression models were used to assess the independent effect of different variables on the risk for elevated Tg or apparent disease. The level of significance was set at p<0.05.
Results
Among the 203 patients who met the criteria for inclusion in the study, evaluation at least 54–64 months after initial therapy revealed stimulated Tg values of <2 ng/mL in 192 (94.6%), 188 of whom had stimulated Tg values of <1 ng/mL. Subsequent follow-up (up to 144 months, mean 102 months) did not detect new cases of tumor recurrence in this subgroup.
Eleven (5.4%) of the 203 patients had stimulated Tg levels of >2 ng/mL (Table 1). Neck US revealed lymph nodes metastases in three patients. Other imaging methods (CT, 99mTc-MIBI scan, RxWBS) detected metastases in five patients with negative US (lymph nodes metastases in two, mediastinum metastases in one, and lung metastases in two) and an additional metastatic focus (in the mediastinum) in one patient with positive neck US. In the other three patients, no metastases were detected initially or during follow-up after repeat Tg stimulation, and stimulated Tg continued to be >2 ng/mL in the last assessment (2.3, 3.5, and 5 ng/mL).
Suppression of thyrotropin and change in follow-up (more frequently submitted to imaging methods).
LN, lymph nodes; CT, computed tomography; positive US, metastases LN; RxWBS, post-therapy whole-body scanning; Tg, thyroglobulin; US, ultrasonography; MIBI, methoxy isobutyl isonitrile.
No relationship could be found between the occurrence of elevated stimulated Tg 5 or more years after initial therapy and gender, age [<45 vs. >45 years (3)], or initial stage of differentiated thyroid cancer (DTC) (I and II vs. III and IVA).
Discussion
Measurement of stimulated Tg after initial therapy is recommended for patients submitted to remnant ablation with 131I, whereas different follow-up tests are used in DTC patients, either those in whom there was not an indication for thyroid remnant ablation, or those with persistent disease including incomplete tumor resection and/or evidence of distant metastases (1 –3).
Stimulation of Tg is not necessary when its levels are already elevated during L-T4 therapy, whereas its repetition (after 12–24 months) is consensually recommended when elevated Tg after TSH stimulation is observed but metastases are not readily detected (1 –3). Therefore, the discussion on the need for repeat stimulated Tg testing does not apply to these situations. Thus, by selecting patients with an indication for ablation without evident disease (or poorly differentiated carcinoma), who presented stimulated Tg <2 ng/mL after initial therapy and who continued to show Tg/T4 <1 ng/mL and negative TgAb during follow-up, we believe we have a sample that corresponds exactly to cases in which the uncertainty regarding the need for long-term follow-up stimulated Tg testing applies. The benefit of this new stimulated Tg testing in patients initially considered to be free of the disease and who continue to present Tg/T4 <1 ng/mL and negative TgAb 5–6 years after initial therapy was higher in the present study than in previous series (7 –9). Among the 203 patients studied, 5.4% converted to elevated Tg and 4% had metastases. Even if neck US would be added to Tg/T4 ∼5 years after ablation, 4% of patients in whom these tests are negative would still present repeat stimulated Tg levels >2 ng/mL, with a consequent change in clinical management (15), and metastases would be detected in 2.5%. We therefore tried to identify these differences between studies.
We do not believe that the omission of neck US in the initial evaluation contributed to the difference between the present study and the previous series (8,9). Not all metastases detected in the second assessment were seen on US scans. With respect to metastases diagnosed by this method, their detection already in the control assessment is unlikely. The fact that patients continued to present Tg/T4 <1 ng/mL, negative TgAb, and normal clinical examination for at least 5 years does not favor the hypothesis that metastases were already present upon initial assessment. In addition, the conversion of stimulated Tg to levels >2 ng/mL indicates that reoccurrence or progression occurred rather than these being cases of persistent stable metastases.
The first stimulated Tg measurement was obtained after L-T4 withdrawal (TSH>30 mIU/L) using an assay with a functional sensitivity of 1 ng/mL and in the absence of TgAb, factors that optimize the sensitivity of this marker. The adoption of a cut-off value of 2 ng/mL instead of 1 ng/mL does not seem to explain the discrepancies between the present study and the other series (7 –9). According to two recent consensuses [LATS (1) and ATA (3)], there is good evidence that a Tg cut-off level higher than 2 ng/mL following TSH stimulation is highly sensitive in identifying patients with persistent tumors.
Differences in risk stratification of the study population would also not explain the distinct percentages found in the present study and in the other series (7 –9). Only patients with well-differentiated tumors (papillary carcinoma), complete tumor resection, and no distant metastases on RxWBS were selected. In addition, when stimulated Tg and US/DxWBS are negative after initial therapy, the risk of recurrence is low even in patients initially classified as high risk based on histological characteristics (2,16 –18), so that when the results of this control assessment are considered, the importance of classical risk factors is reduced (7,9,18). Finally, in the present study initial tumor stage was a predictor of neither Tg elevation upon repeat testing, nor the presence of recurrence.
The interval between the first and second stimulated Tg testing may somehow contribute to the results. Although most recurrences are known to occur within the first 3–5 years after initial therapy (2), specifically in these cases (low stimulated Tg) a longer interval might be necessary for metastases to progress sufficiently to elevate Tg and to become apparent. In agreement with this idea, in one study (19) the interval between the control assessment and detection of metastases was >36 months in all patients with initial stimulated Tg <5 ng/mL. In the other series, this interval was 4.1 years in patients with initial stimulated Tg <0.5 ng/mL (20), and >4 years in patients with initial stimulated Tg <1 ng/mL (21). The interval between the first and second stimulated Tg measurement was <30 months in half the patients studied by Castagna et al. (9) and <36 months in all patients in the series of Crocetti et al. (8). In contrast, this interval was at least 54 months in the present study, a fact that may explain the different results and suggest that, when indicated, repeat stimulated Tg testing should be performed within this interval.
In contrast to other studies (7 –9), a recent report concluded that new Tg stimulation in patients who are initially free of disease might be interesting (10). In that study (10), two undetectable stimulated Tg measurements had a negative predictive value of 100%. In accordance, in our patients with repeat stimulated Tg levels <2 ng/mL (n=192), subsequent follow-up (up to 144 months, mean 102 months) did not reveal new cases of tumor recurrence.
Three strategies are possible for the follow-up of patients considered to be free of disease in the control assessment. First is exclusive annual clinical examination and Tg/T4 measurement, which are low cost but present lower sensitivity for the detection of recurrence. Second is the annual Tg/T4 measurement combined with a single US scan (3–5 years after initial assessment) or periodical scans, which increases the relative cost of this imaging method but provides a higher sensitivity for the detection of cervical metastases. In fact, irrespective of initial risk stratification, persistence of Tg/T4 <1 ng/mL and negative TgAb show a high negative predictive value, that is, 96.2% and 97.6% if combined with neck US showing no abnormalities. The third strategy would be annual clinical examination and Tg/T4 measurement and repeat stimulated Tg testing after 5 years. If Tg remains low, the negative predictive value would be close to 100%. Conversion of Tg to elevated levels would permit an early diagnosis of recurrences and not only those detectable by US. Furthermore, even if these recurrences were not readily apparent, patient monitoring would be intensified during follow-up considering the high positive predictive value of Tg elevation (22,23). One of the limitations of stimulated Tg testing, that is, the need for L-T4 withdrawal (associated with iatrogenic hypothyroidism), can be resolved by preparation with rhTSH (24). The elucidation of the best strategy depends on the percentage of patients who convert to elevated levels upon repeat stimulated Tg testing, the percentage of apparent disease, and the percentage of metastases detectable by US.
Except for the interval between stimulated Tg measurements, we are unable to explain the difference in these percentages between the present results, which favor repeat Tg testing, and those reported in previous studies (7 –9), which do not favor repeat testing. Further studies are necessary to resolve these differences. Nevertheless, the importance of periodical reassessment of patients and recategorization of their risk for recurrence and death seems to be clear.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.