
Abstract
Background:
Papillary thyroid carcinoma (PTC) in young people usually has an aggressive initial presentation, though a good general prognosis despite recurrences in 10%–20% of patients. A number of genetic alterations that activate the mitogen-activated protein kinase (MAPK) pathway have been found in PTC. Some of these alterations have been identified as prognostic factors of PTC in adults. The objective of the current study was to comprehensively characterize all known oncogenic alterations of the MAPK pathway in young people.
Methods:
One hundred three PTCs removed from 9 children, 19 adolescents, and 75 young adults were submitted to molecular analyses.
Results:
Altogether, 57 alterations were found in 56 PTCs (55%) corresponding to V600E BRAF in 20.3%, RAS mutations in 12.6%, RET/PTC 1 in 11.6%, RET/PTC 3 in 8.7%, and rearrangement of NTRK in 1.9%. The prevalence of all alterations increased with age (22.2% in children; 52.6% in adolescents, 51.4% in adults 20–25 years, and 55.1% in adults 25–35 years). Prevalence increased from 39.2% earlier to 61.3% after 20 years mainly due to BRAF mutations. Classic-type PTC was associated with a larger prevalence of alterations, predominantly BRAF and RET/PTC, whereas the follicular variant was chiefly associated with RAS. RET/PTC (1 and 3) was significantly associated with extrathyroid extension (ET) and lymph node metastasis (es) (LNM). This association was found in the adult group. There were no associations of BRAF or RAS mutations with ET or LNM. A 3-year median follow up was available for 90 patients. RET/PTC 1 and 3 was associated with short-term disease dissemination (cervical lymph node recurrences and distant metastases) in young adults (p=0.001). Persistent illness was more prevalent in patients with (15%) than in patients without (7%) genetic alterations.
Conclusion:
PTCs in young patients display a low prevalence of the already identified oncogenic alterations. The increasing prevalence with age is mainly due to V600E BRAF mutation. There is no relation between tumor aggressiveness and BRAF mutation. There is a relation between the presence of RET/PTC (1 and 3) and the histological and clinical short-term aggressiveness of PTC in the population of young adults. Such a relation is not found in children and adolescents.
Introduction
Patients and Methods
Patients
PTCs were collected after surgery for oncogenic molecular analyses. The same surgical team and the same pathological laboratory were involved in this retrospective study. The tumors had been removed from 103 young patients, 80 women and 23 men, between 2002 and 2010; and informed consent was obtained from all patients for tumor molecular studies. Five patients 11, 15, 24, 27, and 33 years had a history of previous malignancy treated with X-ray therapy. Treatment modalities were in accordance with national and international recommendations (28). Surgery consisted of total or near total thyroidectomy in 94% of patients. Neck dissection was performed in patients with preoperative (ultrasonography) or perioperative cervical nodal involvement (according to national consensus). This was performed in 59 patients (57%) consisting of central dissection in 51%, and central with lateral dissection in 49%. In children and adolescents, neck dissection was performed in 68.7%. Follow up (FU) studies were available for 90 patients (8 children, 17 adolescents, and 65 young adults) having a minimum duration of 2 years. The median FU was 3 years (2.5–8 years). Thirteen patients have been operated after 2008 and are not included in the FU study. Most patients in the same university hospital were followed up. According to national consensus, most patients (84%) received postoperative radioiodine (RAI) thyroid remnant ablation by administration of I131 (30–100 mCi) with whole body RAI scanning on the 5th day. If I131 extrathyroidal uptake was demonstrated, patients received iterative RAI therapy (100 mCi per treatment) or surgery depending on clinical data. Thyroid stimulating harmone (TSH) suppressive treatment was administered to all patients. Six to 9 months after RAI initial treatment, all patients underwent neck ultrasonography (US) and determination of thyroglobulin (Tg) under recombinant TSH (rTSH) stimulation. Clinical examination, additional RAI therapies, ultrasound neck examination, fine-needle aspiration cytology, if appropriate, and radiological complementary studies, if necessary, were performed yearly or more depending on clinical conditions. In addition, Tg and Tg auto–antibodies levels were determined under suppressive levo-thyroxine (LT4) treatment (confirmed by TSH levels), off LT4 or after rTSH stimulation. The functional sensitivity of Tg assay is 0.4 ng/mL (Cis Bio International), and the cut-off value is 1 ng/mL under stimulation. Disease recurrence was defined by regional or distant metastasis(es) occurring after 6 months of treatment. Pathological events in the FU included distant metastases, disclosed by abnormal RAI uptake and radiological images, either at the first evaluation or thereafter as a secondary event. Nodal recurrence was recorded after secondary surgical resection and pathological examination. Evaluation at the last visit allowed the classification to be made based on different situations. Disease-free status was defined as the absence of detectable residual disease (at US) and undetectable basal Tg and rTSH-stimulated Tg levels <1 ng/mL. Conversely, persistent disease was defined as the presence of metastasis(es) and/or inappropriately elevated Tg level that is, unsuppressed under LT4 treatment, or stimulated more than 1.5 ng/mL by rTSH, persisting or increasing with time. Written informed consent for tumor use was obtained from all adult patients and from the family of children.
Histopathology
One hundred three cryopreserved thyroid papillary tumors had been collected for studies of the MAP pathway activating mutations. All histologic slides were reviewed by the same pathologist (N.B.), for selecting an appropriate specimen for analyses and for subtyping. The samples included the CPTC, the FVPTC defined by a proportion of at least 90% of follicular structures with nuclear characteristics of PTC and subdivided into two subtypes: E-FVPTC and invasive FVPTC (I-FVPTC), the diffuse sclerosing variant PTC (DSVPTC), the solid variant PTC (SPTC), and insular component. Tumors were classified by pTNM (according to the 2009 edition) (29).
Molecular analyses
DNA RNA extraction
Frozen thyroid tumor biopsies were pulverized in liquid nitrogen using mortar and pestle and immediately collected in 1.5 mL chill tubes. RNA was extracted from a fraction of tissue pulverized (25–50 mg) by using 1 mL of TRIZOL reagent (Invitrogen) and a glass-teflon potter to homogenize according to the user's manual. DNA was extracted from 10–25 mg of tissue pulverized using QIAamp DNA Mini Kit (Qiagen) according to the user's manual. Both nucleic acids were quantified by a NanoDrop spectrophotometer.
cDNA synthesis
One microgram of total RNA was reverse transcribed using QuantiTect Reverse Transcription kit (Qiagen) following the handbook instructions. No DNase treatment was performed, because the QuantiTect Reverse Transcription kit provides an effective genomic DNA elimination by adding gDNA Wipeout buffer. The reverse transcription reaction was performed in 20 μL of final volume.
Polymerase chain reaction
Polymerase chain reaction (PCR) was prepared using HotMaster Taq DNA Polymerase (Eppendorf) in a final volume of 25 μL, with 1× HotMaster Taq Buffer with Mg2+, 200 nM of each dNTP, 200 nM of forward and reverse primers, 1 U of HotMaster Taq, and 50–100 ng of DNA template. PCR cycling parameters were as follows: an initial denaturation of 94°C 2 minutes, 35 cycles of 94°C 20 seconds, 55°C–60°C 20 seconds, 65°C 30 seconds, and a final extension of 65°C 2 minutes. Five microliters of PCR product was run on 1.3% agarose gel to check the specificity of amplification, and the remaining 20 μL was sent to direct sequencing with forward and reverse primers for each gene.
Detection of RET/PTC 1 and RET/PTC 3
This was performed according to standard–sensitivity reverse transcriptase–PCR procedure previously published (7). Briefly, 3 μg total RNA was reverse transcribed using QuantiTect Reverse Transcription Kit (Qiagen) following the manufacturer's protocol. Two microliters of cDNA samples were analyzed for RET/PTC 1 and RET/PTC 3 using 35 cycles of PCR amplification as previously reported (30). TPC1 and PC Cl 3-RE7PTC 3 cells, and previously identified RET/PTC 1 and RET/PTC 3 PTCs were used as positive controls. The RET/PTC 1, RET/PTC 3, and TRK primers sequence are listed in Tables 1 –3. All samples were assessed for the adequacy of RNA by amplification of the G6PD housekeeping gene. The PCR products were analyzed by electrophoresis on a 1.3% agarose gel and visualized by ethidium bromide staining on a Biorad GelDoc 2000 UV transilluminator.
Detection of BRAF and RAS point mutations
V600E BRAF point mutation were detected by PCR amplification of exon 15 and directly sequenced. Primers sequences, annealing temperature, and amplicon length are listed in Table 1. The DNA was tested for most common RAS mutations found in thyroid cancer, that is, NRAS codon 61, HRAS codon 61, and KRAS codons 12 and 13 point mutations using real-time Light Cycler PCR and post-PCR fluorescence melting curve analysis. For each mutation, a pair of primers and two oligonucleotide probes were designed; sequences of primers and probes are listed in Table 2. Amplification was performed using 5–50 ng of DNA, 40 pmol of each primer, 2 pmol of each hybridization probe, and LightCycler FastStart DNA Master HybProbe Kit (Roche). The reaction mixture was subjected to 40 cycles of PCR amplification consisting of denaturation at 95°C for 5 seconds, annealing at 54°C for 20 seconds, and extension at 72°C for 12 seconds. Postamplification fluorescence melting curve analysis was performed by gradual heating of samples at a rate of 0.1°C/second from 45°C to 95°C. Melting temperatures for different mutations are listed in Table 3. For each mutational hot spot, DNA from one or more tumors or cell lines known to carry a specific mutation was used as a positive control.
Statistical analyses
Analyses were performed for the whole group and for the two subgroups of patients (younger and older than 20 years): children and adolescents (27 patients), and young adults (76 patients). Analyses of FU were performed for 90 cases. Chi-square test and nonparametric Spearman linear regression were used (GraphPad Prism 4). Observed differences were assumed to be significant if a p-value was <0.05.
Results
Histopathology
Globally, ET was found in 24.2% and LNM, in 38.8% (Table 4). The proportions of ET and LNM by age groups showed a higher prevalence of LNM in patients younger than 20 years than in patients 20–35 years (p=0.1) (Fig. 1). The distribution of the subtypes of PTC is shown in Table 5. Of the 103 tumors, 54 (52.4%) belonged to the CPTC, 40 (38.8%) to the follicular subtype (FVPTC), 31 (77.5%) of them being E-FVPTC and 9 (22.5%) were I-FVPTC, 6 (5.8%) were SPTC, 1 (0.9%) was DSVPTC, and 2 (1.9%) had an insular component.

Proportions of extrathyroid extension (ET), lymph node metastases (LNM) in the two subgroups of age (<20 years and ≥20 years).
ET, extrathyroid extension; LNM, lymph node metastasis.
Distribution of oncogenic alterations in 103 tumors according to pTN staging: 2009 pTNM edition: (pT1a corresponds to infracentimetric tumors, pT1b corresponds to 1–2 cm tumors without ET). Among the 32 tumors classified as pT3, 25 had a minimal ET, and 7 tumors had a major diameter larger than 4 cm. There was no tumor corresponding to pT4; ET, ET0, and LNM, LNM0; and histopathology: CPTC, FVPTC, E-FVPTC, I-FVPTC, SPTC, DSVPTC and with insular component.
PTC, papillary thyroid carcinoma; CPTC, classic PTC; FVPTC, follicular variant PTC; E-FVPTC, encapsulated FVPTC; I-FVPTC, invasive FVPTC; SPTC, solid PTC; DSVPTC, diffuse sclerosing PTC.
Prevalence of oncogenic alterations and their relationships
Overall, 57 alterations were found in 56 PTCs (55.3%), corresponding to V600E BRAF in 21 tumors (20.3%) and to RAS mutations in 13 tumors (12.6%), located on codon 61 of N-RAS (6 tumors) or of H-RAS (7 tumors); to RET/PTC 1 in 12 tumors (11.6%) and RET/PTC 3 in 9 tumors (8.7%); and rearrangement of NTRK in 2 (1.9%) (Table 5). One CPTC, removed from an 18-year-old male patient, was found to have a double alteration, RET/PTC 1 and N-RAS.
Relations with age
The prevalence of all alterations increased with age (22.2% in children; 52.6% in adolescents, 51.4% in adults 20–25 years, and 55.1% in adults 25–35 years) (Fig. 2A), that is, 39.2% before and 61.3% after 20 years (p=0.1) mainly due to the increased prevalence of BRAF mutations (p=0.05) (Fig. 2B). RET/PTC (1 and 3) was the unique alteration in children. BRAF mutation was present in the tumors of the adolescents and predominant in those of the young adults, attaining 27% in the 25–35 age group (Fig. 2C).
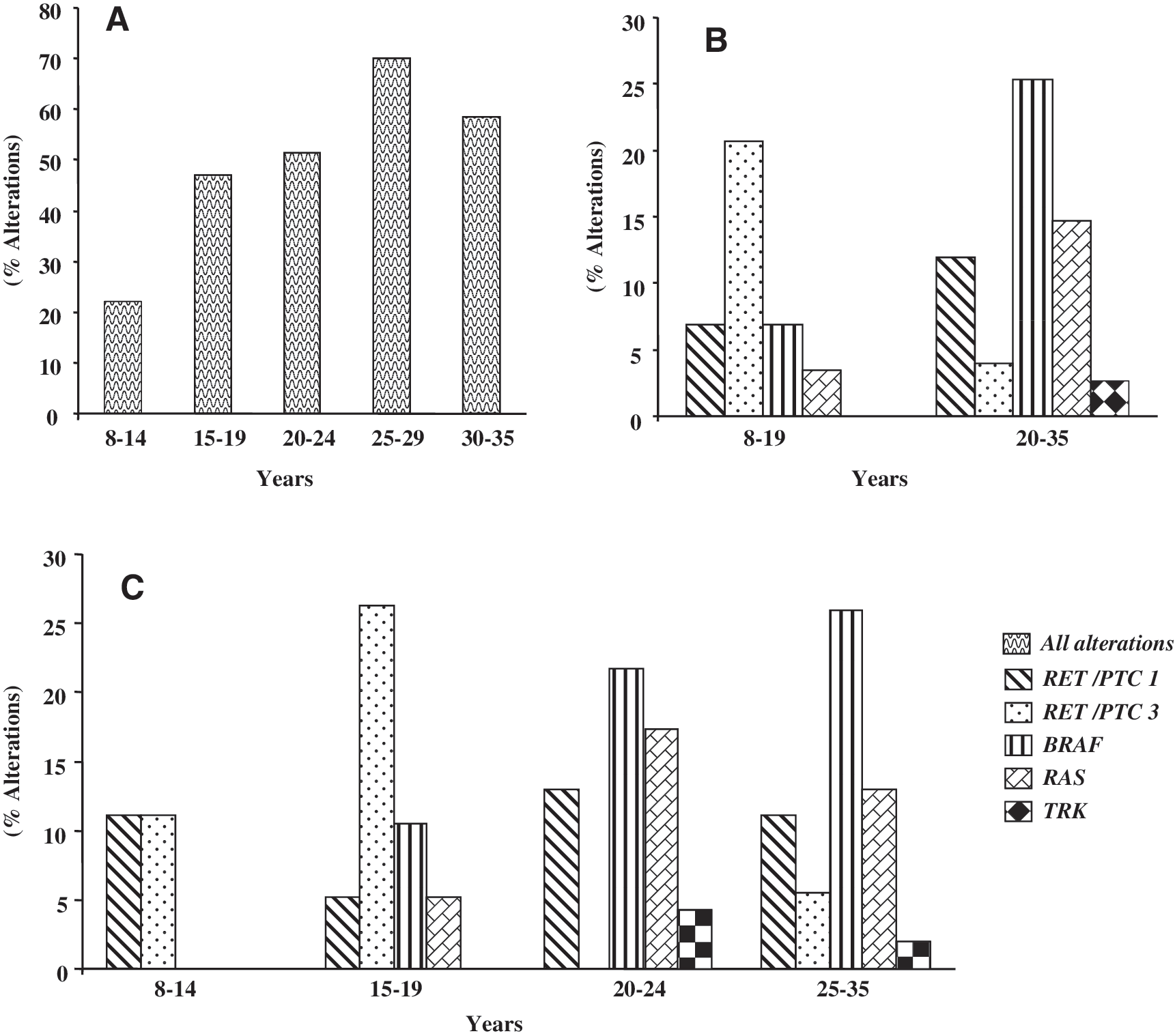
Prevalence of alterations:
Relations with histopathology
The presence of all genetic alterations was inversely related to tumor size (p<0.01), and it showed no correlation with ET or LNM. RET/PTC (1 and 3) was inversely related to tumor size (p=0.04) and was associated with ET (p=0.003) and LNM (p=0.001) when all tumors were considered. However, no correlation was found between RET/PTC (1 and 3) and ET and LMN for the children and adolescent groups taken separately. Conversely, there was a strong association between RET/PTC (1 and 3) and ET (p=0.0004), and LNM (p=0.001) in the adult group. The BRAF and RAS mutations showed no correlations with any of the above-mentioned parameters when all tumors were considered in the adult group. CPTC showed a higher prevalence of genetic alterations (72.2%) compared with FVPTC (35%) (p=0.005) (Table 5). BRAF was present in 37% of CPTC that represented 95% of all BRAF tumors. RET/PTC 1 and 3 were found in 30% of CPTC that represented 66% of all RET PTC tumors. N and H-RAS mutations were found in two CPTC pT2 N0 tumors, as a unique alteration in one tumor and associated with RET/PTC 1 in the other. Mutations were predominant in FVPTC N and H-RAS (27.5%) and represented 84.6% of all RAS tumors in the whole series. N and H-RAS mutations were present in 29% of E-FVPTC and in 22.2% of I-FVPTC (Table 5). Four of the five nonincidental infracentimetric carcinomas, two of them with LNM, had molecular alterations corresponding to RET/PTC1 in one postradiotherapy CPTC, to BRAF in one CPTC and one I–FVPTC, and to H-RAS mutation in one E-FVPTC. Four out of the five radiation-associated CPTCs had a genetic alteration: TRK rearrangement, one RET/PTC 1, and two RET/PTC 3. There was no alteration in the remaining tumor removed from an 11-year-old child, irradiated 5 years before the diagnosis of thyroid cancer.
Oncogenic alterations and clinical outcomes
FU information was available for 90 patients with a median duration of 3 years. Clinical and histopathological characteristics of these 90 cases are shown in Table 6 according to the presence or the absence of genetic alterations. Forty-seven tumors displayed 48 genetic alterations consisting of 17 RET/PTC 1+3, 19 BRAF, 8 RAS, 2 TRK, and 1 RET/PTC1+RAS. The main differences between the two groups consisted of a higher proportion of invaded lymph nodes at initial surgery (p=0.1), a higher prevalence of CPTC (p=0.001) in the group with alterations, and of FVPTC in the group without alterations (p=0.004). Initial treatments were similar for the two groups. The presence of distant metastases in lungs was detected at the first postoperative RAI evaluation in six patients, two women and four men, aged 11, 18, 23, 24, 30, and 34 years. Five of the tumors removed from these patients were stage pT3 N1b, and one was stage pT2 N0. They were five CPTC and one variant with an insular component. The five CPTC tumors carried genetic alterations consisting of (a) rearrangement of TRK in one case secondary to external radiotherapy for Hodgkin's disease, (b) rearrangement of RET/PTC1 in two, (c) rearrangement of RET/PTC 3 in one, and (d) a dual RET/PTC 1 and N-RAS mutation in one. The only tumor without alteration was the one with an insular component. Four patients had diffuse RAI uptake, and two were in remission at the last evaluation. Two patients had lung nodules (2–3/lung) and persistent disease. A 34-year-old female patient operated for an I-FVPTC without oncogenic alteration had a bone metastasis and had persistent disease despite surgical resection of the metastatic iliac bone and RAI treatment. Overall, distant metastases occurred in seven patients (7.7%). A secondary surgery for cervical metastatic lymph nodes was performed on six adults who presented with LNM at initial surgery. Oncogenic alterations were RET/PTC1 alteration in three CPTCs tumors, RAS mutation in one. No alteration was found in two CPTC tumors. The relationships between these 13 outcome events (7 distant and 6 LN metastases) and molecular abnormalities are shown in Table 7. The association between metastatic spreading (lymph node and distant metastases) and the presence of all genetic alterations was not significant. Conversely, a strong relationship was found between the presence of RET/PTC (1 and 3) and metastatic spreading when all patients were considered (p=0.001) and in the group of young adults (20–35 years) (p=0.0007) but not in the children and adolescents group (Table 8). There was no event associated with BRAF mutations. At the last evaluation, nine patients were considered as having persistent disease, due in five cases to distant metastases, in one to LNM despite complementary surgery, and in three patients to persistently elevated Tg levels without detectable metastatic localization. Disease persisted in 7 out of the 47 cases with oncogenic alteration (15%) consisting of RET/PTC (1 and 3) in all cases and in 2 out of the 43 patients without alteration (4.6%).
Alterations consisted of 19 BRAF, 17 RET/PTC (1 and 3), 2 NTRK, 8 RAS, and 1 RAS+RET/PTC. Proportions are expressed as the number of cases in each group, with and without alterations.
SD, standard deviation; RAI, radioiodine.
LNM, reintervention for metastatic cervical lymph node.
Discussion
The pathogenesis of papillary carcinoma involves the perturbation of the MAPK pathway that regulates cell growth, differentiation, and survival. Pathway disturbance is caused by the alteration of specific oncogenes: rearrangements of RET/PTC and TRK, point mutation of BRAF and RAS genes. These oncogenic events rarely overlap in the same tumor, and one of these alterations is found in more than 70% of PTC. The prevalence and significance of these alterations in younger patients were not well studied. The current retrospective study was undertaken as a part within studies of risk and prognostic factors of thyroid cancer in a population of 0–35 years. It focuses on the already identified oncogenic alterations in PTC of young patients and finds the prevalence of at least one genetic alteration in 56% of tumors. This is lower than generally reported for tumors removed from patients with a mean age of between 45 and 50 years, the average age at time of diagnosis for this cancer (3). The prevalence of at least one alteration increases with age from a low 20% in children to 60% in young adults. In children, it consists of only RET/PTC, and it is lower than that reported for sporadic pediatric tumors (11). It is worth noting that the clinical presentation in the nine children included in the current study was rather indolent, as four had metastatic lymph nodes, and one had lung metastases. The results of this reduced series of children, which seems to be representative of the Rhône Alpes region by comparison with a more extensive series (data not shown), are at odds with those reported for children with a more aggressive initial presentation and a higher prevalence of RET/PTC alterations (11). The clinical presentation of adolescent patients in the current series was more aggressive in terms of LNM and distant spreading. BRAF and RAS mutations were found in 20% of adolescent cancers, this proportion being higher than that previously reported (15,16,20). Prevalence of all alterations increases during adolescence to reach in young adults a value comparable to that published for older adults (19). In the young adults, the BRAF mutation reached a prevalence of 25%, a figure intermediate between that found in patients younger than 20 years and that found in adults unselected in age studies. A mean age of 47.7 years has been reported for the patients harboring BRAF positive tumors (8). Porra reported a prevalence of 63% in a group of adult patients living in the Rhône-Alpes region with a mean age of 45 years (31), and we found a prevalence of 47% in another group of patients 35–45 years of age (data not shown). These data confirm the progressive increase with age of tumors with BRAF mutation in the Rhône-Alpes region. In our group, the prevalence of RET/PTC alterations is comparable to that reported in most studies examining age-unselected adults (8). Genetic alterations, corresponding to RET/PTC 1, RET/PTC 3, or NTRK rearrangements, were present in four of the five tumors removed from patients subjected to therapeutic irradiation during childhood.
Regarding the relations with histopathology, the highest prevalence of alterations (73%), predominantly BRAF mutations, was found in CPTC in accordance with what is generally reported. The most represented variant in our series is FVPTC (35%). This prevalence seems rather high compared with the literature (9%–22.5%) (32), and is, however, comparable to the 31% reported by Adeniran (8). This could be a regional characteristic, as comparable proportions have been reported from the Rhône-Alpes thyroid cancer Registry (3). The E-FVPTC represents 77.5% of FVPTC. E-FVPTC possessed the highest proportion of RAS mutations (5 HRAS and 2 N RAS 30%), the unique alteration in this series, in agreement with that recently reported by Rivera (33). The prevalence of alterations and molecular profile of I-FVPTC are comparable to those of CPTC. Another particularity of the current series is the absence of the tall cell variant, a BRAF-mutated type of PTC. Taken together, these particular distributions of PTC associated with the age group of the patients are probably an explanation for the low prevalence of BRAF mutation. Four of the five nonincidental infracentimetric cancers and two of them having LNM had genetic alterations, despite the lack of aggressiveness, at variance with that reported by Lee (34). Only one double alteration (RET/PTC1 and N-RAS) was found in a CPTC tumor removed from an 18-year-old previously irradiated patient. This deviates from the pattern recently reported by Moses, where multiple genetic alterations were detected in 14.2% of a large population (35). The association between genetic alterations and anatomo-clinical data was established based on the initial presentation of aggressiveness based on tumor extension, lymph node invasion, and on the short-term FU collected for 90 patients. RET/PTC (1 and 3) was related to ET and LNM in the adults. This relationship was not found in children and adolescents, probably in relation with the reduced number of patients. This result is in agreement with a report in sporadic PTC in children and adolescents (11). In the current series, the BRAF mutation was not associated with initial aggressiveness, which is at variance with data previously reported (8). The median postoperative period was 3 years, which is generally considered too short to obtain conclusive data. It should be said that this short-term study explores the more eventful period in the evolution of PTC in young people, as postoperative events occur for 50% within the first 2 years and a further 20% within 5 years. In addition, distant metastases, namely in the lung, are usually found early after initial diagnosis, and invaded lymph nodes are secondarily removed from patients with initial LNM, as previously reported, mainly during the first 2 years after surgery (36). There is no significant relationship between the presence of all alterations and postoperative outcome, in contradiction with that previously suggested (37). By contrast, there is a link, demonstrated in this study, between RET/PTC (1 and 3) alterations and early tumor spreading in young adults. This has not been reported by others and to our knowledge, such a young adult population has not been specifically examined in previous studies. From the large group of such patients included in the current study, this population appears to be a valid intermediate between the very young, still young, and older patients, in terms of the phenotype of PTC and of the presence of genetic alterations. Should the link between RET/PTC alterations and disease evolution be confirmed in a larger series of young adults, this would indicate the need for a reinforced surveillance of this population.
Conclusion
PTCs in young patients display a low prevalence of oncogenic alterations of the MAPK pathway. The increasing prevalence with age is mainly due to the V600E BRAF mutation. The lack of relation between tumor aggressiveness and BRAF mutation could be due to the small number of BRAF mutated tumors. By contrast, there is a relation between the presence of RET/PTC (1 and 3) and the histological and clinical short-term aggressiveness of PTC in the population of young adults. Such a relation is not found in children and adolescents.
Footnotes
Acknowledgments
The authors want to warmly thank Dr. Yuri Nikiforov, Manoj S. Gandhi, and Chan Kwon Jung for having performed the RAS studies and for having contributed to this article. This work was supported by Electricité de France, Cancéropole Rhône Alpes, Région Rhône Alpes, Institut National du Cancer, Ligue de Lutte Contre le Cancer.
Disclosure Statement
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.