
Abstract
Background:
Membranous expression of the sodium iodide symporter (NIS) is a prerequisite for iodide uptake in thyrocytes. Previous studies reported heterogenous results on the relative frequency of staining in various pathological conditions of the thyroid. The present study aimed at determining membranous staining by using confocal laser microscopy in benign and malignant thyroid diseases, complemented in a subgroup of patients with recurrent or metastatic disease with functional findings of radioiodine uptake (RIU).
Methods:
There were 380 malignant thyroid tumors (145 papillary, 51 follicular, 87 Hurthle cell, and 97 undifferentiated thyroid carcinomas [UTC]), 115 benign adenomas, 62 diffuse goiters, 89 inflammatory conditions (Graves', Hashimoto, Thyroiditis deQuervain, and lymphocytic thyroiditis), and 179 normal tissues (NT, fetal, and adult). These were subjected to NIS (two different antibodies) and thyroglobulin (TG) staining and evaluated by confocal microscopy.
Results:
In a subgroup of 50 samples from patients with recurrent or metastatic disease, NIS staining was correlated with the RIU. As compared with NT, Graves' patients had significantly higher positive NIS membrane staining (>97% vs. 69%) whereas patients with Hashimoto, lymphocytic thyroiditis but also benign adenomas scored lower than NT (56.7% and 55.8% vs. 69%). Depending on their differentiation NIS staining was significantly lower in thyroid carcinomas in parallel with TG staining with only 1/97 UTCs being positive. RIU was more frequently detectable than NIS staining.
Conclusion:
Confocal staining strictly evaluating only membranous expression of NIS has not used on a large scale before this study. We confirm the loss of membranous NIS in benign but more prominently in malignant thyroid tumors. NIS staining of diagnostic tissues cannot be used to predict RIU.
Introduction
Dedifferentiation of thyrocytes is associated with a gradual loss of functional iodide uptake rendering the more aggressive tumors resistant to radioactive iodine ablation. As these dedifferentiated nonmedullary thyroid cancer (NMTC) tumors may further lose their ability to synthesize thyroglobulin (TG), TG can be successfully used as a prognostic marker in NMTC (11 –14).
Decreased NIS mRNA and protein levels in thyroid cancer reported in previous studies have been related to the differentiation state of the tumor but diverging results have been published on NIS protein and gene expression levels in thyroid disease (1,5,15,16). Most studies do not differentiate between the subcellular compartments where NIS is expressed. Further, comparison of published studies is hampered by different staining methods, the limited number of cases that were investigated, and diverging scoring methods (9,10,15 –32). The difficulties are highlighted by the fact that some articles that present data on NIS protein expression in thyroid tissue omit important information about the methods that were used (9,17 –23).
The aim of the present study was to determine the immunohistochemical staining pattern of NIS in nonmalignant and malignant thyroid tissues. We focused on membranous staining, presumably representing functional NIS protein, by using confocal laser microscopy that allows highly sensitive readings of immunohistochemical staining and comparatively more reliable discrimination among subcellular compartments. We employed two antibodies against NIS to improve the reliability of staining in case of potential differences in antibody affinities.
Materials and Methods
In the present retrospective study, 748 thyroid tissues were investigated. Of these, 368 were non-malignant and 380 were thyroid cancer. Of the latter, there were 145 cases of papillary thyroid carcinoma (PTC), 51 cases of follicular thyroid carcinoma (FTC), 87 cases of Hurthle cell carcinoma (HC), and 97 cases of undifferentiated thyroid carcinoma (UTC). All of these had been unselectively retrieved from the archive of the Institute of Pathology in Hannover between 1975 and 2002, solely on the basis of paraffin block availability. We further included a series of specimens with UTC from the Department of Pathology, University of Graz, Austria. All formalin-fixed, paraffin-embedded tissues have been diagnosed in the Institute of Pathology, Medical School of Hannover, Germany, or at the Department of Pathology, University of Graz, Austria.
Diagnostic H&E slides from each patient, collected prior to any therapy, were reviewed to confirm the diagnosis. Hashimoto thyroiditis was distinguished from lymphocytic thyroiditis by the finding that a majority of follicles were lined by variably sized Hurthle cells. Representative areas of disease were selected to be used for tissue microarray blocks (TMA). TMA containing 60 tissue spots were built using a commercially available kit (MaxArray; Invitrogen Corporation, Carlsbad, CA) as described before (33) and 4 μm sections were cut for immunostaining.
Tissue preparation for fluorescence immunohistochemistry
Sections were deparaffinized in xylene, rehydrated with a series of ethanol concentrations, and epitope retrieval was carried out in a microwave oven (30 minutes; 100°C in 10 mM sodium citrate; pH 6.0). To digest the cell membrane the tissues were incubated in Triton-X 100 (0.5%, 5 minutes) and thereafter washed with phosphate-buffered saline for three times. Subsequently, slides were incubated in a blocking buffer (1% bovine serum albumin and 0.1% Na-acid) overnight. Sections were incubated 45 minutes by primary antibodies against TG (polyclonal, rabbit-ab; Dako, Hamburg, Germany; 1:120) and NIS. For NIS, all cases were stained with a mouse monoclonal antibody (NIS1; 1:100), kindly provided by N. Morgenthaler (BRAHMS Diagnostics, Henningsdorf, Germany); a subset of cases were additionally stained with a second monoclonal clone (NIS2; 1:100) kindly provided by J. Morris (Mayo Clinic, Rochester, MN), for comparison (17).
For detection, secondary antibodies were used: either fluorescein isothiocyanate (FITC; fluorescein-conjugated AffinePure F(ab′)2, Dianova, Hamburg, Germany) labeled for NIS (1:120), or tetramethylrhodamine isothiocyanate (TRITC; Sigma, Dreieich, Germany) labeled for TG (1:90). Counterstaining was performed with ToPro3 (1:1500; Invitrogen Corporation). Finally, slides were covered with ProLong gold antifade reagent (Invitrogen Corporation).
Confocal laser microscopy
A laser scan confocal microscope, Leica Inverted-2, was used to investigate the staining pattern of NIS and TG in the thyrocytes. An argon laser beam of λ=488 nm was applied for excitation of FITC, a laser beam of λ=543 nm for TRITC, and a laser beam of λ=633 nm to stimulate ToPro3.
The fluorescent immunostained slides were examined with the 63 ×-oil-immersion objective, using triple immunofluorescence (green [NIS]–red [TG]–ToPro-blue [nuclear counterstain]). The NIS antibodies were tagged with FITC (green) and membrane staining was scored. The TG antibodies were tagged with TRITC and delineated the intracellular TG distribution.
Evaluation
Based on the evaluation methods described by Wapnir et al. (20), we scored the staining as negative (score 0), weakly positive (score 1), or strongly positive (score 2). In contrast to previously published data, only membrane-associated signals were regarded as positive, whereas cytoplasmatic staining was completely disregarded. Cases with clear membrane signals below 10% were scored 1 and above 10% were scored 2. No membrane-associated staining was scored 0. Staining intensity varied little in our series and did not influence the scoring (preliminary evaluation; data not shown). Therefore, for all further evaluation, staining intensity was disregarded (Fig. 1A–E).
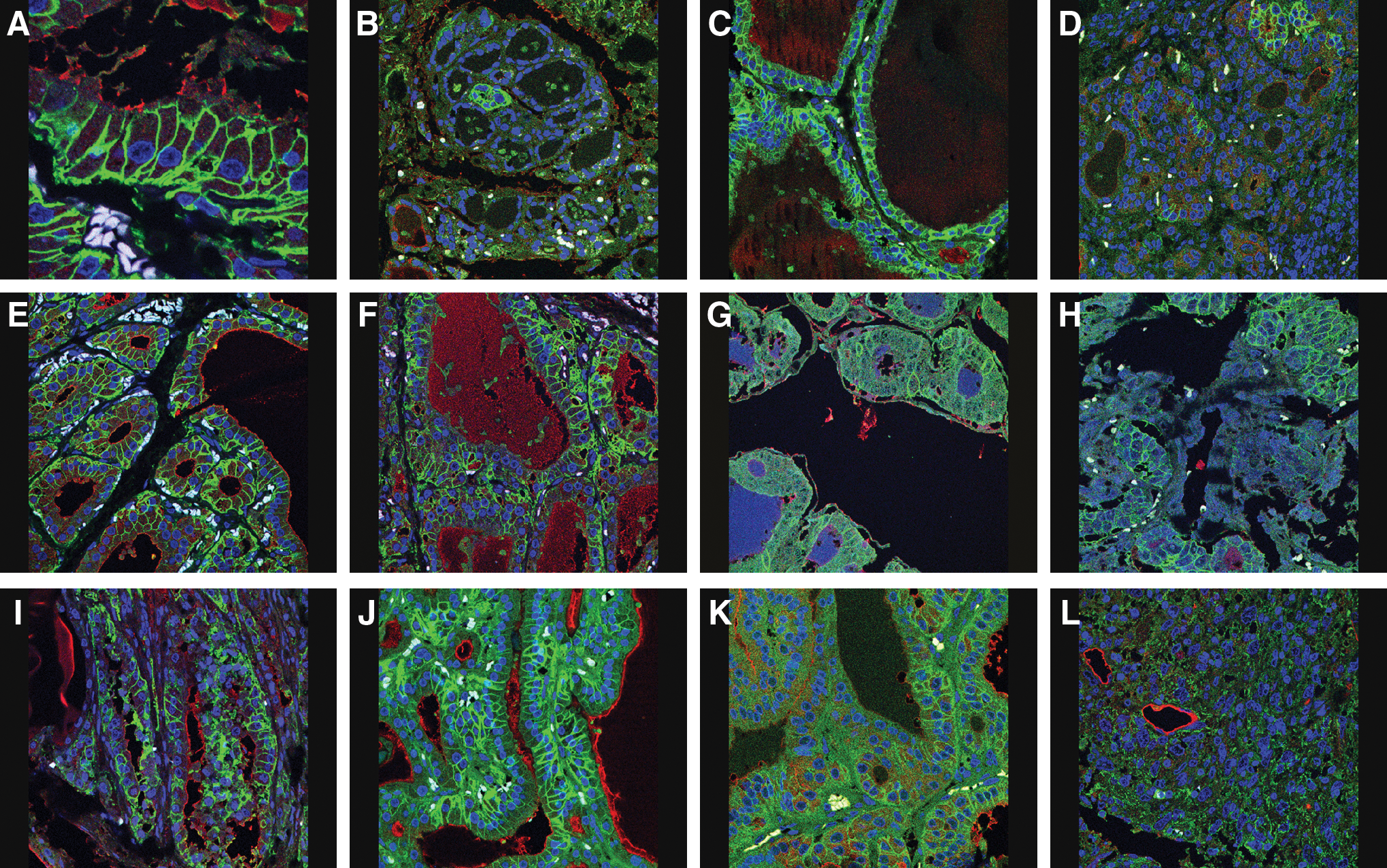
Staining pattern in confocal laser microscopy of sodium iodide symporter (NIS) (green/light gray) and thyroglobulin (red/dark gray) immunohistochemistry. Blue (medium gray) counterstain marks the nuclei.
TG staining was seen in the cytoplasm, and cases were scored only negative (no specific signal) or positive. For all evaluations, slides were read independently by two observers (I.K. and R.V.W.), who were blinded to any clinical data at the time of analysis. The overall interobserver reproducibility for estimating the NIS expression in the three groups (negative, low, or highly positive) was 96.2%. The remaining diverging cases were decided unequivocally after a second review and discussion.
Altogether, 748 cases were available for NIS1, and control staining with NIS2 antibody was performed in 657 cases (87.8%). Results for TG were evaluable in 746 cases (99.7%). In 657 cases, sufficient tissue TMA cores were available for control staining with NIS2.
All cases with differentiated carcinomas operated at the Medical School Hannover (n=196) were evaluated for follow-up data. After surgery, 124 patients were referred to other hospitals, predominantly low-risk patients with limited stage of disease. Seventy-two patients treated at our center could be retrieved from the files of the Department of Nuclear Medicine. In 50/72 (69.4%) of the patients serum TG levels were elevated and information on radioiodine uptake (RIU) was available. Thus, correlation studies of NIS protein expression in primary tumor obtained from archival tissue with the clinical data were only performed in these preselected subsets of patients.
We used the log-rank test for comparisons between groups. All statistical tests were performed using SPSS version 15.0 (SPSS, Inc., Chicago, IL).
Results
Only approximately two-thirds of normal adult thyroid cases stained positive for NIS. In patients with Graves' disease, we found the highest rates of NIS immune positivity of all subgroups and they exceeded the frequency in normal tissue (NT) (>97% vs. 69%) with typical basolateral staining in nearly all cells (Fig. 1A, E). In contrast, thyroid tissue from patients with Hashimoto thyroiditis and from patients with lymphocytic thyroiditis scored lower than normal controls (Fig. 1D; 56.7% and 55.8% vs. 69%). Consistently, a higher percentage of cells were strongly positive (score 2) in fetal tissue as compared with adult normal thyroid. These staining effects were specific for NIS staining; TG immunostaining was comparable in both tissues (Table 1). In thyroid adenomas NIS expression was lower than in normal thyroid or with diffuse thyroid goiter (Table 1 and Fig. 1F).
In parentheses, the percentage of cases showing more than 10% of cells with membrane-bound signals (Score 2).
n, number of cases investigated (NIS1: total 748 cases; NIS2: total 657 cases [87.8%]; see the Materials and Methods section).
NIS, sodium iodide symporter; PTC, papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; HC, Hurthle cell carcinoma; UTC, undifferentiated thyroid carcinoma; TG, thyroglobulin; NT, normal tissue.
Positive readings for NIS staining were reduced in differentiated thyroid carcinomas (DTCs) (PTC and FTC; Fig. 1G–J), and HC (Fig. 1K) had even lower rates of positive readings for NIS staining (Table 1). Positive readings for TG staining were highest in PTC, followed by HC and FTC (86.9%, 73.3%, and 66.7%, respectively). TG expression in DTC was comparable with that of NT and benign thyroid lesions but the percentage of NIS positive readings among cases with TG positive readings was lower. Detailed data regarding TG staining in all subgroups are shown in Table 1.
Only 1 of 97 cases of undifferentiated carcinomas that were analyzed for NIS staining was positive with the NIS1 antibody (Fig. 1L) and none of the 14 UTCs that were tested with the NIS2 antibody for NIS staining was positive. Positive immune staining for TG was detectable in only 3 of these 97 tumors.
No systematic discrepancy between staining patterns as tested for with the two NIS antibodies was detected in UTC tissues but we did note higher, though not significantly higher, rates of positive readings for NIS staining with the NIS1 antibody than with the NIS2 antibodies in tissues from normal controls, goiter patients, or from patients with inflammatory disease.
Relationship of NIS expression with postsurgical findings in DTC
In the subset of 50 thyroid cancer patients with loco-regional recurrence or metastatic disease, information regarding immunohistochemistry for NIS in the primary tumor and the results of the RIU was available. Five cases were positive and 10 were negative in both analyses. Three other cases clearly changed their RIU pattern. Two cases (No. 8 and 40; Table 2) initially stained positive for NIS and showed positivity for RIU, but later developed radionegative metastases. Interestingly, one patient (No. 34; Table 2) was initially negative for both analyses but over time developed radioiodide-positive metastases. In the majority of the remaining 32 patients, differing in NIS protein expression and RIU, no positive NIS staining was detected but they still showed positive RIU.
NIS1 positive/NIS2 negative in case No. 7, 13, and 23; NIS1 negative/NIS2 positive in case No. 41.
NIS membranous negative but positive cytoplasmatic.
Type, subtype of carcinoma diagnosed; Met-loc, localization of metastases; WBS, whole body scan; F, female; M, male; LN, lymph node; B, bone; L, lung; R, recurrence; ST, soft tissue; S, skin; +, NIS positive; −, NIS negative.
Discussion
This is the largest report on the expression of NIS in normal thyroid and in thyroid pathology that, in addition, focused on membranous NIS staining as observed by confocal microscopy. Compared with conventional immunohistochemistry, confocal microscopy has a much higher sensitivity for determining protein localization in the membrane, thus gaining information on NIS expression that is potentially functional. A potential disadvantage of using confocal microscopy is the smaller section of tissue evaluated as compared with conventional slides and immunohistochemistry. This could theoretically limit significant findings particularly for molecules with an uneven distribution within a lesion. However, neither in our present series, nor in published data, was such NIS staining pattern reported. Further, by a preselection process on representative areas of a given lesion, we were able to control the area of choice in TMA before staining. Despite this, NIS staining in the membrane was heterogeneous and restricted to single cells in normal thyroids. This finding is consistent with early functional studies in adults operated for a goiter where radioiodine labeling of active cells was found only in single cells of the thyroid follicle (34). Interestingly, NIS membrane staining was more frequent in fetal than in adult thyroids. Previous systematic studies on the ontogeneity of NIS expression during the course of human fetal development are in agreement with these results with a high NIS expression occurring in the late stages of pregnancy (35).
Our findings in Graves' disease support early data of NIS activation (36). This is not surprising given the stimulatory action of thyroid stimulatory immunoglobulins on TSH receptor signaling and NIS expression. The known intrathyroidal iodide depletion in Graves' patients will further diminish the inhibitory effects of iodide on NIS expression (37,38). Clear determination of an autoimmune origin of goiter may be important. It may explain the discrepancies between a recent report of Morari et al. on benign goiter tissue not specified for autoimmunity that found high and almost homogenous NIS expression compared with our results of normal or lower NIS expression in goiter tissue (39). Comparably membranous NIS expression is substantially reduced in our benign adenomas, an observation that is consistent with a number of previous reports (39). In DTC, NIS expression in the membrane is similarly decreased and almost completely lost in HC and UTC. HC as a special subtype of DTC displayed a lower membranous NIS positivity than PTC or FTC in our large series of 87 cases. This is particularly interesting as it is known that iodide uptake is poor in HC. Our data confirm the few cases reported so far on NIS expression in HC (17 –20,26,28) and confirm the absence of RIU in this condition (17,18). Our study represents the largest series of NIS expression in UTC reported so far (n=97). Only a single case showed weak NIS positivity in the membrane. This result contrasts with previous data where positive staining for NIS was reported in up to 1/3 of UTCs (20).
Methodological differences may in part explain the published discrepancies of NIS expression in thyroid carcinomas (1,5,9,10,15 –32). Large series reported an increased rather than decreased NIS expression in thyroid carcinomas (40). Peyrottes et al. explained an increased intracellular staining in some of the published series by nonspecific antibody binding (23). This fits our data when using two different NIS antibodies. In our series differences in the NIS peptide used for raising the antibodies (position 608–621 in NIS1 and position 468–643 in NIS2 antibodies) (17) may explain some of the differences observed, particularly, in UTCs. Thus, even though both monoclonal antibodies share a common epitope, we do not get identical results. Defective routing of the protein to the plasma membrane appears to be another important aspect. A recent study of Sodré et al. suggests that defective targeting of NIS was key to negative membranous staining (29). By using the superior sensitivity of confocal microscopy, our data support these findings. Subgroup analysis of patients with recurrent and/or metastatic thyroid cancer further supports that negative NIS staining in the membrane is an early event. The presence of positive RIU in some of these tissues may reflect different sensitivities of the methods for NIS. The very high affinity of NIS to iodide may be able to sufficiently trap iodide even at very low expression levels of the protein in thyroid carcinomas and may thus be able to result in detectable RIU. Differences are, however, more likely explained by the discrepancies in testing conditions. Whereas the tissue is stimulated by high TSH levels when the RIU is determined, NIS expression is evaluated under baseline, normal, or low TSH levels. Evidence has been shown that TSH-dependent regulatory mechanisms exist that influence NIS phosphorylation pattern and its subcellular distribution (7,18). In addition, heterogeneity of NIS expression within a tumor might influence detection rates and differences in published literature. No data are available to quantify the influence of heterogeneous NIS expression on detection rates in relation to the area of examination and the algorithm of evaluation. In either instance, it may be concluded that NIS staining of diagnostic tissues cannot be used to predict uptake of radioiodine.
In summary, we found, in a very large series of patients with a range of thyroid diseases, that NIS membrane expression is abundant in fetal tissue and tissue from patients with Graves' disease but almost completely lost in HC and UTC.
Footnotes
Acknowledgment
This work was supported by the Deutsche Krebshilfe No. 106294.
Disclosure Statement
R.v.W. is coinventor and licenser of the MaxArray Technology. For all other authors, no competing financial interests exist.