
Abstract
Background:
Diffuse sclerosing variant of papillary thyroid carcinoma (DSPC) is a rare variant of papillary thyroid carcinoma (PTC). We report a 61-year-old female of DSPC whose course was complicated by multiple metastases and an elevated serum carcinoembryonic antigen (CEA) level.
Summary:
The patient presented with upper back pain. X-ray showed an osteolytic lesion of the sixth cervical spinous process. She had a hard, nonmovable mass with fixed enlarged lymph nodes (LNs) over right neck. Fine-needle aspiration cytology revealed PTC with LNs metastasis. Positron emission tomography demonstrated multiple brain, bone, liver, and lung metastases. However, the patient had an elevated serum CEA level. She underwent a total thyroidectomy and 200 mCi radioactive 131I therapy. The pathological findings were diffuse sclerosing variant of PTC with capsular and lymph vessel invasion. A double staining of tumor specimen appeared concomitantly positive for CEA and thyroglobulin.
Conclusions:
To our knowledge, DSPC with an elevated CEA level is extremely rare.
Introduction
We describe a case of DSPC whose course was complicated by multiple brain, bone, liver, and lung metastases and an elevated serum carcinoembryonic antigen (CEA) level. DSPC with an elevated CEA level is extremely rare.
Patient
A previously healthy 61-year-old woman with no prior radiation exposure or family history of thyroid cancer suffered from upper back pain for about one month. X-ray of the cervical spine revealed osteolytic lesion of the sixth cervical spinous process. There was a nonmovable mass (about 2×3 cm) over the right thyroid gland, hard in consistency, an irregular surface with fixed enlarged lymph nodes (LNs) over right neck. The thyroid ultrasound showed a diffusely enlarged right lobe of thyroid with multiple tiny calcified spots and bilateral neck lymphadenopathy. Diffuse infiltrative tumor in the right lobe of thyroid was considered. Fine-needle aspiration of the right lobe of thyroid and fixed enlarged LNs revealed PTC as markedly enlarged follicular cells in papillary arrangement, variable in size and shape with a distinct cellular border and prominent nucleoli (Fig. 1). Baseline laboratory findings revealed a free thyroxine level of 1.15 ng/dL (normal range 0.8–1.9 ng/dL), a thyroid-stimulating hormone (TSH) level of 6.390 μU/mL (normal range 0.4–4.0 μU/mL), an antithyroglobulin antibody (ATA) level of 237.00 U/mL (normal range<60 U/mL), antibodies to thyroid peroxidase level of 12.80 U/mL (normal range<60 U/mL), a thyroglobulin level of 0.96 ng/mL (by immunochemilumiscent assays, Immulite 2000, Simens), a calcitonin level of 0.38 pg/mL (normal range<10 pg/mL), and an elevated CEA level of 205 ng/mL (normal range<6 ng/mL). Both upper gastrointestinal endoscopy and colonoscopy disclosed negative findings. For evaluation of suspicious multiple metastases, the patient received whole-body 18-fluorodeoxyglucose (FDG) positron emission tomography/computed radiographic tomography (PET-CT) imaging. The PET-CT readings were compatible with thyroid cancer with multiple lymphadenopathy bilaterally in the neck and in the mediastinum. In addition, there were multiple-organ metastases, including in the brain, lung, liver, and bone (Fig. 2).
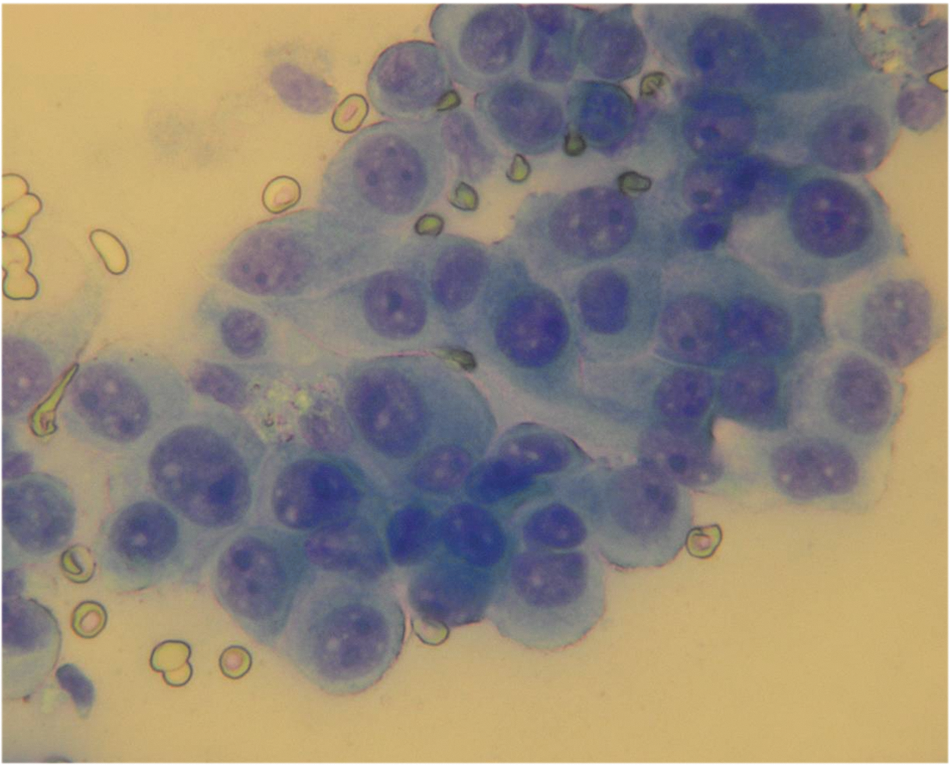
Fine-needle aspiration cytology revealed markedly enlarged follicular cells in papillary arrangement, variant in size and shape with a distinct cellular border and prominent nucleoli (Liu's stain, 400×). Color images available online at
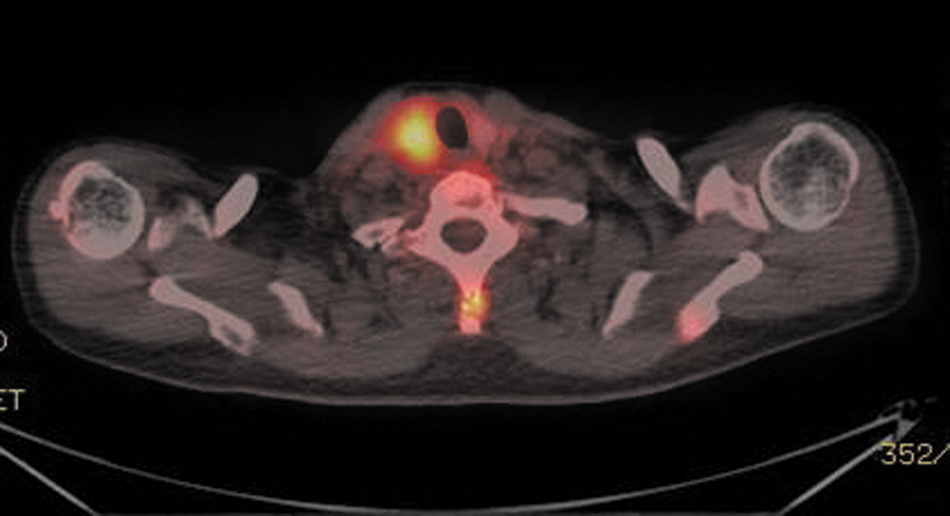
18-fluorodeoxyglucose (FDG) positron emission tomography/computed radiographic tomography imaging illustrated high 18-FDG uptake lesions over right thyroid (standardized uptake value=7.4), the sixth cervical spinous process and left side scapula. Color images available online at
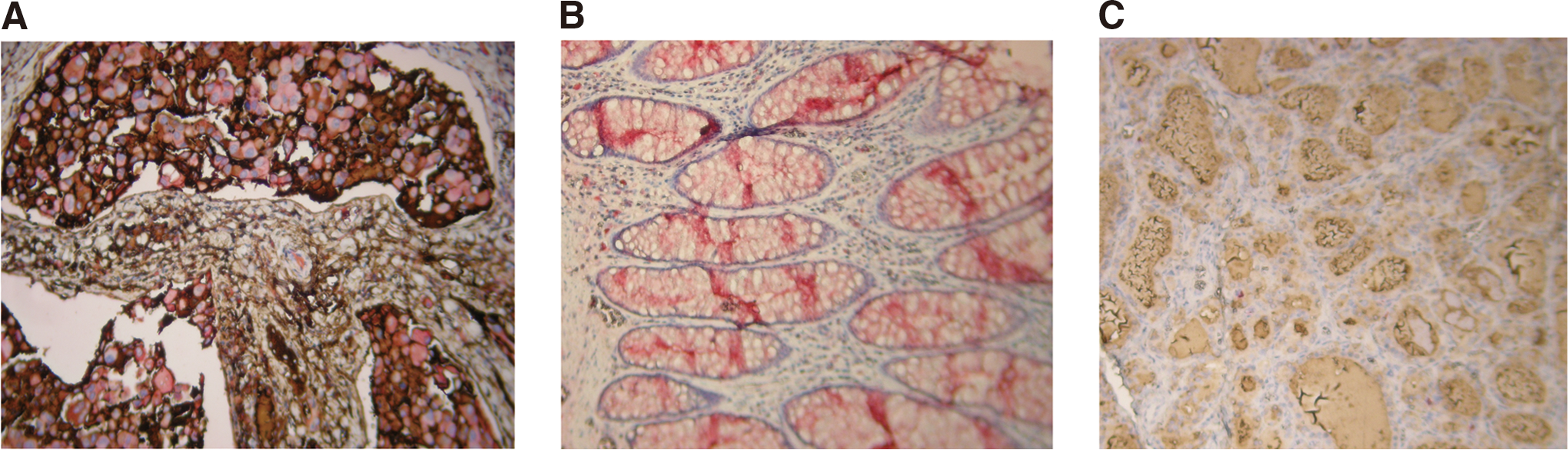
Under the impression of PTC with multiple metastases, the patient underwent total thyroidectomy, central compartment dissection, and right modified radical neck LN dissection. We also attempted to perform Level VII (anterior superior mediastinal group) dissection without opening the sternum. The histology showed a 4 cm×2.4 cm×1.5 cm tumor in the right lobe with intrathoracic extension. The microscopic findings were DSPC with capsular and lymph vessel invasion, without blood vessel invasion or squamous metaplasia (Fig. 3). There was metastasis in 17 out of 17 LNs from level II–VII. The tumor cells were immunoreactive for thyroid transcription factor-1, glucose transporter type1 (GLUT1), and thyroglobulin, weakly immunoreactive for sodium iodide symporter (NIS), while negative for synaptophysin. We also performed double staining of the tumor specimen for CEA and thyroglobulin in one slide (Fig. 4). The pathological tumor node metastases staging was pT3N1bMx. The clinical staging is stage IV C (9).
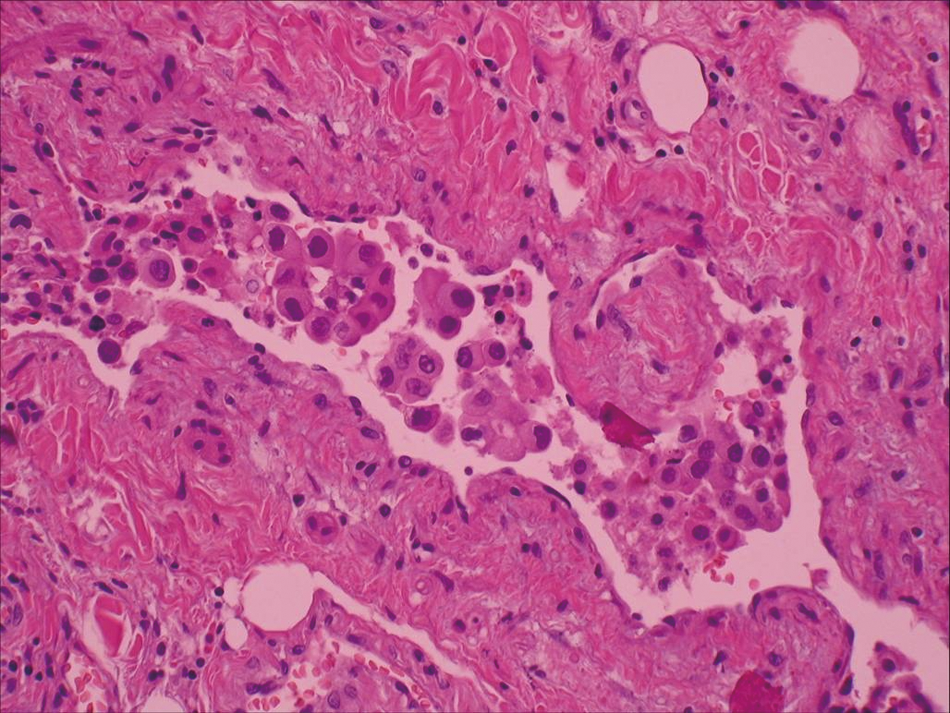
The pathological findings of the right thyroid tumor appeared marked sclerosis, lymphocytes infiltration, and nests of papillary thyroid carcinoma (hematoxylin and eosin, 400×). Color images available online at
On day 12 after operation, she received recombinant human TSH to assist ablation therapy with 200 mCi 131I. The post-therapy scan (9 days after 131I ablation) showed focal uptake in the anterior neck region and physiologic uptake in the liver, nose, and oral cavity. Abnormal focal uptake was not seen elsewhere. Palliative external radiation was performed for pain relief over fifth cervical spine to second thoracic spine and whole brain 20 Gy in eight fractions. The serum CEA level decreased mildly from 205 to 182 ng/mL 40 days after operation.
Discussion
DSPC, a rare variant, accounts for 0.7–5.3% of PTC in larger series (7,8,10). Before 2011, there were up to about 250 cases of DSPC in the literature review by Regalbuto et al. (4). Several series were published to clarify more clearly the clinical presentations (11,12), ultrasound (13), frequent RET/PTC rearrangements, and lack of BRAF mutation (14) noted in DSPC. Here we described a 61-year-old woman with DSPC, stage IVC, with multiple metastases. There seems to be female preponderance in DSPC (4), as our reported case. In the literature, the mean ages reported for DSPC (in series with more than five patients) was 18–43.2 years (4). In Korea, DSPC may even be a major subtype (49.1%) of PTC in the patients less than 20 years old (15). Only a few cases of DSPC have been reported in patients older than 60 years (4, 8,11,14). DSPC is biologically more aggressive than conventional PTC, but survival may not be significantly different (16). Squamous metaplasia transformation into aggressive squamous cell carcinoma has been associated with DSPC especially in older patients (16). Thompson et al. suggested that clinicians should aggressively manage these patients (thyroidectomy and LN dissection) in an effort to achieve an excellent long-term clinical outcome (16).
18-FDG PET-CT imaging was useful in this case for detecting the multiple metastases that were not seen by the post-therapy scan. PET-CT can offer the benefit of precise anatomic localization that planar 131I imaging lacks (17). Whether for confirmation of physiologic uptake or true pathology, PET-CT plays an important role in clarifying equivocal findings (17). In our patient, we found multiple metastases, especially liver metastases, by PET-CT, but not by liver sonography or 131I scan. The tumor showed immunoreactivity to GLUT1 by an immunohistochemical study. Liver metastases are rare in PTC. In fact, in a large series at the Mayo Clinic, only 1% of patients had distant liver metastases (18). Schönberger et al. reported that GLUT1 gene expression is related to thyroid neoplasms with an unfavorable prognosis (19). In thyroid neoplasms, an increased uptake of glucose measured by 18-FDG PET seems to be restricted to more aggressive and high-grade tumors (19). There are few reports about the PET scan in patients with DSPC (20,21). Wong et al. (20) reported that 123I was more sensitive than 131I and PET scanning for detecting residual or recurrent disease in a patient of DSPC having low preoperative thyroglobulin levels. Scott et al. (21) reported a case of DSPC with cervical LN metastasis imaged with the 18-FDG PET scan.
CEA is a useful tumor marker in medullary thyroid carcinoma (MTC) (22). It has been demonstrated that there is almost a linear relationship between abnormal preoperative CEA levels and increasing tumor size, number of LN metastases, both reflecting the overall tumor mass (22). A preoperative CEA level of >30 ng/mL in MTC almost invariably signifies intractable systemic disease (23). A CEA level >100 ng/mL is highly associated with extensively LN and distant metastases (23). In MTC, an increasing CEA level in the presence of a stable calcitonin level can be a sign of dedifferentiation of tumor and is associated with a worse prognosis (22). An abnormal serum CEA level with follicular cell-derived thyroid carcinoma has been reported by Kobayashi et al. in a 70-year-old woman of poorly differentiated follicular carcinoma having elevated serum concentrations of both thyroglobulin and CEA (22 ng/mL) (24). She died from systemic metastases 21 months after surgery (24). Ostrowski and Merino reported a high tumor recurrence rate and death in 11 cases of tall cell variant of PTC with positive CEA staining after 1 to 4 years of follow-up (25). Serum CEA levels were not measured in this series.
DSPC with elevated CEA levels, as we described here, has not yet been reported in the literature. We tried to demonstrate the tumor was producing and secreting CEA. Double staining of the tumor was concomitantly positive for CEA and thyroglobulin. The small decline in CEA levels (from 205 to 182 ng/mL) after removal of primary tumor may indicate that there was a lot of tumor mass remaining, relating to extensive distant metastases. Serum thyroglobulin levels may be falsely low by the immunochemilumiscent assay methods in the presence of antithyroglobulin antibody (26). This may be one reason why the preoperative serum thyroglobulin level was low (0.96 ng/mL) in our patient. Another explanation may be that the tumor was very poorly differentiated. This is consistent with the aggressive nature of the tumor and its lack of radioiodine uptake. Serum CEA levels, rather than thyroglobulin levels, may be the better tumor marker in following our patient.
The prognosis of DSPC still seems to be controversial (8,10,15). Falvo et al. reported that DSPC had a poorer prognosis than pure PTC with more aggressive diffuse intrathyroid growth and a high prevalence of lymph node and a pulmonary metastasis (10). On the other hand, the 5- and 10-year survival rates of DSPC were 95% (15) and 93% (8), respectively, a survival similar to conventional PTC. We consider the prognosis of our patient to be relatively poor due to her relatively old age, advanced tumor stage, and relatively small decline of CEA after her primary tumor was removed. The tumor also behaved as a poorly differentiated neoplasm based on its lack of radioiodine uptake, weak Na–I symporter staining, and high GLUT1 expression. Multiple metastases, including brain, lung, bone, and liver, which were not seen on the post-therapy scan indicate she was likely to be refractory to 131I therapy. In our patient with DSPC, the high CEA level is probably a dedifferentiated marker associated with a worse prognosis. Further experience may confirm if this is the case.
Footnotes
Disclosure Statement
The authors declare that no competing financial interests exist.