
Abstract
Background:
Although thyroid diseases exist in patients with renal failure, thyroid function tests are not routine tests in patients on chronic hemodialysis (HD). Therefore, the impact of thyroid diseases on erythropoietin (EPO) dosage in HD patients is not well defined. This study evaluated the relationship between the dose of EPO and the presence or absence of thyroid dysfunction in HD patients.
Methods:
This study included 1013 adult patients on HD who did not have a malignancy, liver cirrhosis, thalassemia, iron deficiency, gastrointestinal bleeding, or a major operation within 6 months. Patients were characterized as being euthyroid, or having the sick euthyroid syndrome, primary hypothyroidism, subclinical hypothyroidism, hyperthyroidism, or subclinical hyperthyroidism based on thyroid function tests. Routine biochemistry profiles including an index of the efficiency of HD, along with clinical data over the previous 6-month period, were collected and analyzed. Multiple regression models were employed to assess the relationship between the dose of EPO and the presence or absence of thyroid status.
Results:
The mean monthly EPO dosages were 77.7±37.0, 70.2±40.6, 90.8±68.4, 78.5±46.7, and 82.3±41.2 μg, respectively, in the sick euthyroid syndrome, euthyroid patients, hypothyroidism, subclinical hypothyroidism, and subclinical hyperthyroidism groups (p<0.05). After adjustment of all other variables in multiple regression, the mean monthly EPO dosage was 19.00±8.59 μg more in hypothyroid patients compared with euthyroid patients (p=0.027). Further, considering an interaction with the presence of diabetes, the mean monthly EPO dosage in patients with either hypothyroidism or subclinical hypothyroidism and diabetes was 54.66±17.12 μg (p=0.001) and 31.51±10.38 μg more than that of euthyroid patients, respectively (p=0.002).
Conclusions:
In HD patients, the EPO dosage required to maintain the target hemoglobin level is significantly higher in patients having both hypothyroidism or subclinical hypothyroidism and diabetes than in euthyroid patients.
Introduction
Materials and Methods
Participants
A total of 1209 patients aged ≥18 years who had received HD for more than 3 months at eight in-hospital dialysis units and six HD centers in northern Taiwan in January 2009 were screened for possible participation in this study. All patients provided written informed consent. The study protocol was approved by the institutional review board of Taipei Veterans' General Hospital (VGHIRB No. 97-07-30A) and performed in accordance with the ethical principles of the Declaration of Helsinki. To avoid misinterpretation of the treatment response to EPO, patients with other causes of poor response to EPO therapy, including the presence of a malignancy, liver cirrhosis, thalassemia, iron deficiency, gastrointestinal bleeding, and major operation within 6 months before the thyroid function evaluation, were excluded. Ultimately, there were 1013 patients recruited into this study (Fig. 1).
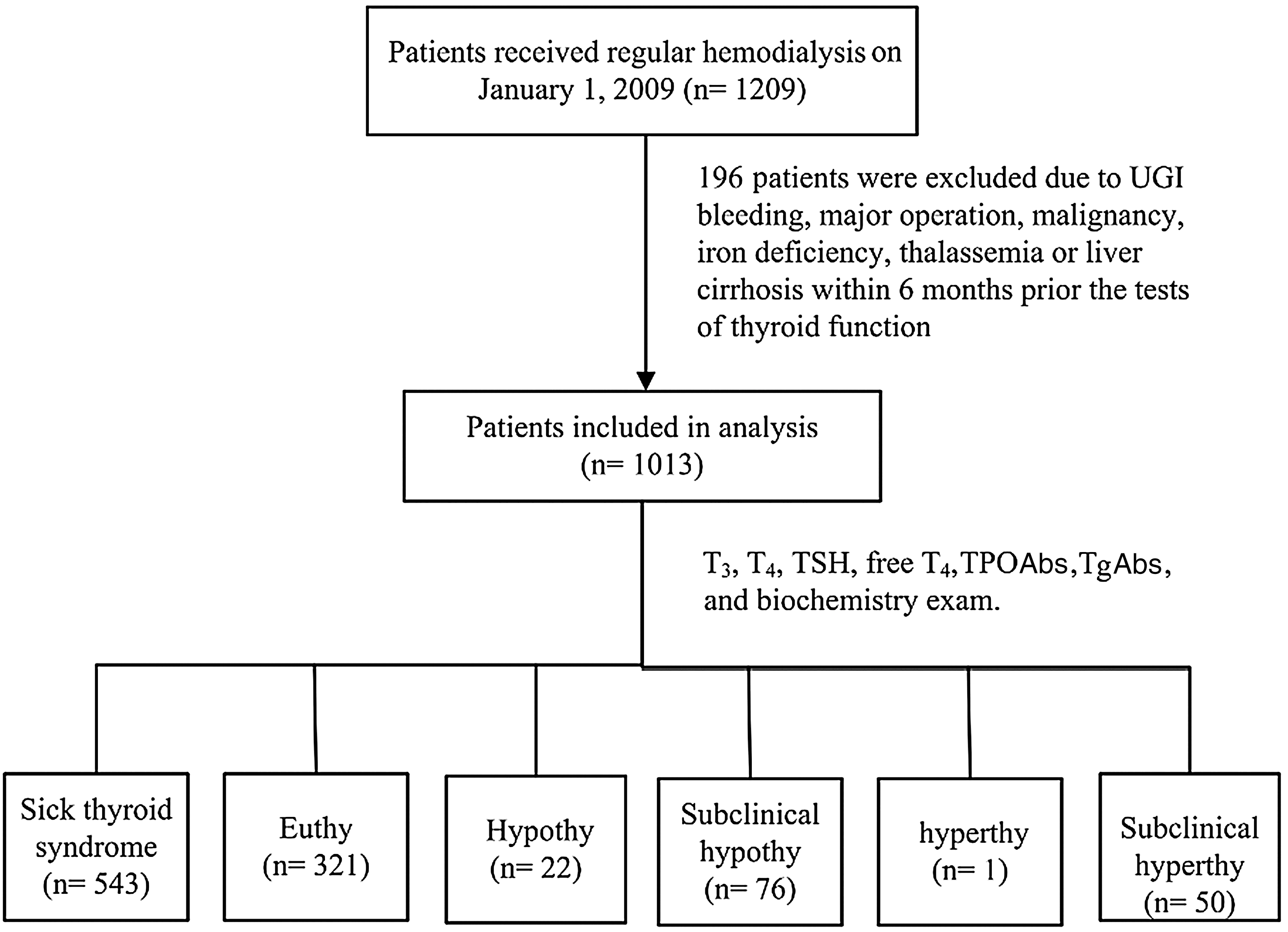
Study design and classification of thyroid dysfunction. The values of the above biochemistry data, erythropoietin dosage, and the efficacy of dialysis over a 6-month period were obtained at the time the thyroid function tests were obtained. The mean monthly values of these data were used as the basic data for our statistical analysis. UGI, upper gastrointestinal; T3, triiodothyronine; T4, thyroxine; TPOAbs, anti–thyroid peroxidase antibodies; TgAbs, anti-thyroglobulin antibodies; Euthy, euthyroid patients; Hypothy, hypothyroid patients; Subclinical hypothy, patients with subclinical hypothyroidism; Hyperthy, patients with hyperthyroidism; Subclinical hyperthy, patients with subclinical hyperthyroidism.
Blood samples and laboratory data
To ensure that the thyroid function tests were performed by the same assay and reference range, venous blood samples were drawn immediately before HD at each participating site and sent to the central laboratory at Taipei Veterans' General Hospital for measurement of serum thyrotropin (TSH), anti–thyroid peroxidase antibodies (TPOAbs), auto-antibodies against thyroglobulin (TgAbs), free thyroxine (FT4), total thyroxine (T4), and total triiodothyronine (T3) levels. TSH, TPOAbs, and TgAbs were measured by chemiluminescence using an immunometric assay (DPC Immulite 2000; Seracon Diagnostic Co., Brownsville, TX). FT4, T4, and T3 levels were measured by chemiluminescence using a competitive analogue immunoassay (DPC Immulite 2000; Seracon Diagnostic Co.). In Taiwan, each HD patient has to have a monthly biochemistry profile, which includes the serum levels of predialysis creatinine, albumin, uric acid, calcium, phosphate, glucose, and Hb, as well as efficacy of dialysis (demonstrated by Kt/V *). The serum levels of iron saturation, ferritin, and C-reactive protein (CRP) were also evaluated every 3 months. The serum level of intact parathyroid hormone was checked every 6 months. Therefore, the values of the above biochemistry data and the efficacy of dialysis over a 6-month period were obtained at the time of thyroid function tests. The mean monthly values of these biochemistry data were used as the basic data for biostatistical analysis and comparison of clinical manifestations of patients with thyroid diseases. The patients with abnormal values for serum ferritin (<38 ng/mL) or iron saturation (<10%) were defined as iron-deficient and excluded in this study.
HD patients are given subcutaneously at least 100 μg EPO monthly as required by the National Health Insurance scheme. For patients with a hematocrit (Hct) level >30%, the monthly EPO dosage is reduced. In other words, whether the EPO dosage is to be reduced depends on the patient's Hct level, which is to be kept at >30%. Since the EPO treatment is included in the HD payment package, all nephrologists try to keep iron saturation >20% and ferritin >300 ng/mL by iron supplement to reduce the cost of HD by reducing the EPO dosage. Owing to different formulations of EPO and for standardization of analysis, this study used μg as the unit of EPO. EPO 200 IU was converted to 1 μg according to the manufacturer's suggestion.
Personal data
Demographic data, including age, sex, body mass index, history of diabetes, diabetic duration, thyroid diseases, mean dosage of EPO, and efficacy of dialysis (demonstrated by Kt/V) over a 6-month period before the thyroid function tests were collected from each participating site for comparison of the basic characteristics of patients with thyroid diseases. The patients with a history of gastrointestinal bleeding, major operation, malignancy, or liver cirrhosis within 6 months before the tests of thyroid function were excluded in this study.
Definitions of thyroid diseases
The reference ranges of TSH, FT4, T3, T4, TPOAbs, and TgAbs were 0.4–4 μIU/mL, 0.8–1.9 ng/dL, 72–170 ng/dL, 4.5–12.5 μg/dL, <35 IU/mL, and <40 IU/mL, respectively. Hypothyroidism (H
Statistical analysis
The data collected were analyzed with SPSS for Windows version 13.0. The prevalence of thyroid diseases was shown by frequency. Chi-squared tests and one-way analysis of variance were conducted to examine the difference among different thyroid disease groups. Dunnett t-tests were used for the post hoc test to compare euthyroidism with other groups of thyroid disease. Stepwise multiple regression models were employed to assess the association between the EPO dosage and the Hb level among various thyroid disease groups. The variance inflation factor (VIF) is used to measure collinearity among independent variables in a multiple regression analysis. The larger the VIF, the more troublesome is the variable. Generally, VIF values >10 indicate collinearities among predictor variables.
There were only four patients in the immH
Results
Prevalence of thyroid diseases in HD patients
After the thyroid function test, the 1013 HD patients were categorized as follows: siE
Data represent number (percentage) of patients. Percentages are calculated based on the total number of patients in each disease group.
The single case of hyperthyroidism in this study was not analyzed.
TPOAbs, anti–thyroid peroxidase antibodies; TgAbs, auto-antibodies against thyroglobulin; siE
Data represent number (percentage) of patients. Percentages are calculated based on the total number of patients in the same Initial diagnosis category.
The single case of hyperthyroidism in this study was not analyzed.
H
Demographics and characteristics of thyroid diseases
The TSH levels (mean±SD, in μIU/mL) for each group were as follows: siE
N=1012; the single case of hyperthyroidism in this study was not analyzed.
The cases of immune and nonimmune-related hypothyroidism were put together for analysis.
Weighted mean EPO=mean EPO dosage/body weight.
One-way analysis of variance (# p<0.05; ## p<0.005) and Chi-squared († p<0.05; †† p<0.005) were conducted to test the difference among different thyroid disease groups; Dunnett t-tests were used for post hoc test to compare the euthyroid group with other groups of thyroid disease (* p<0.05; ** p<0.005).
RR, reference range; TSH, thyrotropin; FT4, free thyroxine; T3, total triiodothyronine; T4, total thyroxine; EPO, erythropoietin; iPTH, intact parathyroid hormone; CRP, C-reactive protein.
Comparison of patients' characteristics and clinical manifestations of thyroid diseases in HD patients
This study included 517 (51.1%) women and 495 (48.9%) men. Among them, 423 patients (41.8%) were diagnosed with diabetes and 400 patients (39.5%) were >65 years (Tables 2 and 3). Parameters such as sex, duration of diabetes, body mass index, uric acid, phosphate, intact parathyroid hormone, iron saturation, CRP, and efficacy of dialysis (Kt/V) showed no significant differences among the groups. In contrast, parameters such as patients aged >65 years, presence of diabetes, and dialysis duration >5 years varied significantly among the groups. Patients in both the siE
Subgroup analysis of diabetes
The proportion of siE
N=1012; the single case of hyperthyroidism in this study was not analyzed.
p<0.05 compared with nondiabetic hemodialysis (HD) patients who were euthyroid; ** p<0.005 compared with nondiabetic HD patients who were euthyroid; # p<0.05 compared with diabetic HD patients who were euthyroid; ## p<0.005 compared with diabetic HD patients who were euthyroid. Dunnett t-tests were used for post hoc test to compare euthyroid patients with other groups having thyroid disorders.
DM+/−, patients with and without diabetes mellitus (DM).
The predialysis creatinine in the diabetic H
Multiple regression model analysis for EPO use and Hb level
As seen in Model 1 of Table 5, the mean monthly EPO dosage was associated with sex, age, dialysis duration >5 years, hypothyroidism, and subclinical hyperthyroidism after adjustment for all other variables in multiple regression. The mean monthly EPO dosage was 19.38 μg less in male patients (p<0.001), 0.28 μg more for each additional year in age (p=0.007), 8.80 μg less in patients on dialysis for a duration >5 years (p=0.001), 19.00 μg more in hypothyroidism (p=0.027), 13.05 μg more in subclinical hyperthyroidism (p=0.026), and 5.23 μg more in diabetic patients (p=0.052). In Model 2, which is Model 1 incorporated with the interaction of diabetes with thyroid function, age (p=0.005), sex (p<0.001), and dialysis duration >5 years (p<0.001) were still significantly associated with EPO dosage. Diabetes mellitus plays a critical role in patients with hypothyroidism (p=0.001) and subclinical hypothyroidism (p=0.002). Compared with those in diabetic patients who were euthyroid, the mean monthly EPO dosage was 54.66 μg more in diabetic patients with hypothyroidism and 31.51 μg more in diabetic patients with subclinical hypothyroidism.
N=1012. Data are expressed as standardized regression coefficient (β), standard error (SE), and p-value. Stepwise multiple regression is employed to enter all significant variables in Table 3 simultaneously and to eliminate predictors gradually, one-by-one with p-to-enter=0.05 and p-to-leave=0.10, creatinine and albumin were forced in. A p-value <0.05 indicates statistical significance.
Hb, hemoglobin; ×DM, interaction between thyroid diseases and diabetes.
In Models 3 and 4, the Hb level was 0.74 g/dL higher in men (p<0.001), 0.33 g/dL higher in patients on dialysis >5 years (p<0.001), and 0.24 g/dL lower in sick euthyroid patients (p=0.006). None of the groups showed any association with the Hb level if the interaction of thyroid function with diabetes was considered (Table 5). The VIF values in the four models were <2, indicating no collinearities among predictor variables.
Discussion
A substantial number of HD patients unknowingly had laboratory evidence of thyroid dysfunction at the beginning of this study. Although this study showed that the prevalence of hypothyroidism (3%), subclinical hypothyroidism (7.5%), hyperthyroidism (0.1%), and subclinical hyperthyroidism (4.9%) in these 1013 HD patients (Table 2) resemble those in the general population (0.3%–7%, 4%–10%, 0.5%–3%, and 0.7%–2%, respectively) (2 –8,29,30), the similarities in signs and symptoms, such as lethargy, constipation, cold intolerance, poor appetite, and normochromic with normocytic anemia between uremia and hypothyroidism (10,11,13), might have misled physicians to neglect concurrent hypothyroidism in HD patients. The scarcity or even absence of clinical signs and symptoms in patients with subclinical hypothyroidism and subclinical hyperthyroidism might also be the reason for this clinical unawareness of thyroid diseases in HD patients. Therefore, clinicians should maintain a high level of suspicion for thyroid diseases in HD patients, especially in female diabetes patients requiring a high EPO dosage and/or having lower albumin and creatinine levels (Table 4). Besides thyroid dysfunction, 543 of 1012 (53.6%) patients in this study had thyroid function tests suggestive for the presence of the sick euthyroid syndrome. This finding also supports previous reports that sick euthyroid syndrome is common (37.5%–62.2%) among dialyzed uremic patients. Patients with chronic kidney disease and uremia are known to have notable effects on the hypothalamus–pituitary–thyroid axis. In particular, the secretion of pituitary TSH is impaired in uremia. Contrary to other nonthyroidal chronic disease, it is not unusual to observe the sick euthyroid syndrome in uremic patients (31 –33). Such changes in HD patients may be a self-protective adaptation to conserve energy (34,35), as in any patient during severe illness (36).
Hypothyroidism and subclinical hypothyroidism in HD patients is not as closely associated with antithyroid antibodies as it is in the general population. The presence of antithyroid antibodies (positive TPOAbs and/or TgAbs) in patients with hypothyroidism and subclinical hypothyroidism in the general population was around 54%–67% (4,30,37 –39), compared with 18.2%–25% in this study (Table 1) and in previous reports in HD patients with hypothyroidism and subclinical hypothyroidism (40,41). The reasons for this inconsistency between the proportion of antithyroid antibodies of hypothyroidism in the general population and HD patients are unclear. It is possible that chronic renal failure severely influences the immune functions of the host, and the impaired immunity of ESRD patients cannot be improved by maintenance dialysis (42,43). When vaccinations are given to dialysis patients, severely impaired vaccine responses such as low titer and responsive rate are common, especially for hepatitis B, tetanus, or influenza (44,45). Therefore, the relatively low proportion of antithyroid antibodies in hypothyroid HD patients may be related to impaired immunity. Whether the low proportion of antithyroid antibodies in HD patients with thyroid diseases is related to the burn-out phenomenon, as the serologic markers (such as antinuclear antibodies and double-stranded DNA) decline in patients with systemic lupus erythematosus who progress to ESRD (46 –48), requires further investigation. The low proportion of antithyroid antibodies in HD patients with thyroid diseases also supports previous results that retention of excess iodide or uremic toxins, rather than autoimmune mechanism, may play a principal role in the development of these thyroid diseases in HD patients (1,9,24,41,49 –52).
Tables 4 and 5 show that diabetic patients with hypothyroidism or subclinical hypothyroidism need higher EPO dosages to maintain their Hb levels, which was not related to iron status, inflammation, or efficacy of dialysis (iron, iron saturation, CRP, and Kt/V showed no significant difference among groups). These findings have not been reported before, implying that additional factors, such as hypothyroidism or subclinical hypothyroidism, may contribute to the increased demand for EPO to maintain the Hb level in diabetic HD patients. According to previous reports, hypothyroidism contributes to EPO resistance and a euthyroid state is essential for the action of EPO on the bone marrow (16 –19). Furthermore, the inappropriately low EPO level due to impaired production of EPO by the peritubular fibroblasts in patients with diabetes has been reported (20 –23). Therefore, in diabetic patients with hypothyroidism or subclinical hypothyroidism, EPO may not exhibit appropriate actions compared with diabetic patients with a euthyroid state. Diabetic HD patients with hypothyroidism or subclinical hypothyroidism need higher EPO dosage to maintain their Hb level.
As already mentioned, each month HD patients are given at least 100 μg EPO subcutaneously as required by the National Health Insurance scheme. For patients with a Hct level >30%, the monthly EPO dosage will be reduced. In other words, whether the EPO dosage is to be reduced depends on the patient's Hct level, which is to be kept at >30%. It is plausible that the adjustments made in EPO dosage to maintain the Hb level in our study resulted in no statistically significant difference in the Hb levels observed among the different groups of thyroid disease. The increased demand for EPO to maintain the Hb levels in diabetic HD patients with hypothyroidism or subclinical hypothyroidism also echoes previous results that diabetic ESRD patients have a suboptimal response to EPO and lower Hb levels (20 –23), implying that an increased EPO dose supplement can still improve the Hb production.
This study further supports previous findings that the duration of dialysis affects the rise in Hb levels in long-term dialysis patients (27,28), who have higher Hb levels and require less EPO (Table 5). The mean albumin and creatinine concentrations were 0.1–0.6 g/dL and 1.1–3.2 mg/dL lower among diabetic HD patients in each group of thyroid disease, compared with those among nondiabetic HD patients with euthyroidism in this study (Table 4). The lower albumin and creatinine levels resulting from renal loss of albumin as well as low muscle mass were reported as a common clinical feature in diabetic patients (53 –55). The symptoms of hypothyroidism, such as lethargy and poor appetite, may exacerbate the albumin and creatinine levels. In spite of the significantly lower levels of creatinine (8.0 vs. 10.3 mg/dL, p<0.05) and albumin (3.4 vs. 4.1 g/dL, p=0.001) in the diabetic hypothyroidism group compared with those in the diabetic euthyroid group (Table 4), little attention has been paid to the investigation of thyroid diseases in diabetic HD patients.
Although there are occasional reports of EPO resistance in association with hyperthyroidism (56,57), the only hyperthyroid patient in this study did not show EPO resistance and was not analyzed any further. The mean EPO dosage and weighted mean EPO dosage in HD patients with subclinical hyperthyroidism were not significantly different from those in HD patients with euthyroidism, indicating that subclinical hyperthyroidism might not be a usual cause of anemia compared with hypothyroidism and subclinical hypothyroidism.
Several methodological issues should be considered in the interpretation of our results. First, the values of metabolic parameters related to diabetes, such as microalbuminuria, were not measured in all patients. In addition, the HbA1c value was not required in the monthly biochemistry profile for each HD patient in Taiwan. The glucose levels over a 6-month period might serve as a parameter of glucose control in lieu of the HbA1c levels. Second, the onset, duration, and pathogenesis of thyroid diseases could not be determined in this cross-sectional study. Changes in antithyroid antibodies and the progression/regression of thyroid disease, such as from subclinical hypothyroidism to hypothyroidism or euthyroid state, may need further investigation. Finally, the small number of patients with hypothyroidism in the nondiabetic (12/589, 2.04%) and diabetic HD (10/423, 2.36%) groups may be due to the relatively low prevalence of hypothyroidism in this study. The thyroid controls a large number of physiological functions, and anemia is a multifactorial syndrome, particularly in this population. Thus, this study may not be able to answer all of the questions regarding the complex interactions in hypothyroid patients. Notwithstanding these possible limitations, the strength of our study is a larger sample size, which helps avoid biases present in studies with a smaller number of cases. In our large sample of HD patients, we found a strong graded association between diabetes, thyroid dysfunction, and treatment response to EPO.
In conclusion, the prevalence of thyroid diseases in HD patients is similar to that in the general population, but a substantial proportion of HD patients unknowingly have laboratory evidence of thyroid disease due to clinical unawareness. There is an interaction between thyroid function and diabetes. The EPO requirement was significantly higher in diabetic HD patients with hypothyroidism and subclinical hypothyroidism.
Footnotes
Acknowledgments
This study was financially supported by the National Science Council (NSC 96-2314-B-075-020-MY3) and the Taipei Veterans' General Hospital (V98C1-106), Taiwan. We thank Jung Ai Lu, Sandy Shan-Ying Cho, Yea Yun Chou, Shih Min Chiu, and Ya Hui Sun, our associates at Taipei Veterans' General Hospital for their technical support: We also thank Sandy Cho (Taipei Veterans' General Hospital) for her editing and valuable input.
Disclosure Statement
The authors declare that no competing interests exist.
*
Kt/V is the most widely used objective quantitative measurement of adequacy. In this formula, K=urea clearance (mL/min), t=treatment duration (min), and V=volume of distribution for urea. A Kt/V of 1.2 or more should be required for patients.