
Abstract
Background:
While cross-sectional data on thyroid epidemiology are common, few longitudinal data on the incidence and progression of thyroid disorders exist. The aim of this study was to analyze the 5-year change and the incidence of morphological and functional alterations of the thyroid gland in a previously iodine-deficient area.
Methods:
We used 5-year follow-up data based on 2941 participants (20–79 years) of the population-based Study of Health in Pomerania. The thyroid structure and size were measured by ultrasonography. Thyroid function and serum autoantibodies to thyroperoxidase (anti-TPO-Ab) were evaluated.
Results:
During follow-up, the median iodine/creatinine ratio decreased slightly from 134.2 to 130.4 μg/g. The mean thyroid volume was nonsignificantly increased by 0.73 mL [confidence interval (CI) −1.68–3.41 mL]. The incidence rate of goiter was 34.0 [CI 30.7–37.7] per 1000 person-years (py), the incident rate of nodules was 16.6 [CI 14.5–19.1] per 1000 py. Median serum thyrotropin levels increased slightly (0.10 [CI −0.10–0.34 mIU/L]). The incidence of positive anti-TPO-Ab was 3.4 [CI 2.6–4.7] per 1000 py. For all thyroid parameters, the regression rates were higher than the incidence rates.
Conclusions:
After iodine fortification became effective in this previously iodine-deficient region, there is a negative net balance between occurring and reverting goiter and nodules. Along with balanced incidences of hyper- and hypothyroid dysfunction and the low incidence of autoimmune-related findings, these findings indicate that the current iodine status is sufficient to prevent iodine deficiency-related disorders in the adult population of the study region.
Introduction
In contrast, there are only few longitudinal cohort studies on thyroid disorders. By investigating proportions of incident alterations of the thyroid gland, cohort studies may answer the question of clinicians: What is the likelihood of new cases of thyroid disorders to be expected in medical practices and hospitals? Thus, incidence rates provide a more valid estimate of the a priori probability for newly diagnosed thyroid disorders than prevalence rates. The latter are more suitable for developing an evidence-based expectation of how often known cases visit medical facilities or how many cases can be expected if screening is performed.
Although the potential value of longitudinal studies is well documented, few cohort studies that focus on thyroid disorders are available (1 –4), and some of them assessed change in thyroid function using stored biomaterials (1) or were register based (4). The only current cohort study with comprehensive assessments of thyroid morphology and function was conducted in China (2). It is not clear if findings from that study are representative for Caucasian populations of European descent and residence.
Like many regions in the world, Germany is a previously iodine-deficient country. In the late 1990s, a voluntary program based on iodine-fortified table salt became effective. Since then, population-based studies in children (5) and adults (6) have been repeatedly demonstrated median urinary iodine excretion values of about 120 μg/L. The question arises whether the current status of iodine supply is sufficient for the prevention of progressive iodine deficiency disorders in the general population.
The Study of Health in Pomerania (SHIP) is designed to observe the changes in prevalence and incidence of thyroid disorders in Northeast Germany after the introduction of an iodine fortification program. First baseline examinations (SHIP-0) were performed between 1997 and 2001 during the transition phase from iodine deficiency to sufficiency. Five years later, follow-up examinations (SHIP-1) were conducted. For the current period, an independent population sample (SHIP-Trend) was recruited to analyze the 10-year prevalence trend of thyroid disorders in this region.
Here we report the longitudinal findings at baseline and 5-year follow-up, including a comprehensive evaluation of thyroid morphology and function. The aims of the present analyses were to report the incidence of thyroid disorders in the general population and to analyze the change in thyroid-related variables over time.
Methods
Study population
SHIP is a population-based cohort study in West Pomerania, a region in the northeast of Germany. Study details are given elsewhere (7). In brief, from the total population of West Pomerania comprising 212,157 inhabitants, a sample of adults aged 20–79 years was drawn from population registries. Data collection started in October 1997 and was finished in March 2001. The net sample (without migrated or deceased persons) comprised 6265 eligible subjects. The invitation procedure included three written invitations, phone calls, and one personal contact. Finally, 4308 subjects (2193 women) participated (response 68.8%). Between 2002 and 2006, all participants were re-invited for a follow-up examination, in which 3300 subjects (83.5% of still living and achievable persons) took part (8,9). The invitation procedure for follow-up examinations was the same as for baseline, but in addition, older and immobilized subjects were offered at home examinations, which included not only interviews but also all laboratory and ultrasonography examinations. All participants gave written informed consent, and the study conformed to the principles of the Declaration of Helsinki as reflected by an a priori approval of the Ethics Committee of the University of Greifswald.
Of the 3300 participants (1711 women) who participated in both baseline and follow-up examinations, all 297 subjects (228 women) with known thyroid disorders at baseline and a further of 62 subjects (60 women) who had taken antithyroid medication at baseline were excluded, resulting in a study population of 2941 subjects (1423 women) available for the present study. As illustrated in Figure 1, subjects having each of the specific thyroid disorders at baseline were excluded from incidence analyses for specific thyroid disorders.
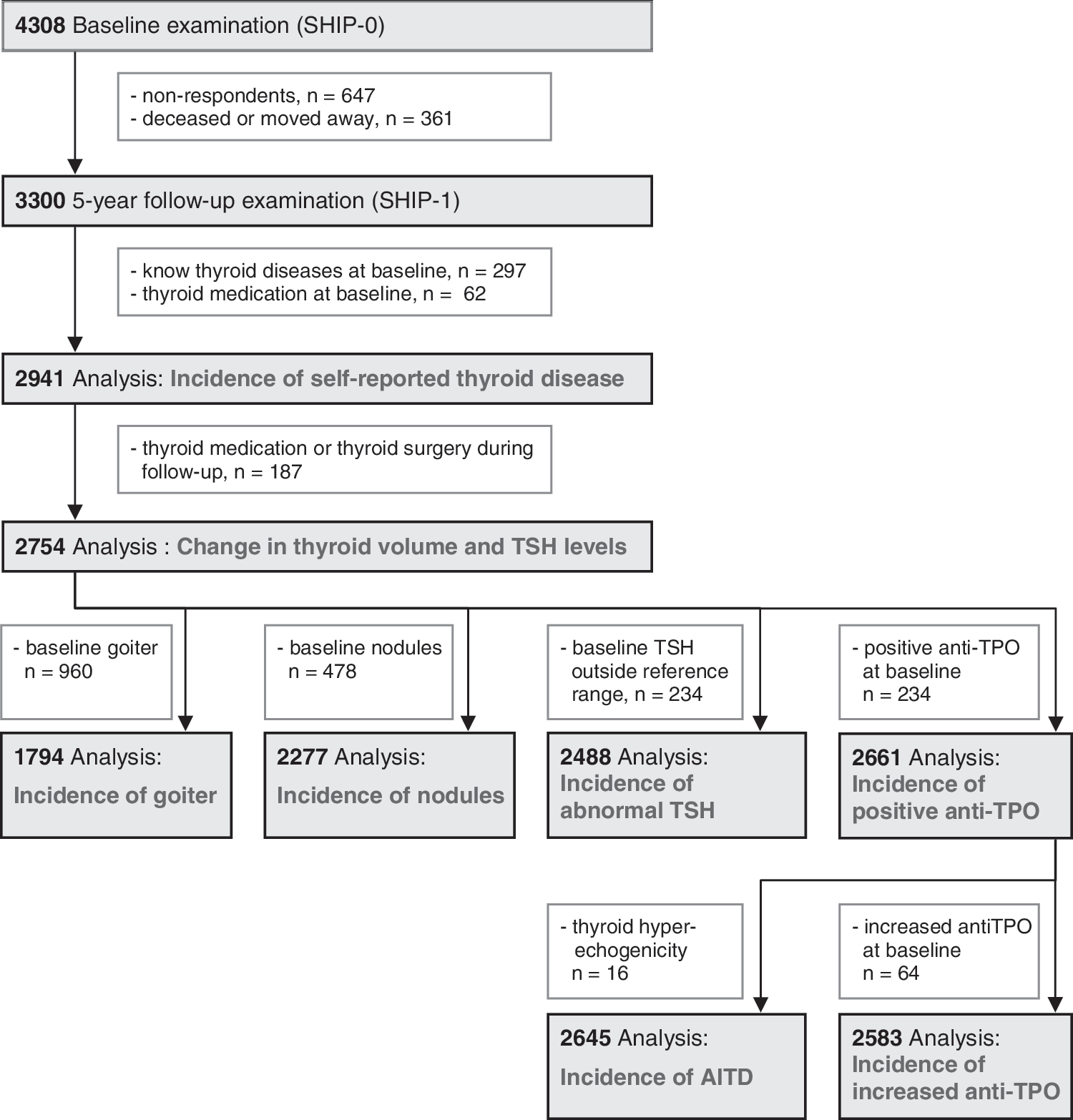
Flow diagram illustrates exclusion criteria and sizes of study population for each of the subanalyses.
Measurements
The sociodemographic characteristics and medical history of subjects with thyroid disorders were assessed by computer-assisted personal interviews.
Blood samples were taken, and laboratory parameters were analyzed in one central laboratory. In the baseline SHIP investigations, serum thyrotropin (TSH) and free- thyroxine (FT4) levels were analyzed by an immunochemiluminescent procedure (LIA-mat; Byk Sangtec Diagnostica GmbH). The functional sensitivity of the TSH assay was 0.03 mIU/L. The reference range recently established for the SHIP region was 0.25–2.12 mIU/L for TSH and 8.3–18.9 pmol/L for FT4 (10). TSH levels <0.25 mIU/L were considered decreased, and levels >2.12 mIU/L increased. At follow-up, serum TSH and FT4 levels were also analyzed by an immunochemiluminescent method (Immulite 2000; Third generation, Diagnostic Products Corporation, DPC). Method comparison of the DPC method against the Byk Sangtec method revealed a regression equation according to Passing-Bablock (11) of y=1.029x – 0.032 mIU/L for TSH, and y=1.058x – 6.238 for FT4. All serum TSH and FT4 levels from the follow-up investigation were corrected using this formula. While FT4 levels at baseline were analyzed in all participants, they were only determined at follow-up when TSH levels were outside the reference range. Coefficients of variation for TSH were 5.0% at 0.3 mIU/L, 3.7% at 16.1 mIU/L, and 8.9% over the whole study period. Coefficients of variation for FT4 were 4.1% at 12.0 pmol/L, 3.8% at 17.4 pmol/L, and 12% over the whole study period.
Serum TSH levels below 0.25 mIU/L with FT <18.9 pmol/L were defined as subclinical hyperthyroidism. Overt hyperthyroidism was defined according to serum TSH levels below 0.25 mIU/L and FT4 levels above the reference range. Serum TSH levels above 2.12 mIU/L with FT4 >8.4 pmol/L were defined as subclinical hypothyroidism. Overt hypothyroidism was defined according to serum TSH levels above 2.12 mIU/L and FT4 levels below the reference range.
At baseline and follow-up, serum autoantibodies to thyroperoxidase (anti-TPO-Ab) were measured by an enzyme immunoassay (VARELISA; Elias Medizintechnik GmbH). The functional sensitivity of this assay was 1 IU/mL, and the coefficient of variation over the whole study period was 12%. The reference range provided by the manufacturer was <60 IU/mL for men and <100 IU/mL for women. The anti-TPO-Ab status was defined as follows: normal, <60 IU/mL in men and <100 IU/mL in women; elevated, >60 IU/mL in men and >100 IU/mL in women; positive, >200 IU/mL in both sexes (6).
Urinary iodide concentrations were measured in spot urine samples, which were taken exclusively for the iodide analysis. Iodine concentrations were evaluated by a photometric procedure (Photometer ECOM 6122; Eppendorf) with the Sandell and Kolthoff reaction (12). Urinary creatinine concentrations were determined with the Jaffé method (SHIP-0: Hitachi 717; Roche Diagnostics, SHIP-1: Dimension RXL; Siemens). The limit of detection was 1 μg/L. Coefficients of variation were 9.3% at 50 μg/L, 2.1% at 100 μg/L, 1.9% at 200 μg/L, and 4.2% at 300 μg/L. The iodine/creatinine ratio was calculated by dividing urinary iodine by urinary creatinine concentration.
Thyroid ultrasonography was performed in both examinations using an ultrasound VST-Gateway with a 5-MHz linear-array transducer (Diasonics). Thyroid volume was calculated as length×width×depth×0.479 (mL) for each lobe (13). The intra- and interobserver reliabilities were assessed before the start of the study and semiannually during the study. All measurements of the thyroid volume showed mean differences (±2 standard deviation) of the mean bias of <5% (<25%) (14). To warrant best possible comparability between baseline and follow-up, all examinations were conducted using the same devices, which were checked weekly by phantom measurements. Thyroid volume progression was defined as the difference between the thyroid size at follow-up and baseline. Goiter was defined as a thyroid volume >18 mL in women and >25 mL in men (15). If the echo pattern was not homogeneous, showing small lesions or distinct diffuse abnormalities in the echotexture of the gland, it was classified as inhomogeneous. Nodular changes exceeding 10 mm in diameter were defined as nodules. A homogeneous echo pattern with reduced echogenicity was defined as hypoechogenic. Autoimmune thyroiditis was assumed if a hypoechogenic echo pattern of both thyroid lobes was observed combined with a positive test for anti-TPO-Ab (16).
Statistical analysis
All calculations are weighted according to the age and gender distribution of the general German population and for nonresponse. Nonresponse weights accounted for loss to follow-up considering sociodemographic and health-related variables. For continuous variables, changes are described as median and interquartile range for each of the age and gender strata. For dichotomous variables, incidence rates per 1000 person-years (py) with 95% confidence intervals (CIs) are reported for each of the age and gender strata. All calculations were performed using STATA 11.0 (Stata Corporation).
Results
Between baseline and follow-up, the median iodine/creatinine ratio decreased slightly from 134.2 to 130.4 μg/g, indicating a stable iodine supply.
Self-reported thyroid disorders
Six subjects (three women) had missing values on self-reported disorders in SHIP-1. Among the rest, 459 individuals (15.6%, incident rate 29.6 [CI 27.2–32.4] per 1000 py) reported a new thyroid disorder or took antithyroid medication at follow-up. The incidence was higher among women (n=281, 19.9%, incident rate 37.5 [CI 33.7–41.8] per 1000 py) than among men (n=178, 11.7%, incident rate 22.1 [CI 19.1–25.6] per 1000 py). With the exception of the oldest decade, incident rates showed a clear increase over age (Table 1). Thyroid-related medication comprised thyroid hormones (n=114, 81 women, incident rate 10.4 [CI 8.7–12.6] per 1000 py), thyrostatic medication (n=17, 13 women, incident rate 1.4 [CI 0.9–2.6] per 1000 py), and iodine (n=17, 13 women, incident rate 1.4 [CI 0.9–2.5] per 1000 py).
Data are incidence rates per 1000 py [CI].
py, person-years; CI, 95% confidence interval.
With respect to thyroid disease subentities, most subjects reported newly diagnosed thyroid nodules (n=245, incident rate 15.7 [CI 13.9–17.8] per 1000 py). Newly diagnosed goiter was reported by 35 subjects (incident rate 2.4 [CI 1.7–3.5] per 1000 py). Regarding self-reported incident thyroid dysfunction, the incidences of hyperthyroidism (n=64, incident rate 4.4 [CI 3.4–5.7] per 1000 py) and hypothyroidism (n=68, incident rate 4.4 [CI 3.5–5.7] per 1000 py) were similar. At follow-up, 144 subjects (102 women) took thyroid-related medication, which they had not at baseline (incident rate 9.0 [CI 7.6–10.6] per 1000 py). Between baseline and follow-up, 25 subjects (13 women) underwent thyroid surgery (incident rate 1.6 [CI 1.1–2.5] per 1000 py), and 56 subjects (27 women) received radioiodine therapy (incident rate 3.7 [CI 2.8–4.9] per 1000 py). Those 187 subjects (122 women), who had received thyroid-related medication or underwent thyroid surgery or radio-iodine therapy after baseline, were excluded from all following analyses (Fig. 1).
Ultrasonography findings
Among the remaining 2754 subjects (1301 women), the mean change in the thyroid volume over 5 years was 0.73 mL [CI −1.68–3.41 mL]. The mean thyroid volume change did not differ between men (0.73 mL [CI −2.46–3.92 mL]) and women (0.76 mL [CI −1.16–2.83 mL]). In all age groups, there was a mean increase in thyroid volume, but lower CIs were always negative, indicating no significant thyroid growth over time (Fig. 2).
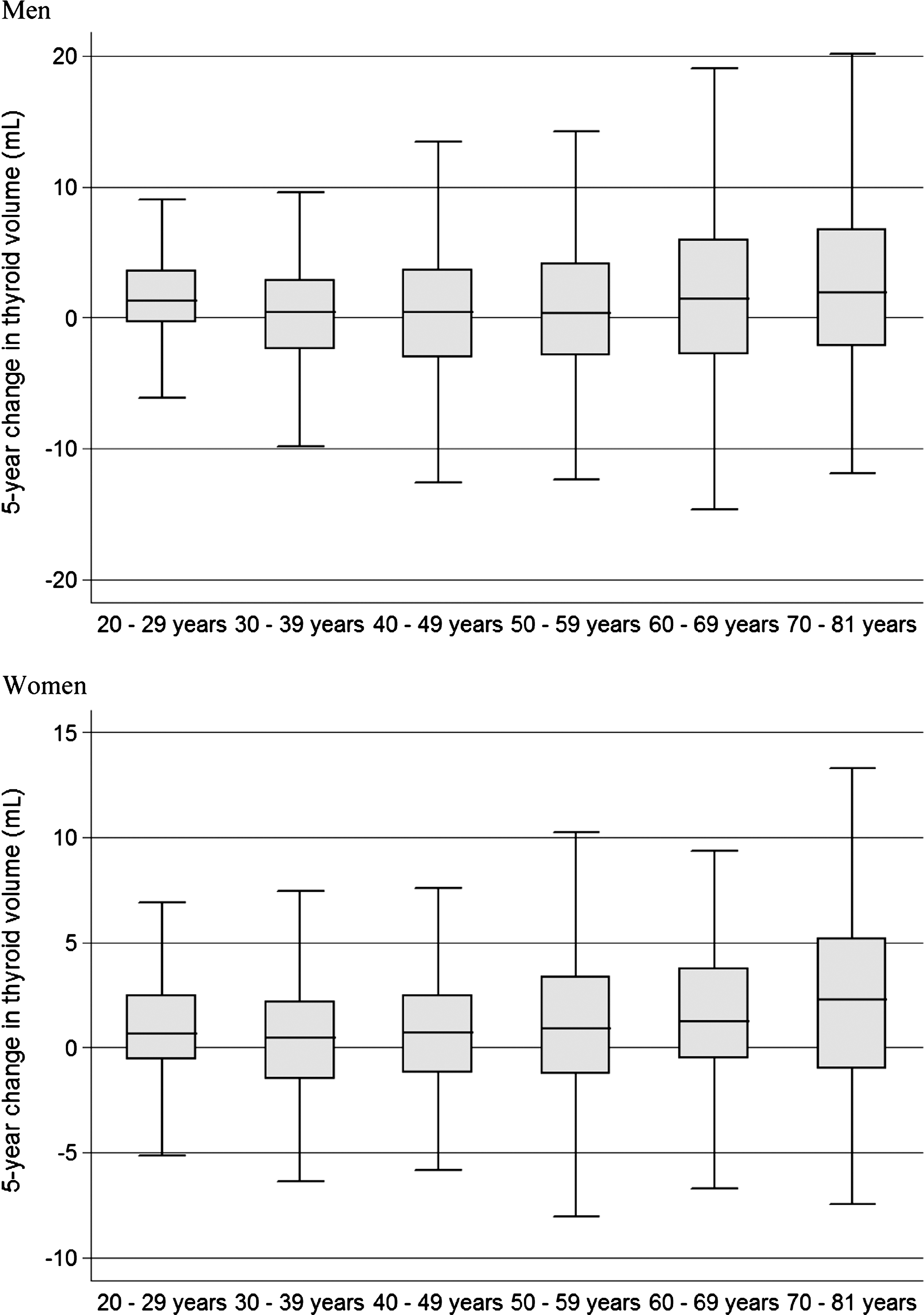
Change in the thyroid volume between baseline and 5-year follow-up examination in men and women displayed by box plots.
To calculate the goiter incidence, 960 subjects (415 women) with goiter at baseline were further excluded from analyses. Of the remaining 1794 subjects (886 women), 339 (18.0%, 173 women, incidence rate 34.0 [CI 30.7–37.7] per 1000 py) had a new sonographic finding of goiter. Incident rates were similar between men (32.3 [CI 27.9–37.6] per 1000 py) and women (35.7 [CI 31.1–41.1] per 1000 py). In both sexes, there was an age-related increase in goiter incidence (Table 2). Of those 960 subjects who had goiter at baseline, the thyroid volume of 199 subjects (20.7%, 87 women, normalization rate 40.2 [CI 35.5–45.9] per 1000 py) regressed to normal.
Data are incidence rates per 1000 py [CI].
All 478 subjects (253 women) with ultrasound diagnosis of thyroid nodules were excluded from analyses of nodule incidence (Fig. 1). Of the remaining 2277 subjects (1048 women), 209 (8.8%, 117 women, incident rate 16.6 [CI 14.5–19.1] per 1000 py) had incident sonographic evidence of thyroid nodules. Men (incident rate 13.5 [CI 11.0–16.9]) were less often affected than women (incident rate 20.1 [CI 16.9–24.1]). There was an age-related increase in the incidence of thyroid nodules (Table 2). Of those 478 subjects with thyroid nodules at baseline, 74 (15.5%, 35 women, normalization rate 30.5 [CI 24.7–38.8] per 1000 py) had no evident thyroid nodules in follow-up ultrasonography.
Thyroid function
There was a slight increase in median serum TSH levels (0.10 [CI −0.10–0.34] mIU/L), which was more pronounced in older age groups (Fig. 3). The median change in TSH was nearly identical in men (0.10 [CI −0.11–0.33] mIU/L) and women (0.10 [CI −0.10–0.35] mIU/L).
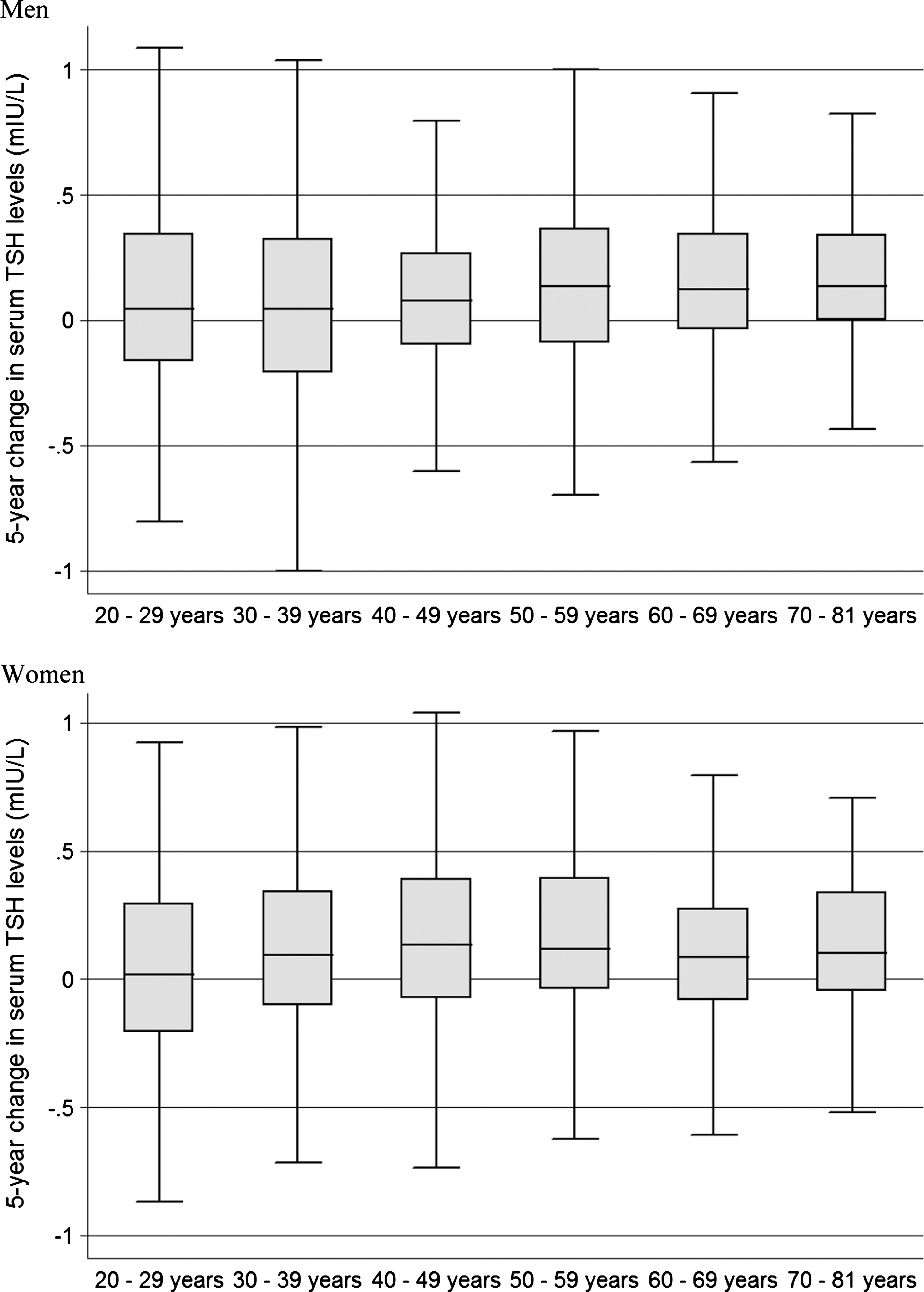
Change in serum thyrotropin levels between baseline and 5-year follow-up examination in men and women displayed by box plots.
To evaluate the incidence of serum TSH levels outside the reference range, all 234 subjects (104 women) who had serum TSH levels outside the reference range at baseline were excluded (Fig. 1). Of the remaining 2488 subjects (1176 women), 142 subjects reached the endpoint at follow-up (5.7%, 69 women, incidence rate 10.8 [CI 9.1–12.9] per 1000 py). The incidence was similar in men (incidence rate 10.6 [CI 8.4–13.6] per 1000 py) and women (incidence rate 11.0 [CI 8.7–14.2] per 1000 py) (Table 3). Of those 234 subjects (102 women) with serum TSH levels outside the reference range at baseline, the TSH regressed to normal in 78 subjects (33.3%, 30 women, normalization rate 126 [CI 114.3–139.2] per 1000 py).
Data are incidence rates per 1000 py [CI].
TSH, thyrotropin.
The incidence of increased serum TSH levels (incidence rate 6.6 [CI 5.3–8.3] per 1000 py) was higher than the incidence of decreased serum TSH levels (incidence rate 4.2 [CI 3.2–5.6] per 1000 py). There was the tendency toward higher incidence of thyroid dysfunction in older age groups with one exception: in women, hypothyroid forms of dysfunction occurred more often in middle-aged women. In both hypo- and hyperthyroidism, the subclinical forms occurred much more frequently than the overt ones (Table 3). One third of subjects with serum TSH levels outside the reference range at baseline reverted to normal at follow-up.
Anti-TPO-Abs and autoimmune thyroiditis
Subjects with increased and positive anti-TPO-Ab levels at baseline were excluded from the respective incidence analyses, yielding a study population of 2583 (1193 women) and 2661 (1231 women), respectively (Fig. 1). At follow-up, 73 subjects (4.0%, 46 women) had increased anti-TPO-Ab levels, and 46 subjects (1.8%, 32 women) had positive anti-TPO-Ab levels. The incidence of increased anti-TPO-Ab was 5.7 [CI 4.6–7.3] per 1000 py, and the incidence of positive anti-TPO-Ab was 3.4 [CI 2.6–4.7] per 1000 py. In both cases, women (incidence rate for increased levels 7.8 [CI 5.9–10.5], incidence rate for positive levels 5.2 [CI 3.7–7.5] per 1000 py) were more commonly affected than men (incidence rate for increased levels 3.9 [CI 2.7–6.0], incidence rate for positive levels 1.9 [CI 1.1–3.4] per 1000 py). With the exception of oldest men, the incidence was highest in younger and middle-aged adults (Table 4). Of those 166 subjects (106 women) with increased serum anti-TPO-Ab at baseline, 35 (21.1%, 20 women), and of those 88 subjects (68 women) with positive levels at baseline, 27 (30.7%, 23 women) reverted to normal levels at follow-up. The normalization rates for increased and positive anti-TPO-Ab levels were 38.3 [CI 27.9–54.0] and 57.2 [CI 41.4–81.0] per 1000 py, respectively. The normalization rate for increased anti-TPO-Ab levels was higher in males (49.2 [CI 30.2–86.7] per 1000 py) than in females (32.7 [CI 21.8–51.2] per 1000 py). In contrast, the normalization rate for positive anti-TPO-Ab levels was lower in males (38.9 [CI 16.3–118.5] per 1000 py) than in females (62.2 [CI 44.0–90.8] per 1000 py).
Data are incidence rates per 1000 py [CI].
TPO, thyroperoxidase.
The incidence of autoimmune thyroiditis was very low (incidence rate 0.7 [CI 0.4–1.4] per 1000 py). Only female patients developed autoimmune thyroiditis (Table 4). Of the 31 subjects (28 women) with autoimmune thyroiditis at baseline, 22 (71.0%, 20 women) had no such finding at follow-up (normalization rate 140.4 [CI 112.5–177.6] per 1000 py).
Discussion
This study is one of few reports from population-based longitudinal studies with comprehensive characterization of thyroid morphology and function. The interpretation of our findings has to consider the previous and current status of iodine supply of the population investigated: Since legislative changes in 1993, the study region has now become iodine sufficient. While the baseline SHIP-0 examinations were conducted during the transition period in the end of the 1990s, the follow-up SHIP-1 examinations were performed 10 years after the introduction of the iodine fortification program. The current data on median urinary iodine excretion confirm previous studies (5,6), indicating a stable iodine status of the German population.
The high incidence of known thyroid disorders has to be interpreted with caution, because information on all thyroid-related findings from baseline SHIP-0 examinations was provided to the participants. For example, the prevalence of thyroid nodules was 20.2% at baseline (6), and all participants with thyroid nodules were advised to visit GPs or endocrinologists for further monitoring or diagnostic work-up. Therefore, the high incidence of known thyroid nodules is not surprising and cannot necessarily be related to the incidence of newly diagnosed nodules, which became symptomatic or incidentally detected over the previous 5 years.
While the incidence of known thyroid disorders increased over age, in general, it was relatively low in subjects over 70 years. This decline in the oldest age group appears to be counterintuitive, but may be explained by higher mortality in patients with thyroid diseases and co-morbidities as well as recall bias in elderly subjects. Although we weighted our analysis for nonresponse and offered home visits to older and immobile subjects (9), we cannot fully rule out that a substantially higher proportion of patients with thyroid disorders and additional co-morbidities were among the respondents than the nonresponse weights could have accounted for (8). Consequently, we may have underestimated the incidence of known thyroid disorders among the elderly. On the other hand, younger individuals may be screened for thyroid disorders more intensively compared to older individuals, which would result in a lower detection rate of thyroid disorders in the latter ones. This is supported by a study demonstrating that younger patients with hypothyroidism were more likely to be referred to hospitals than older patients (17).
Because cohort studies like the present are mainly based on self-reported history of diseases, they very likely misestimate the real incidence of clinically relevant thyroid disorders compared to registry studies (18). Our study, however, provides valuable information on the change in subclinical alterations of the thyroid gland as defined from ultrasonography and laboratory analyses in subjects without known thyroid disorders. In men and women, there was a modest increase in thyroid volume, which was stronger in elder than in younger subjects. Given the formerly high presence of goiter, which at baseline reached a prevalence of >40% in middle-aged and older subjects (6), only a modest progression in thyroid volumes during follow-up argues for a sufficient iodine supply of the general population. The cumulative incidence of goiter in our study was 18% and therefore higher than in a Chinese population with mildly deficient iodine intake (2). However, 20.7% of our subjects with goiter at baseline had no goiter at follow-up. Thus, there is a tendency toward a negative balance between newly occurring and spontaneously regressing goiter in our population, which also argues for a sufficient iodine intake.
The 20-year follow-up of the Wickham Survey (3) demonstrated conflicting results with respect to goiter prevalence. While the prevalence at baseline was 23% in women and 5% in men, it declined to 10% in women and 2% in men at follow-up. These findings might be attributed to an improved iodine supply of the investigated population, but may also be explained by methodology for defining goiter, which was based on palpability and visibility. While the Wickham Survey put much effort into standardization of the examination procedure in each wave, it cannot be unequivocally ruled out that bias in the clinical determination of goiter might have been occurred between baseline and follow-up, particularly considering the long period of two decades between the two examinations.
Similarly to goiter incidence, the incidence of thyroid nodules was also higher in SHIP than in the Chinese population (2). However, there was clearly a negative balance between newly detected nodules and nodules that were present at baseline, but regressed during follow-up. The higher nodule incidence in women than in men is concordant with a number of cross-sectional studies, which demonstrated similar sex differences (6,19,20). Unfortunately, our study protocol did not include detailed assessments of the nodules as in other studies (21); therefore, we were not able to assess the natural course in terms of size and echo pattern of individual nodules.
From baseline to follow-up, the distribution of serum TSH levels somewhat shifted toward to the right, which might best be explained by the history of iodine supply in the investigated population. The introduction of iodine fortification programs gives rise to a transient decline of mean serum TSH levels in populations and, consequently, to an increased prevalence and incidence of low serum TSH levels and hyperthyroidism over the next few years (22,23). For baseline SHIP-0, data were collected during this transition phase, and mean serum TSH levels were therefore comparably low in the prevalence study (6,10). Data collection for SHIP-1 was performed after the transition phase; in good agreement with other studies (24), not only did serum TSH levels increase, but also the incidence rate of increased serum TSH levels increased somewhat. The high normalization rate of 33.3% in subjects with serum TSH levels outside the reference range may be interpreted as cumulative effects from biological variation of serum TSH levels (25), measurement errors of laboratory methods leading to regression to the mean (26), changes in population means by optimized iodine supply, and spontaneous reversion to normal.
Compared to other studies (27), the TSH reference interval used herein to define thyroid dysfunction is relatively low and narrow (10). As recently discussed in detail, reference intervals are always population specific and, in case of thyroid function tests, mainly depend on the iodine supply of the population (28). When defining the incidence of thyroid dysfunction using these reference intervals, the incidence rates are consequently also population specific, which limit the comparability of incidence estimates from different population-based studies. Likewise, the distribution of serum values for thyroid function tests may vary across studies due to different laboratory methods. Hence, population studies on thyroid disorders like ours should put more efforts in improving standardization and external validity to enhance the comparability of their results.
In general, the incidence of autoimmune findings was low, but showed—as also for incident high serum TSH levels—clear female predominance, as repeatedly found in other studies (2,3). In addition, a high proportion of subjects with increased or positive anti-TPO-Ab levels reverted to normal during follow-up. For subjects with features of autoimmune thyroiditis at baseline, nearly three out of four did not have such a finding at follow-up. These findings are in concordance with the concept that the current iodine supply does not substantially increase the risk of autoimmune thyroid changes in the general German population.
We conclude that in the Northeast German population, which had lived under mildly to moderately iodine-deficient conditions until the mid-1990s, there is only a modest mean thyroid growth and a negative net balance between occurring and reverting goiter and thyroid nodules. These findings, along with the balanced incidences of hyper- and hypothyroid dysfunction and the low incidence of autoimmune-related thyroid findings, indicate that the current iodine status is sufficient to protect an adult population from iodine deficiency-related disorders on the one hand, and to not substantially increase the risk of autoimmune thyroid disease on the other hand.
Footnotes
Acknowledgments
The work is part of the Community Medicine Research net (CMR) of the University of Greifswald, Germany, which is funded by the Federal Ministry of Education and Research (BMBF 01ZZ9603 & 01ZZ0103), the Ministry of Cultural Affairs, as well as the Social Ministry of the Federal State of Mecklenburg-West Pomerania. The CMR encompasses several research projects that share data from the population-based SHIP (
Disclosure Statement
No conflicts of interests are stated.