
Abstract
Background:
Whether the prevalence of thyroid cancer is different in thyroid glands with a single nodule (SN) versus multinodular goiter (MNG) remains uncertain. Therefore, a meta-analysis was performed to evaluate the extant literature on the comparative prevalence of thyroid cancer in SN compared with MNG.
Methods:
We searched MEDLINE, EMBASE, Scopus, Cochrane Central, and reference list for selected observational, cross-sectional, and longitudinal studies evaluating thyroid cancer in SN and MNG. Toxic nodules were not included in the analysis. Two reviewers working independently extracted descriptive, methodological and outcome data from each study with consensus resolution of discrepancies. Meta-analytic estimates of treatment effects were generated using a random-effect model.
Results:
Fourteen studies encompassing 23565 patients with MNG and 20723 patients with SN were eligible for inclusion. Most eligible studies were at a moderate risk of bias. MNGs were associated with a lower risk of thyroid cancer than SN (pooled odds ratio 0.8 [95% confidence interval 0.67–0.96]; I 2=35%). Subgroup analysis suggested that this difference depends on the inclusion of studies conducted outside the United States (odds ratio 0.71 [95% confidence interval 0.60–0.83]; I 2=11%).
Conclusions:
Thyroid cancer may be less frequent in MNG compared to SN, particularly outside the United States and perhaps in iodine-deficient areas.
Introduction
The prevalence of malignancy in SN has been estimated at 5% (5,6). Recent guidelines for the management of thyroid nodules make recommendations for evaluation based on the assumption of a comparable risk of thyroid cancer in SN as in MNG (7). Individual studies, however, provide cancer prevalence in patients with MNG that are lower (4.1%) (8) or higher (18%) (9) than those reported for patients with SN.
These differences in thyroid cancer risk might impact recommendations and practice. Therefore, this systematic review aims to summarize the available comparative prevalence of adults with single or multiple thyroid nodules undergoing evaluation with fine-needle aspiration or surgery and to explore the reasons for differing prevalence estimates across studies.
Methods
This systematic review is reported in accordance with the PRISMA (preferred reporting items for systematic reviews and meta-analyses) statement (10).
Study eligibility
We searched for full publications in Spanish or English of longitudinal and cross-sectional observational studies that included adults (≥18 years of age) with diagnoses of MNG or single thyroid nodule by thyroid ultrasound who underwent either fine-needle aspiration biopsy (FNA) of a thyroid nodule or surgical intervention with a pathological specimen. Malignant, suspicious, or indeterminate nodules by FNA required histopathological diagnosis. Toxic nodules were not included in the analysis.
Data sources and search strategies
We searched PubMed MEDLINE, Ovid Medline In-Process & Other Non-Indexed Citations, Ovid MEDLINE, Ovid EMBASE, Ovid Cochrane Database of Systematic Reviews, Ovid Cochrane Central Register of Controlled Trials, and Scopus from inception until July 2011. Additionally, and to ensure a comprehensive literature search, we examined reference lists from retrieved articles.
A reference librarian (L.J.P.) experienced in searches for systematic review designed the search strategy with input from the study's investigator (J.P.B.). The search strategy used controlled vocabulary supplemented with keywords describing the following concepts: thyroid cancer, solitary thyroid nodule, and MNG. The full search strategy is presented in the appendix.
Study selection
Two reviewers (J.P.B. and A.J.Y.) performed first-stage screening of titles and abstracts based on the research question and study design with a substantial chance-adjusted inter-rater agreement (kappa statistic=0.8 [95% confidence interval (CI) 0.68–0.92]. We retrieved articles based on the initial screening in full text for second-stage screening. Chance-adjusted inter-rater agreement for this stage was also substantial (kappa statistic=0.81 [CI 0.61–1.01]), and discrepancies were resolved by discussion.
Data extraction
For each eligible study, one reviewer (J.P.B.) extracted the following data items: total number of patients, thyroid gland ultrasound, age, sex, country in which the study was conducted, diagnostic method (FNA vs. surgery), exposure to radiation (yes/no), family history of cancer (yes/no), obstructive symptoms (yes/no), diagnoses of hyperthyroidism (yes/no), indication for surgery, histopathology, or/and cytology results. A second reviewer verified the data extracted against the full-text publications (A.J.Y.).
Additionally, studies were classified according to the iodine status. This information was inferred from the country where the study was conducted and, according to the World Health Organization (11), used a threshold of median urinary iodine excretion of 788 nM (100 μg/L) for iodine sufficiency.
Quality assessment
Two reviewers working independently (J.P.B. and A.J.Y.) assessed the methodological quality of included observational studies using the Newcastle-Ottawa Scale (12). This instrument assesses the protection against bias afforded by the manner in which the investigators selected patients (4 criteria), ensured the comparability of study groups (1 criterion), and measured outcomes (3 criteria).
Data synthesis
To assess for heterogeneity across studies, we used the Cochran Q chi-square statistic (significance level set at p<0.10). To quantify inconsistency, we estimated the I 2 statistic, which quantifies the proportion of observed differences in estimates across studies not attributable to chance: I 2>50% indicates a large inconsistency. Because there are too few studies and there was substantial inconsistency in results, we could not assess publication bias by statistical or visual analyses of funnel plots.
To conduct the meta-analysis, we used Review Manager (Revman) (13). For our main analysis, we categorized the data by the diagnostic method and type of nodular goiter. We used DerSimonian and Laird random-effect models to calculate the pooled odds ratio (OR) and its CIs.
Subgroup analyses
We tested for the interaction (14) between the association of thyroid cancer and MNG versus SN and the following study-level covariates: history of radiation, family history of thyroid cancer, diagnostic method (cytology vs. surgical pathology), country where the study was conducted (United States vs. elsewhere), sex, prevalence of endemic goiters where the study was conducted (endemic vs. no endemic), and the study design (cohort vs. cross-sectional).
Results
Included studies
We deemed 14 studies published between 1987 and 2010 eligible for this review (Fig. 1) (4,15 –27). These studies enrolled 20,723 patients in the SN group and 23,565 in the MNG group (Table 1). The mean age was 49 and 46 years old in patients with SN and MNG, respectively. Five studies documented the indications for surgery, which included compression symptoms or suspicion of malignancy. Only one study documented family history of cancer, and no study reported prior radiation exposure. The most common thyroid cancer in both groups was papillary thyroid cancer, followed by follicular thyroid cancer.
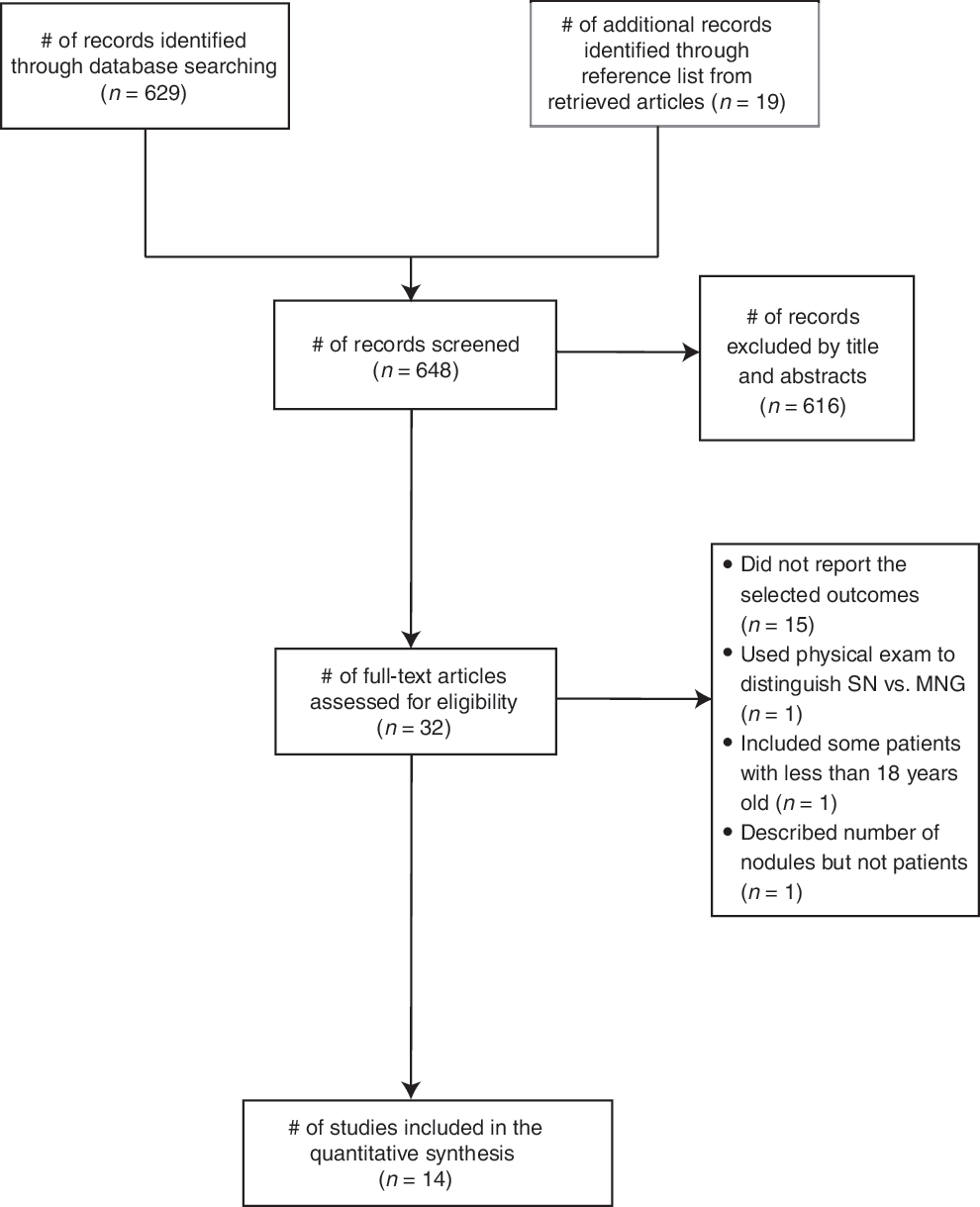
Study selection process.
Dx, diagnostic; nod., nodularity; TC, thyroid cancer; PTC, papillary thyroid cancer; FNA, fine-needle aspiration; MNG, multinodular goiter; SN, single nodule; nr, not reported.
Methodological quality
Table 2 summarizes the reported methodological quality of the included observational studies. Chance-adjusted inter-rater agreement was substantial (K=0.75 [CI 0.65–0.85]); disagreements were resolved by consensus. Limitations in the ascertainment of exposures associated with a higher risk of thyroid cancer, and comparability of MNG and SN cohorts on the basis of age and sex reduced the quality of the evidence and increased the likelihood of bias.
RL, record linkage.
Meta-analysis main analysis
Fourteen studies were included in this analysis (Table 3). The risk of thyroid cancer was significantly lower in the MNG than in the SN group (OR 0.8 [CI 0.67–0.96]), with moderate inconsistency across studies (I 2=35%).
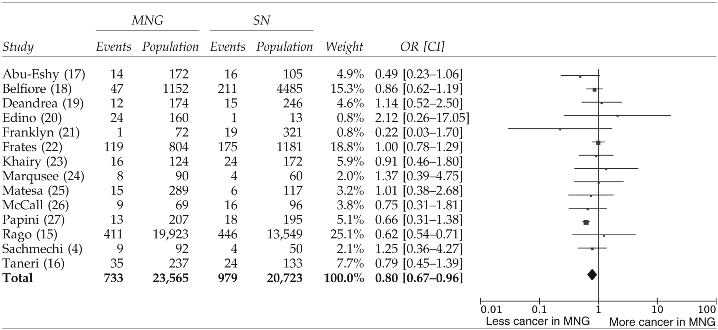
Heterogeneity: τ2 = 0.03; χ2 = 19.86; df = 13 (p = 0.10); I 2 = 35%. Test for overall effect: Z = 2.37 (p = 0.02). Odds ratio (OR): M–H, random. Vertical lines indicate no risk difference; squares and horizontal lines indicate ORs and associated 95% confidence intervals (CIs) for each study; diamond indicates pooled OR.
Meta-analysis subgroup analysis
We found insufficient data to conduct subgroup analyses by family history of thyroid cancer and radiation exposure. We found two interactions of potential importance (Table 4). The first one is by country. While non-U.S. studies were consistent with the result of our main analysis, U.S. studies differed importantly indicating no significant difference in the odds of thyroid cancer in MNG versus SN (OR 1.00 [CI 0.79–1.26], I 2=0%; p interaction=0.002). Nevertheless, there was no difference in the thyroid cancer prevalence between studies conducted in the United States versus Italy (OR 0.83 [CI 0.65–1.05], I 2=55%; p interaction=0.12). The second interaction of interest may partially explain this association, in so far as studies in iodine-sufficient areas also found no association between the type of goiter and risk of cancer, while studies in iodine-deficient areas were consistent with the result of our main analysis (p interaction=0.05).
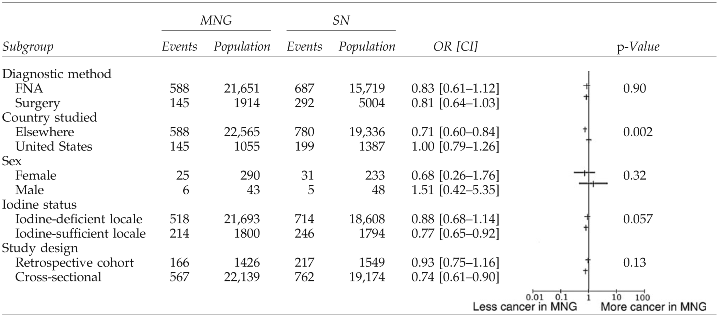
OR: SE IV, random. Subgroup analysis was conducted by evaluating the influence of variables on the prevalence of thyroid cancer (e.g., studies in which FNA biopsy was used as diagnostic method of thyroid cancer). Random-effect values <1.00 favor less cancer in MNGs. Large vertical line indicates no risk difference; small vertical line and horizontal lines indicate OR and associated 95% CI for each study.
Sensitivity analysis
We performed one-way sensitivity analysis to evaluate the robustness of the study. Removal of the Rago study (15) decreased precision of estimates and inconsistency of results, but the pooled findings are essentially unchanged: ORRago− 0.90 [CI 0.77–1.05], I 2=0%).
Discussion
We conducted a systematic review on the comparative prevalence of thyroid cancer in patients with MNG or SN. We found 14 studies at moderate risk of bias. Taken together, these studies supported the inference that thyroid cancer is less frequent in MNG than in SN, although this inference appears to hold true mostly outside the United States, in iodine-deficient populations.
Limitations and strengths
Several limitations weaken the inferences we can draw in this review. We were unable to obtain data on the U.S. Office of Management and Budget race/ethnicity categories of the participants, size of the nodules, ultrasound nodule characteristics, thyrotropin values, prior FNA results, lymph node involvement, and staging of the thyroid cancers. These data could contribute to an individual patient data meta-analysis, not within the scope of this project. Only a few studies described having excluded patients with known thyroid cancer risk factors (radiation and family history), and others included patients with this risk factor without any adjustment.
The studies did not specify the criterion for selection of nodules for FNA in patients with MNG (i.e., whether all nodules above a certain size, dominant nodules, or suspicious nodules only were biopsied). If only the dominant or largest nodule was sampled, thyroid cancer could have been missed, a potential unexplored explanation for the lower prevalence of thyroid cancer in those studies finding a lower risk in patients with MNG than in patients with SN. Likewise, diagnosis of benign nodules ascertained by FNA and not removed by surgery did not have any follow-up period. This brings uncertainty about the absence of confirmation of a negative diagnosis.
Importantly, the difference between U.S. studies and non-U.S. studies might be a reflection of practice variation in the assessment of MNG. Current Clinical guidelines from Latin America, North America, and Europe (28 –30) recommend that cytology sampling should be focused on lesions with suspicious U.S. features; however, FNA from the dominant nodule was the common practice few years ago as demonstrated in two survey studies in Europe and the United States. Variation in the application of changes in the recommendation may be an important confounder not accounted in this meta-analysis that could explain heterogeneity of the results.
Additionally, this study also shows that the prevalence of cancer using FNA is no different from the prevalence of cancer based on surgical pathology; this could be due, however, to cancer enrichment in the FNA group (given the disposition to target suspicious nodules and avoid benign-appearing ones) and dilution in surgical MNG specimens obtained, for instance, after surgery to alleviate compression symptoms.
Although we conducted a comprehensive search, some relevant studies that were not in the referenced databases might be missing in our analysis. We could not explore publication bias due to the moderate between-study heterogeneity and the small number of studies.
The strengths of this review stem from the extensive literature search, reproducible judgments about inclusion and methodological quality, duplicate judgments and data collection, and preplanned and parsimonious analyses, including predefined subgroup analyses.
Implication for practice and for further research
To our knowledge, this is the first meta-analysis to address the comparative prevalence of thyroid cancer in MNG and SN. Our results do not require any change in extant recommendations for the management of MNG and SN; ultrasound should be the main tool to assess the dominant nodule and the ones with a worrisome sonographic appearance (suspicious features and change of size), in SN and MNG, as possible targets for FNA.
Future studies should be conducted to clarify the clinical relevance and prognostic significance of thyroid carcinomas in MNG, especially papillary microcarcinomas and their relation with goitrogenesis in areas of iodine sufficiency.
Conclusion
Low-quality evidence suggests that thyroid cancer is less frequent in MNG than in SN, particularly outside the United States and perhaps in iodine-deficient areas.
Footnotes
Acknowledgment
Mayo Clinic Foundation for Medical Education and Research: this funding source had no role in the design, conduct, or decision to publish this study.
Disclosure Statement
The authors declare that no competing financial interests exist.