
Abstract
Background:
Fine-needle aspiration (FNA) is the most accurate and cost-effective method for evaluating thyroid nodules. However, FNA-induced secondary changes completely replacing thyroid tumors (vanishing tumors) may create a novel problem. In this study, we highlight the diagnostic and management issues associated with the unintended consequences of ultrasonography (US)-guided FNA.
Methods:
Fourteen thyroid glands (11 women and 3 men, ages 33–64 years) with vanishing tumors were prospectively identified between 2009 and 2012 upon surgical resection. Cytology and histopathology slides were reviewed, and second opinions were obtained when necessary.
Results:
The cytology of the 14 vanishing tumors was suspicious/positive for papillary thyroid carcinoma (PTC) in 5, indeterminate (atypia of unknown significance) in 5, benign in 2, follicular neoplasm in 1, and nondiagnostic in 1 nodule. Upon thyroidectomy, the vanishing tumors ranged in size from 0.4 to 3.5 cm (median 0.7 cm). Microscopically, the nodules showed cystic degeneration, organizing hemorrhage, granulation tissue, fibrosis, and microcalcifications. In seven tumors, a few residual malignant cells (PTC in five) or residual benign follicles (hemorrhagic cyst in two) at the periphery of the vanishing tumors helped with the final diagnosis. The remaining seven tumors were completely replaced by FNA-induced secondary changes, and had the cytology diagnosis of benign in one, follicular neoplasm in one, and suspicious/positive for PTC in five. Of the latter five, two showed additional separate foci of PTC, while three vanishing tumors (0.5, 1.2, and 1.6 cm) had no residual malignant cells and no additional carcinoma leading to a final diagnosis of negative for malignancy.
Conclusions:
US-guided FNA may lead to complete obliteration of thyroid nodules, rendering final diagnosis upon thyroidectomy difficult or impossible. In these unusual circumstances, the possibility that the surgical pathology may be nonrepresentative should be considered if the cytologic features on FNA are sufficient by themselves to support a definitive diagnosis of PTC.
Introduction
However, FNA-induced reactive changes in thyroid nodules can be worrisome (6 –9) and include atypical nuclei, hemorrhage, infarction, fibrinoid necrosis, fibrosis, cystic degeneration, pseudocapsular invasion, and squamous metaplasia. Rarely, these changes completely or extensively replace a thyroid nodule, so as to render the final surgical pathology diagnosis on thyroidectomy difficult or impossible (vanishing tumors). Should the surgical pathology diagnosis of negative for malignancy rendered in the absence of any residual malignant cells be considered final when the FNA cytology is unequivocally malignant? Here we discuss the management dilemma encountered with these vanishing tumors.
Methods
We defined vanishing tumors as thyroid nodules with at least one FNA before surgery that upon resection showed complete or near-complete replacement by reactive changes with no or minimal residual malignant or benign thyroid follicles. Cases were prospectively identified on thyroidectomies performed between July 2009 and January 2012. All FNAs were performed under US guidance using a 25-gauge needle with two to three passes. All thyroids were entirely submitted for microscopy, and all vanishing tumors were further examined at multiple levels until they were finished (consumed, cut through). When multiple nodules were present within the thyroid, all nodules with worrisome features at the initial section were leveled (at least three levels) until a definitive diagnosis was reached. The cytology slides were sent to an expert endocrine cytopathologist (Z.B.) blinded to the surgical pathology findings, and the histopathology slides were sent to an expert endocrine pathologist (A.K.) blinded to the cytopathology diagnosis to remove any bias. FNA-induced changes were differentiated from spontaneous degenerative changes as follows: (i) reactive changes tended to be in a linear needle-track-like distribution in the former, and irregular, usually associated with larger nodules in the latter; (ii) FNA in the specific nodule was confirmed by the ultrasonographers' drawings designating the sampled nodule (Supplementary Fig. S1; Supplementary Data are available online at
BRAF V600E mutation on four vanishing tumors was analyzed by single-strand conformational polymorphism after extraction of DNA from the needle rinse, and the BRAF V600E region was amplified by PCR, as described elsewhere (10).
Results
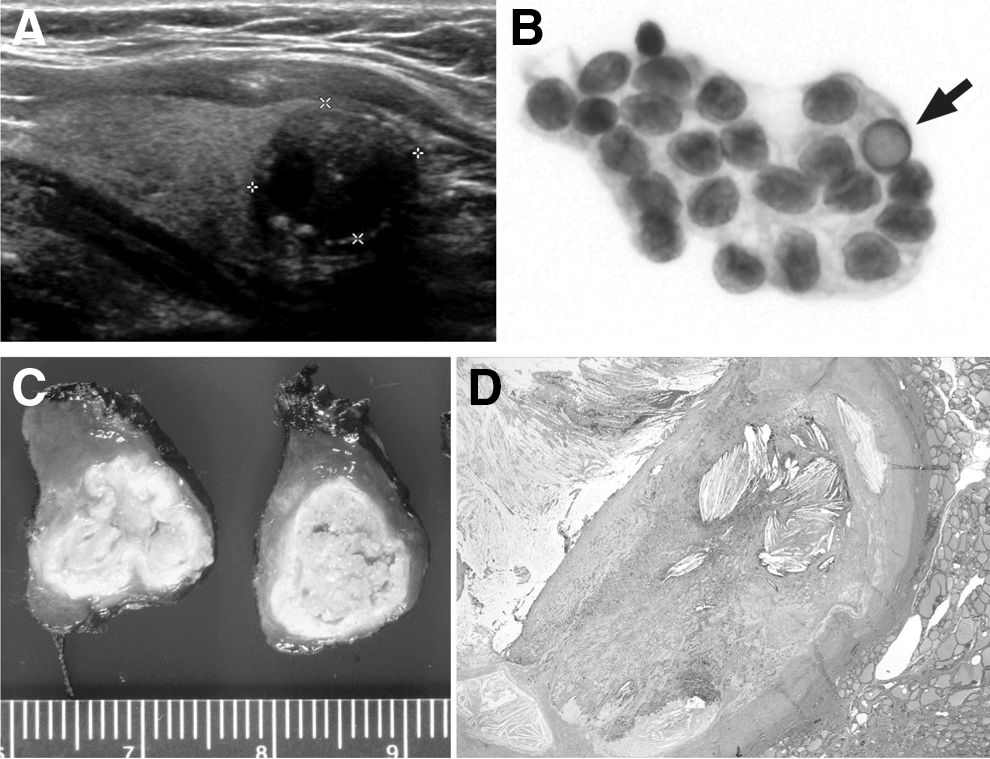
Fourteen thyroids (lobectomy 4 and total thyroidectomy 10 [5 with and 5 without central neck dissection]) with vanishing tumors were identified among 1516 thyroid resections (0.9%). The patients were aged 33–68 years (11 women and 3 men). The most common presentation was thyroid nodule. The relevant clinicopathological and US findings are shown in Figure 1 and Table 1.
In case of multiple nodules, the vanishing tumor is highlighted in bold.
Number of times (and when) FNA was performed, initial diagnosis (Dx), and second opinion.
Second opinion from our institution (initially diagnosed at the referring institution).
AUS, atypia of undetermined significance; F, female; FNA fine-needle aspiration; M, male; PTC papillary thyroid carcinoma.
The FNA diagnosis was suspicious (n=3) or positive (n=2) for papillary thyroid carcinoma (PTC) in 5, follicular neoplasm in 1, indeterminate (atypia of unknown significance [AUS]) in 5, benign in 2, and nondiagnostic in 1 vanishing tumor. Upon second opinion (cases 1–6, and 14), an indeterminate (AUS) cytology was upgraded to suspicious (case 6), and suspicious was changed to positive for PTC (cases 2 and 5). In four cases, multiple FNAs were performed on the same nodule. The FNA needle rinse tested positive (cases 11 and 13) and negative (cases 7 and 12) for BRAF V600E mutation in 2 cases each.
The vanishing tumors ranged from 0.4 to 3.5 cm (median 0.7 cm) in size. A decrease of 0.1–0.7 cm was noted compared to the size measured by US. The nodules showed variable degrees of cystic change, organizing hemorrhage with hemosiderin pigment-laden macrophages, granulation tissue, fibrosis, sclerosis, and microcalcifications in all vanishing tumors in proportion to the temporal relationship of FNA to surgery (Fig. 1C, D). Acute and chronic inflammatory cells, including eosinophils, foamy macrophages, cholesterol granulomas with multinucleated giant cells, and squamous metaplasia frequently lining the cyst, were seen. Two vanishing tumors showed focal ossification.
Seven tumors (cases 2–6, 13, and 14) were completely replaced by reactive changes. These included 3 tumors considered suspicious/positive for PTC on FNA (cases 2, 5, and 6), but negative for malignancy on surgical pathology, one with indeterminate/benign FNA (case 4), one with indeterminate (AUS), but BRAF V600E-positive FNA (case 13) that also had multifocal PTC, one with benign (case 3), and one with Hürthle cell/follicular neoplasm (case 14) on FNA. PTC was diagnosed in five tumors (cases 7, 9–12), based on a few residual malignant cells at the periphery of the vanishing tumors of which three (cases 7, 9, and 10) had multifocal PTC. Cases 1 and 8 had a few residual benign thyroid follicles in the wall of the hemorrhagic cyst.
Discussion
Inability to find malignancy on thyroid resections is typically documented in the final pathology report as negative for malignancy. We demonstrate that the final diagnosis may be compromised when no representative follicular cells remain in a suspicious nodule that is completely replaced by secondary reactive changes after single or repeated US-guided FNA. Certain patterns emerged among the vanishing tumors. Five of the nodules were ≤1 cm, the smallest being 0.5 cm by US. Four nodules ranging in size from 1 to 2 cm were subjected to multiple FNA before surgery. FNA-induced hemorrhage completely obliterated a large 3.9-cm thyroid nodule in a patient on warfarin (case 1). One nodule was likely a Hürthle cell neoplasm (case 14), which are known to undergo infarction or ischemic necrosis when subjected to FNA. We considered two hypotheses regarding the vanishing tumors: (i) the cytology may have been false positive, or (ii) the surgical pathology may be false negative. The value of second opinion in cytopathology is well established. Second opinions in cytopathology may change management in 13% to 30% of cases (11,12). Multiple reviews and expert consultations suggest that the FNA diagnosis was not false positive, and therefore at least three patients in our series (cases 2, 5, and 6) may have had 0.5-cm (pT1a), 1.2-cm and 1.6-cm (pT1b) PTC. Thus, the final surgical pathology diagnosis of negative for malignancy indicates nonrepresentation of the original tumor rather than true negative.
The vanishing-cancer phenomenon has been described in prostates where minute cancers identified on biopsies disappeared on radical prostatectomies (13). Unlike prostate, where a final diagnosis of cancer is rendered on a needle core biopsy, the Bethesda system of reporting thyroid FNA implies cancer risk varying from 1–4% in the nondiagnostic category to 97–99% in the positive for malignancy category (14). Thus, the final confirmation of malignancy is made on surgical pathology. This general wisdom may be open to question in the rare event of vanishing tumor. Furthermore, a reduction in the size of the vanishing tumors after US-guided FNA could potentially lead to understaging of malignant tumors. There is significant distress and morbidity associated with total thyroidectomy for a BRAF V600E mutation-positive thyroid carcinoma diagnosed on FNA that is finally deemed negative for malignancy. By reporting our experience, we hope to raise awareness to these unexpected events. Currently, there are no consensus guidelines for the management of vanishing tumors. In a recent publication, Marchetti et al. macrodissected tumor cells from the FNA cytology slides and performed BRAF mutational analysis that helped improve their suspicious diagnosis to definite for carcinoma by 37% (15). A search for conclusive evidence of malignancy on FNA cytology may need to be undertaken when no residual tumor cells remain in a thyroid nodule.
This observational study has several limitations, the absence of follow-up being one. The issue of mixed identity or mixed specimens was not explored due to technical reasons. We are also unable to comment on the incidence of vanishing tumors after US-guided FNA, since only a subset of the thyroids subjected to FNA undergoes thyroidectomy. However, we noted a prevalence of <1% among all thyroid resections performed during the same period for various reasons.
In conclusion, vanishing tumors of the thyroid may be an unintended consequence of US-guided FNA. With wider acceptance of high-resolution US and US-guided FNA for thyroid nodules, there may be an increase in their incidence leading to diagnostic and management dilemmas.
Footnotes
Acknowledgments
The funding for this work is provided by the Doris Duke Charitable Foundation and the Yale Office of Student Research.
Disclosure Statement
The authors have no competing financial interests.