
Abstract
Background:
Multiple studies have demonstrated successful radioactive iodine remnant ablation (RRA) following preparation with recombinant human thyroid stimulating hormone (rhTSH). Short-term studies in relatively low-risk patients have also suggested that rhTSH-stimulated RRA can have an effective adjuvant therapy function in destroying residual microscopic thyroid cancer cells. However, very few of these studies have included a significant number of intermediate or high-risk patients. The goal of this study was to examine clinical outcomes after rhTSH stimulated RRA in a larger cohort of thyroid cancer patients at higher risk of recurrence and disease-specific mortality.
Methods:
A retrospective chart review identified 586 thyroid cancer patients prepared for RRA with either a thyroid hormone withdrawal (THW) (n=321) or rhTSH preparation (n=265). The primary end points included both the best response to initial therapy and the clinical status at final follow-up. Clinical outcomes were compared within each of the American Thyroid Association (ATA) risk groups (low, intermediate, and high) and American Joint Committee on Cancer (AJCC) stages (I–IV) based on the method of preparation for RRA (THW vs. rhTSH).
Results:
Preparation with rhTSH was more likely to be associated with an excellent response to therapy (39.4% for rhTSH vs. 30% for TWH, p=0.03) and fewer additional therapies (29% for rhTSH vs. 37% for TWH, p=0.05) than THW. However, after a median follow-up period of 9 years, the final clinical outcomes were not significantly different with respect to recurrence rates (1.5% for rhTSH vs. 1.2% for TWH), likelihood of having persistent disease (46% for rhTSH vs. 48% for THW) or likelihood of having no evidence of disease (53% for rhTSH vs. 52% for TWH). Furthermore, clinical outcomes were similar between rhTSH and THW preparation across all ATA risk groups and AJCC stages.
Conclusions:
rhTSH preparation for RRA is associated with a small, but statistically significant improvement in an initial response to therapy and similar final clinical outcomes across a wide range of risk of recurrence and risk of disease-specific mortality. These data suggest that rhTSH preparation for RRA can be effectively used in intermediate and high-risk patients without known distant metastases.
Introduction
While these data showing similar short-term clinical outcomes with either rhTSH preparation or THW are encouraging, it is important to recognize that most (1 –6,8,9,11,13,19), but not all (14,15,18), of these early studies involved predominantly low-risk thyroid cancer patients. Furthermore, only four publications have reported clinical outcomes beyond the one-year time point (12,15,17,20). And finally, the results of these previous studies have generally been presented as clinical outcomes for the entire cohort without having an adequate sample size to allow a subgroup analysis of specific higher risk groups undergoing radioactive iodine remnant ablation (RRA).
In an effort to address some of these important issues, we previously published the clinical outcomes in a cohort of 394 thyroid cancer patients followed for a median of 2.5 years (15). This was a relatively high-risk cohort with nearly 50% of the patients having N1 disease and nearly 30% with the American Joint Committee on Cancer (AJCC) stage III or IV. For the entire cohort, recurrence rates were very similar in the 320 patients prepared for ablation with rhTSH, and the 74 patients prepared for RRA with THW (4% rhTSH vs. 7% THW). In a subsequent post hoc subgroup analysis, we reported very similar rates of recurrence in patients with N1 disease (n=194, 13% THW vs. 6% rhTSH), T3/T4 disease (n=203, 10% THW vs. 6% rhTSH), or T3N1 disease (n=108, 18% THW vs. 8% rhTSH) (18). Recently, in a letter to the editor, Rosario et al. reported very similar findings in a cohort of 276 differentiated thyroid cancer patients at relatively high risk of recurrence (T3 or N1 disease was present in 54% of the rhTSH cohort and 56% of the THW cohort) (12). Recurrence rates after a median of 5 years of follow-up were 5.2% (4/79 patients) following rhTSH preparation and 4.2% (8/197) following THW.
In this article, we extend our initial observations (15,18) by describing both short-term (2 years) and-long term (9 years) clinical outcomes following preparation for RAI remnant ablation with either rhTSH or THW across a wide spectrum of recurrence risk (ATA low, intermediate, and high risk) and disease-specific mortality risk (AJCC stage I, II, III, and IV). The primary end points of the study include both an assessment of the response to initial therapy using our previously described dynamic risk assessment scheme (excellent, acceptable, or incomplete response to thyroidectomy and RAI ablation) (21) and an assessment of the final clinical status determined at the time of last follow-up (no evidence of disease, persistent disease, or disease recurrence).
Methods
Subjects
A total of 586 patients with differentiated thyroid cancer who had undergone total thyroidectomy and RRA between January 1994 and December 2004 were the basis of this study with the final clinical status updated as of November 2011 with the appropriate Institutional Review Board approval (21).
The choice of preparation method for RAI ablation (rhTSH vs. THW) was a decision made by the treating physician and the patient. When rhTSH became commercially available, several Memorial Sloan-Kettering Cancer Center (MSKCC) clinicians began to offer rhTSH preparation for ablation for all patients without distant metastases (including ATA intermediate and high-risk patients). Other clinicians at MSKCC and most referring physicians continued to offer THW preparation for many years. As a result, we now follow many intermediate and high- risk patients prepared for RAI ablation with either rhTSH or THW in whom the choice of preparation was based more on clinician practice patterns than on specific clinicopathologic risk factors. Therefore, as with our previous studies (9,15), we expected to find no significant detectable differences in the standard clinicopathologic risk factors between patients prepared with rhTSH and those prepared with THW.
All patients included in the study received TSH suppressive therapy and had at least one neck ultrasound performed at our center after initial therapy during the first 2 years of follow-up and two or more serum Tg and thyroglobulin antibodies (TgAb) determinations on levothyroxine suppression during the first 2 years of follow-up. A minimum of 3 years of follow-up was required for entry into the study unless one of the clinical end points (recurrence or death) was reached before that point. All patients had Tg and TgAb levels measured while on TSH suppressive therapy at the time of final follow-up. A stimulated Tg value within the first 2 years of follow-up was not a requirement for inclusion in the study, but was available in 80% (n=471) of the patients.
Between 1994 and 1997, a variety of Tg assays were used with functional sensitivities of ∼1 ng/mL. Starting in 1998, all Tg values were measured using the Dynotest-TgS immunoradiometric assay (Brahms, Inc.; functional sensitivity 0.6 ng/mL normalized to CRM 457).
Radioactive iodine remnant ablation
After total thyroidectomy, 321 patients underwent THW as preparation for RRA. Their stimulated TSH and Tg levels were drawn on the day 55.5 MBq (1.5 mCi) of 123I RAI was administered (day 1). As per the standard protocol at MSKCC, a TSH level of more than 25 mIU/L was required before RRA. The patients returned on day 2 for a diagnostic whole-body scan with subsequent administration of the ablative dose of 131I as previously described (15).
The 265 patients who underwent rhTSH-stimulated RAI remnant ablation received levothyroxine immediately after surgery and continued to take levothyroxine throughout the RRA procedure. One to 3 months after surgery, patients received 0.9 mg of rhTSH intramuscularly on the mornings of day 1 and 2, followed 55.5 MBq (1.5 mCi) of 123I on the afternoon of day 2. They returned on the morning of day 3 for a diagnostic whole-body scan and an ablative dose of 131I. A post-therapy scan was obtained for each patient 5–7 days after administration of the ablative dose of 131I (15).
All patients were provided with information on low-iodine diets and encouraged to adhere to them carefully. The administered activity of 131I chosen for ablation was based on the recommendations of a thyroid cancer tumor board consisting of adult and pediatric endocrinologists, nuclear medicine physicians, thyroid surgeons, and oncologists. The activity selected was based on the clinical features of the patient, the histologic findings, intraoperative findings, risk of recurrence, and results of diagnostic whole-body scanning.
Follow-up
Patients were usually followed every 6 months during the first year and at 6–12-month intervals thereafter at the discretion of the attending physician based on the risk of the individual patient and the clinical course of the disease. All patients received TSH suppressive therapy.
Initial risk stratification
Each patient was risk-stratified using the seventh edition of the AJCC/UICC staging system (stage I, II, III, or IV) and the ATA risk of recurrence stratification system (low, intermediate, or high risk of recurrence, Table 1) (22).
ATA, American Thyroid Association; PTC, papillary throid cancer; RAI, radioactive iodine; Tg, thyroglobulin; US, ultrasound.
Best response to initial therapy
All clinical data obtained during the first 2 years of follow-up were used to assess the best response to initial therapy (total thyroidectomy and RAI ablation) as either excellent, acceptable, or incomplete using the restratification scheme proposed and validated by our group (Table 1) (21). This system classifies patients based on the best clinical response to total thyroidectomy and RAI ablation obtained during the first 2 years of follow-up.
Clinical status at the time of last follow-up
At the time of final clinical follow-up, each patient was reclassified as having no evidence of disease, persistent disease, or recurrent disease (Table 1). The clinical status at final follow-up reflects not only the initial response to total thyroidectomy and RAI ablation, but also the potential effects of continued levothyroxine suppressive therapy, any additional surgeries or radiation therapies, and the passage of time.
Statistical methods
Continuous data are presented as means and standard deviations (SD) or median and range values, as appropriate for each variable. Categorical comparisons were performed using Chi square testing with the Fischer's exact test when appropriate. The analysis was performed using SPSS software (version 19.0.0: SPSS, Inc., Chicago, IL). A p-value less than or equal to 0.05 was considered statistically significant.
Results
Patient characteristics
Of the 586 patients included in the study, 321 had RRA following traditional THW and 265 were ablated following rhTSH stimulation. As can be seen in Table 2, there were no significant identifiable differences between the two cohorts with respect to gender, age at time of ablation, size of the primary tumor, histology of the primary tumor, administered activity of RAI, AJCC stage, ATA initial risk stratification, or clinical status at the final follow-up. The M1 patients included in these cohorts either received their RRA outside our center or had their distant metastases identified on RAI imaging done as part of RRA and therefore did not undergo whole-body RAI dosimetry studies before RRA. The median duration of follow-up for the entire cohort was 9 years (mean 8.5 years±3.5 years, range 2–20 years). The THW cohort had a longer follow-up duration (8.8±3.6 years, median 11 years) than the rhTSH cohort (8.1±3.3 years, median of 8 years, p=0.03).
TSH, thyroid stimulating hormone; SD, standard deviation; NS, not statistically significant; RRA, radioactive iodine remnant ablation; AJCC, American Joint Committee on Cancer.
Response to initial therapy
As can be seen in Table 3, patients prepared with rhTSH were significantly more likely to have an excellent response to initial therapy than patients prepared with THW (39.4% vs. 30%, p=0.03). Conversely, patients prepared with THW were significantly more likely to demonstrate an incomplete response to initial therapy than patients prepared with rhTSH (46.8% vs. 38.5%, p=0.03). Furthermore, patients prepared with THW were significantly more likely to receive additional therapies during subsequent follow-up (36.8% vs. 29.1%, p=0.05) than patients prepared with rhTSH.
When additional therapies were given, 62% received additional RAI treatments, 5% had neck surgery, 20% had both neck surgery and RAI, and 13% received a variety of other therapy combinations. There were no differences with regard to the type of additional treatments given between the rhTSH and the THW cohorts (data not shown).
Clinical status at final follow-up
After a median follow-up of 11 years for the THW cohort and 8 years for the rhTSH cohort, the final clinical outcomes were not significantly different (Table 3). The percentage of patients classified as having no evidence of disease (51.1% THW vs. 52.5% rhTSH), persistent disease (47.7% THW vs. 46% rhTSH), or recurrent disease (1.2% THW vs. 1.5% rhTSH) were remarkably similar between the cohorts. The median time to detection of disease recurrence was also not significantly different between the patients prepared with THW (median 6 years, mean±SD 6.2±3.3) and those prepared with rhTSH (median 6.5 years, mean±SD 6.5±3.6 years) (Fig. 1 for recurrence-free survival curves).
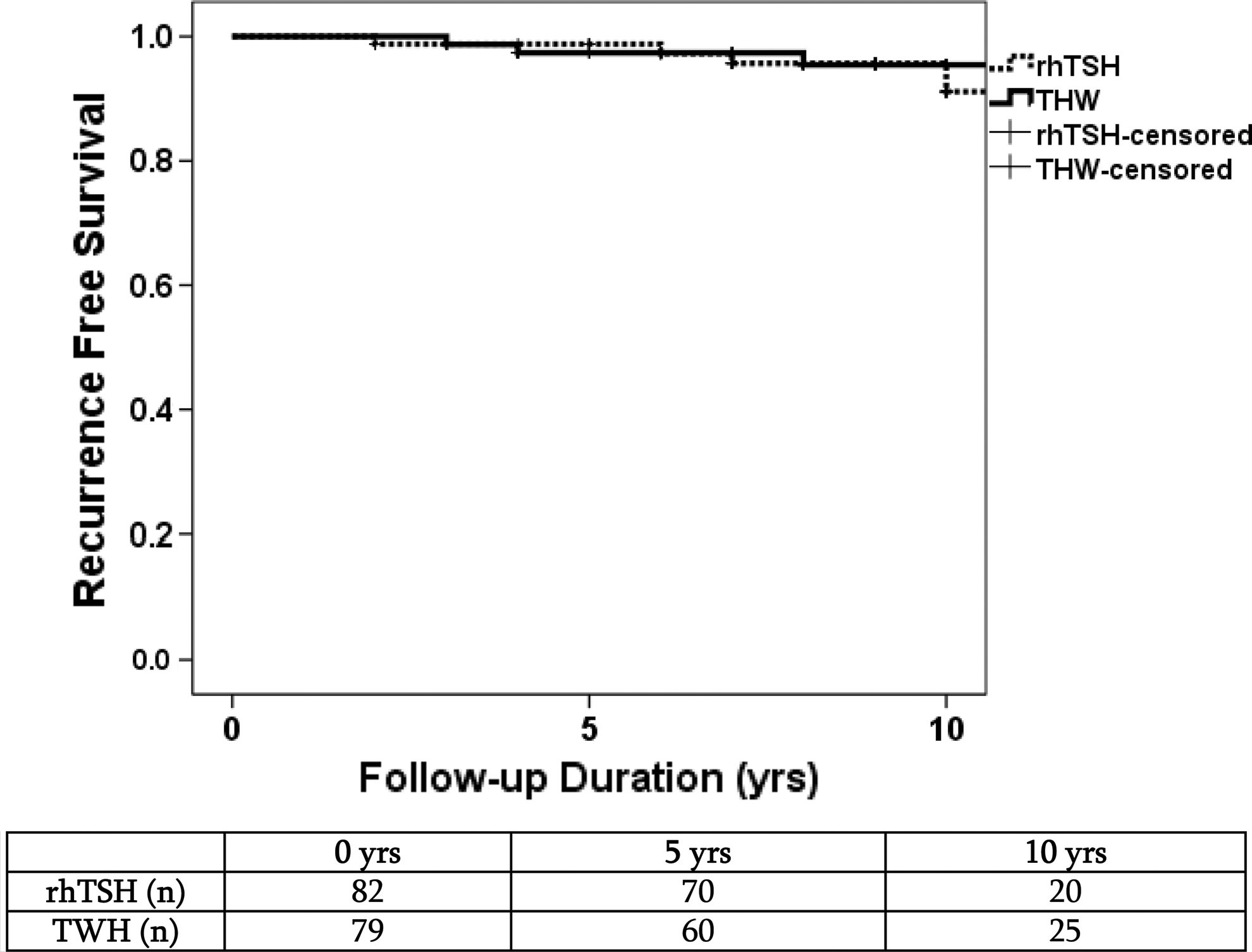
Recurrence-free survival curves over the first 10 years of follow-up.
Clinical outcomes based on initial AJCC staging
The study included a significant number of AJCC stage III (n=89) and stage IV patients (n=147). Within each of the AJCC stages (I, II, III, and IV), there were no significant differences between the THW and the rhTSH cohort with regard to gender, age at time of ablation, size of the primary tumor, histology of the primary tumor, administered activity of RAI, or tumor histology. As can be seen in Table 4, in patients across all AJCC stages no statistically significant differences were detected in either the response to initial therapy or the clinical status at final follow-up between patients prepared with THW and those prepared with rhTSH.
Clinical outcomes based on initial ATA risk stratification
As can be seen in Table 5, the study cohort also included a large number of patients classified as ATA intermediate risk (n=291) or ATA high risk (n=161). Within each of the ATA risk categories (low, intermediate, and high), there were no significant differences between the THW and the rhTSH cohort with regard to gender, age at time of ablation, size of the primary tumor, histology of the primary tumor, method of preparation, administered activity of RAI, tumor histology, AJCC stage, or ATA initial risk stratification.
No significant differences were seen between rhTSH and THW preparation with regard to the response to initial therapy or the final clinical outcome in either the ATA low-risk or the ATA high-risk subgroups (Table 5 and Fig. 2). However, in the ATA intermediate risk cohort, rhTSH was statistically more likely to be associated with higher rates of excellent response (43.1% vs. 30.8%, p=0.02) and lower rates of incomplete response (30.3% vs. 44.4%, p=0.02) than THW preparation. Additional treatments after ablation were given to 25.5% of the rhTSH cohort and 28% of the THW cohort (not statistically significant). Final clinical outcomes did not differ in the ATA intermediate risk cohort with 54.7% of the THW group and 58.9% of the rhTSH group classified as no evidence of disease at last follow-up.
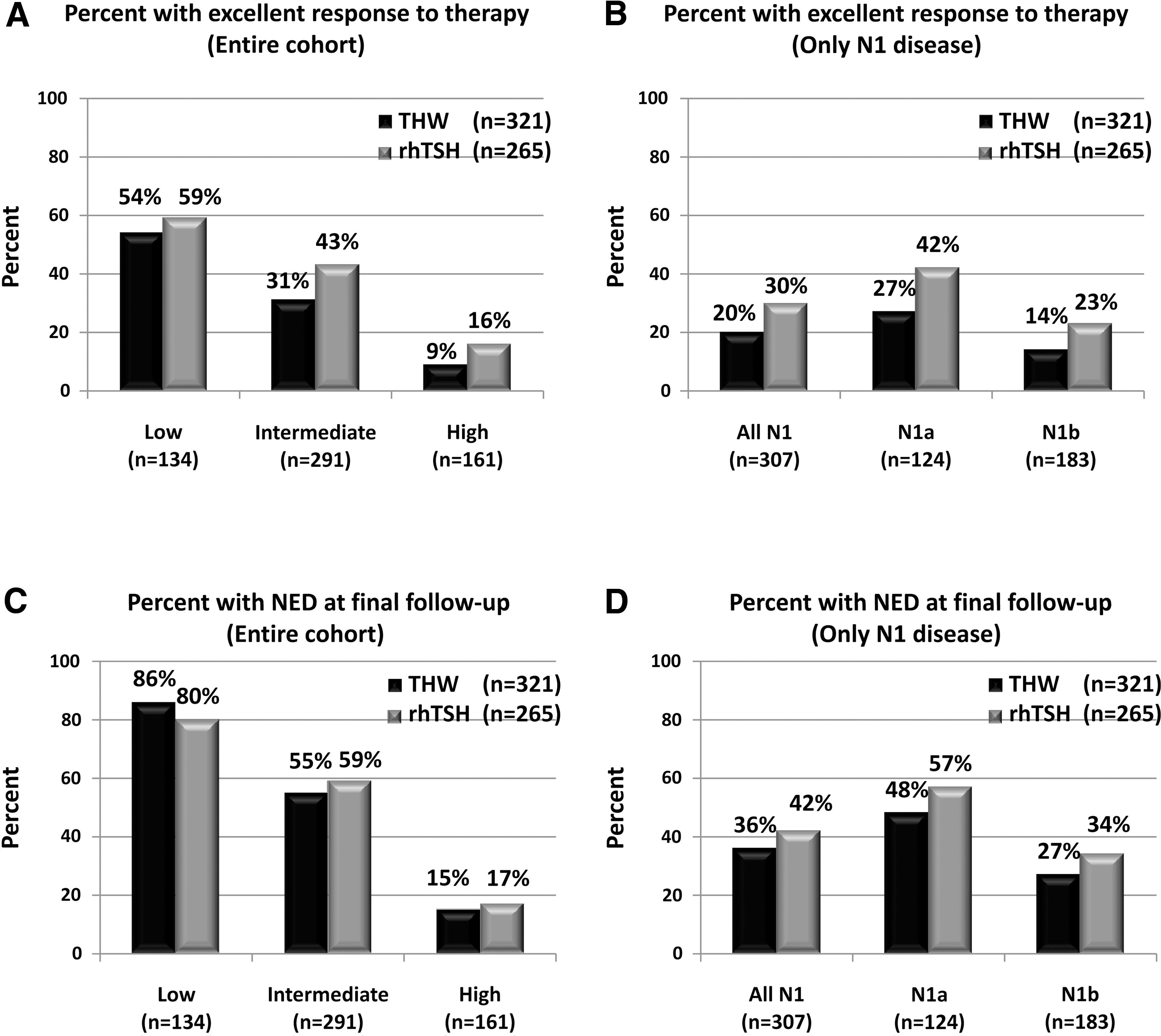
Comparison of primary clinical end points between patients prepared with THW versus rhTSH. The percentage of patients achieving an excellent response to therapy (suppressed and stimulated Tg<1 ng/mL and negative imaging in the first 2 years of follow-up) based on the ATA risk group is shown in
Clinical outcomes in patients with N1 disease
Of the entire cohort, 21% (n=124) had N1a disease and 31% (n=183) had N1b disease. The administered activity was not significantly different between the N1 patients prepared with rhTSH (145±64 mCi) and those prepared with THW (147±83 mCi). As can be seen in Table 6, when analyzing all patients with pN1 disease (N1a+N1b) preparation with rhTSH was associated with significantly higher rates of excellent response to therapy (30.1% vs. 20%, p=0.02) and with lower rates of incomplete response to therapy (46.9% vs. 61.4%, p=0.02) than preparation with THW. Furthermore, N1 patients prepared with THW were more likely to receive additional therapies after initial ablation than patients prepared with rhTSH (48.8% vs. 32.6%, p=0.005). When given, the additional therapy usually consisted of additional RAI therapy with or without additional surgery. The final clinical outcomes for all patients with N1 disease were very similar and not statistically significantly different (Table 6).
The subgroup analysis comparing the methods of preparation in patients with either central neck metastases (N1a disease) or lateral neck metastases (N1b disease) demonstrated no significant differences with respect to either the response to initial therapy or the clinical status at final outcome (Table 6 and Fig. 2).
Discussion
In this retrospective cohort of 586 patients with differentiated thyroid cancer, preparation for RAI remnant ablation with rhTSH was associated with a small, but significantly higher percentage of patients achieving an excellent response to therapy than preparation with THW (39.4% vs. 30%, p=0.03) with similar rates of recurrence (1.2% THW vs. 1.5% rhTSH) over a median follow-up of 9 years. These data are consistent with our previous study, which demonstrated that rhTSH preparation was associated with better short-term clinical outcomes than THW preparation in a smaller series followed for a median of 2.5 years (15).
While Rosario et al. also demonstrated nearly equivalent short-term clinical outcomes following either rhTSH or THW preparation in a cohort of high-risk patients (all N1 or T3), they demonstrated what appears to be significantly higher overall rates of excellent response to initial therapy (80% of 169 patients prepared with THW vs. 80% of 70 patients prepared with rhTSH) than we found in our cohorts (12). While the precise reason for these differences cannot be completely known, it is likely that there is a difference in selection criteria with regard to which patients with N1 disease and T3 disease are chosen for RRA. While many centers routinely offer RRA to all patients with N1 disease or any degree of microscopic extrathyroidal extension (T3), we usually reserve RRA for N1 patients with higher volume metastatic disease (multiple positive lymph nodes, larger lymph node metastases) and usually don't recommend routine RRA on the basis of only minor extrathyroidal extension (23). Furthermore, since we do not routinely perform prophylactic central neck dissection, most of our N1 patients would have clinically evident macroscopic lymph node metastases. Therefore, it is likely that the N1 and T3 patients selected for RRA at our center were at higher risk for recurrence than similar staged patients selected for ablation at other centers. It is also important to emphasize that patients that achieve an excellent response to therapy [alternatively referred to as remission (24)] in our study meet the very strict criteria set forth in the ATA guidelines for being classified as having no evidence of disease (22).
In addition to the benefit of being less likely to need additional therapies after ablation than patients prepared with THW (29.1% vs. 36.8%, p=0.05), patients prepared with rhTSH also required a less aggressive follow-up and less intense TSH suppression. According to the current ATA guidelines, after patients achieve an excellent response to therapy, they can transition to a less intense long-term follow-up program that is based primarily on yearly suppressed Tg values and physical examination (Recommendation 45b) and also have the degree of TSH suppression reduced (Recommendation 49). Thus, patients that achieve an excellent response to therapy will require fewer repeat surgical procedures and/or RAI treatments, shorter duration of TSH suppression, which may have less adverse effects on the cardiac and skeletal systems in the long-term and less intense follow-up with imaging and blood tests.
Even though the rhTSH cohort had higher rates of excellent response to initial therapy, both cohorts appeared to be very similar at the time of final follow-up with ∼52% of each group classified as no evidence of disease, 47% classified as persistent disease, and 1.5% classified as recurrent disease. It is important to note that definition of the absence of disease is more stringent with the “excellent response to therapy” definition (requires stimulated Tg<1 ng/mL and no structural/functional evidence of disease) than in the final outcome “no evidence of disease” definition (requires suppressed Tg<1 ng/mL and no structural/functional evidence of disease). Therefore, if stimulated Tg values were available for patients at the time of final follow-up, it is likely that some of the patients classified as no evidence of disease could in fact have a low-level persistent biochemical disease. While a stimulated Tg value would improve the definition of no evidence of disease at final follow-up, it was not a practical end point as very few of the patients included in the study had stimulated Tg values obtained at the time of final follow-up.
Our data is consistent with the previous studies that have reported very low recurrence rates in both low (17)- and high-risk patients (12,15,18) prepared for RRA with either rhTSH or THW. After a median follow-up of 3.7 years, Elisei et al. demonstrated no clinical recurrences in a low-risk cohort of patients previously randomized to receive either rhTSH (n=27)- or THW (n=21)-stimulated RRA ablation (17). In the recent publication by Rosario et al., recurrence rates after a median of 5 years of follow-up were also very similar (THW, 4.2% vs. rhTSH, 5.2%, p=not significant) in a higher risk cohort of patients (12). In our previous publication (15), we reported clinical recurrence rates of 6.8% in 74 patients prepared with THW, and 3.8% in 320 patients prepared with rhTSH using a definition of the absence of disease that included a stimulated Tg value of less than 2 ng/mL and a negative follow-up diagnostic RAI scan. Over the last several years, we have moved to a more strict definition of the absence of disease [stimulated Tg<1 ng/mL, negative neck ultrasound, and no structural or functional evidence of disease (21)]. This more strict definition of remission results in a higher percentage of patients being classified as having persistent disease. Since a recurrence can only occur in patients previously classified as having no evidence of disease, when structural disease is identified during follow-up, it will be more likely to be classified as continued persistent disease than disease recurrence. Therefore, the lower recurrence rates we report in this article (1.2% THW, 1.5% rhTSH) are a reflection of the definitions of persistent and recurrent disease that are now in common use. These lower rates of recurrence and higher rates of persistent disease reflect our current understanding of the disease.
While most previous studies that evaluated the clinical utility of rhTSH in RRA have focused primarily on low-risk patients, our cohort provides the opportunity to evaluate clinical outcomes in significant numbers of patients at higher risk of recurrence and disease-specific mortality. When analyzed based on initial AJCC staging, no differences in either the response to initial therapy or the final clinical outcome was seen within any of the stages (I, II, III, or IV) or ATA risk categories based on the method of preparation for RRA, except for a better response to therapy in the ATA intermediate risk group prepared with rhTSH. Because of the higher risk of recurrence is often associated with having lymph node metastases at diagnosis (N1 disease), some clinicians have refrained from using rhTSH preparation in patients that presented with clinically significant lymph node metastases. Our data are very reassuring in that rhTSH preparation was associated with a similar or better initial response to therapy and similar final clinical outcomes when compare to THW in patients with lymph node metastases at diagnosis. Furthermore, the finding of similar initial response to therapy and final clinical outcomes in patients that had N1b disease is also confirmatory that rhTSH preparation appears to be as effective as THW in preparing patients with clinical significant lymph node metastases to RRA. These findings are consistent with previous reports of the effectiveness of rhTSH preparation for both RAI adjuvant therapy (16) and RAI therapy of distant metastases (20,25).
One of the primary limitations of this study is the design, which describes a retrospective review of nonrandomized selection of patients for either rhTSH or THW preparation. While we cannot rule out subtle selection bias, we were unable to detect any major differences in the standard clinicopathologic risk factors between the study cohorts. Furthermore, important clinical decisions such as the intensity of follow-up and the need for additional therapy were not standardized and probably varied significantly between patients and treating physicians.
In conclusion, rhTSH preparation for RRA is associated with a small, but a statistically significant improved initial response to therapy and similar final clinical outcomes in a large cohort of patients followed for a median of 9 years. In subgroup analyses based on either risk of recurrence, presence of lymph node metastases, or risk of disease-specific mortality, both rhTSH and THW preparation provided very similar outcomes. These data demonstrate the efficacy of rhTSH-assisted ablation in higher risk patients.
Footnotes
Disclosure Statement
J.H., R.G., S.L., and E.R. have nothing to declare. R.M.T. is a consultant to and has received honoraria from the Genzyme Corporation.