
Abstract
Background:
Traditionally, thyroid surgery has been an inpatient procedure due to the risk of several well-documented complications. Recent research suggests that for selected patients, outpatient thyroid surgery is safe and feasible, with the additional potential benefit of cost savings. In recognition of these observations, we hypothesized that there would be an increase in U.S. outpatient thyroidectomies with a concurrent decline in inpatient thyroidectomies over time.
Methods:
Comparative cross-sectional analyses of the National Survey of Ambulatory Surgery (NSAS) and Nationwide Inpatient Sample (NIS) databases from 1996 and 2006 were performed. All cases of thyroid surgery were extracted, as well as data on age, sex, and insurance status. Diagnoses and surgical cases were identified using International Classification of Diseases, Ninth Revision (ICD-9) diagnostic and treatment codes. Hospital charges were acquired from the NIS 1996 and 2006 and NSAS 2006 releases, using imputed data where necessary. After survey weights were applied, patient characteristics, diagnoses, and procedures were compared for inpatient versus outpatient procedures.
Results:
The total number of thyroidectomies increased 39%, from 66,864 to 92,931 cases per year during the study timeframe. Outpatient procedures increased by 61%, while inpatient procedures increased by 30%. The proportion of privately insured inpatients declined slightly from 63.8% to 60.1%, while those covered by Medicare increased from 22.8% to 25.8%. In contrast, the proportion of privately insured outpatients declined sharply from 76.8% to 39.9%, while those covered by Medicare rose from 17.2% to 45.7%. These trends coincided with a small increase in the mean inpatient age from 50.2 to 52.3 years and a larger increase in the mean outpatient age from 50.7 to 58.1 years. Inflation-adjusted per-capita charges for inpatient thyroidectomies more than doubled from $9,934 in 1996 to $22,537 in 2006, while aggregate national inpatient charges tripled from $464 million to $1.37 billion. By comparison, per-capita charges for outpatient thyroidectomy totaled $7,222 in 2006.
Conclusions:
From 1996 to 2006, there has been a concurrent modest increase in inpatient and pronounced increase in outpatient thyroidectomies in the United States, with a consequential demographic shift and economic impact.
Introduction
Research in the 1970s and 1980s in obstetrics, otolaryngology, general and pediatric surgery, urology, and other specialties suggested that outpatient procedures could be safely performed for an increasing variety of indications (3 –7). This changing paradigm was informed greatly by the potential for significant economic benefits from shifting surgical procedures to the ambulatory setting (8,9). From 1980 to 1995, the number of ambulatory procedures in the U.S. grew ninefold to 27 million cases (10), and in 2006 an estimated 57.1 million procedures were performed during 34.7 million ambulatory surgery visits (11). Although high-volume hospitals have been associated with improved outcomes in several types of major inpatient surgeries such as bariatric surgery (12), pulmonary lobectomy (13), and nephrectomy (14), an analysis of data from the National Surgical Quality Improvement Program found poor correlation between inpatient and outpatient surgical quality at the same hospitals (15). Thus, it is unclear whether rising ambulatory surgical volume has translated into better patient outcomes.
While thyroidectomy has traditionally been an inpatient procedure to permit monitoring for these potential morbidities, this standard has been changing gradually. For reasons of shorter convalescence, patient and surgeon convenience, and cost containment, thyroidectomy has been transitioning toward the ambulatory setting (16,17), following the pattern of outpatient care for about two-thirds of all surgical encounters in the United States (18). Multiple institutional case series have documented the safety, feasibility, and cost-effectiveness of outpatient thyroidectomy for selected patients, strengthening the argument in support of performing surgery in the ambulatory setting (19 –27).
The incorporation of outpatient surgical approaches into the management of thyroid disease has potential health and economic implications, and it has not been broadly characterized at the national level. The objective of this study was to summarize the epidemiological trends and economic impact of inpatient and outpatient thyroidectomy in the United States in order to determine the extent to which ambulatory procedural trends have affected thyroid surgery. We initially hypothesized that there would be an increase in outpatient thyroidectomies over time, coupled with a decrease in inpatient thyroidectomies.
Materials and Methods
This study included cross-sectional analyses of the Healthcare Cost and Utilization Project (HCUP) Nationwide Inpatient Sample (NIS) (28), which is supported by the Agency for Healthcare Research and Quality (AHRQ), and the National Survey of Ambulatory Surgery (NSAS) for the years 1996 and 2006 (29). The NIS is the largest national inpatient care database in the United States, with discharge data from ∼8 million hospitalizations annually, and currently is available from 1988 to 2009. The NSAS is the only national study of ambulatory surgical care at both hospital-based and ambulatory surgical centers and was conducted from 1994 to 1996, then again in 2006. This study used publicly available data and was judged exempt by the University of Michigan Institutional Review Board as a secondary analysis of de-identified records.
Diagnoses and procedures were identified using the International Classification of Diseases, Ninth Revision (ICD-9) manual (30). All patients underwent subtotal or partial thyroidectomy (ICD-9 procedure codes 06.2, 06.3, 06.31, or 06.39), total or complete thyroidectomy (06.4), or other types of thyroidectomy such as substernal or lingual thyroidectomy (06.5, 06.51, 06.52, 06.6, or 06.98). Neck dissections were identified using ICD-9 codes 40.3, 40.4, 40.40, 40.41, and 40.42. Data on patient age, sex, insurance, and pertinent primary diagnosis (using ICD-9 diagnostic codes) were extracted from the 4 databases utilized in this study. All diagnostic variables provided in each dataset were analyzed, since patients could have more than one clinically relevant diagnosis. Data on total charges were obtained from the 1996 and 2006 NIS and the 2006 NSAS databases. The 1996 NSAS database does not contain economic data.
Both the NIS and NSAS databases represent stratified samples of healthcare sites across the United States. Therefore, weighting variables were applied to obtain national estimates of the populations of interest, and all statistics presented in the results were derived from weighted data. After survey weights were applied, descriptive statistics regarding hospital charges and patient characteristics, diagnoses, and procedures were calculated. The thyroidectomy rate per 100,000 people for each year was calculated using U.S. Census data from 1996 and 2006 (31). Due to over 52% missing data in the total charges variable for the NSAS 2006 release, we conducted multiple imputation by chained equations five times, which appropriately replaced missing observations with values consistent with patterns in the dataset and allowed us to provide better estimation of mean and total charges for outpatient thyroidectomy (28). Stata 12.1 (StataCorp LP, College Station, TX) was used for data analysis.
Results
Applying hospital-based weights yielded 52,062 inpatient and 19,099 outpatient thyroidectomy patients in 1996, and 62,200 inpatients and 30,731 outpatients in 2006 (Table 1). Thus, from 1996 to 2006, the aggregate national thyroidectomy surgical volume increased from 71,161 to 92,931 cases. Within this increase, using the difference in proportions test there was a significantly marked shift in case volume away from the inpatient setting from 73.1% [95% confidence interval (CI) 72.8%–73.5%] in 1996 to 66.9% [CI 66.6%–67.2%] in 2006. Consequently, population-adjusted annual rates of thyroidectomy increased by 8.7% in the inpatient setting and 45.9% in the outpatient setting.
All figures (n) are weighted. Column percentages may not total 100% due to rounding. The rate of all thyroidectomies was calculated for each year using U.S. Census data for 1996 and 2006 (31).
Subtotal thyroidectomy was the most commonly performed procedure, regardless of the year or disposition, although there was a 15.1% decrease in the inpatient cohort and 65% increase in the outpatient cohort. Total thyroidectomies experienced the largest percentage gains in both inpatient and outpatient groups over time. Very few outpatient “other” thyroidectomies, including substernal and lingual thyroidectomies, were reported in 2006. Concurrent neck dissections increased over 70% in the inpatient group, though still comprising <4% of all inpatient cases, while in the outpatient group neck dissections decreased from 612 cases to a figure too low to estimate.
The mean age of inpatients rose slightly, from 50.2 to 52.3 years in 1996 and 2006, respectively, while the mean age of outpatients increased from 50.7 to 58.1 years. After stratifying patients into ≤44, 45–64, and ≥65 years of age, the number of inpatients aged 65 years or older rose from 11,943 (22.9% of the inpatient cohort) in 1996 to 14,974 (24.1%) in 2006, an overall increase of 25.4%. In contrast, the number of outpatients aged 65 years or older rose from 3148 (16.5% of the outpatient cohort) in 1996 to 12,375 (40.3%) in 2006, an increase of 293.1%. Meanwhile, inpatients aged 44 years or younger declined 5.9% during the same time period, from 20,692 (39.7% of inpatients) to 19,466 (31.3%). The number of outpatients in the same age group decreased 25.2%, from 7120 (37.2% of outpatients) to 5329 (17.3%). Female patients far outnumbered males in all years and operative settings, ranging between 80.8% and 81.5% for inpatients and 79.5% and 91.2% for outpatients.
The distribution of insurance coverage for both inpatients and outpatients is shown in the Figure 1. In 1996, nearly two-thirds of all thyroidectomy patients had private or commercial insurance regardless of surgical setting. However, the largest proportional changes in patient volume were seen in the outpatient Medicare and Medicaid groups. The number of outpatients with Medicare rose from 3155 (17.2%) to 13,907 (45.7%), an increase of 340.8%, while those with Medicaid jumped from 193 (1.1%) to 2822 (9.3%), an increase of 1362.2%. Thus, by 2006 Medicare became the predominant insurer for outpatient cases, and combined with Medicaid represented over half of all outpatients. Proportionally, outpatients with private insurance declined from 14,096 (76.8%) to 12,151 (39.9%). Inpatients continued to be represented primarily by private insurance in 2006.
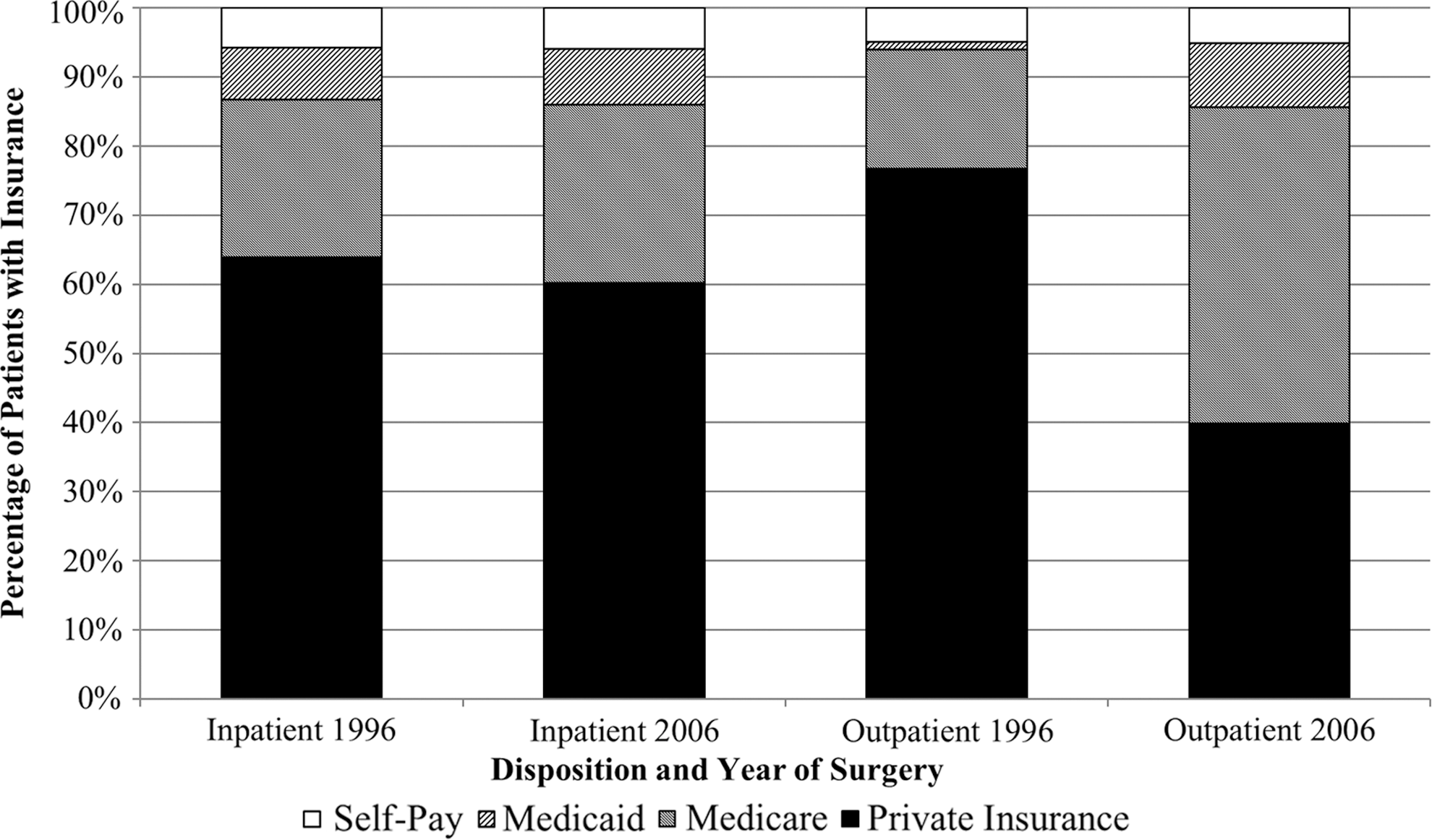
Distribution of insurance status in thyroidectomy patients.
The top three diagnoses overall were, in decreasing order of frequency, nontoxic nodular goiter, malignant neoplasm, and benign neoplasm (Table 2). The type and distribution of diagnoses in inpatient cases changed relatively little over time. In the outpatient cohort, “other” miscellaneous disorders, including thyroid cysts and hemorrhage, experienced the largest percentage gain (+447.2%) from 1996 to 2006. This was followed by a 157% increase in malignant thyroid neoplastic diagnoses. Unspecified endocrine neoplasms, which include both thyroid and parathyroid lesions, became a top-five outpatient diagnosis in 2006.
Since patients could have multiple diagnoses, percentages for each year and surgical disposition do not add up to 100%.
Cases of thyrotoxicosis were too few to estimate in 2006.
1099 cases of unspecified endocrine neoplasm were reported in 1996.
ICD-9, International Classification of Diseases, Ninth Revision (30).
After adjusting for inflation to 2006 levels using the U.S. Consumer Price Index (32), the estimated mean hospital charges for all inpatient thyroidectomies increased from $9934 in 1996 to $22,537 in 2006. Along with the simultaneous increase in case volume, the aggregate national charges for inpatient thyroidectomy increased from $464 million in 1996 to $1.37 billion in 2006.
After imputation, the estimated total charges for all ambulatory thyroid surgeries in 2006 were $1.16 billion, while the mean hospital charges per case were $7222. Using 1996 case volume proportions as a baseline, we estimated that 4153 cases that would have been inpatient in 1996 were done in the ambulatory setting in 2006. Multiplying this figure by the difference in unit charge between inpatient and outpatient thyroidectomy ($15,315) in 2006 yielded estimated yearly savings of $63.6 million by transitioning cases to the outpatient setting.
Discussion
This is the first study to use national databases to determine whether the uptake of thyroid surgery into the ambulatory setting has occurred at the national level and whether surgeons have been pursuing fewer inpatient surgeries as a result. Our research suggests that there has indeed been a substantial increase in ambulatory thyroidectomy from 7.2 to 10.5 cases per 100,000 people from 1996 to 2006. This rise was accompanied by a modest increase in inpatient thyroidectomy volume. The significance of these trends is not entirely clear in the greater context of healthcare, as examining different specialties and procedures reveals high variability in inpatient and outpatient surgical utilization over time. For example, kyphoplasty procedural rates have increased in both inpatient and outpatient settings, similar to the results of our study (33). In contrast, adenotonsillectomy, facial fracture repair, lumbar spine surgery, rotator cuff repair, and vertebroplasty have all shown different combinations of utilization trends across the inpatient and ambulatory settings (33 –37).
To our knowledge, this is the first study to demonstrate a marked difference in payer status over time based on operative setting. In 1996, both inpatients and outpatients were predominately covered by private insurance. Yet, by 2006, over half of all outpatients were covered by government-based insurance, with the Medicare group more than quadrupling and the Medicaid group increasing >14-fold. Meanwhile, inpatients covered by private insurance experienced an increase of just 13% in the absolute number of cases and proportionally remained stable relative to inpatients covered by other payers. The change in distribution could be explained by the surgeries performed: total thyroidectomies and neck dissections were performed far more frequently in inpatients than in outpatients. However, regardless of operative setting the most common procedure was still subtotal thyroidectomy. Although malignant neoplasms comprised a greater fraction of inpatient diagnoses compared to outpatient diagnoses, the underlying distribution of inpatient diagnoses was essentially stable. From a demographic standpoint, the outpatient group was actually older than the inpatient group in 2006. The long-term outcomes and socioeconomic implications of keeping younger, better-insured thyroidectomy patients hospitalized—despite no notable changes in inpatient diagnostic distribution over time—while discharging older, government-insured patients from the ambulatory setting require further investigation.
The current study also establishes an estimated economic burden of both inpatient and ambulatory thyroid surgery in the United States. Adjusted for inflation, the aggregate cost of inpatient thyroidectomy tripled during the study timeframe, while the per-capita cost more than doubled. Similar economic trends have been observed in hospitalizations for pediatric skin and soft tissue infections (38), subdural hematomas (39), and cerebral aneurysms (40), among other disorders. Though much of the increase in costs may be attributable to specialty-specific issues such as changes in clinical practice, other more universal factors such as type of treating hospital, regional or system-based resource availability, and introduction of new therapeutic technologies can also escalate charges (40 –43). There may also be increases in the component costs of hospitalization, such as changes in room and board, drug pricing, or provider staff salaries. Furthermore, other research has indicated that increasing age is associated directly with increased costs of inpatient surgery (44,45), which may be relevant given that in our study the average age of the typical thyroidectomy patient rose from 1996 to 2006. This specific association may exist due to higher comorbidity burden and increased complications in the elderly. Prior research also has demonstrated that patients undergoing neck dissection also have been shown to have significantly higher thyroidectomy expenses, and from 2002 to 2009 there was a documented rise in neck dissections for malignant thyroid disease (46).
The mean charges for ambulatory surgery were only about one-third of the mean for inpatient surgery in 2006. This may be explained by the reduced need for physical space and utilization of ancillary services, and changes in anesthetic technique to accommodate outpatient surgery (47 –49). We estimate that the shift to the ambulatory setting may have saved $63.6 million in 2006, compared with operative setting patterns in 1996. Nonetheless, since the number of inpatient thyroidectomies was still double the outpatient figure in 2006, the expectation that aggregate hospital charges might be lessened further with the transition to the ambulatory setting may not be realistic yet.
Unfortunately, given the lack of comparative data from 1996 and the high percentage of missing data from the 2006 NSAS database, we could not determine whether the charges per ambulatory thyroid surgery have increased. However, it is all but certain that aggregate charges have risen substantially due to the much higher volume of ambulatory procedures in 2006. Rising costs in both the inpatient and outpatient theaters should be of particular concern to healthcare stakeholders, particularly since it is unclear whether patients are experiencing better outcomes. The importance of high-volume surgeons and hospitals in improving inpatient thyroidectomy outcomes has been demonstrated repeatedly (44,50). However, research into whether this tenet holds true in outpatient thyroidectomy patients is relatively sparse (51). Furthermore, no cost–benefit analyses exist of transitioning surgery to the outpatient setting while demonstrating comparable costs and benefits. Evaluating short-term and long-term health and economic outcomes as a result of shifting thyroidectomy to the ambulatory setting was beyond the scope of the project and would be an important area for future investigation.
Limitations to this study are in part inherent to the national databases used. Coding and sampling errors and missing data (particularly with respect to cost figures in the NSAS datasets) are significant issues, and ICD-9 codes in particular do not distinguish between thyroid cancer subtypes. Neither the NIS nor the NSAS datasets contain detailed information on cancer staging or severity, though Surveillance, Epidemiology, and End Results (SEER) analyses up to 2005 have suggested that differentiated thyroid neoplasms, particularly papillary cancers, appear to be the primary contributor to the surge in cancer diagnoses (52,53). Comorbidity data, which would have helped elucidate the overall frailty of the patient cohorts, was available for the NIS [based on the Elixhauser criteria (54)], but not specifically for the NSAS. Data on race/ethnicity are not available for the NSAS 2006 release. Extracting these data from ICD-9 codes in the NSAS datasets is possible, but we would be significantly underestimating the comorbidity burden in outpatients because only seven diagnostic variables are stored in the 1996 and 2006 NSAS datasets, a few of which would be occupied by codes pertaining to thyroid disease or complications from surgery. Because the NIS and NSAS databases are administrative and not outcomes-based, no pre- or posthospitalization data are available, precluding the analysis of possible changes in cancer diagnosis following surgery or the determination of trends in long-term morbidity or survival. Finally, the NIS and NSAS datasets are not linked, preventing us from tracking planned ambulatory cases that may have been hospitalized due to complications or other causes.
In summary, this study demonstrates that thyroid surgery rates in the United States have been increasing in both the inpatient and the ambulatory settings over the 1996–2006 period, though the increase in ambulatory procedures has greatly outpaced inpatient cases. The typical thyroidectomy patient in 1996 was female, middle-aged, and carried private insurance, regardless of operative setting. These demographics still describe inpatients in 2006, but for outpatients the average patient is now more likely to carry government-based insurance and nearly as likely to be at least 65 years old as middle-aged. Hospital charges for inpatient thyroidectomies have tripled in total and more than doubled on a per-capita basis. Further research is necessary to explain the demographic changes, determine the impact of operating setting changes on long-term health-related outcomes, the massive rise in total inpatient charges over the past decade, and the difference between per-capita inpatient and ambulatory charges. Additional research is also necessary to determine whether the increased thyroidectomy case volume and expenditures have resulted in direct health benefits to the patients served. These findings have significant policy-level implications for healthcare stakeholders hoping to institute effective cost-containment strategies and reduce health services disparities among thyroidectomy patients.
Footnotes
Acknowledgment
The authors thank HwaJung Choi, PhD (Robert Wood Johnson Foundation Clinical Scholars, University of Michigan), for statistical assistance.
Disclosure Statement
G.H.S. is a current Robert Wood Johnson Foundation Clinical Scholar supported by the U.S. Department of Veterans' Affairs. The Robert Wood Johnson Foundation and the Department of Veterans' Affairs were not directly involved in study design, data acquisition and interpretation, or manuscript preparation or review. Any opinions expressed herein do not necessarily reflect the opinions of the Robert Wood Johnson Foundation or the Department of Veterans' Affairs. All authors declare that no competing financial interests exist.