
Abstract
Background:
Neck lymph nodes may be involved in the pathogenesis of chronic autoimmune thyroiditis (CAT). This study was undertaken to identify which of the sonographic features of cervical lymph nodes are readily applicable to patients affected by CAT compared to healthy control subjects.
Methods:
We recruited 106 patients (92 females and 14 males) with CAT and 70 control subjects (53 females and 17 males) without clinical, biochemical, and ultrasonographic evidence of thyroid and neck diseases. We performed laboratory tests (thyrotropin, antithyroperoxidase antibodies, antithyroglobulin antibodies, and ultrasonography) to evaluate in each group: (i) thyroid function, autoimmunity, and morphology; (ii) number, topographic distribution (levels I–VI), and morphology of neck nodes (long-axis diameter; short-axis diameter; short-axis/long-axis ratio; absence or presence of hilus).
Results:
Total number of neck nodes with long-axis diameter >10 mm was significantly higher in the CAT group than in the control group (mean±standard deviation [SD]: 3.7±2.4 vs. 0.8±1.3; p<0.001) with significantly increased differences in levels II (1.4±0.8 vs. 0.3±0.5; p<0.001), III (2±1.2 vs. 0.3±0.7; p<0.001), and IV (0.7±0.7 vs. 0.07±0.2; p<0.001). More nodes with a hilus were found in the CAT group than in the control group (mean number of nodes±SD: 2.8±1.9 vs. 0.7±1.1; p<0.001). Short-axis diameter of level III (4.4±1 vs. 3.7±1.2 mm; p=0.002) and level IV nodes (3.9±1 vs. 3.1±0.5 mm p=0.030) was increased in CAT patients when compared with healthy controls.
Conclusions:
The present study is the first one aiming at a systematic description of the sonographic pattern of cervical lymph nodes in CAT. An increased number of benign hyperplastic neck nodes, especially in levels II–IV, appears to be a characteristic sonographic finding associated with CAT.
Introduction
In the context of autoimmune thyroid diseases, ultrasonography (US) is a well-established tool to identify patients with CAT (8), to predict the development of subsequent hypothyroidism (9), to discriminate pseudonodular areas from suspicious thyroid nodules, and to guide fine-needle aspiration biopsy (10). Moreover, US is able to distinguish two main forms of CAT: atrophic thyroiditis, characterized by a reduced thyroid volume and a large number of hyperechoic fibrous streaks superimposed on a hypoechoic background; and the most common classical form (Hashimoto's thyroiditis), characterized by various degrees and heterogeneously distributed zones of parenchymal hypoechogenicity, with a thyroid volume ranging from normal-increased to frankly increased (11).
US has also been extensively used to study cervical lymph nodes in the context of thyroid focal lesions (12) and thyroid cancer (13), but no systematic study is available to describe the sonographic pattern of cervical lymph nodes in CAT, despite the involvement of lymphoid tissue (14).
We hypothesized that the involvement of cervical lymph nodes in CAT may be associated with a different sonographic pattern of neck nodes in comparison to subjects without thyroid diseases. The knowledge of the characteristic features of CAT-associated reactive hyperplasia of neck nodes could be useful for clinicians as an additional element to establish a diagnosis. The aim of this study was to describe the ultrasonographic pattern of cervical lymph nodes in patients affected by CAT compared to healthy control subjects.
Materials and Methods
Patients
We considered 146 consecutive patients (106 females and 40 males; age range: 15–83 years) with CAT who attended the thyroid ambulatory at our Institutions during the period between April 2010 and June 2010 as eligible for the study. All patients showed a euthyroid state (thyrotropin [TSH] in the reference range).
All eligible patients underwent clinical examination, including neck US, and were evaluated with the following laboratory tests: TSH, antithyroperoxidase antibodies (TPOAb), and antithyroglobulin antibodies (TgAb).
Diagnosis of CAT was based upon the presence of parenchymal hypoechogenicity (compared to adjacent muscle structures) for at least one year, in conjunction with elevated levels of TPOAb and/or TgAb.
We excluded 40 patients who presented the following criteria: occurrence of thyroid nodules or pseudonodular images on clinical and/or US examination (23 patients); clinical evidence of nonthyroidal benign diseases of the neck and head (13 patients: 5 patients with recent acute upper respiratory tract infection; 5 patients with chronic upper respiratory tract inflammation; 1 patient with Sjögren's syndrome; 2 patients with periapical granuloma); a positive history of malignant diseases (2 patients with Hodgkin's lymphoma); a positive history of other autoimmune systemic or other systemic diseases involving lymphoid tissue (2 patients with lupus erythematosus). No suspicious neck lymph nodes were found on clinical examination and/or neck US.
The remaining 106 patients (92 females and 14 males, mean age 40.5±14.8) were included in the study (CAT group). For each patient included in the study, we recorded the following: sex; age (expressed in years); duration of disease (expressed in years after diagnosis); thyroid volume by US (expressed in mL), calculated using the ellipsoid formula (longitudinal diameter×transverse diameter×anteroposterior diameter×π/6) applied to each lobe; levothyroxine substitution dose (expressed in μg/day).
As the control group, we selected 70 healthy subjects (53 females and 17 male; age range, 12–87 years; mean age 44.9±16) with no clinical, laboratory (TSH, TPOAb, TgAb, leukocyte count, C-reactive protein, and erythrocyte sedimentation rate), and ultrasonographic evidence of thyroid diseases or other neck diseases.
Laboratory tests
Laboratory tests were performed both in CAT patients and the control group. TSH, TPOAb, and TgAb were measured using chemiluminescence immunometric assays (Immulite 2000; Siemens Medical Solutions Diagnostics, Los Angeles, CA), with the following reference ranges: TSH=0.4–4 μIU/mL (analytical sensitivity=0.004 μIU/mL); TPOAb=0–35 IU/mL; TgAb=0–40 IU/mL.
US evaluation
Gray-scale (GSUS) and power Doppler sonography (PDUS) were performed using an ultrasound mobile system, the Logiq P5 (General Electric Medical Systems, Milwaukee, WI), equipped with a wide-bandwidth (range 7–12 MHz) linear transducer.
All examinations were performed by two examiners with at least 17 years of experience in thyroid US. GSUS was performed at 12 MHz, and PDUS was performed at 6.7 MHz in both the CAT and control groups. Standardized Doppler settings were chosen to optimize detection of the signals from the lymph node vessels, which had low-velocity flow (pulse-repetition frequency=500 Hz; wall filter=77 or 50 Hz). Representative images by GSUS were obtained from each lymph node, so that the maximal area of the node appeared on the sonograms, with an axial orientation relative to the neck. For each neck lymph node with a long-axis diameter >10 mm, we recorded the following: long-axis diameter (expressed in mm); short-axis diameter (defined as the widest diameter of the node in the axial plane perpendicular to the long-axis diameter; expressed in mm); short-axis diameter/long-axis diameter ratio (S/L ratio); presence or absence of hilus, defined as a linear, hyperechogenic, nonshadowing structure containing nodal vessels, and continuous with fat around the node; location in the neck, classified according to the simplified level system proposed by Som et al. (15). Briefly, nodes were assigned to six levels (level I: submental and submandibular nodes; level II: upper internal jugular nodes; level III: middle jugular nodes; level IV: low jugular nodes; level V: nodes in the posterior neck triangle; level VI: upper visceral nodes, between carotid arteries, from the level of the bottom of the body of the hyoid bone to the level of the top of the manubrium). Level VII (superior mediastinal nodes) was not considered, given the scanning limits of GSUS.
Statistical analysis
Continuous variables were shown as mean values±standard deviation (SD). Rates and proportions were calculated for categorical data. Differences between the two groups were analyzed by the Mann–Whitney test (nonparametric test), as they were continuous variables without normal distribution. For categorical variables, differences were analyzed with χ 2 test and Fisher's exact test when appropriate. We considered a p-value <0.05 significant. We used SPSS v.13 software, Windows Edition (SPSS, Chicago, IL), for all our statistical analysis.
Results
The characteristics of the patients studied and the control subjects are shown in Table 1. There was no significant difference between the control and the CAT group in sex, age, thyroid function (TSH), and thyroid volume. Given the design of the study, TPOAb and TgAb were significantly higher in the CAT group (p<0.001). The patients in the CAT group had a mean levothyroxine substitution dose of 83.4±36.6 μg/day and a mean duration of disease of 5.7±4.2 years. The total number of neck nodes with a long-axis diameter >10 mm was significantly higher in the CAT group than in the control group (mean±SD: 3.7±2.4 vs. 0.8±1.3 mm; p<0.001) (Table 2). When we analyzed the number of neck nodes subdivided by level, we found a higher number of neck nodes in the CAT group than in the control group for each level analyzed, but the difference was only statistically significant in level II, III, and IV nodes (mean±SD: level II 1.4±0.8 vs. 0.3±0.5 mm, p<0.001; level III 2±1.2 vs. 0.3±0.7 mm, p<0.001; level IV 0.7±0.7 vs. 0.07±0.2 mm; p<0.001) (Table 2). More nodes with a hilus were found in the CAT group than in the control group (mean±SD: 2.8±1.9 vs. 0.7±1.1 mm; p<0.001) (Table 2).
TPOAb, antithyroperoxidase antibodies; TgAb, antithyroglobulin antibodies; NS, not significant; CAT, chronic autoimmune thyroiditis; TSH, thyrotropin; SD, standard deviation.
The neck node morphology is shown in Table 3. When we analyzed long-axis and short-axis diameter level by level, we found significantly higher short-axis diameter in level III and level IV nodes in the CAT group compared to the control group (short-axis diameter of III level, mean±SD: 4.4±1 vs. 3.7±1.2 mm, p=0.002; short-axis diameter of IV level, mean±SD: 3.9±1 vs. 3.1±0.5 mm, p=0.030). No statistical difference was found in the S/L ratio. Significantly, we always found nodes with S/L ratio <0.5. Figure 1 shows representative neck nodes from a CAT patient (Fig. 1A) and one control subject, respectively (Fig. 1B).
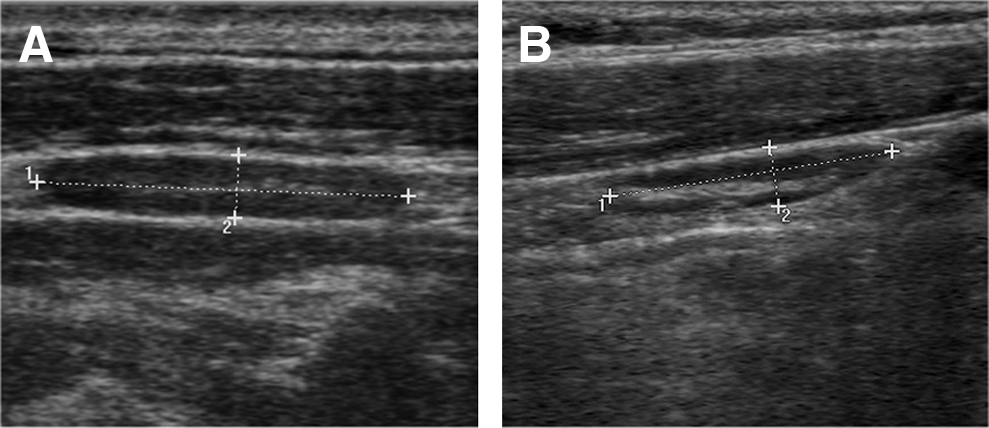
Representative example of neck lymph node in one chronic autoimmune thyroiditis patient
US, ultrasonography; S/L ratio, short-axis diameter/long-axis diameter ratio.
Discussion
Previously, only anecdotal reports about the description of neck nodes in CAT were available to the medical community. To the best of our knowledge, the present study is the first one aiming at providing a systematic description of the sonographic pattern of cervical lymph nodes in CAT.
Until recent years, neck nodes of increased size in CAT patients were considered as a finding pointing to malignancy (11). More recently, the extensive use of more refined ultrasound equipment has made it possible to understand that the presence of benign hyperplastic neck lymph nodes is common in CAT patients, especially close to the jugular vein and, less frequently, in the retrothyroid region.
Significantly, we did not find any lymph nodes suggestive for malignancy in the 106 patients with CAT included in the analysis (23 patients with CAT and coexistent thyroid nodules or pseudonodular images were excluded; see Materials and Methods). Therefore, even if we cannot definitely exclude other thyroid occult neoplasm in our series, we can assert that finding neck nodes suggestive for malignancy is infrequent in CAT.
By contrast, we found an increased number of neck nodes with long-axis diameter >10 mm and with benign reactive features (hilus more frequently present; S/L ratio always <0.5). In other autoimmune diseases (i.e., Sjögren's syndrome and systemic lupus erythematosus), Ying et al. described an increased size of cervical neck nodes (16); in a preliminary study, supraisthmian and/or juxtajugular lymph node enlargement appeared to be a very useful US sign of subacute thyroiditis with positive thyroid autoantibodies (17); moreover, the involvement of cervical lymph node in the pathogenesis of CAT is well documented (3 –5,18,19). Our findings are consistent with this well-known phenomenon. Furthermore, subdividing the nodes for each level explored, we found an increased number of neck nodes with long-axis diameter >10 mm, which was statistically significant in level II–IV lymph nodes; moreover, nodes from levels III and IV showed an increased short-axis diameter. Pathological reports from neck dissections and ultrasonographic studies assessing cervical metastases of patients with papillary thyroid carcinomas show that levels II, III, and IV are most frequently involved, revealing that drainage from the thyroid is mainly from these levels (20,21); this may partially explain our findings, demonstrating a more evident involvement of level III and IV nodes in CAT patients. We cannot confirm previous anecdotal reports suggesting a frequent involvement of the retrothyroid region (22). In five CAT patients, we found one lymph node each in the retrothyroid region (we excluded a parathyroid pathology by demonstrating a normal serum PTH and calcium). Conversely, we did not find any lymph nodes in the retrothyroid region of control subjects. However, our numbers (five retrothyroid neck nodes in CAT patients vs. zero retrothyroid neck nodes in control subjects) are too small to perform a statistical analysis.
The present study is the first one aiming at a systematic description of the sonographic pattern of cervical lymph nodes in CAT. We conclude that an increased number of benign hyperplastic neck nodes, especially in levels II, III, and IV, appears to be a characteristic sonographic finding associated with CAT.
Footnotes
Acknowledgments
This article was written with the fundamental contribution of Prof. Aldo Galluzzo (1943–2011), Chair of Endocrinology, University of Palermo, Italy. The authors dedicate the manuscript to his memory, and they wish to acknowledge their missing such a scientist with an unusual aptitude for both teaching and research activities.
Disclosure Statement
The authors declare that no competing financial interests exist.