
Abstract
Background:
Currently, there are no protein biomarkers for aggressive subtypes of thyroid carcinomas (TC) in clinical use that would allow for early detection and patient management. We hypothesized that activated leukocyte cell adhesion molecule (ALCAM or CD166) expression in thyroid tissues will reveal ALCAM to be a potential diagnostic and/or prognostic marker for TC aggressiveness.
Methods:
Forty-five benign and 158 malignant thyroid tissues were analyzed for ALCAM expression using immunohistochemistry. ALCAM expression was correlated with different subtypes and clinicopathological features of TC, as well as patient disease-free survival.
Results:
Combined membranous and cytoplasmic (total) expression of ALCAM was significantly reduced in patients with poorly/undifferentiated (aggressive) TC as compared to well-differentiated (nonaggressive) tumors (p<0.001; area-under-curve=0.865, sensitivity=82%, specificity=74%). The decreased ALCAM expression in TC correlated significantly with extrathyroidal extension, distant metastasis, and TC histotype. Notably, Kaplan–Meier survival analysis for follow-up data of 134 patients revealed significantly reduced disease-free survival for patients with TC with decreased ALCAM membranous, cytoplasmic, and total expression. Median survival of patients with decreased cytoplasmic ALCAM expression was 6 years, as compared to 13.7 years for patients with higher ALCAM expression (p<0.001).
Conclusion:
ALCAM has the potential to serve as a diagnostic and prognostic biomarker for aggressive TC. This protein can be taken forward for analysis in sera of patients with TC to determine its applicability as a minimally invasive serum biomarker for TC aggressiveness and patient disease-free survival.
Introduction
Although anaplastic thyroid carcinoma (ATC) is among the most aggressive and deadly cancers known, with a median survival of <6 months, it accounts for only 2% of all thyroid tumors (10). Thus, even though TC generally has an impressive survival rate, there exists a subset of aggressive and poorly differentiated or undifferentiated thyroid tumors that accounts for the majority of deaths attributed to this malignancy (11). The differentiation between aggressive and nonaggressive TC, therefore, becomes vitally important in clinics and presents a challenge for oncologists. It is important to identify biomarkers to accurately distinguish patients with aggressive TC from nonaggressive cases. Early stratification of thyroid malignancy with a poor clinical outcome would aid in the formulation of an effective and comprehensive treatment plan. This could help set up clear criteria for patients who require adjuvant treatment, especially 131I ablation, where discrepancy currently exists (12).
Activated leukocyte cell adhesion molecule (ALCAM or CD166) has come to the forefront of cancer markers due to its consistent dexterity in distinguishing cancers of an aggressive nature and having a poor prognosis (13 –15). The mature ALCAM molecule is a 110-kDa glycoprotein belonging to the immunoglobulin superfamily with diverse participation in cell–cell adhesion, signal transduction in intracellular signaling pathways, T-cell activation, hematopoiesis, transendothelial migration of neutrophils, inflammation, and development (14). These disparate functions strongly suggest an important role for ALCAM in tumor cell biology. ALCAM possesses the innate function to serve as an important tool aiding cancer cells to coalesce and bind to one another resulting in a mass while at the same time abetting aggressive behavior through promotion of cancer cell interactions with endothelial, nerve, and surrounding cells (13). It has been demonstrated that specifically targeting ALCAM cell adhesion in melanoma cells negates tumor cell coalition and disinhibits tumor cell migration, thus stimulating the progression of primary tumor proliferation to development of an invasive tumor front (16,17). ALCAM expression has been shown in several cancer cell lines, including prostate, lung, breast, and colon (17 –20). The association of altered ALCAM expression with cancer progression has been reported in multiple cancers, including cancers of the prostate (21), bladder (13), breast (22), colorectum (23), oral cavity (24), esophagus (25), and skin (26). ALCAM expression has also been demonstrated to predict response to chemotherapy in cervical cancer (27) and pancreatic cancer cell lines (28). Proteolysis of the extracellular domain of ALCAM by tumor necrosis factor-alpha converting enzyme (TACE) leads to its shedding (29); soluble ALCAM levels have been measured in sera of cancer patients with divergent findings (27,30,31). However, studies on ALCAM in TC patient specimens are limited (32).
The aim of this study was to investigate ALCAM expression in benign thyroid nodules and different subtypes of TC, and to determine its correlation with clinicopathological parameters and patient survival to define its applicability as a biomarker for aggressive potential and disease prognosis.
Materials and Methods
Patient specimens
The study was approved by the Mount Sinai Hospital (MSH) Research Ethics Board (REB), Toronto, Canada. Informed consent for the scientific use of anonymized patients' data and tumor tissues had been obtained from all patients (REB guideline #07-0212-E). All data were analyzed anonymously. Archived formalin-fixed paraffin-embedded (FFPE) tissue blocks from the MSH tumor bank were retrieved and reviewed by the pathologist (C.M.). The clinicopathological parameters were obtained from histopathological analyses and the clinical database (I.K.). Diagnoses at the time of surgery were used to stratify patients. Forty-five benign thyroid nodules and 158 malignant tissues were analyzed for ALCAM expression. Of the malignant cases, there were 13 ATC, 4 poorly differentiated follicular TC (PDFTC), 6 poorly differentiated PTC (PDPTC), 77 classic PTC, 44 follicular variants of PTC, 9 oncocytic (Hürthle cell) variant PTC, and 5 tall-cell variant PTC. Benign nodules were obtained from patients with multinodular goiters, Graves' disease, Hashimoto's thyroiditis, or hyperplastic nodules. The age of patients ranged from 16 to 85 years, median 47 years, including 47 males and 156 females.
Immunohistochemical analysis in human thyroid tissues
FFPE human TC and benign tissue sections (4-μm thickness) were deparaffinized in xylene and hydrated with graded alcohol series as described earlier by us (33). For antigen retrieval, slides were immersed in a Tris–EDTA buffer (10 mM Tris base, 1 mM EDTA, and 0.05% Tween 20, pH 9.0) and pretreated in a 900-watt microwave oven for 30 minutes (20 minutes full power, then 10 minutes half power). The liquid boiled throughout the whole duration of antigen retrieval. All further incubations were conducted at room temperature. The VECTASTAIN rapid protocol was used. The slides were incubated with 10% blocking serum for 20 minutes consisting of horse serum for anti-mouse secondary antibodies. After blocking the nonspecific binding sites, the sections were incubated with anti-human antibody ALCAM, 1:200 dilution (Abcam, Cambridge, MA) for 1 hour. Tissues were then treated with 3% H2O2 in TBS for 10 minutes to block the endogenous peroxidase activity and subsequently incubated with biotinylated horse anti-mouse secondary antibody for 10 minutes. The sections were finally incubated with VECTASTAIN Elite ABC Reagent (Vector Labs, Burlingame, CA) for 10 minutes, and diaminobenzidine was used as the chromogen. Negative control tissues were incubated with biotinylated horse anti-mouse secondary antibody following the same protocol.
Evaluation of immunohistochemistry
The immunostaining scores were based on percentage positivity and staining intensity. Sections were scored as positive if epithelial cells showed immunoreactivity in the membrane and/or cytoplasm when observed by two evaluators (S.C., and I.K.). Percentage positive scores were assigned according to the following scale: 0,<10% cells; 1, 10%–30% cells; 2, 31%–50% cells; 3, 51%–70% cells; and 4,>70% cells. Staining intensity was scored semiquantitatively as follows: 0, none; 1, mild; 2, moderate; and 3, intense. A total score for each membrane and cytoplasmic staining was then obtained (ranging from 0 to 7) by adding the percentage positivity scores and intensity scores for each section. Average scores of the two evaluators were used for subsequent analyses. To assess the total expression of ALCAM in the tissues, we added the membrane and cytoplasm scores to obtain a total score ranging up to 14. Box plots were used to determine the distribution of total score of membranous, cytoplasmic, and total expression for ALCAM.
Statistical analyses
The immunohistochemical data were subjected to statistical analysis using SPSS 20.0 software (SPSS, Inc., Chicago, IL). We report frequencies for categorical variables. Area-under-curve (AUC), sensitivity, and specificity were determined using receiver-operating characteristic (ROC) analysis. Based on sensitivity and specificity values for ALCAM, cutoffs of ≥3, ≥4.5, and≥7 were defined as the positive criteria for immunoreactivity of membrane, cytoplasmic, and total ALCAM expression, respectively, for statistical analysis. The relationships between ALCAM expression (positive/negative) and clinicopathological parameters were tested using Chi-square and/or Fischer's exact test. Two-sided p-values were calculated, and p<0.05 was considered to be significant. Odds ratio (OR) and 95% confidence interval (CI) were also calculated. Kaplan–Meier survival plots were used to determine correlation of ALCAM expression and disease-free survival in patients with TC. Hazard ratios (HR) were also calculated. Cox-regression (multivariate) analysis was performed to determine the prognostic potential of ALCAM expression in comparison with known clinical and pathological parameters.
Results
Immunohistochemical analysis of ALCAM was carried out to determine differences in its subcellular localization and levels of expresssion, including total expression, in benign thyroid tissues and different subtypes of TC in a large patient cohort. ALCAM expression in relation to the patients' clinicopathological characterisitics is listed in Table 1. Representative tissue sections showing the immunostaining pattern of ALCAM in benign thyroid nodules and several variants of TC are shown in Figure 1. Intense membrane and cytoplasmic staining of ALCAM was observed in the stage I classic PTC compared to the benign tissues (Fig. 1a, b), whereas decreased membrane expression was observed in the stage IV PTC (Fig. 1c). No membrane staining and very mild cytoplasmic staining were seen in ATCs (Fig. 1d). The PDPTC and PDFTC showed reduced membrane and cytoplasmic staining (Fig. 1e, f). Differences in patterns of staining were observed in the PTC variants.The tall-cell variant PTC displayed strong membranous and moderate cytoplasmic staining (Fig. 1g); the follicular variant showed decreased postivity and mild membrane staining with mild-to-moderate cytoplasmic staining (Fig. 1h), while the oncocytic (Hürthle cell) variant showed moderate cytoplasmic staining and mild membranous staining (Fig. 1i). Comparison of the staining patterns of histological variants of TC revealed significant differences in levels of ALCAM staining intensity and percentage positivity among the different groups for both total and subcellular ALCAM expression; membrane p=0.007, cytoplasm p<0.001, and total p<0.001 (Table 1).
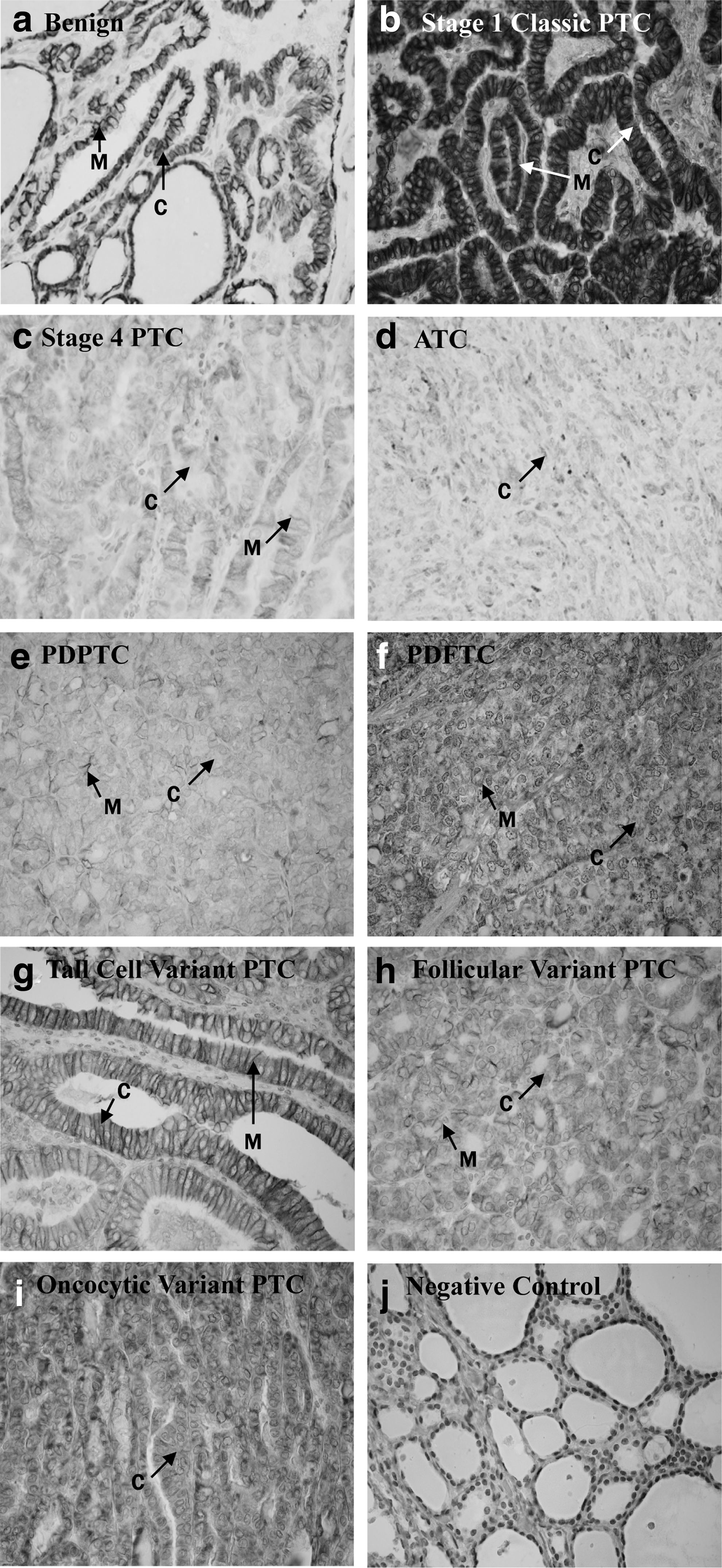
Immunohistochemical analysis of activated leukocyte cell adhesion molecule (ALCAM) in human benign and thyroid carcinoma (TC) tissues. Paraffin-embedded sections of benign thyroid nodules and different subtypes of TCs were immunostained using an anti-CD166 monoclonal antibody as described in Materials and Methods. The photomicrographs of representative immunostained tissues depict
Statistical significance (p<0.05) is indicated by boldface.
Poorly/undifferentiated group includes PDPTC, PDFTC, and ATC
OR, odds ratio; CI, 95% confidence interval; TC, thyroid carcinoma; ATC, anaplastic thyroid carcinoma; PDFTC, poorly differentiated follicular TC; PDPTC, poorly differentiated PTC.
Membrane, cytoplasmic, and total ALCAM expression was significantly decreased in TC as compared to benign tissues (p<0.001). ALCAM expression was also decreased in TC cases with distant metastasis. Cytoplasmic ALCAM was positive in three of seven distant metastasis cases, while membranous ALCAM was positive for two of seven cases. Decreased cytoplasmic expression was significantly associated with extrathyroidal extension (p=0.002, Table 1).
To evaluate the ability of ALCAM to serve as a marker for aggressive TC, the malignant cases were subdivided into two groups according to histological grade: well-differentiated (nonaggressive) and poorly/undifferentiated (aggressive) TC (Fig. 2a). The poorly/undifferentiated group includes PDPTC, PDFTC, and ATC. Significantly decreased membrane (p<0.001), cytoplasmic (p<0.001), and total ALCAM (p<0.001) expression was observed in the aggressive compared to the nonaggressive group. Using ROC analysis, AUC for total ALCAM expression was 0.865 (Fig. 2b), and the sensitivity and specificity were 82% and 74%, respectively (OR=15.38 [CI=5.43–43.54]). The AUC values were 0.790 and 0.802 for membrane and cytoplasmic ALCAM expression, respectively. Membrane expression sensitivity and specificity were 62.2% and 78.3%, respectively, and cytoplasmic expression sensitivity and specificity were 80% and 69.6%, respectively.
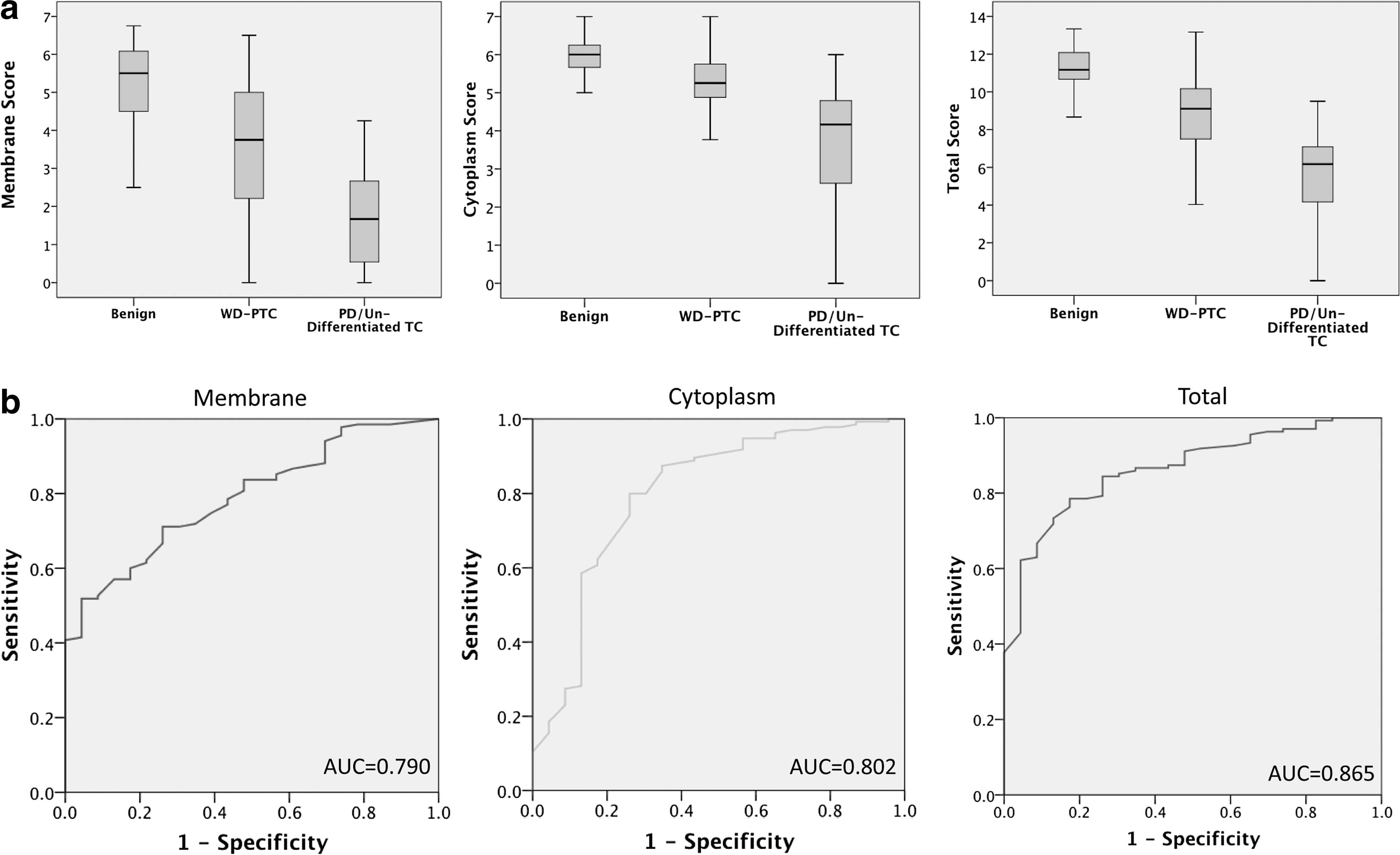
ALCAM expression is decreased in poorly/undifferentiated TC tissues. Categories include benign nodules, well-differentiated PTC (WD-PTC), and PDPTC or undifferentiated TC. The poorly/undifferentiated group includes PDPTC, PDFTC, and ATC.
Kaplan–Meier survival analysis of follow-up data of 134 patients with TC showed significantly reduced disease-free survival for patients with TC with decreased ALCAM membrane expression (p=0.016, median survival 8.3 years, range 0.2–11.8 years), as compared to a median survival of 13.7 years for those with higher ALCAM membrane expression (Fig. 3). Similarly, TC patients with decreased ALCAM cytoplasmic expression had reduced disease-free survival (p<0.001, median survival 6 years) as compared to a median survival of 13.7 years for those with higher ALCAM cytoplasmic expression (Fig. 3). Total ALCAM expression emerged as a prognostic marker; overall decreased expression correlated with poor prognosis (p=0.002), with a median survival of 7.3 years for patients with decreased expression as compared to 13.5 years for patients with higher ALCAM expression (Fig. 3).
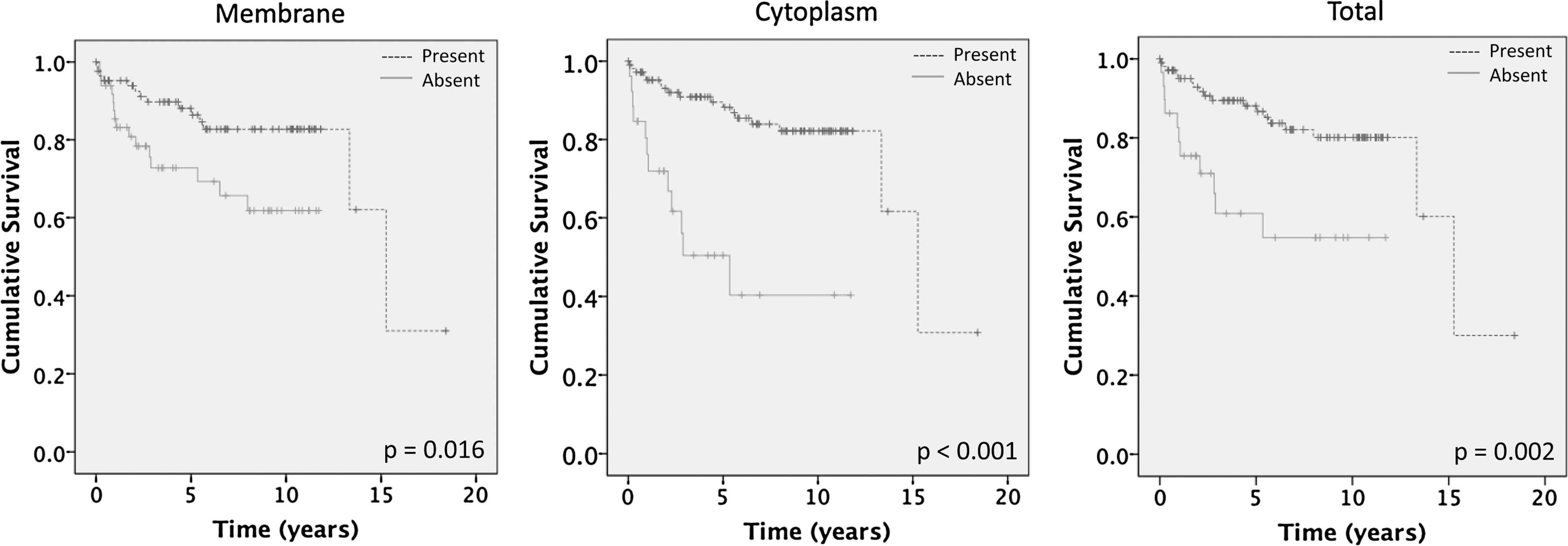
Decreased ALCAM expression is associated with reduced disease-free survival. Kaplan–Meier estimation of cumulative proportion of disease-free survival was assessed. Significantly reduced disease-free survival for TC patients with decreased ALCAM membrane expression (p=0.016, median survival 8.3 years), as compared to patients with higher ALCAM membrane expression (median survival 13.7 years). TC patients with decreased cytoplasmic ALCAM expression also had reduced disease-free survival (p<0.001, median survival 6 years) compared to patients with higher cytoplasmic ALCAM (median survival 13.7 years). Decreased total ALCAM expression was associated with reduced disease-free survival; median survival 7.3 years compared to 13.5 years for higher total ALCAM expression (p=0.002). Absence of ALCAM expression defines immunohistochemistry (IHC) scores below the respective cutoffs, whereas presence of ALCAM represents IHC scores above the respective cutoffs.
Cox-regression (multivariate) analysis was performed to determine the prognostic potential of ALCAM expression in comparison to clinical and pathological parameters that were independently significant in Kaplan–Meier analysis. The parameters tested were ALCAM staining (membrane, cytoplasmic, and total), age, tumor size, AJCC stage (stage I/II vs. III/IV) (8), histological grade, extrathyroidal extension, as well as ALCAM staining combined with each of the clinicopathological parameters. Distant metastasis was not used as a parameter in this analysis, because by definition, recurrence included presence of local or distant recurrence (distant metastases); inherently, this would be the most significant predictor of disease-free survival. The most significant parameters for prognosis were combined cytoplasmic ALCAM expression and histological grade (p<0.001, HR=22.78 [CI=5.15–100.71]), and extrathyroidal extension (p=0.002, HR=4.70 [CI=1.74–12.69]).
Discussion
Our study demonstrates the correlation of ALCAM expression with TC aggressiveness. Using tissue specimens from a large cohort of patients, including those with benign nodules, several variants of PTC, and aggressive features of TC, we demonstrate ALCAM expression to be negatively correlated with increased tumor aggressiveness. Namely, we show that decreased membrane, cytoplasmic, and total ALCAM expression is associated with poor differentiation, presence of metastasis, and extrathyroidal extension, all of which are characteristic features of aggressive TC. Most importantly, our data demonstrate decreased membrane, cytoplasmic, and total ALCAM expression to be associated with decreased disease-free survival, underscoring its applicability as a prognostic marker for TC.
In support of our findings, ALCAM downregulation has been reported in breast cancer and correlated with poor prognosis, recurrence, and death (22), as well as in high-grade prostate cancer (21). A similar association of high ALCAM expression with favorable prognosis was reported in chemotherapy-treated breast cancer patients, which might be explained by its influence on apoptosis (34,35). Decreased or lost ALCAM membrane expression was also associated with poorer outcome in epithelial ovarian cancer, whereas cytoplasmic expression of ALCAM was found in these patients (36). In contrast, elevated ALCAM expression has been correlated with the vertical-phase proliferation in melanomas (26) and reduced survival or poor prognosis in esophageal squamous cell carcinoma (31), oral cancer (24,37), pancreatic cancer (38), and colorectal cancer (23,39). Collectively, these reports underscore the prognostic potential of ALCAM in human cancers, pointing to divergent roles played by ALCAM in progression of different tumor types. Thus, in-depth understanding of the biological roles of ALCAM is needed to explain the divergent variations in ALCAM expression reported in human cancers.
The molecular basis to explaining the diverse roles that ALCAM plays in TC progression and aggressiveness might lie in the critical triggering event that initiates the change of focus from homotypic adhesion to heterotypic tumor cell interaction with surrounding cell types. The clinical relationship of membrane ALCAM loss with aggressiveness of TC may relate to the process of proteolytic cleavage of ALCAM by ADAM/TACE and its shedding. The experimental evidence for this rationale has been provided in a recent study that addressed the role of ALCAM in thyroid tumor biology (32). ALCAM was detected in proteomic analysis of cell lysates from TC cell lines (TPC-1 and SKOV-3) and in their conditioned media, as well as in four PTCs and two medullary TCs by immunostaining (32). These authors demonstrated that the extracellular surface domain of ALCAM is cleaved by metalloproteinases ADAM17/TACE, which subsequently translocates to the cytoplasm, where it facilitates aggressive transformation of tumor cells. In the initial stages of tumor formation, the cells must be able to attach to each other; therefore, adhesion molecules are required, and this was observed in our study with intense ALCAM membrane staining in the nonaggressive PTC. As the cancer progresses and metastasis is initiated and tumor cells originally attached to a particular organ begin to spread to distant sites, cells must detach from the primary tumor, and therefore the expression of adhesion molecules are altered to facilitate this process. Herein, ALCAM membrane expression was absent, with mild-to-moderate cytoplasmic expression in the aggressive TC cases. The increased TACE-mediated proteolysis of ALCAM in aggressive TC could account for the loss of membrane ALCAM in these tumors, and consequent relocalization from the cell membrane to the cytoplasm might ultimately enhance the migratory potential of malignant cells facilitating metastasis. The involvement of TACE in increasing the motility of PTC cells (TPC-1) has been reported (32). The loss of ALCAM by proteolysis from the membrane might likely be accompanied by increased levels of cytoplasmic ALCAM. However, in our study, we also observed reduced cytoplasmic ALCAM levels in the most aggressive TC, such as ATC. This might be explained by the recently reported promoter methylation that mediates ALCAM silencing, thereby consequently reducing protein expression in these tumors, as was shown in breast cancer (15).
The limitations of this study include the lack of testing ALCAM expression cutoffs on a set of tissues independent from those used to create these cutoffs. Using designated cutoffs from this analysis in another cohort of patients would determine the reproducibility and reliability of this marker. The number of aggressive TC cases was limited in this study. Future aims include the expansion of the study to analyze ALCAM expression in a larger population of patients with aggressive TC. Furthermore, ALCAM expression in fine-needle aspiration biopsies can be assessed to determine if it improves the diagnostic accuracy of this method.
In conclusion, we propose ALCAM to be a potential clinically useful diagnostic and prognostic biomarker for TC aggressiveness. Furthermore, future analysis of ALCAM expression in sera of patients with TC would assess the clinical applicability of ALCAM as a serum-based biomarker for minimally invasive assays to provide earlier detection of aggressive TC with effective long-term patient management.
Footnotes
Acknowledgments
Financial support for this work came from the Mount Sinai Foundation of Toronto, Da Vinci Gala Fundraiser, Alex and Simona Shnaider Chair in Thyroid Cancer, Canadian Institutes of Health Research (CIHR) for CIHR Chair in Advanced Cancer Diagnostics, The George Knudson Oakdale Golf Fund Raiser, and the Mount Sinai Hospital Department of Medicine Research Fund.
Disclosure Statement
The authors declare that they have no competing interests.