
Abstract
Background:
Columnar cell variant is a recognized rare variant of papillary thyroid carcinoma (PTC) that has an uncertain clinical course. This variant has two subvariants, and one is regarded as a more aggressive form in comparison to the more common classical and follicular variants. These tumors have morphological resemblance with endometrial or colonic adenocarcinoma. CDX2, a transcription factor of the caudal homeobox family, plays a key role in intestinal development and differentiation, and it is widely used as a marker to detect adenocarcinomas of intestinal and colonic origin. CDX2 has been rarely reported in PTC.
Methods:
We studied 10 cases of columnar cell variant of PTC (CCV-PTC). The histological, architectural, and cytological features fulfilled the diagnostic criteria of the CCV-PTC, as defined by the current World Health Organization classification. Ten patients (six men and four women) ranging in age from 32 to 90 years (mean, 58.3 years) presented with tumors classified as indolent (four cases) or aggressive (six cases); three harbored a BRAF V600E mutation. All cases were β-catenin negative. The Ki-67 proliferative index was up to 50%. All cases were thyroid transcription factor-1–positive. Using paraffin-embedded blocks, immunohistochemistry for CDX2 was performed to evaluate the reactivity of this antibody to this variant of PTC.
Results:
Nuclear positivity for CDX2 was detected in one out of the 10 cases studied (10%); the other nine cases did not express CDX2.
Conclusion:
Only one of our cases showed nuclear positivity for CDX2. Therefore, our study failed to confirm it as a marker for CCV-PTC. The absence of CDX2 in the majority of the cases does not support the theory of CDX2 playing a role in the intestinal phenotype of these tumors.
Introduction
CCV-PTC is defined as being composed of pseudostratified columnar cells, some of which may contain supranuclear and subnuclear cytoplasmic vacuoles (2). This morphology can resemble tubular glands, sometimes creating a challenge when present as metastatic deposits (5). In these cases, immunohistochemistry (IHC) becomes a very important tool for the proper identification and classification of these tumors.
CDX2 is a transcription factor of the caudal homeobox family (6). It plays a key role in intestinal development and differentiation. Its mRNA is expressed in normal human small intestinal, colonic, and rectal epithelium. It is usually used as a marker of colonic differentiation as well as other types of intestinal malignancies.
CDX2 has been rarely reported in PTC. We studied 10 cases of CCV-PTC for CDX2 expression.
Materials and Methods
Ten cases of columnar cell carcinoma were identified from 10 patients with PTC seen over the last 10 years by one of the authors. These consisted of nine surgical specimens and one autopsy specimen. Patients ranged in age from 32 to 90 years, and consisted of six men and four women. The clinical history and pathology material were reviewed, and all cases fulfilled the current World Health Organization classification criteria for CCV-PTC, including neoplastic cells with elongated nuclei, hyperchromasia, supranuclear and/or subnuclear cytoplasmic vacuolization, and papillary, follicular, trabecular, and/or solid growth patterns (2,7,8). All neoplasms evaluated had ∼95% of typical columnar cell histomorphology. They all tested positive for thyroid transcription factor-1 (TTF-1) by IHC.
The tumors were then further classified as clinically indolent or aggressive based on morphology, clinical features, and outcome. The indolent ones are typically seen in younger female patients and tend to be well-circumscribed and small, while the aggressive forms occur in older male patients and are usually ill-defined, large, and tend to exhibit regional and distant metastasis (3).
The specimens were fixed in 10% neutral-buffered formalin, dehydrated, and embedded in paraffin resin. In all cases, routine and immunohistochemical stains for CDX2 (mouse monoclonal to CDX2 [CDX2-88], 1:50 dilution; Biogenex Laboratories, San Ramon, CA), cyclin D1, β-catenin, Ki-67, estrogen receptor (ER), and progesterone receptor (PR) were performed.
In nine of the 10 cases, mutational analysis of the BRAF gene was performed on formalin-fixed paraffin-embedded tissue, as previously described (9 –11). In summary, unstained 5-μm sections were prepared from blocks with the areas rich in the cells of interest. Those areas were scraped into a microcentrifuge tube using a clean scalpel blade. Slide scrapings were deparaffinized by serial extractions with xylenes and ethanol and allowed to air-dry at room temperature. DNA was extracted using the Qiagen minikit in accordance with the manufacturer's recommendations (Qiagen, Valencia, CA). Cultured cells were trypsinized, collected by centrifugation, and washed with phosphate-buffered saline (PBS) twice. Genomic DNA from the cell lines was extracted using the same procedure. Genomic DNA from paraffin-embedded specimens was prepared from four to six 10-m-thick sections. The sections were deparaffinized and gradually dehydrated and air-dried. Polymerase chain reaction (PCR) amplification was performed using standard methods. After an initial denaturing hold at 95°C for 60 sec, 250 ng of purified tumor DNA was subjected to 42 cycles of PCR (94°C for 30 sec, 56°C for 30 sec, 72°C for 30 sec) using the High Fidelity PCR system (Roche, Indianapolis, IN), followed by a final extension hold at 72°C for 7 min. Following the process, mutation screening was performed by denaturing high-performance liquid chromatography (D-HPLC). Finally, all D-HPLC–detected mutants were bidirectionally sequenced on an ABI 310 sequencer using the Big Dye Terminator kit (Applied Biosystems, Inc., Foster City, CA). Novel D-HPLC–detected mutants were confirmed by three methods: (i) reamplification of the exon and repeat D-HPLC analysis; (ii) reextraction of DNA from the tumor tissue, reamplification, and repeat D-HPLC analysis; and (iii) bidirectional sequence analysis after each analysis by D-HPLC. Where available, nonmalignant tissue from cases with BRAF mutations was analyzed using the procedure outlined above.
Results
By hematoxylin and eosin (H&E) staining, all cases fulfilled the current World Health Organization classification criteria for CCV-PTC, including neoplastic cells with elongated nuclei, hyperchromasia, and supranuclear and/or subnuclear cytoplasmic vacuolization. They all had a diffuse pattern of involvement by this tumor (Figs. 1 and 2).
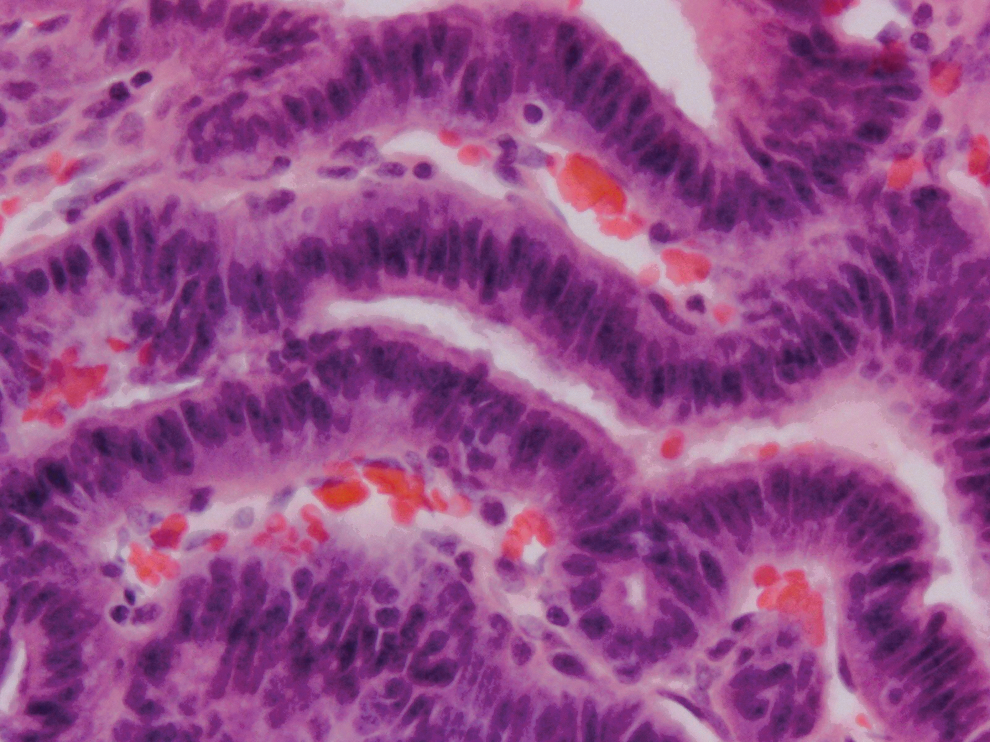
Hematoxylin and eosin (H&E) histology showing a case of columnar cell variant of papillary thyroid carcinoma (CCV-PTC), demonstrating pseudostratified columnar cells and hyperchromasia. Magnification, 400×. Color images available online at
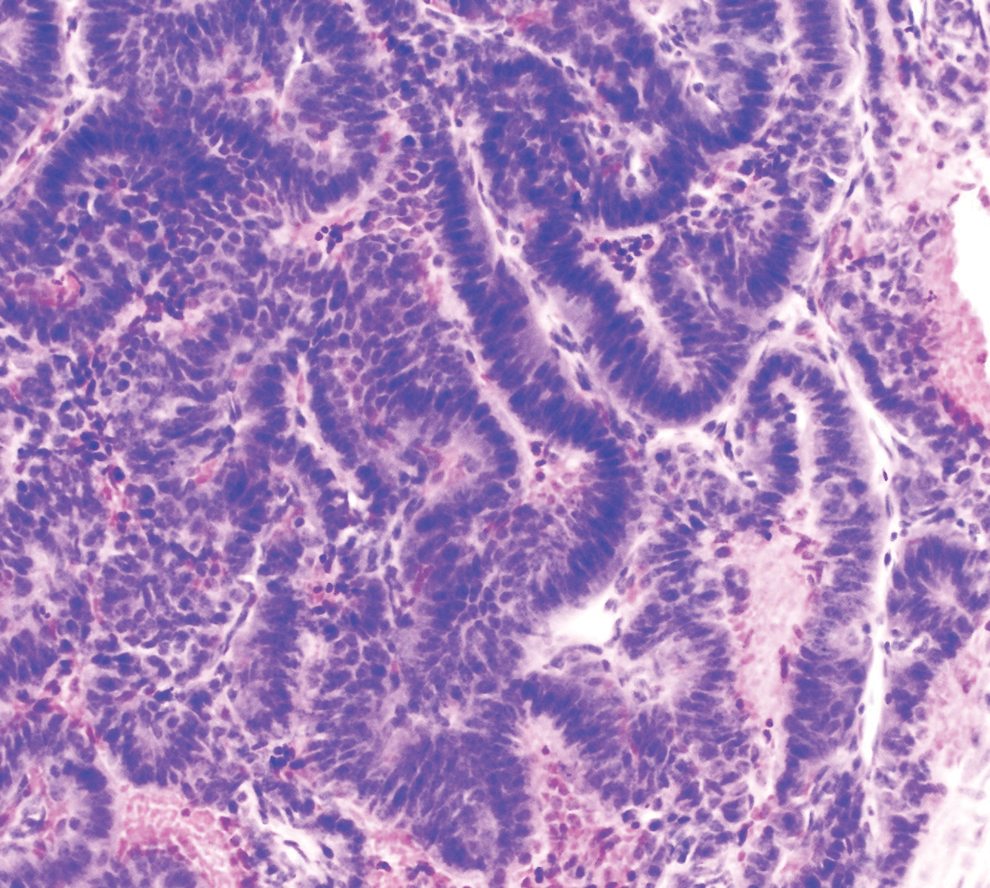
H&E-stained slide of CCV-PTC with trabecular pattern of growth, elongated nuclei, and the characteristic subnuclear and supranuclear vacuolization. Magnification, 200×. Color images available online at
CDX2 nuclear positivity by IHC was detected in only one out of the 10 (10%) cases of CCV-PTC studied. The other nine cases (90%) showed no reaction to CDX2 (Table 1).
Pathological TNM stage according to AJCC 7th edn. (12).
Nuclear.
ER, estrogen receptor; PR, progesterone receptor; encap, encapsulated; carc, carcinoma; min, minimal; inv, invasion; ETE, extrathyroidal extension; +, positive; −, negative; circ, circumscribed; FTC, follicular thyroid carcinoma; met, metastasis; LNs, lymph nodes; PTC, papillary thyroid carcinoma.
The CDX2-positive case (case 1; Fig. 3) belonged to a 32-year-old woman with an indolent CCV-PTC. The mass was 4 cm, encapsulated, and minimally invasive with lymphovascular invasion, and there was no extrathyroidal extension. It was staged as T2 based on the American Joint Committee on Cancer (AJCC) TNM staging system (12). It had a wild type BRAF and was also positive for ER and PR by IHC.

CDX2-positive CCV-PTC case. Note the moderate to strong nuclear staining of tumoral cells, and adjacent endothelial cells as negative internal control. This was the only case among 10 others that was immunoreactive for this marker in our study. Magnification, 400×. Color images available online at
Of the CDX2-negative cases (cases 2–10), six cases were of the aggressive type (cases 5–10), and three cases were of the indolent type (cases 2–4). The patients' ages in this group ranged from 35 to 90 years. These cases ranged in size from 1.3 to 11.5 cm (mean: 4.9; median: 5). Three of the CDX2-negative cases were pT1b (cases 2–4), three were pT3 (cases 5, 6 and 9), and three were pT4a (cases 7, 8 and 10; Table 2). The other markers were as follows: ER was positive in six cases (cases 2, 3, 6–8, and 10); PR was positive in four of these cases (cases 2, 3, 6, and 8). Six of these cases showed the wild type BRAF codon at position 600 (cases 2, 3, 5, 6, 9, and 10), and three had the BRAF V600E mutation (cases 4, 7, and 8).
F, female; M, male; Tx, thyroidectomy; TTx, total Tx; RAI, radioactive iodine.
Discussion
The incidence of PTC has increased over the past 30 years (2). More than 95% of the cases are well differentiated with an excellent prognosis. However, of the multiple variants of PTC, a small subset of these tumors may progress to a more aggressive behavior, presenting with a higher histologic grade, extracapsular spread, large size, and sometimes even with distant metastases (4). These aggressive variants include the columnar cell variant of PTC, the tall cell variant, the diffuse sclerosing variant, and the newly described tumor with hobnail cell features (13).
CCV-PTC was originally described by Evans in 1986 (7). He described two cases of this variant of PTC, which were characterized by tall columnar cells that were in excess of those seen in the already described tall cell variant of PTC. Both of those cases showed an aggressive tumor behavior, which led to the patient's death within two years.
CCV is a rare tumor representing only 0.15% to 0.2% of all PTC (3). In 2011, Chen et al. reported on 48 cases of CCV throughout the literature (3). Of those cases, 20 were clinically indolent (2 males and 18 females), and 23 were aggressive (13 males and 10 females). Of those who had follow-up, almost all of the patients with indolent tumors (18 out of 19) were alive or without disease 9 months to 22 years after diagnosis. Of the patients with aggressive tumors, more than half (12 out of 20) died of their disease 7–126 months after diagnosis, and another five were alive with residual disease.
The classic morphology that defines CCV includes columnar cells with pseudostratified hyperchromatic nuclei and subnuclear vacuolization (similar to that seen in early secretory endometrium). The follicles can appear elongated and empty (2). The typical nuclear features of classic PTC are seen only focally in some of these tumors. Multiple growth patterns can be seen, even within the same tumor, including papillary, solid, follicular, and trabecular parts. In order to be classified as CCV-PTC, there has to be a minimal percentage of columnar cells throughout the tumor, which ranges from 30% to 50% depending on the study (4,14), with the largest series showing >70% of columnar cells in each of the tumors (14,15). Our study demonstrated the characteristic columnar features in ∼95% of cells in all cases.
CCV-PTC can sometimes represent a diagnostic dilemma, particularly when present as metastatic deposits in cervical lymph nodes or in distant organs. They can be easily confused with other kind of adenocarcinomas, particularly of colonic origin (5,14). To complicate things even further, CCV-PTC has variable thyroglobulin immunoreactivity; however, TTF-1 is typically positive. Therefore, this tumor should be kept in mind when dealing with this kind of differential diagnosis.
No definitive relation between Ki-67 and biological behavior of tumors was observed in our study. As illustrated in Table 1, we have examples of very aggressive carcinomas with a low proliferative index (case 5, Ki-67 <5% on a patient with lymph nodes and multiple organ metastases), as well as indolent tumors with high proliferative marker expression (case 3, Ki-67 30%, well-circumscribed tumor with no clinical and radiological evidence of nodal or systemic metastasis). Controversial results are found in the literature on this aspect. Hirokawa et al. (16) showed that proliferation markers were associated with poor prognosis in CCV-PTC, while in classical PTC, Tallini et al. (17) demonstrated that no significant association could be seen between cellular proliferation and clinicopathologic parameters such as age, sex, tumor size, extrathyroidal extension, vascular invasion, lymph node metastases, distant metastases, tumor stage, and survival rate.
With regard to β-catenin and cyclin D1 expression in these tumors, Jingdong et al. (18) state that β-catenin is a well-known regulator of cyclin D1, and this interaction appears important as PTCs metastasize and cyclin D1 is an important marker in both primary PTC and nodal metastases. In another study that evaluated these markers in papillary thyroid microcarcinomas (PMC), cyclin D1 expression was significantly associated with tumor size and lymph node metastases (19). However, according to our data, no discernible correlation between cyclin D1, β-catenin, and Ki-67 labeling index was identified, suggesting that other factors may promote further malignant growth.
CDX2 is a transcription factor of the caudal homeobox family. They are homeobox genes necessary for intestinal organogenesis, and encode for nuclear transcription factors involved in proliferation and differentiation of intestinal cells (20). CDX2 plays a key role in intestinal development and differentiation (6). Its role in the development of intestinal cancer has not been elucidated yet; it has been proposed to play a role as a tumor suppressor, although it has not been reported to be mutated in most adenocarcinomas (6,20). CDX2 is supposed to be a highly sensitive and specific marker of colorectal adenocarcinomas (6,20,21), as well as some neoplasms with intestinal phenotypic differentiation. In addition, it has also been reported as being positive in mucinous ovarian adenocarcinomas and primary adenocarcinomas of the urinary bladder (21), as well as in certain subtypes of germ cell tumors of the testis (22). A recent study suggests that CDX2 could be a positive marker for CCV-PTC (23).
In our study, CDX2 was positive in only one out of 10 cases of CCV-PTC. Therefore, we failed to confirm it as a marker for CCV-PTC. The positive case was not different clinically or morphologically from the other nine cases.
In conclusion, CDX2 can be occasionally expressed in a variety of neoplasms, and only rarely in thyroid CCV-PTC. For that reason, this marker should not be considered as a diagnostic tool for this rare variant of thyroid papillary carcinoma. However, it may be useful to identify metastasis from colonic carcinomas to the thyroid in an appropriate clinical and immunopathological setting.
Footnotes
Acknowledgments
The authors thank Dr. R.V. Lloyd (University of Wisconsin-Madison), Dr. J.H. Chen (CellNetix Pathology and Laboratory) and Dr. W.C. Faquin (Massachusetts General Hospital) for sharing their cases with us.
Author Disclosure Statement
No competing financial interests exist.