
Abstract
Background:
Thyroid disease during pregnancy may be associated with increased risk of various pregnancy complications. It is known that serum thyrotropin (TSH) is suppressed because of the increased hormone production induced by human chorionic gonadotrophin (hCG) in early pregnancy, and that higher hCG levels in twin pregnancies may cause a more pronounced physiologic suppression. The recognition of this phenomenon is important in order to avoid unnecessary concerns and to correctly establish the diagnosis of overt thyroid disease in twin pregnancies. The aim of this study was to establish reference ranges of maternal serum TSH and free thyroxine (FT4) at gestational weeks 11–13 in twin pregnancies.
Methods:
This is a case series of 177 dichorionic and 58 monochorionic twin pregnancies with normal outcomes, and 19 monochorionic pregnancies complicated by severe twin–twin transfusion syndrome. Maternal serum concentrations of TSH, FT4, antithyroperoxidase, and antithyroglobulin antibodies were measured at gestational weeks 11–13. The measured TSH and FT4 were converted to multiple of median (MoM) of normal singleton pregnancies and MoM values in the different groups were compared.
Results:
In the antibody-negative twin pregnancies with normal outcomes, compared to singletons, serum TSH MoM was lower (median 0.62 [interquartile range [IQR 0.16–1.18] vs. 1.01 [IQR 0.61–1.51]; p<0.0001), FT4 MoM was not significantly different (median 0.98 [IQR 0.91–1.08] vs. 0.99 [IQR 0.91–1.09]; p=0.975), and free β-hCG MoM was higher (median 1.91 [IQR 1.33–2.59] vs. 0.98 [IQR 0.66–1.50]; p<0.0001). In the antibody-positive group (n=37), compared to the negative group (n=198), the median TSH was higher, but FT4 and free β-hCG were not significantly different. In the twin–twin transfusion syndrome group, compared to normal twin pregnancies, TSH, FT4, and free β-hCG were not significantly different.
Conclusion:
In twins, compared to singleton pregnancies, TSH is lower but FT4 is not significantly different. These reference ranges of thyroid hormones in twins can form the basis for the study of early thyroid function in pathological pregnancies and the investigation of the consequences of overt and subclinical hypothyroidism on twin pregnancy outcome.
Introduction
A screening study of thyroid function in normal singleton pregnancies at gestational weeks 11–13 established that maternal serum TSH increases with gestational age, whereas FT4 decreases, and both are lower in women of African origin than in Caucasians (11). Serum FT4 decreases with maternal age, but TSH does not change significantly; serum TSH increases with body mass index (BMI), whereas FT4 decreases (11). It is important to adjust the measured TSH and FT4 levels for these variables before comparing results with pathological pregnancies. In women with antithyroid antibodies, compared to the antibody-negative group, TSH is higher and FT4 is lower. A study in 132 twin pregnancies, compared to 13,599 singletons, reported that serum TSH is lower (12). This has been attributed to the higher levels of hCG in twins.
The aims of this study were to establish a reference range of serum TSH and FT4 at gestational weeks 11–13 in dichorionic and monochorionic twins, including those that later developed severe twin–twin transfusion syndrome (TTTS), to determine whether chorionicity or developing severe TTTS affects thyroid function, and to compare the values to singleton pregnancies. In addition, this study determined TSH and FT4 levels in antibody-positive twin pregnancies with normal outcomes.
Materials and Methods
This is a case series of women with twin pregnancies evaluated at their first routine hospital visit during pregnancy. At this visit, which was held at gestational weeks 11–13, we recorded maternal characteristics and performed an ultrasonography scan to confirm gestational age by measuring the fetal crown-rump length (13) of the bigger twin, determined chorionicity by assessing the presence or absence of the lambda sign (14), diagnosed any major fetal abnormalities, and measured fetal nuchal translucency thickness and maternal serum free β-human chorionic gonadotropin (β-hCG) and pregnancy-associated plasma protein-A as part of screening for aneuploidies (15). Additionally, blood was collected for research, and the separated plasma and serum were stored at −80°C for subsequent biochemical analysis. Written informed consent was obtained from the women agreeing to participate in the study aimed at predicting adverse pregnancy outcomes that involve testing the serum/plasma for various biomarkers. The study was approved by the King's College Hospital Ethics Committee.
Maternal characteristics recorded were age, racial/ethnic origin (Caucasian, African, South Asian, East Asian, and mixed) and method of conception (spontaneous or assisted conception requiring the use of ovulation-inducing drugs). Maternal weight and height were measured, and the BMI was calculated in kg/m2. Maternal serum pregnancy-associated plasma protein-A and free β-hCG were measured using the Delfia Express analyzer (PerkinElmer, Waltham, MA), and the measured concentration was converted to multiples of the expected normal median (MoM) as previously described (15).
Data on pregnancy outcomes were collected prospectively from the hospital maternity records or the general medical practitioners of the women. The inclusion criteria were twin pregnancies with live fetuses at 11–13 weeks and delivery of live births at or after 33 weeks of gestation during March 2006 to March 2011. We excluded cases with a maternal history of hypothyroidism, hyperthyroidism, or diabetes mellitus, fetal abnormalities, pre-eclampsia, and small-for-gestational-age neonates with a birth weight below the fifth percentile of our normal range for gestation (16) since there is some evidence that thyroid dysfunction is associated with adverse pregnancy outcomes (1 –3). These criteria were met by 235 cases with available serum for analysis (normal group). Additionally, we examined 19 cases that developed severe TTTS necessitating endoscopic laser surgery (17). None of the women suffered from hyperemesis gravidarum at the time of testing.
Sample analysis
The maternal serum concentrations of FT4, TSH, antithyroperoxidase antibodies (anti-TPO), and antithyroglobulin antibodies (anti-Tg) were measured retrospectively by immunoassays using direct, chemiluminometric technology (Siemens Advia Centaur assays; Siemens Healthcare Diagnostics Ltd., Surrey, United Kingdom). A study that examined the effects of storage on serum concentrations of thyroid hormones and TSH found that they are relatively stable independent on whether they are stored at room temperature, refrigerated, or frozen (18). The minimum detectable concentrations of FT4, TSH, anti-TPO, and anti-Tg were 1.3 pmol/L, 0.01 mIU/L, 15 U/mL, and 30 U/mL, respectively. The intra-assay coefficients of variation were 4.69%, 2.31%, and 2.22% at FT4 concentrations of 6.1, 13.9, and 39.9 pmol/L, respectively; 2.48%, 2.44%, and 2.41% at TSH concentrations of 0.74, 5.65, and 18.98 mIU/L, respectively; 7.93%, 4.54%, and 6.26% at anti-TPO concentrations of 1.70, 10.01, and 14.95 U/mL, respectively; and 5.5% and 2.9% at anti-Tg concentrations of 62 and 333 U/mL, respectively. Only if the serum concentrations of anti-TPO and anti-Tg were both <60 U/mL, which was the manufacturer's reference limit, were the patients considered to be antibody-negative. Cross-reactivity was assessed by adding hCG to samples containing varying concentrations of TSH. Cross-reactivity was undetectable at concentrations of hCG of 200,000 mIU/L.
Statistical analysis
The characteristics of the dichorionic and monochorionic twins were compared by the Mann–Whitney U-test for continuous variables and Fisher's exact test or chi-square test for categorical variables.
The measured serum TSH and FT4 in the twins with normal outcomes were converted to MoM of normal singleton pregnancies, corrected for gestational age, maternal age, BMI, and racial origin as previously described (11). The limitation with this statistical approach is the assumption that the effects of maternal characteristics such as age, race/ethnicity, and BMI on thyroid functions are the same in twins as in singleton pregnancies. In the antibody-negative group, linear regression analysis was used to determine if twinning was a significant predictor of square-root TSH MoM and log10 FT4 MoM. These transformations of square-root for TSH and log10 for FT4 were used to achieve Gaussian normality of the distributions (11). Normality of distribution was assessed using probability plots. The observed values of TSH and FT4 were then expressed as MoM for normal twin pregnancies. Similarly MoM values were also calculated for the TTTS group.
Regression analysis was used to determine the significance of the inter-relations between serum TSH, FT4, and free β-hCG. Comparison of TSH MoM and FT4 MoM between the antibody-positive and antibody-negative groups was done by the Kruskal–Wallis test with post hoc Bonferroni correction (critical statistical significance p<0.0167). Similarly, the normal outcome group was compared with the TTTS group. The proportion of cases with serum TSH above the 97.5th percentile and serum FT4 below the 2.5th percentile in the antibody-positive and antibody-negative groups were compared using the chi-square test with post hoc Bonferroni correction. The statistical software package SPSS 20.0 (SPSS Inc., Chicago, IL) was used for data analyses.
Results
In the 235 twin pregnancies with normal outcomes, there were 177 (75.3%) with dichorionic and 58 (24.7%) with monochorionic twins (Table 1). Additionally, we studied 19 cases that resulted in severe TTTS (Table 1). None of the patients showed evidence of overt thyroid disease that needed treatment or undetectable TSH levels.
Comparisons by the chi-square test for categorical variables and by the Mann–Whitney U-test for continuous variables (p<0.05).
IQR, interquartile range; TTTS, twin–twin transfusion syndrome.
In 198 (84.3%) of the 235 pregnancies, the serum concentration of anti-TPO and anti-Tg was <60 U/mL, and in 37 (15.7%), the concentration of one or both antibodies was ≥60 U/mL. In 17 (7.2%), both antibodies were positive; in 12 (5.1%), only anti-TPO was positive; in 8 (3.4%), only anti-Tg was positive. The prevalence of antibody positivity was not significantly different between dichorionic (25 of 177, 14.1%) and monochorionic twins (12 of 58, 20.7%; p=0.298).
Serum TSH and FT4 in antibody-negative twin pregnancies with normal outcomes
In the antibody-negative twin pregnancies with normal outcomes, compared to singletons, serum TSH MoM was lower (median 0.62 [interquartile range (IQR) 0.16–1.18] vs. 1.01 [IQR 0.61–1.51]; p<0.0001; Figs. 1 and 2), FT4 MoM was not significantly different (median 0.98 [IQR 0.91–1.08] vs. 0.99 [IQR 0.91–1.09]; p=0.975; Fig. 2), and free β-hCG MoM was higher (median 1.91 [IQR 1.33–2.59] vs. 0.98 [IQR 0.66–1.50]; p<0.0001; Fig. 2).
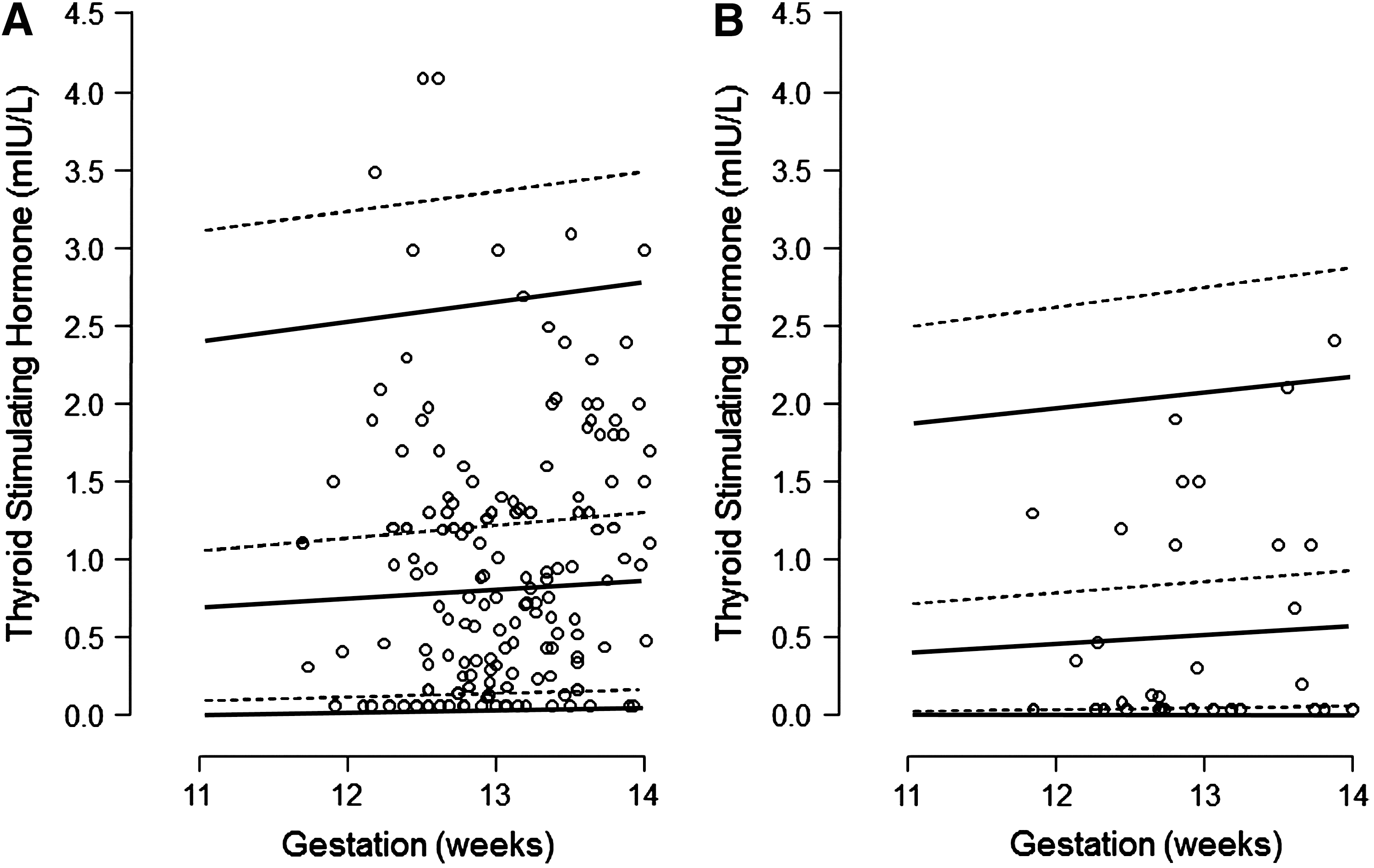
Maternal serum thyrotropin concentration of twin pregnancies in Caucasian

Box-whisker plots of the multiples of median (MoM) thyrotropin and free thyroxine in antithyroid antibody-negative singleton (n=3592) and twin (n=198) pregnancies excluding those that developed twin–twin transfusion syndrome.
Regression analysis demonstrated that twinning, but not chorionicity (TSH: p=0.722; FT4: p=0.911), had significant contribution on the level of TSH but not FT4:
The observed values of TSH and FT4 were then expressed as MoM for normal twin pregnancy. The 50th, 95th, 97.5th, 5th, and 2.5th percentiles of serum TSH and FT4 for antibody-negative twin pregnancies are shown in Table 2.
Free thyroxine values are the same as in singleton pregnancies (11).
BMI, body mass index.
In dichorionic twins, compared to monochorionic twins, there were no significant differences in TSH MoM (median 0.98 [IQR 0.28–1.29] vs. 1.13 [IQR 0.23–2.22]; p=0.856), FT4 MoM (median 0.98 [IQR 0.91–1.08]; vs. 1.01 [IQR 0.94–1.06]; p=0.537), or free β-hCG MoM (median 0.98 [IQR 0.70–1.29] vs. 1.13 [IQR 0.68–1.63]; p=0.299).
There was a significant correlation between log10 TSH MoM and log10 FT4 MoM (r=−0.487, p<0.0001) and log10 free β-hCG MoM (r=−0.280, p<0.0001); as well as between log10 FT4 MoM and log10 free β-hCG MoM (r=0.199, p=0.005).
Serum TSH and FT4 in antibody-positive twin pregnancies with normal outcome
In the cases where both anti-TPO and anti-Tg were positive, compared to the antibody-negative group, the median TSH was higher, but FT4 and free β-hCG were not significantly different (Table 3). Serum TSH was above the 97.5th percentile in 2.0% of the antibody-negative group, and this increased to 29.4% (5 of 17) in the group with both anti-TPO and anti-Tg positivity. There was no significant difference in the proportion of FT4 below the 2.5th percentile between the antibody-negative and antibody-positive groups (Table 3).
Comparisons between each antibody-positive group with the antibody-negative group by the Fisher exact test with post hoc Bonferroni correction for categorical variables and by the Kruskal–Wallis with post hoc Bonferroni correction for continuous variables.
p<0.0167.
hCG, human chorionic gonadotrophin; MOM, multiples of the expected normal median; anti-Tg, antithyroglobulin antibodies; anti-TPO, antithyroperoxidase antibodies.
Serum TSH, FT3, and FT4 in TTTS
In the TTTS group, 17 (89.5%) of the 19 pregnancies were antibody-negative; in this group, compared to the antibody-negative normal outcome twins, there was no significant difference in TSH MoM (median 1.38 [IQR 0.52–2.05] vs. 1.00 [IQR 0.26–1.36] p=0.424), FT4 MoM (median 0.94 [IQR 0.90–1.16] vs. 0.98 [IQR 0.91–1.08]; p=0.773), or free β-hCG MoM (median 0.95 [IQR 0.51–2.22] vs. 1.00 [IQR 0.69–1.36]; p=0.997).
Discussion
This study demonstrates that in normal twin pregnancies at gestational weeks 11–13, compared to singletons, maternal serum FT4 is not significantly different, but TSH is about 40% lower. The most likely explanation for the low TSH is the high level of free β-hCG, which is twice as high as in singletons. The levels of serum TSH and FT4 were similar in dichorionic and monochorionic twins, with or without TTTS, and there were no significant differences between the three groups in serum free β-hCG.
In establishing reference ranges of thyroid function in twins, we excluded pregnancies complicated by miscarriage or fetal death, fetal growth restriction, pre-eclampsia, and preterm delivery because of the reported association between these pregnancy complications and clinical or subclinical hypothyroidism (1 –3). We also excluded pregnancies with known thyroid disease and those with antithyroid antibodies. In our population, about 12% of pregnancies had detectable anti-TPO antibodies and 11% had anti-Tg antibodies, frequencies that are similar to the respective prevalences of 10% and 14% in our singleton pregnancies (11). When both antibodies were positive, compared to the antibody-negative group, median TSH values were higher and the percentage of cases with TSH values above the 97.5th percentile was higher, whereas serum FT4 and β-hCG were not significantly different. A previous study reported that the majority of antibody-positive women with subclinical hypothyroidism during pregnancy will develop clinical hypothyroidism within the subsequent 10 years (4). Consequently, in establishing normal ranges of thyroid function, it is necessary to exclude antibody-positive patients.
The measured serum TSH and FT4 in twin pregnancies were converted to MoM of normal singleton pregnancies, corrected for gestational age in weeks, maternal age, BMI, and racial/ethnic origin as previously described (11). In women of African origin, the serum concentration of both TSH and FT4 is lower than that in Caucasians, suggesting that the hypothalamic–pituitary–thyroid gland axis in the two racial/ethnic groups is set at different thresholds. The minimum detectable concentration for TSH is 0.01 mIU/L. In the Caucasian population, the 2.5th percentile raw values were all detectable. Although typically reference ranges are defined as mean±2 SD, many hospitals in the United Kingdom use the 5th or even the 10th percentile as cutoffs. In the African population, the 2.5th and the 5th percentile can be undetectable depending on other maternal characteristics and gestation as shown in Table 2. This illustrates that more accurate assays will help in diagnosing hyperthyroidism in pregnancy in that group. None of the women in our cohort had undetectable serum TSH levels, and this is probably because we only examined 32 women of African origin.
The most likely explanation for the finding that maternal serum FT4 was not significantly different but TSH was lower in antibody-negative twins compared to singletons is the physiological increase in β-hCG. hCG, which has an identical α-subunit and structurally similar β-subunit with TSH, has thyrotropic properties, and there is an inverse relationship between maternal serum levels of TSH and hCG in early pregnancy (19 –24). A study of 3961 dichorionic and 759 monochorionic twins at gestational weeks 8–13 reported that the maternal serum free β-hCG, expressed as MoMs for singleton pregnancies, increased from 1.5 MoM at 8–9 weeks to 2.0 MoM at 12–13 weeks for dichorionic twins, and from 1.0 MoM to 2.0 MoM for monochorionic twins (25). Consequently, at a median gestational age of 13 weeks in our study, the levels of free β-hCG in twins, irrespective of chorionicity, were twice as high as in singletons. Similarly, the levels of free β-hCG and TSH in monochorionic twins that subsequently developed severe TTTS were similar to those of normal twins.
This study establishes reference ranges of maternal thyroid function in twin pregnancies at 11–13 weeks after appropriate correction for maternal characteristics, which can affect the measured serum concentrations of TSH and FT4. These ranges can be used in clinical practice to help diagnose subclinical and overt hypo- and hyperthyroidism. Given the lower levels of TSH in twin pregnancies, it is important to use the twin-specific reference range in order to avoid an overdiagnosis of thyrotoxicosis in twin pregnancies. These values can also form the basis for the study of early thyroid function in pathological pregnancies as well as for the investigation of the consequences of overt and subclinical hypothyroidism outcomes of twin pregnancies.
Footnotes
Acknowledgments
This study was supported by a grant from the Fetal Medicine Foundation (Charity No. 1037116). The assays were performed by Ms. Tracy Dew, Department of Clinical Biochemistry, King's College Hospital, London, United Kingdom.
Author Disclosure Statement
No competing financial interests exist.