
Abstract
Background:
Levothyroxine (L-T4) absorption varies between individuals, and can be affected by various concomitantly administered drugs. Case reports have indicated an association between cotreatment with ciprofloxacin or rifampin and hypothyroidism in patients on a stable L-T4 dose.
Methods:
The effects of two antibiotics on T4 absorption were prospectively assessed in a double-blind, randomized, crossover fashion. Eight healthy volunteers received 1000 μg L-T4 combined with placebo, ciprofloxacin 750 mg, or rifampin 600 mg as single doses. We measured total plasma thyroxine (T4) concentrations over a 6-hour period after dosing using liquid chromatography–tandem mass spectrometry. For each study arm, areas under the T4 plasma concentration–time curve (T4 AUCs) were compared.
Results:
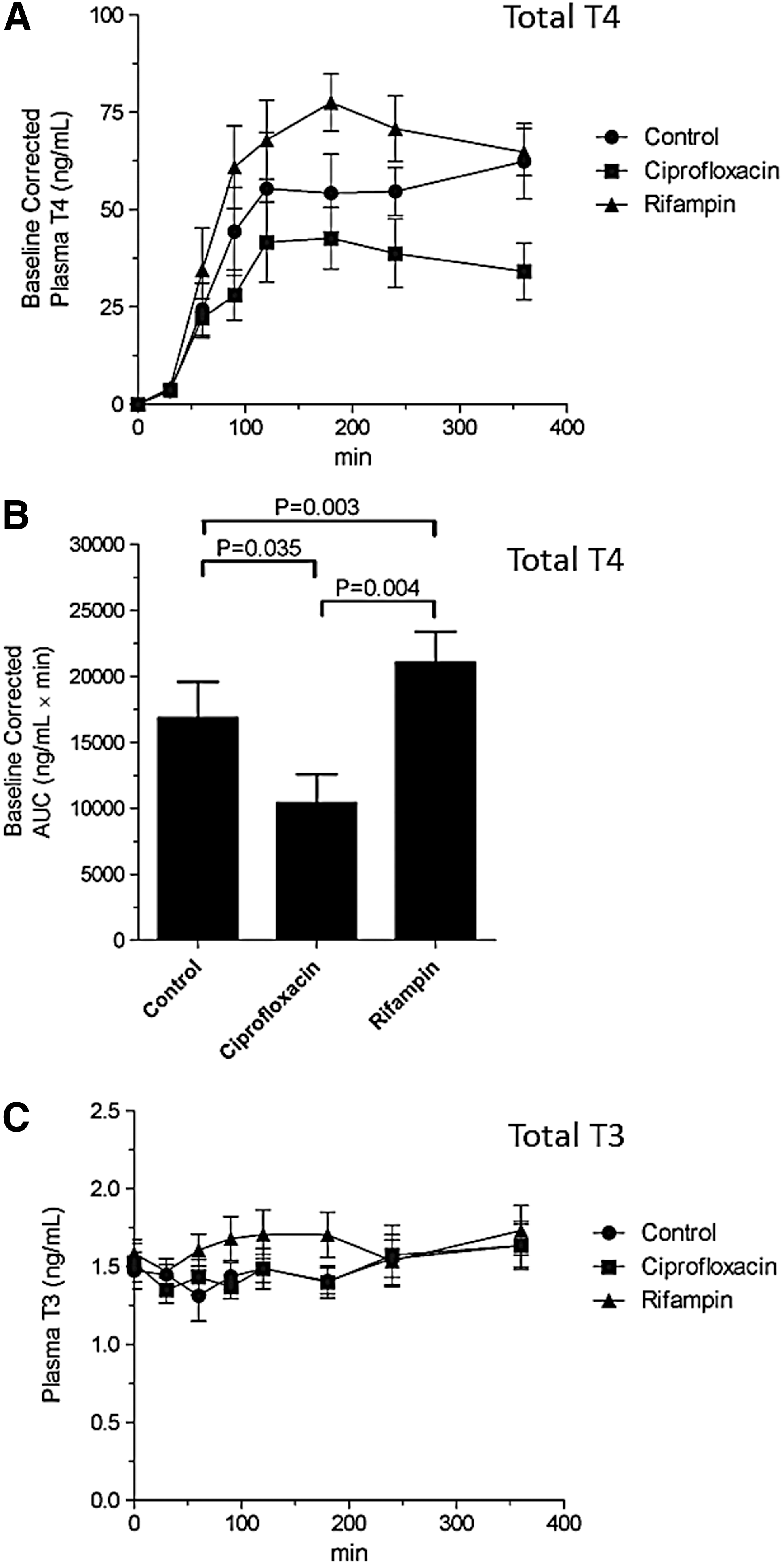
Coadministration of ciprofloxacin significantly decreased the T4 AUC by 39% (p=0.035), while, surprisingly, rifampin significantly increased T4 AUC by 25% (p=0.003).
Conclusion:
Intestinal absorption of L-T4 is differentially affected by acute coadministration of ciprofloxacin or rifampin. Mechanistic studies focused on intestinal and possibly hepatic thyroid hormone transporters are required to explain the observed drug interactions with L-T4.
Introduction
Several drugs have been shown to interact with L-T4 absorption and metabolism. A number of specific mechanisms have been proposed: (i) mechanical interference with absorption (2); (ii) altered transport of thyroxine (T4) and triiodothyronine (T3) due to increase of T4-binding globulin, requiring a transient change in the L-T4 dose to maintain the same free levels, as seen with estrogen (3); (iii) inhibition of L-T4 deiodination manifested as increased free T4 with reduced free T3, as seen with amiodarone (4); or induction of type 3 deodination manifesting as decreased T3 and T4, as seen with sunitinib (5); (iv) interaction with hepatic metabolism [implicated with rifampin (6)]; and (v) interference at the hypothalamic thyroid axis (7). However, some drug–L-T4 interactions cannot be explained by these mechanisms. For example, in patients receiving a stable dose of L-T4, simultaneous intake of ciprofloxacin resulted in hypothyroidism, an effect that could be reversed by taking L-T4 and ciprofloxacin 6 hours apart, but not by increasing the L-T4 dose (8). This effect could not be explained by any of the above-mentioned proposed mechanisms, including mechanical interference. An alternative interaction mechanism may involve alterations in carrier-mediated transport of T4 across the gastrointestinal and hepatic membranes.
Evidence accumulated over the last decade clearly indicates that tissue-specific thyroid hormone entry is facilitated by transporter proteins (9), such as monocarboxylate transporter (MCT) 8, considered to be one of the most specific and active T4 transporters identified thus far, and highly expressed in thyroid-hormone–sensitive neurons in the brain. Several transporters have been localized in the intestine that might be involved in thyroid hormone absorption, including organic anion transporting polypeptide (OATP)1A2, OATP2B1, L-type amino acid transporters (LAT)1 and LAT2, and MCT10 (10). A potential role for OATP1A2 is supported by the reduction of L-T4 absorption following simultaneous ingestion of grapefruit juice, a known inhibitor of OATP1A2 activity (11). Interestingly, ciprofloxacin has been shown to be transported by OATP1A2 (12), suggesting that it may also inhibit T4 transport. Rifampin, a well-known OATP inhibitor (13), has been found to decrease measured free T4 when taken with thyroid replacement. The mechanism for the rifampin effect has been ascribed to induction of hepatic metabolic and biliary clearance (6). Indeed, the chronic use of rifampin necessitates an increase in thyroid supplementation (14). However, the acute effect of rifampin on thyroid hormone absorptive transport is unknown.
In patients receiving L-T4 therapy, we hypothesized that T4-transporting proteins expressed in the first-pass organs, the gut and liver, are the mechanistic sites for interaction with thyroid hormone absorption by concomitantly administered drugs. Thus, the goal of this study was to formally determine the acute effect of coadministration of ciprofloxacin on L-T4 absorption and compare that with a well-known OATP inhibitor (rifampin) to examine the potential relevance of intestinal transporters to L-T4 absorption.
Materials and Methods
The study was approved by the Western University Human Subjects Research Ethics Board. All subjects provided informed written consent. We included eight healthy men and women, 18–40 years old, not on any medications, with normal thyroid, kidney, and liver function test results. Patients already taking thyroid hormone or any routine prescription, over-the-counter medications, or natural health products within the last 2 months were excluded. Additional exclusion criteria included any known thyroid, heart, kidney, liver, or gastrointestinal disease; pregnancy or breastfeeding; known allergy to any of the study medications; and wearing contact lenses (as rifampin can cause orange coloring to contact lenses).
All subjects were studied on three different occasions using the same protocol, with at least a 4-week washout interval between study sessions. Fasting blood samples were obtained through an indwelling catheter inserted into an arm vein, and blood samples (each 4 mL) were collected at −15 and 0 minutes before, and at 30, 60, 90, 120, 180, 240, and 360 minutes after administration of drugs. About 1000 μg of L-T4 was administered orally with 250 mL water. On each of the 3 study days, L-T4 was combined with placebo, ciprofloxacin (750 mg orally), or rifampin (600 mg orally). The administration order of these drugs was randomized by the study pharmacist; the participants and investigators were blinded to the coadministered medications. Thyrotropin was measured using a commercially available test (Roche Diagnostics, Mannheim, Germany). Total plasma T4 and T3 concentrations were measured using a sensitive and specific liquid chromatography–tandem mass spectrometry method. Plasma samples (100 μL) were spiked with internal standard, 13C6-T4 (10 μL, 1000 ng/mL in 0.1% formic acid in water/acetonitrile 75:25; Toronto Research Chemicals, Toronto, Canada). After addition of 300 μL of ice-cold acetonitrile and vortexing, precipitated protein was pelleted by centrifugation at 14,000 g at 4°C for 10 min. To 100 μL of the resulting supernatant, 200 μL of Mobile Phase A (0.1% formic acid in water) was added and 100 μL of this mixture was injected into the liquid chromatograph (Agilent 1200; Thermo Aria TLX1, San Jose, CA). Standard curve samples were prepared in water spiked with L-T4 (0–400 ng/mL final concentration; Sigma, St. Louis, MO) or T3 (0–10 ng/mL final concentration; Sigma) and 13C6-T4 as above. Analytes were separated using reverse-phase chromatography on a Thermo Hypersil Gold C18 column (50 mm×5 mm; 5 μm). Mobile phase was delivered at a flow rate of 0.5 mL/min with gradient flow with Mobile Phase A and Mobile Phase B (0.1% formic acid in acetonitrile). For the first 60 seconds, the mobile phase consisted of 25% Mobile Phase B and then increased linearly to 60% Mobile Phase B over 5 minutes. Thereafter, a linear decrease to 25% Mobile Phase B occurred over 1.5 minutes, which was held for an additional 1.5 minutes. The retention times for 13C6-T4, L-T4, and T3 were 4.4, 4.4, and 3.8 minutes, respectively. Analytes were detected by tandem mass spectrometry on a Thermo TSQ Vantage triple quadrupole instrument equipped with a heated electrospray ionization probe (HESI-II) set with probe voltage (3000 V), vaporizer temperature (350°C), ion transfer tube temperature (350°C), sheath gas (30 arbitrary units), and auxiliary gas (10 arbitrary units). The following multiple reaction monitoring transitions were used with detection in positive mode and collision gas (1.5 mTorr) and declustering voltage (10 V): 13C6-T4 (783.6→737.9 m/z), L-T4 (777.6→731.9 m/z), and T3 (651.8→606.0 m/z) with collision energy at 23, 23, and 20 V, respectively. Standard curves were linear (r 2>0.998) over the concentration range of 10–400 ng/mL and 0.5–10 ng/mL for L-T4 and T3, respectively. Assay precision for quality control samples was 11%, 7%, and 8% for L-T4 at 10, 100, and 400 ng/mL, respectively. Assay bias for quality control samples was 21%, 8%, and 5% for L-T4 at 10, 100, and 400 ng/mL, respectively.
For each study day, thyroid indices and clinical data were recorded. Response area under the T4 plasma concentration–time curves (AUCs) corrected for baseline levels were calculated using trapezoidal integration. We compared AUCs using paired Student's t-test (GraphPad version 5.04). A p-value less than 0.05 was considered statistically significant.
Results
Eight healthy subjects were included in the study. Their baseline characteristics are described in Table 1. The total T4 concentrations following administration of L-T4 with placebo, rifampin, or ciprofloxacin are shown in Figure 1A. Baseline-corrected T4 AUC was significantly increased 25% with coadministration with rifampin (p=0.035), but decreased 39% when coadministered with ciprofloxacin (p=0.003) (Fig. 1B) compared with the control (placebo) phase. The total T3 concentrations following administration of L-T4 with placebo, rifampin, or ciprofloxacin are shown in Figure 1C. The T3 AUC was not different between coadministration with placebo, rifampin, or ciprofloxacin; results (mean±SD) were 537±91, 587±115, and 534±92 ng/(mL·min), respectively (p=not significant).
Reference ranges are shown in parentheses. T3, triiodothyronine; T4, thyroxine; TSH, thyrotropin.
Safety analysis
None of the participants reported any signs of hyperthyroidism. Further, there was no significant change seen in the heart rate of the subjects either during the administration of the medications or between visits. Fasting morning concentrations of thyrotropin, free T4, and free T3 obtained at each of the study days did not change throughout the 12 weeks (data not shown, p=not significant).
Discussion
Changes in absorption of thyroid hormone resulting from coadministration of commonly prescribed medications are well documented (15). The novel findings of this study are reduced L-T4 absorption with ciprofloxacin coadministration, but an increase in L-T4 absorption with rifampin coadministration. The reduction in T4 AUC after coadministration of ciprofloxacin with L-T4 is consistent with inhibition of an intestinal T4 uptake transporter, possibly members of the OATP family (16). Although OATP1A2 has been shown capable of transporting T4, current evidence suggests minimal expression of OATP1A2 in enterocytes (17). It is tempting to speculate that thyroid hormone transporters MCT8, MCT10, or LAT1/2, which are expressed in the intestine, may be the site of the L-T4 interaction with ciprofloxacin (18 –21).
The effect of rifampin was unexpected. However, acute dosing of rifampin increases the plasma level of known OATP drug substrates such as atorvastatin (22). We know that certain members of the OATP family, including OATP1B1 and 1B3, are liver-specific in their expression, and inhibition of hepatic OATPs can lead to an apparent increase in AUC of substrate drugs (23). Moreover, in the Oatp1b2 knockout mouse model, our group has shown that there is reduced hepatic entry of thyroid hormone (24).
Accordingly, it is possible that rifampin preferentially inhibited hepatic T4 uptake mediated by liver-specific OATP transporters relative to intestinal T4 transporters. It is also possible that rifampin may have increased net intestinal absorption of L-T4 through inhibition of an intestinal efflux transporter such as P-glycoprotein, which is known to be highly expressed on the brush border domain of intestinal enterocytes and which has been shown capable of mediating T4 efflux transport (25). In light of these hypothetical mechanisms, it will be critical to perform additional in vitro studies to identify T4 transporters in the intestine and liver, and to characterize their drug interactions to more fully clarify the mechanistic basis of our observations. Furthermore, assessment of the effects of rifampin and ciprofloxacin on the intestinal absorption of T3 would be of clinical interest.
Despite the small number of subjects included in this study, the difference in AUC between groups is robust. Given the tight regulation of serum T4 physiologically, the interaction described here is clinically relevant since L-T4 absorption with ciprofloxacin is 61% and with rifampin is 125% compared with controls. Closer monitoring of the thyroid status of patients who are to take these medications together would be warranted.
It should be noted that despite the high dose of L-T4 administered on three occasions, no subjects were clinically hyperthyroid or showed changes in vital signs or electrocardiogram throughout the study. Accordingly, there were no significant (statistical or clinical) changes to thyroid indices at the 4-week intervals. Since total T4 concentrations were measured and not free hormone levels, this may limit the generalizability to the clinical setting, and may explain the lack of clinical symptoms, suggesting that adequate binding proteins were present to offset the elevated dose. Total T3 levels were measured as well, but there were no significant changes observed in plasma levels after each L-T4 dose regardless of the coadministration arm (Fig. 1C). This may also have contributed to the safety of this study and lack of clinical effects after high-dose L-T4 was consumed. A lack of changes in T3 plasma levels throughout each study phase also argues against the possibility that altered L-T4 deiodination during absorption is the cause of the changes in plasma T4 with coadministration with the antibiotics.
This controlled, prospective, placebo-controlled, randomized, double-blind study design provides key evidence for a pharmacokinetic interaction between L-T4 and ciprofloxacin and rifampin that has not been compellingly demonstrated by previous case reports. There are, however, some limitations to the study design. First, a larger number of subjects, as well as a longer sampling period extending beyond 6 hours, may provide better estimates of pharmacokinetic parameters such as C max, T max, and half-life. Second, it is important to note that ciprofloxacin and rifampin were administered as one-time doses, and therefore the effects of chronic dosing are not captured by the current study design. Indeed, while a single dose of coadministered rifampin caused increased T4 bioavailability and plasma levels, chronic rifampin treatment is expected to reduce T4 plasma levels as a result of the known induction of hepatic T4 clearance pathways (14). Hence, for rifampin co-treatment, a biphasic influence on T4 plasma exposure is expected to occur, making L-T4 dose adjustments challenging.
In conclusion, acute coadministration of rifampin or ciprofloxacin has distinct effects on the oral absorption of L-T4. It is expected that additional studies that define the roles of specific intestinal and liver transporters in L-T4 absorption will further elucidate our understanding of the mechanistic basis of this interaction.
Footnotes
Acknowledgment
This study was funded by the Lawson Health Research Institute.
Author Disclosure Statement
No competing financial interests exist.