
Abstract
Background:
Studies have described an encapsulated and an infiltrative form of the follicular variant of papillary thyroid carcinoma (FVPTC). Encapsulated FVPTCs have been reported to have virtually no recurrence risk or metastatic potential and to harbor RAS mutations but not BRAF mutations. In contrast, infiltrative tumors have significant metastatic potential, a risk of recurrence, and a BRAF mutation frequency of approximately 25%. In our experience, a substantial number of FVPTCs are neither fully encapsulated nor infiltrative, but instead are partially encapsulated (PE) or well circumscribed (WC). We have previously reported that PE/WC FVPTCs behave in an indolent fashion similar to encapsulated tumors. The purpose of the current study was to evaluate the molecular alterations in PE/WC FVPTC.
Methods:
We identified 28 PE/WC FVPTCs resected consecutively at our institution. Targeted mutation analysis of 41 genes including members of the RAS and RAF families was performed on DNA extracted from formalin-fixed, paraffin-embedded blocks using single-base extension chemistry and mass spectrometry.
Results:
Lymph node metastases were absent in all cases with sampled lymph nodes, and no patients developed tumor recurrences (median follow-up time, 72.8 months). Overall, 13 cases (46%) harbored RAS mutations, including seven (25%) with NRAS mutations (p.Gln61Arg) and six (21%) with HRAS mutations (five had p.Gln61Arg and one had a p.Gln61Lys substitution). No PE/WC FVPTCs had BRAF mutations.
Conclusions:
The results of this study confirm our previous finding that PE/WC FVPTCs pursue an indolent clinical course. Additionally, we found that PE/WC tumors have a similar molecular profile to that of encapsulated FVPTCs with frequent RAS mutations (46%) and no BRAF mutations. These molecular results provide further evidence that PE/WC and encapsulated FVPTCs are biologically similar and should be distinguished from more aggressive infiltrative FVPTCs.
Introduction
In the past decade it has become clear that not all FVPTCs are biologically alike (18 –24). Studies have described an encapsulated and an infiltrative form of FVPTC (18 –20). Liu et al. (18) reported that encapsulated FVPTCs that lack vascular invasion and capsular penetration (i.e., non-invasive encapsulated FVPTCs) have virtually no metastatic potential or recurrence risk. In contrast, infiltrative FVPTCs (i.e., tumors that lack a capsule and have tongues of tumor infiltrating into adjacent thyroid parenchyma) had a significant metastatic potential and a risk of recurrence (18). Rivera et al. (19) subsequently demonstrated that encapsulated and infiltrative FVPTCs not only behave different clinically, they also have different molecular profiles. Seventy percent of PTCs and follicular thyroid carcinomas (FTCs) harbor a known genomic alteration, including point mutations in BRAF and RAS and rearrangements involving RET/PTC and PAX8/PPARγ (25). Activating BRAF mutations, RET/PTC rearrangements, and activating mutations in RAS family members have been reported in approximately 45%, 15%, and 15% of PTCs, respectively (though the frequency of these mutations may be changing) (25 –31). FTCs (and follicular adenomas) lack BRAF mutations and RET/PTC translocations and instead have more frequent mutations in RAS family members (seen in approximately 45% of FTCs), or demonstrate PAX8/PPARγ rearrangements (seen predominantly in FTC, with a frequency of approximately 35%) (25,30 –37). Within PTC, there are genotype–phenotype correlations. For example, BRAF mutations are most frequently seen in tall cell variant and classical type PTC (28,38), while RET/PTC rearrangements are more often associated with classical type and solid variant PTC (28,29). Overall, FVPTC has been shown to harbor molecular alterations more similar to those seen with follicular adenomas/FTCs than those associated with classical type PTC (28,39 –42). Rivera et al. (19) found that encapsulated tumors lacked BRAF mutations and instead harbored RAS mutations at a frequency of 36% and PAX8/PPARγ rearrangements in 4% of cases. In contrast, infiltrative tumors had a significantly higher rate of BRAF mutations (26%), a lower rate of RAS mutations (10%), and a RET/PTC rearrangement frequency of 10% (19). Hence, encapsulated FVPTCs appear genetically similar to follicular adenomas/FTCs, whereas infiltrative FVPTCs show overlap with classical type PTC. On the basis of these clinical and molecular differences in encapsulated and infiltrative FVPTCs, the authors of the described studies have advocated conservative management (i.e., lobectomy only) for noninvasive encapsulated FVPTC.
As a result of these studies, pathologists have started to document whether an FVPTC is encapsulated or infiltrative in the pathology report. However, in our experience, a significant number of FVPTCs are not easily classified as encapsulated or infiltrative. Instead, many FVPTCs would be best characterized as partially encapsulated or well-circumscribed (PE/WC). We recently investigated the metastatic potential and recurrence risk of PE/WC FVPTCs as compared with encapsulated and infiltrative tumors and found that PE/WC FVPTCs were clinically similar to the encapsulated tumors in our cohort, with no associated lymph node metastases, and no recurrences (outside of a single tumor bed recurrence associated with the only tumor in the group with a positive resection margin) (43). In contrast, 78% of infiltrative tumors in our cohort had lymph node metastases and 15% recurred, including one distant metastasis. In light of the clinical similarities between PE/WC and encapsulated FVPTCs, we hypothesized that their genetic alterations might also be similar; therefore, we utilized a targeted genotyping strategy to investigate the molecular profile of PE/WC tumors.
Materials and Methods
Pathology and medical record review
A search of the pathology database at Brigham and Women's Hospital was performed for lobectomy and thyroidectomy specimens with PTC measuring >1 cm diagnosed between 2005 and 2006. All available hematoxylin and eosin-stained slides of tumor for all cases were reviewed by two pathologists (BEH and JAB), and FVPTCs were identified. Tumors diagnosed as FVPTC were required to have an entirely or almost entirely (99%) follicular architecture (44) and cytologic features of PTC. Cases were excluded if the patient had another thyroid carcinoma measuring >1 cm or had more than two additional microcarcinomas. Cases with an anaplastic or a poorly differentiated component, as defined according to the criteria described in the Turin proposal (45), were excluded. Each tumor was subclassified as encapsulated, PE/WC, or infiltrative as previously described (43). Briefly, tumors with a complete fibrous capsule delineating the tumor from the benign thyroid parenchyma were categorized as encapsulated tumors. Infiltrative tumors were defined as tumors either entirely or partially lacking a tumor capsule with tongues of tumor infiltrating into the benign thyroid parenchyma. PE/WC tumors also entirely or partially lacked a tumor capsule, but, unlike infiltrative tumors, they had a well-circumscribed edge with no tumor invading into adjacent thyroid parenchyma (Fig. 1). Cases with any indication of an infiltrative edge were considered infiltrative. Only PE/WC tumors were included in this study. Based on the inclusion and exclusion criteria, we had 28 cases of PE/WC FVPTC in our cohort. The PE/WC FVPTCs in this study were distinct from the cohort we previously evaluated to compare the metastatic potential and recurrence risk of PE/WC, encapsulated, and infiltrative FVPTCs (43).
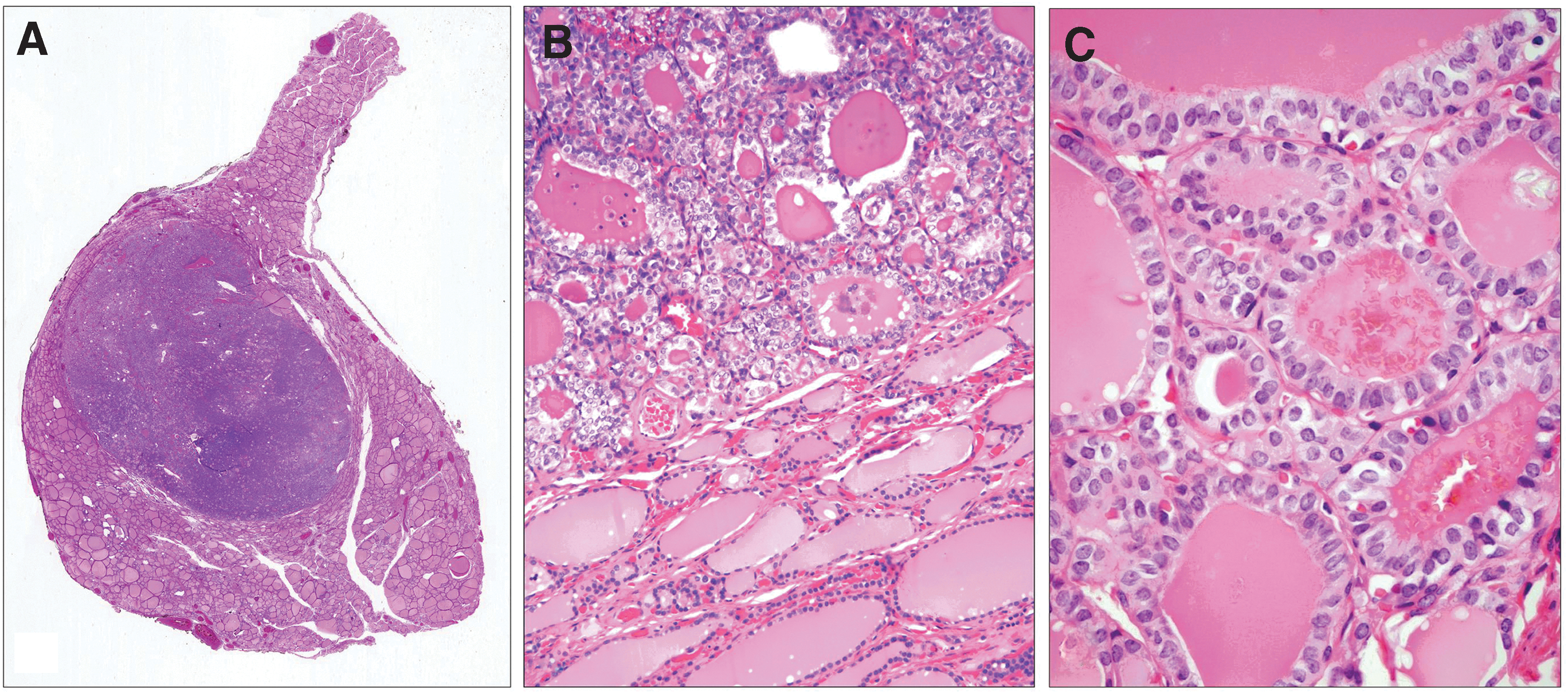
Architectural and cytologic features of PE/WC FVPTC.
The following features were recorded based on the original pathology reports: type of specimen (lobectomy, thyroidectomy), size of tumor, presence of extrathyroidal extension, margin status, and lymph node status. For each patient, the medical record was examined, and the following information recorded: age at time of procedure, sex, date of procedure, additional surgery, treatment with RAI, date of clinical recurrence, type of recurrence (tumor bed, lymph node metastasis, distant metastasis), and date of last follow-up.
Molecular analysis of mutations in PE/WC FVPTC
Molecular analysis was performed in a CLIA-certified laboratory. DNA was extracted from formalin-fixed, paraffin-embedded (FFPE) tumor tissue with >90% tumor purity from all 28 PE/WC FVPTCs. Briefly, FFPE blocks were cored with 1 mm punches (∼8–10 per sample), and genomic DNA was extracted using standard protocols (Qiagen, Valencia, CA). A total of 200 ng of DNA was required. Following whole genome amplification, mutation profiling for 471 mutations in 41 genes, including BRAF and RAS family members (Oncomap), was performed using single base extension chemistry (iPLEX) followed by MALDI-TOF mass spectrometry to separate the products (Sequenom), as previously described. Variant alleles were identified through automated and manual reviews and confirmed with homogenous MassEXTEND chemistry (46,47). The genes that were evaluated are listed in Table 1. All of the specific mutations interrogated are available in Supplementary Table S1 (Supplementary Data are available online at
Immunohistochemical staining for BRAF V600E
Immunohistochemistry was performed following pressure cooker antigen retrieval (0.01 M citrate buffer; pH 6.0) using the mouse anti–BRAF V600E monoclonal antibody (clone VE1; 1:50 dilution with overnight incubation, Spring Bioscience, Pleasanton, CA) on 4-μm-thick FFPE tissue sections of tumor. This antibody has been shown to have a high correlation between expression and mutation status on tissue sections from PTCs (48). Cytoplasmic staining was scored as positive or negative with a known BRAF-mutant PTC used as a positive control.
Results
Clinical characteristics and histopathologic features
The clinical characteristics are summarized in Table 2. Of the 28 patients included in the study, there were 23 (82%) women and 5 (18%) men. The mean age at time of thyroidectomy was 49 years (range 24–78 years), with 12 (43%) under the age of 45 and 16 (57%) 45 years of age or older. Twenty (71%) patients underwent initial total thyroidectomy, while eight (29%) patients underwent an initial lobectomy followed by a completion thyroidectomy. Seventeen (61%) patients had no lymph node sampling, while lymph node sampling was performed in 11 (39%) patients. Fourteen (50%) patients received RAI treatment, six (21%) patients did not receive RAI, and the RAI treatment status was unknown for eight (29%) cases.
The histopathologic features are summarized in Table 3. The mean tumor size was 2.4 cm (range, 1–7.6 cm). Fourteen (50%) tumors were 1–2 cm (pT1), 12 (43%) tumors were 2–4 cm (pT2), and two tumors were >4 cm (pT3). No tumors had associated lymphovascular invasion or extrathyroidal extension. The surgical margins of resection were negative in all cases. Overall, 17 (61%) tumors were multifocal (with no more than two additional foci of tumor <1.0 cm based on the exclusion criteria).
Lymph node metastases and clinical follow-up
Lymph node metastases and clinical follow-up data are summarized in Table 4. Lymph node metastases were absent in all 11 patients that had sampled lymph nodes. No patients had tumor recurrences (mean follow-up time, 63 months; median, 72.8 months; range, 4.8–90.3 months).
ANED, alive with no evidence of disease.
Molecular alterations and BRAF V600E immunohistochemical results
The molecular alterations and BRAF V600E immunohistochemical results are summarized in Table 5. Overall, thirteen (46%) tumors harbored RAS mutations. Seven (25%) cases had NRAS mutations (p.Gln61Arg), and 6 (21%) cases had HRAS mutations (5 had p.Gln61Arg and 1 had a p.Gln61Lys substitution). No tumors had KRAS mutations. No cases in our study had BRAF mutations. In keeping with this molecular finding, all cases were negative for BRAF V600E by immunohistochemistry. One tumor was found to have a mutation in VHL (p.Pro81Ser). While this VHL mutation has been reported in renal cell carcinoma (49), and loss of heterozygosity of VHL has been reported in follicular thyroid tumors (50), the significance of this mutation is unclear. No mutations were detected in any other of the genes evaluated. Retrospectively, all tumors were reviewed for possible histologic features related to the specific molecular alterations; however, tumors with wild type RAS and NRAS- and HRAS-mutated tumors all appeared histologically similar (Fig. 2).
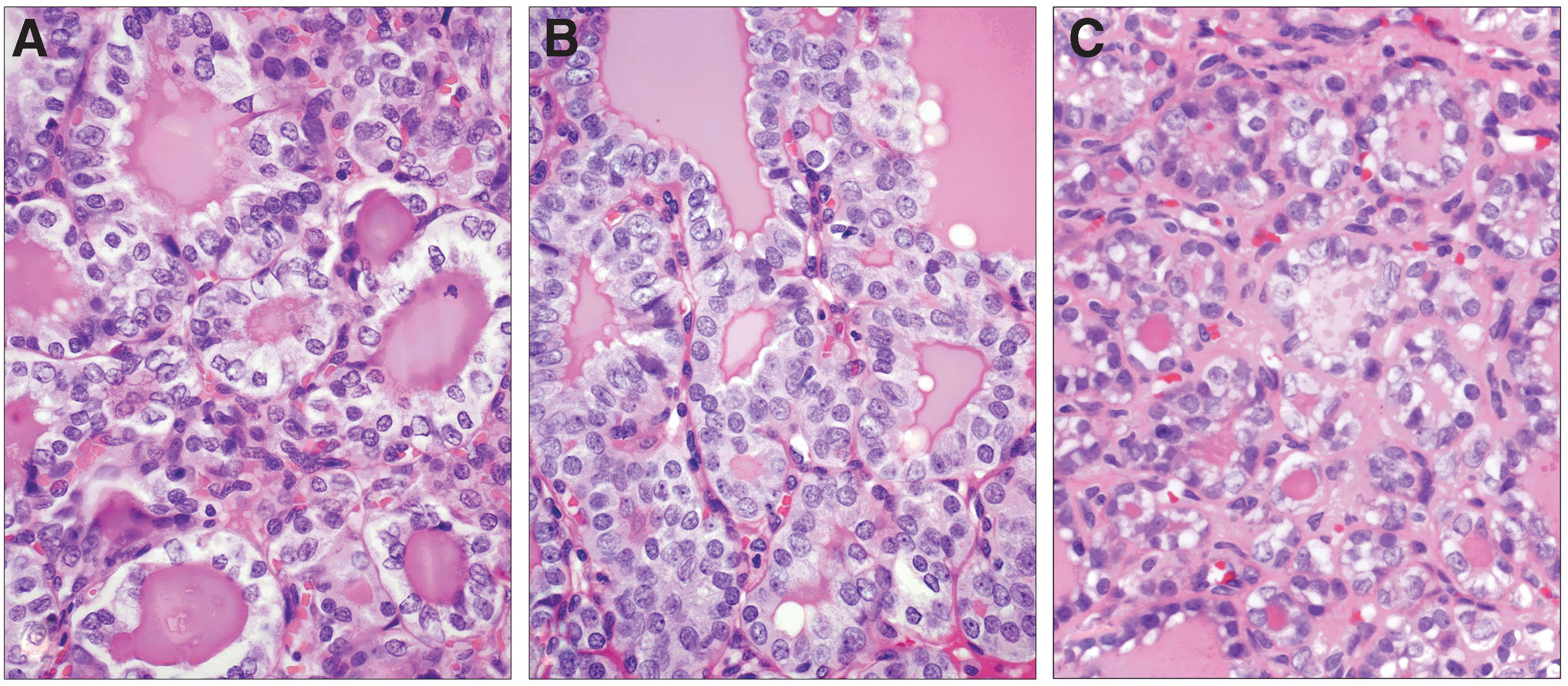
PE/WC FVPTC and mutation status. HRAS-mutant
Discussion
While FVPTC is in general an indolent tumor, further risk stratification of patients diagnosed with FVPTC is important both to identify patients who might benefit from more aggressive management and to spare others from overtreatment. Studies have shown that encapsulated and infiltrative FVPTCs follow a different clinical course and have distinct molecular profiles (18 –20). We recently evaluated the clinical outcome of FVPTCs that were neither completely encapsulated nor infiltrative, but instead were partially encapsulated or well circumscribed (43). We found that the clinical behavior of PE/WC FVPTCs was similar to that of encapsulated tumors. The aim of the current study was to determine if the molecular profile of PE/WC tumors was also similar to encapsulated FVPTCs.
In our cohort of 28 PE/WC FVPTCs, no cases had associated lymph node metastases or disease recurrence in a 72.8 months median follow-up period. These results provide additional support that PE/WC FVPTCs are clinically indolent. Targeted mutation analysis of the tumors, revealed that 13 (46%) cases harbored RAS mutations, including seven (25%) with NRAS mutations (p.Gln61Arg) and six (21%) with HRAS mutations (five had p.Gln61Arg and one had a p.Gln61Lys substitution). Tumors harboring NRAS and HRAS mutations were morphologically indistinguishable from each other and from tumors that lacked these mutations. No cases had BRAF mutations. Accordingly, all cases were also negative for BRAF V600E by immunohistochemistry. These molecular findings are similar to those of encapsulated FVPTC described by Rivera et al. (19). They found that RAS mutations were present in 36% of encapsulated tumors, of which 50% occurred in NRAS, 40% in HRAS, and 10% in KRAS. Also, similar to our findings, they found that no encapsulated tumors had BRAF mutations. In contrast, they found that infiltrative FVPTCs had a BRAF mutation rate of 26% and a RAS mutation frequency of 10%. In a study by Gupta et al. (21), the clinical and molecular features of FVPTC were also examined according to growth pattern (diffuse, non-encapsulated, and encapsulated). They reported that all diffuse tumors had associated lymph node metastases, whereas the encapsulated and non-encapsulated tumors had no associated lymph node metastases. Molecular analysis revealed a BRAF mutation rate of 50% in their diffuse group, with no underlying RAS mutations. In their encapsulated group, the BRAF and RAS mutation frequencies were 5% and 10%, respectively. In their nonencapsulated group they found a BRAF mutation frequency of 11% and no underlying RAS mutations. Different histologic classification of tumors makes it challenging to compare the results of their study with our findings. Based on prior descriptions of diffuse FVPTC (51), Gupta et al. (21) required extensive infiltration of tumor through the thyroid gland for a case to be classified as diffuse. Thus, it is likely that many of the tumors we would classify as infiltrative, would be characterized as non-encapsulated by these authors. Nonetheless, the low rate of RAS mutations in their encapsulated and non-encapsulated groups is remarkable. It is interesting that thyroid tumors harboring RAS mutations appear different histologically with some lacking nuclear features of PTC (and thus best classified as follicular adenoma or FTC), while others have diagnostic nuclear features of PTC (and thus are best classified as an encapsulated or PE/WC FVPTC). While we currently do not know of a biologic explanation for these findings, perhaps future molecular studies interrogating genes that were not evaluated on our platform will be informative.
In studying FVPTC, it is important to acknowledge that it is an entity known for problems with diagnostic reproducibility (52 –54). Due to differences in threshold for what is considered sufficient nuclear features to render a diagnosis of FVPTC, tumors that some pathologists might consider as an encapsulated FVPTC or a PE/WC FVPTC may be interpreted by others as an adenoma or adenomatous nodule, respectively. This observer variation is problematic since the divergent diagnoses would prompt different clinical management. Completion thyroidectomy and RAI treatment may be carried out for a diagnosis of FVPTC in a lobectomy specimen, whereas a diagnosis of follicular adenoma or adenomatous nodule requires no further treatment. Reporting the growth pattern of FVPTC could reduce the clinical impact of these divergent diagnoses since patients found to have either an encapsulated or PE/WC FVPTC on lobectomy, could potentially be treated with lobectomy only (the same management prompted by a diagnosis of follicular adenoma or adenomatous nodule). In this manner, evaluating the growth pattern of FVPTC could substantially reduce the clinical significance of divergent pathologic interpretations.
Based on the results of this study, and our previous outcome data (43), we would advise reporting FVPTC as encapsulated, PE/WC, or infiltrative, to distinguish the indolent PE/WC and encapsulated tumors from the more aggressive infiltrative FVPTCs. Since encapsulated and PE/WC tumors appear to have similar clinical and molecular characteristics, distinguishing an encapsulated FVPTC from a PE/WC tumor may not be clinically essential. Instead, the clinically important distinction would be distinguishing infiltrative FVPTCs from encapsulated or PE/WC tumors. In our studies, tumors that had any indication of an infiltrative border were characterized as infiltrative FVPTCs. We would advocate this approach in clinical practice as well. Additionally, although not all infiltrative tumors are associated with BRAF mutations, immunohistochemical analysis for BRAF V600E could be performed on PE/WC cases to demonstrate that the tumor lacks an underlying BRAF mutation.
In conclusion, we have shown that the molecular alterations of PE/WC FVPTCs, like their clinical behavior, are similar to those of encapsulated FVPTCs. If our results are confirmed, it would seem reasonable to advocate conservative management (i.e., lobectomy only) for patients with either PE/WC or noninvasive encapsulated FVPTCs.
Footnotes
Acknowledgments
This work was supported by the Eleanor and Miles Shore Fellowship for Scholars in Medicine, Harvard Medical School. The authors would like to thank Ms. Chanese Brown and members of the Center for Advanced Molecular Diagnostics (CAMD) for their help with this study.
Disclosure Statement
No competing financial interests exist for any of the authors.