
Abstract
Background:
Subclinical thyroid dysfunction is common among older people and has been associated with decreased functional capacity but with conflicting data. The aim of this study was to assess the association between subclinical thyroid dysfunction and functional capacity in an elderly population.
Methods:
We included 5182 participants with a mean age of 75.2 years from the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER). Self-reported functional capacity was assessed using the Barthel Index (BI) and the Instrumental Activities of Daily Living (IADL) scores at baseline and during follow-up. Participants with subclinical hyperthyroidism (n=65) and subclinical hypothyroidism (n=173) were compared to euthyroid participants (n=4944). The association between persistent subclinical thyroid dysfunction and functional capacity and decline was also investigated.
Results:
At baseline, compared to euthyroid participants (BI 19.73±SE 0.06; IADL 13.52±0.02), there was no difference in functional capacity for participants with subclinical hyperthyroidism (BI 19.60±0.09; IADL 13.51±0.12, p>0.05) or subclinical hypothyroidism (BI 19.82±0.06; IADL 13.55±0.08, p>0.05). Over a mean 3.2-year follow-up period, there was no association between thyroid function and annual decline of either BI or IADL (p>0.05). No association was found between persistent subclinical thyroid dysfunction and functional capacity at baseline or during follow-up (p>0.05). Results were similar after excluding participants with a maximum BI and/or IADL score at baseline.
Conclusion:
Among well-functioning community-dwelling elderly, we found no evidence that subclinical thyroid dysfunction contributes to decreased functional capacity.
Introduction
S
Subclinical thyroid dysfunction has been associated with several adverse outcomes, such as cardiovascular disease (8 –10), osteoporosis (1,11 –13), and cognitive dysfunction (6,14,15). Furthermore, subclinical thyroid dysfunction has also been associated with decreased functional capacity (16) and neuromuscular abnormalities (17), but data are conflicting (17 –20), and reliable evidence on the association between subclinical thyroid dysfunction and functional capacity in an older population is lacking.
Both subclinical hyperthyroidism and subclinical hypothyroidism may progress to overt disease or revert to euthyroidism in the course of months (21). Studies with repeated TSH measurements, which can identify persistent thyroid dysfunction, may be more strongly associated with specific endpoints than studies with a single measurement of TSH. To date, there are no data on the association between persistent subclinical thyroid dysfunction and functional capacity.
Therefore, we assessed the association between subclinical thyroid dysfunction and functional capacity in the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER) (22). In more than 5000 participants, we investigated the association between thyroid status at baseline and persistent thyroid status after six months, and repeated assessments of functional capacity during a mean 3.2-year follow-up period.
Methods
Subjects
All subjects were participants of the PROSPER trial, designed to assess if pravastatin would reduce the risk of cardiovascular events in an elderly population with cardiovascular disease or at high risk of developing cardiovascular disease. Details on the study design have been previously described (23). A total of 5804 men and women aged 70–82 years with pre-existing cardiovascular disease (including coronary, cerebrovascular, or peripheral artery disease) or at risk to develop such a condition (current cigarette smoking, hypertension, known diabetes mellitus, or fasting blood glucose >7 mmol/L) were randomized to receive either pravastatin 40 mg daily or placebo over a mean 3.2-year period in Scotland, Ireland, and the Netherlands. Participants with congestive heart failure (New York Heart Association III or IV), physical or mental inability to attend the clinic for the screening visit, or poor cognitive function (Mini Mental Score Examination <24 points) were excluded from the PROSPER trial.
From the initial trial population, we excluded participants with missing TSH and/or free T4 levels and with missing Barthel Index (BI) or Instrumental Activities of Daily Living (IADL) scores. Participants using antithyroid medication and/or thyroxine supplementation were also excluded. The trial protocol was approved by the Medical Ethic Committees of all involved centers, and all participants provided written informed consent.
Thyroid function
TSH was measured at baseline in all participants. Measurements were performed in three respective laboratory centers (Glasgow in the United Kingdom, Cork in Ireland, and Leiden in the Netherlands). Indications for additional measurements of free T4 were different between countries. In Scotland and Ireland, free T4 levels were measured when TSH was abnormal based upon specific cutoff levels of TSH (when TSH was <0.45 or >10 mIU/L in Scotland, and <0.3 or >5 mIU/L in Ireland), while they were measured in all participants in the Netherlands, independently of the TSH result.
TSH and free T4 levels were measured using state-of-the-art immunoassays (third-generation assays with a functional sensitivity ≤0.05 mIU/L). For both measurements, estimated inter- and intra-assay coefficients of variation were less than 5%. Both TSH and free T4 levels were measured again at six months of follow-up in available frozen plasma samples of all participants, which were stored at the University of Glasgow. The same electrochemiluminescence immunodetection method on a Roche Elecsys 2010 (Burgess Hill, United Kingdom) was used. The limits of detection were <0.005 mIU/L for TSH and 0.3 pmol/L for free T4 (reference range: 12–22 pmol/L). A reference range between 0.45 and 4.50 mIU/L derived from relevant literature was used for TSH (4,9). The narrowest free T4 reference range (12–18 pmol/L) was chosen to take interlaboratory differences into account (24).
On the basis of previous publications (4,25 –28), we classified participants into three thyroid states groups. At baseline, subclinical hypothyroidism was defined as TSH levels ≥4.5 mIU/L with normal free T4 levels. Subclinical hyperthyroidism was defined as TSH levels ≤0.45 mIU/L with normal free T4 levels. Participants with normal TSH levels (0.45–4.5 mIU/L) were considered euthyroid. At six months, we used the same classification to define subclinical thyroid status. Participants with the same condition at baseline and after six months were defined as having persistent subclinical hypothyroidism, persistent subclinical hyperthyroidism, or persistent euthyroidism. Based on previous studies (4,8,9,24,26,28) and expert reviews (4,27), we further stratified our analyses for other TSH ranges (TSH <0.1, TSH 0.1–0.45, TSH 4.5–10, and TSH >10 mIU/L).
Functional capacity
Functional capacity was measured using two questionnaires: the BI and the IADL. Both questionnaires have previously been proven to be sensitive to detect changes in an elderly population (29,30). The measurements were performed at baseline; after 9, 18, and 30 months; and at the end of the study, which varied between 36 and 42 months.
The BI is a common questionnaire used to assess self-care activities of daily living and level of dependence of an individual (31). The BI consists of 10 items, in which fecal and urinary continence, grooming, toilet use, feeding, transfers (e.g., from chair to bed), walking, dressing, climbing stairs, and bathing are scored. The maximum score of the BI is 20 points; a higher score represents higher independence and mobility, that is, higher functional capacity.
The IADL questionnaire also measures activities of daily living, but involves interaction with the physical and social environment (32), and is therefore questioning about more complex tasks compared to the BI. The questionnaire includes seven items, including housework, taking medication as prescribed, managing money, shopping for groceries or clothing, use of telephone or other form of communication, using technology, and transportation within the community. The maximum score of the IADL is 14 points; a higher score also means higher independence and mobility in both indoor and outdoor environment, that is, higher functional capacity.
Statistical analyses
Baseline characteristics are reported in three thyroid subgroups, according to thyroid status. t-Tests and chi-square tests were used to compare participants with subclinical thyroid dysfunction to euthyroid participants. We performed linear regression analyses to assess the cross-sectional association between subclinical thyroid status and functional capacity. Adjustments were made for age, sex, country, history of vascular disease, history of diabetes, history of hypertension, and current smoking.
Since treatment with pravastatin did not affect functional capacity (22), we combined data from both groups to investigate the association between subclinical thyroid dysfunction and functional decline. For this longitudinal association, we used linear mixed models, which included baseline thyroid status or persistent thyroid status, time (in years), and the interaction term between time and baseline thyroid status or persistent thyroid status. The dependent variable was the score on BI and IADL questionnaires. The change in functional capacity per year for each group was represented by the estimated value for annual change over time. Models were adjusted for age, sex, country, statin treatment, history of vascular disease, history of diabetes, history of hypertension, and current smoking.
Additionally, we further performed analyses in which we (i) investigated participants with suppressed or elevated TSH levels (TSH <0.1 or TSH >10 mIU/L); (ii) included TSH levels as a continuous variable in our analyses; (iii) stratified the analyses by cardiovascular disease and risk factors to investigate their potential confounding effect; (iv) excluded participants with a maximum BI and/or IADL score at baseline; (v) stratified the longitudinal analyses by treatment group; and (vi) used a wider free T4 range, with 10.3–25.7 pmol/L considered normal according to relevant literature (4,33). Finally, since we previously reported that subclinical hypothyroidism with TSH levels >10 mIU/L was associated with a higher rate of heart failure in PROSPER (24), a decreased level of functional capacity among those participants is expected. Therefore, we further investigated whether excluding these participants from the analyses changed our results.
p-Values below 0.05 were considered statistically significant. All analyses were conducted using SPSS (v20.0; PASW Statistics Inc., Chicago, IL).
Results
Baseline characteristics
From the initial study population of 5804 participants, 8 individuals with missing TSH values, 303 with abnormal TSH and unknown free T4 values, 136 with overt thyroid disease, and 1 with missing BI and IADL scores were excluded (Fig. 1). Six participants taking antithyroid medication and 160 participants using thyroxine supplementation were excluded. The final sample of our study was therefore 5182 participants.
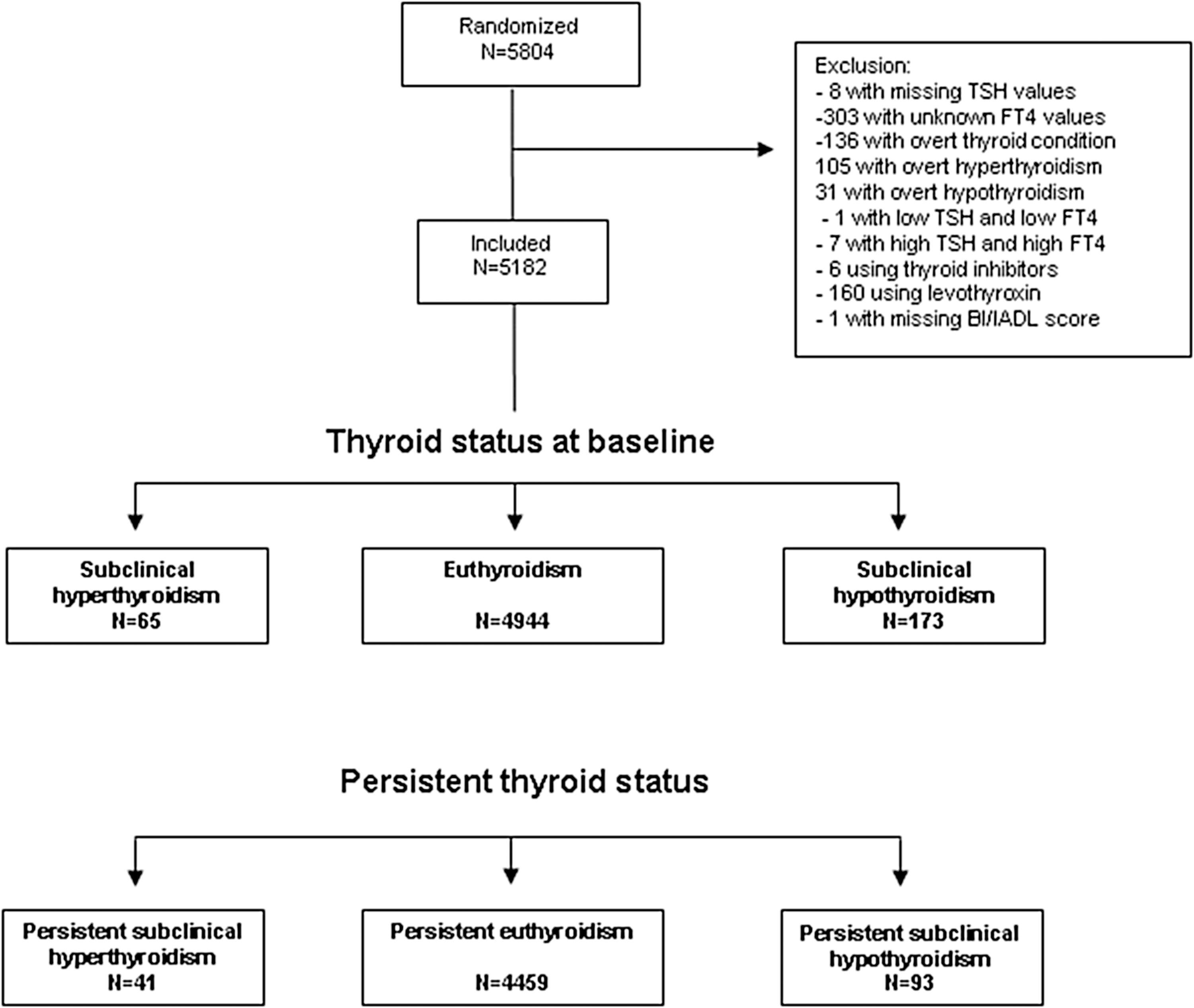
Flowchart of study participants. TSH, thyrotropin; FT4, free thyroxine; BI, Barthel Index; IADL, Instrumental Activities of Daily Living.
The mean age of the study population was 75.3 years (standard deviation [SD] 3.3 years; Table 1). A total of 65 participants had subclinical hyperthyroidism. In line with our expectation, this condition was more common in women (73.8%) than in men. Subclinical hypothyroidism was found in 173 participants, and 64.2% were women. Groups were similar on most variables, except for body mass index (BMI) and hypertension. Subclinical hyperthyroidism was associated with lower BMI when compared to euthyroid participants (25.7 vs. 26.8; p=0.03). The prevalence of hypertension was higher in participants with subclinical hypothyroidism compared to those with euthyroidism (68.2% vs. 61.0%; p=0.02).
Adjusted for age and sex.
N, number; SD, standard deviation; SE, standard error; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; TIA, transient ischemic attack.
Baseline thyroid status and functional capacity
At baseline, the overall mean BI and IADL scores were high (19.71 and 13.53 points respectively) with a range of 11–20 points for the BI and 4–14 points for the IADL (Table 2). The mean score on BI and IADL did not differ among participants with subclinical hyperthyroidism and subclinical hypothyroidism compared to euthyroid participants (p>0.05). Although a significant decrease in functional capacity over the 3.2-year follow-up time was observed for both BI and IADL (−0.09 and −0.16 points per year respectively; p<0.001), there was no difference in annual decline of BI or IADL when comparing participants with subclinical thyroid dysfunction to euthyroid participants (p>0.05). The results did not materially change after (i) investigation of potential differences within TSH subgroups (TSH <0.1 and TSH >10 mIU/L); (ii) analysis of TSH as a continuous variable; (iii) stratification by presence or absence of cardiovascular disease at baseline; (iv) exclusion of participants with a maximal BI and/or IADL score at baseline; (v) stratification by treatment group; and (vi) using a wider free T4 range (data not shown). Furthermore, we found that participants with incident heart failure hospitalization (n=235) had a significant decrease in both BI and IADL over the 3.2-year follow-up time (−0.31 and −0.51 points per year respectively; p<0.001), but excluding these participants did not change the results.
Data represent mean±SE. Adjusted for age, sex, country, history of vascular diseases, history of hypertension, history of diabetes mellitus, current smoking, and additionally for statin treatment in the longitudinal analyses.
IADL, Instrumental Activities for Daily Living.
Persistent thyroid status and functional capacity
Among the 65 participants with subclinical hyperthyroidism at baseline, 41 still had subclinical hyperthyroidism after six months and were defined as having persistent subclinical hyperthyroidism. Among the 173 participants with subclinical hypothyroidism at baseline, 93 had subclinical hypothyroidism at six months and were defined as having persistent subclinical hypothyroidism. After exclusion of participants with changing thyroid status, there were no differences in functional capacity between groups with persistent thyroid status at six months (Table 3; p>0.05). No association between persistent thyroid status and functional decline over time was observed (p>0.05).
Data represent mean±SE. Adjusted for age, sex, country, history of vascular diseases, history of hypertension, history of diabetes mellitus, current smoking and additionally for statin treatment in the longitudinal analyses.
Discussion
In this large prospective cohort study of more than 5000 older persons, including an analysis with persistent subclinical thyroid dysfunction, we found no consistent association between subclinical thyroid dysfunction and self-reported functional capacity or decline in old age.
Previously, few studies evaluated the relationship between subclinical thyroid dysfunction and functional capacity, with conflicting results. A cross-sectional study that included 42 participants with subclinical hypothyroidism found no association with functional capacity as measured by the Bruce treadmill (17). Similarly, the Leiden 85-Plus Study, a population-based study, showed that subclinical thyroid dysfunction was not associated with functional capacity in 558 participants from the age of 85 years onwards (18). Simonsick et al. showed that people between 70 and 79 years of age did not have more frequent mobility problems (20). In this study, individuals with a mild elevation in TSH levels (4.5–7 mIU/L) had a faster mean usual and rapid gait speed and better cardiorespiratory fitness and reported walking ease. Portella et al. reported that subclinical hyperthyroidism was not associated with changes in exercise performance in young female adults (19). This experimental study included only 14 participants with well-differentiated thyroid carcinoma on suppressive levothyroxine therapy leading to subclinical hypothyroidism, and assessed exercise capacity by using the treadmill cardiopulmonary test. Furthermore, a randomized study demonstrated that exercise performance was improved in individuals with subclinical hypothyroidism treated with levothyroxine after six months of TSH normalization (16).
According to several hypotheses, we expected to find an association between subclinical thyroid status and functional capacity. First, as subclinical thyroid dysfunction has been associated with cardiovascular disease (8 –10), we hypothesized a decline in functional capacity in those with subclinical thyroid status due to a higher rate of cardiovascular events, such as stroke or myocardial infarction (24). Second, literature shows that individuals with both subclinical and overt thyroid conditions have more frequent musculoskeletal symptoms. An experimental study demonstrated that higher free T4 concentrations were associated with decreased physical performance and muscle strength, independently of TSH levels (34). A cross-sectional study including 137 participants showed that Dupuytren's contracture, limited joint mobility, and carpal tunnel syndrome were significantly more common among middle-aged subjects with hypothyroidism (35). Moreover, subclinical hyperthyroidism and overt hyperthyroidism have also been associated with increased risk of osteoporosis (1,11 –13), which could also contribute to impaired functional capacity. Therefore, we expected that similar manifestations could be observed in subclinical thyroid states, leading to decline of functional capacity. Finally, as subclinical thyroid dysfunction has been linked to adverse cognitive outcomes (6,14,15), we assumed that functional capacity could be impaired in individuals with subclinical thyroid dysfunction due to additional cognitive decline.
The fact that we did not find any association between subclinical thyroid dysfunction and changes in functional capacity could be explained by two main reasons. The first is that the hypothesized biological relation does not exist. So far, only one study investigated muscle metabolism and exercise tolerance impairments as possible biological mechanisms involved in subclinical hypothyroidism (36). Muscle metabolism has also been suggested to be impaired in Hashimoto's hypothyroid myopathy (37). The few other positive studies on the association between subclinical thyroid dysfunction and functional capacity did not clearly report which biological mechanisms could be involved (16,17). Second, the participants in the PROSPER study were excluded at baseline if they had poor cognitive function (Mini Mental Score Examination <24/30 points) or if they were physically or mentally unable to attend the clinic for the screening visit (23). Therefore, the population in this study excluded elderly with functional and cognitive impairment, potentially leading to reduced power to detect changes in functional capacity. However, we did observe a significant decline in functional capacity among all participants (n=5182) and in a small subgroup analysis (n=235), suggesting that our measurements were sensitive enough to detect functional decline. Although the rate of spontaneous normalization of TSH levels in subclinical thyroid disorders can be as high as 65%, studies evaluating persistent subclinical thyroid dysfunction are rare (38,39). The fact that we have data on persistence of subclinical thyroid dysfunction, which is the most robust reflection of subclinical thyroid status and a limitation of several previous studies, together with repeated measurements of functional capacity increased our power to detect a potential association and a decline in functional capacity over time. Moreover, the large sample size of our study and the overall high prevalence of subclinical thyroid dysfunction increased the power to detect an association between subclinical thyroid conditions and functional capacity.
There are several limitations in our study. First, the studied population had a good functional capacity at baseline. Therefore, our findings are only generalizable to a high functioning population. Second, the 3.2-year follow-up period could have limited the power to detect changes in functional capacity among our population. A longer follow-up period might be needed to find changes in functional capacity. Furthermore, only two self-reporting questionnaires to assess functional capacity were used, which might be insensible to detect changes. However, it has recently been shown that subclinical thyroid dysfunction was not associated with cognitive performance or decline in the present population (33). Although cognitive decline has been reported for many determinants in the studied population (40 –42), the absence of such association between subclinical thyroid dysfunction and cognitive decline further strengthens the findings of our analyses, which shows no association with functional capacity or decline. Finally, as indications for free T4 measurements differed for each country, this could have resulted in some differences between the participants in Scotland, Ireland, or the Netherlands. However, free T4 was measured in all participants with TSH >10 mIU/L, a group in which we also did not find a significant association.
In conclusion, there is no evidence to support a relationship between subclinical thyroid dysfunction and functional capacity in a large population of well-functioning community-dwelling older people.
Footnotes
Acknowledgments
This study was supported by a grant from the Swiss National Science Foundation (SNSF 320030-138267) and partially supported by a grant from the Swiss Heart Foundation (both to Prof. N. Rodondi). The original PROSPER trial was supported by an unrestricted, investigator-initiated grant from Bristol-Myers Squibb.
Author Disclosure Statement
No competing financial interests exist. The funders had no role in analysis and interpretation of the data nor in writing and publishing of the manuscript. There are no patents, products in development, or marketed products to declare.